
A Safety Model for Preventing Nosocomial Infections in Stroke Patients
Authors Info & Affiliations
Abstract
Introduction
Hospital-acquired infections (HAIs) are cases of infection that occur in patients after being admitted to the hospital within 48–72 hours. The high number of cases of nosocomial pneumonia and urinary tract infection in the care of stroke patients can increase the length of stay and the risk of ongoing infection. The development of a safety model for preventing infection in stroke patients is urgently needed as an effort to reduce the risk of nosocomial infections in hospitals.
Materials and Methods
This type of quantitative research with a survey approach aims to formulate the construction of an infection prevention safety model with all nurse stakeholders N = 225 with a sample of n = 120 nurses. The research variables studied consisted of safety management practices, safety knowledge, safety motivation, and safety prevention. Data collection involved using a questionnaire with data analysis using a structural equation model (SEM) with the application of smart partial least square (SmartPLS 3.0).
Results
There is a positive and significant effect of safety management practices on safety knowledge (p-value = 0.000 > 0.05), safety motivation (p-value = 0.028 > 0.05), and safety prevention infection (p-value = 0.005 > 0.05). In addition, there is a positive and significant effect of safety knowledge on safety motivation (p-value = 0.028 > 0.05), safety knowledge on safety prevention infection (p-value = 0.002 > 0.05), and safety motivation on safety prevention infection (p-value = 0.001 > 0.05).
Conclusion
There is a strong influence of safety management practices on the formation of safety prevention nosocomial infection through safety knowledge. The safety prevention model of nosocomial infection in stroke patients can be recommended in an effort to prevent and reduce the incidence of nosocomial infections in hospitals.
1. INTRODUCTION
Infectious diseases are still a health problem in the world, including Indonesia. Judging from the origin or acquisition of the issue and the incidence of infection, it can originate from the community (Community-acquired infection) or originate from the hospital environment (Hospital acquired infection), which was previously known as nosocomial infection [1], thereby increasing mortality, length of stay, and cost of care [2]. With the development of the health service system, especially in the field of patient care, treatment is now possible not only in hospitals but also in other healthcare facilities, which includes home care. Medical actions performed by health workers for the purpose of treating or curing patients, if carried out inappropriately, have the potential to transmit Healthcare-Associated Infections (HAIs), both to patients and health workers themselves.
The impact of unexpected events in the form of nosocomial infections on patients and health workers is complex enough to increase the length of hospitalization for patients who experience adverse events. Data on the incidence of nosocomial infections in public health reported by the National Health Services NHS revealed that these infections affect more than 100 million patients each year globally [3]. Meanwhile, efforts to prevent nosocomial infectious diseases still need to be improved through safe, quality, and professional service management. The general condition of weak stroke patients is very vulnerable to the entry of disease germs. Therefore, it requires strict management, and even the incidence of cross-infection can be life-threatening for the patients [4].
Healthcare-associated infections (HAIs) are infections that occur in patients after admission to the hospital within 48–72 hours. The incidence of nosocomial hospital infections from 14 countries, including 4 regions of Europe, the Middle East, Southeast Asia and the West Pacific, is 10.0%. Survey results in Europe revealed that the prevalence of nosocomial infections every year is more than 4-4.5 million patients. In comparison, in the United States, the prevalence of patients with nosocomial infections per year is estimated at around 1.7 million patients with 99,000 fatalities [5]. The impact of disparities in stroke patients affects insurance and patient safety [6].
Stroke has become the 3rd most common cause of death in the world after heart disease and cancer. It can cause paralysis, which results in a decrease in independence in self-care. As a result, patients have difficulty carrying out daily life activities, such as walking, dressing, eating or controlling defecation or urination. Stroke patients with disabilities require the help of families and nurses in the hospital for quite a long time. Conditions, where the level of dependency on nursing care is very high, are very risky and cause nosocomial infections in stroke patients. Further, nosocomial infections, with a 10% incidence of pneumonia and post-stroke urinary tract infections, can complicate stroke care and can increase the risk of death [7].
The application of safety measures to avoid the risk of nosocomial infection in stroke patients is still not widely carried out, and hospitals are required to provide quality, effective, and efficient health services that guarantee patient safety in accordance with predetermined standards. One of the indicators of patient safety is reducing the risk of infection associated with health services carried out optimally so that it has an impact on high rates of nosocomial infections. The safety model framework must consider the commitment of the management to patient safety as an important dimension of safety management practice [8].
The safety model proposed by Vinodkumar and Bhasi (2010) states that there are 3 important components in safety management practices, namely safety knowledge, safety motivation, and safety performance [9]. These findings provide valuable guidance for researchers and practitioners to identify mechanisms by which they can improve workplace safety. This study aims to develop a safety model for preventing nosocomial infections and examine the relationship between factors that influence safety management in hospitalized stroke patients.
2. MATERIALS AND METHODS
This research employed a quantitative study with a survey approach that aimed to provide data sources and insights from respondents as input in constructing the safety model of Vinodkumar and Bhasi (2010) to prevent nosocomial infections in stroke patients in hospitals. The population in this study were all nurses in the inpatient unit, nursing staff leaders, and nursing committees as stakeholders, providing direct and indirect care for stroke patients, totaling 275 people. A proportionate sampling of each health worker and staff was done using the Slovin sample formula and a 5% margin of error so that the total sample included 120 nurses.
Data analysis used a structural equation model (SEM) with the Smart Partial Least Square (SmartPLS) 3.0 application [10]. Identification of analytical tests included validity and reliability tests of questionnaire instruments, inner model analysis tests, Collinearity Statistics VIF, and the results of nosocomial infection prevention safety models. While the analysis of the mediation variable regression analysis test used the coefficient product method developed by Sobel. Therefore, this test is often called the Sobel test. This test was carried out by testing the strength of direct influence between the variables like Safety Management Practices (X1), Safety Knowledge (X2), Safety Motivation (X3), and Safety Prevention Infection (Y1).
The condition for accepting the hypothesis is significant if the p-value <0.05. The nosocomial infection prevention model for stroke patients meets the requirements (goodness of fit) if the Average Full Collinearity (VIF) values for all variables are acceptable; <5 and ideally <3.
3. RESULTS
Based on the table above, Cronbach's Alpha value for internal consistency reliability is met if > 0.60, where Cronbach's Alpha values are 0.777, 0.824, 0.725, and 0.866 greater than 0.60, so the questionnaire for all variables fulfills internal reliability. The composite reliability value is fulfilled if the value is > 0.70, whereas if the composite reliability values are 0.780, 0.859, 0.735, and 0.885 greater than 0.70, then it is fulfilled so that the questionnaire for all variables fulfills composite reliability. The Average Variance Extracted (AVE) value is fulfilled if > 0.50, whereas if the Average Variance Extracted (AVE) values are 0.691, 0.588, 0.647, and 0.602 greater than 0.50, the questionnaire for all variables already describes the variables being measured (Table 1).
| - | Cronbach's Alpha | rho_A | Composite Reliability | Average Variance Extracted (AVE) |
|---|---|---|---|---|
| Safety Management Practices (X1) | 0.777 | 0.780 | 0.870 | 0.691 |
| Safety Knowledge (X2) | 0.824 | 0.859 | 0.875 | 0.588 |
| Safety Motivation (X3) | 0.728 | 0.735 | 0.846 | 0.647 |
| Safety Prevention Infection (Y1) | 0.866 | 0.886 | 0.900 | 0.602 |
| Variable | Coefficient | p-value |
|---|---|---|
| Safety Management Practices (X1) to Safety Knowledge (X2) Safety Management Practices (X1) to Safety Motivation (X3) Safety Management Practices (X1) to Safety Prevention Infection (Y1) Safety Knowledge (X2) to Safety Motivation (X3), Safety Knowledge (X2) to Safety Prevention Infection (Y1), Safety Motivation (X3) to Safety Prevention Infection (Y1) |
0.719 0.510 0.335 0.150 0.187 0.332 |
0.000* 0.028* 0.005* 0.028* 0.002* 0.001* |
Sumber: Output SmartPLS, 2023.
| - | X1 | X2 | X3 | Y1 |
|---|---|---|---|---|
| Safety Management Practices (X1) | - | - | 2,069 | 2,106 |
| Safety Knowledge (X2) | 1,000 | - | 2,069 | 2,497 |
| Safety Motivation (X3) | - | - | - | 1,645 |
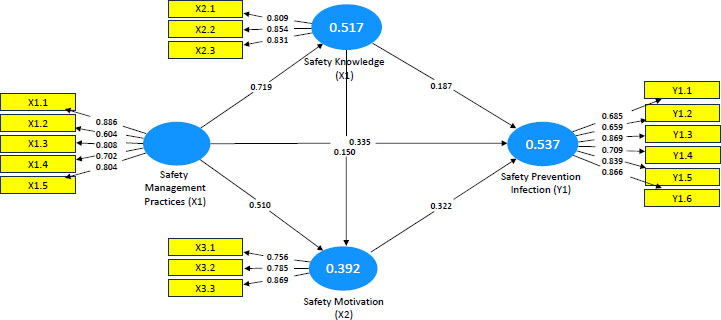
The results of the Inner Model analysis explain that there is a positive and significant direct relationship between all variables in the nosocomial infection prevention safety model.
1. The Safety Management Practices variable (X1) has an effect on the Safety Knowledge variable (X2),
2. The Safety Management Practices variable (X1) has an effect on the Safety Motivation variable (X3),
3. The variable Safety Management Practices (X1) has an effect on the variable Safety Prevention Infection (Y1),
4. The variable Safety Knowledge (X2) has an effect on Safety Motivation (X3),
5. The Safety Knowledge variable (X2) has an effect on the Safety Prevention Infection variable (Y1),
6. The variable Safety Motivation (X3) influences the variable Safety Prevention Infection (Y1)
There is an influence with the largest significant and positive coefficient, namely Safety management practices (X1) on Safety Knowledge (X2), showing a coefficient of 0.719 or 71.9% with a p-value of 0.000 <0.05. The higher the Safety management practices (X1), the higher the Safety Knowledge (X2). Meanwhile, the effect with the smallest significant and positive coefficient of Safety is found in Safety Knowledge (X2) on Safety Motivation (X3), showing a coefficient of 0.150 or 15.0% with a p-value of 0.028 <0.05. The higher the Safety Knowledge (X2), the higher the Safety Motivation (X3) (Table 2).
Based on the results of the VIF Average Full Collinearity value = 1.89 for all variables, the conditions are acceptable if <= 5. Moreover, ideally <=3 indicates that the safety model for preventing nosocomial infections in stroke patients is ideal (Table 3). The results of the SmartPLS image output show that the construction of a safety model for preventing nosocomial infections in stroke patients can be recommended (Table 3).
4. DISCUSSION
4.1. Effect of Safety Management Practices on Safety Prevention Infection
This study reveals that Safety Management Practices have a significant effect on the Safety Prevention Infection in nurses. The results of this study reveal that nurses who apply good safety management practices tend to have a high ability to prevent infection. This finding is consistent with previous studies linking safety management practices with infection prevention in the workplace [11]. Other research that is in line stated that increasing Safety Performance can be done by improving Safety Management practices to protect nurses during a pandemic. Safety Management Practices cover various measures and policies implemented in the work environment to protect employees and prevent work accidents. These practices include the use of proper personal protective equipment, good hand hygiene, strict infection control, and monitoring and reporting of infection incidents [12]. Nurses who have a good understanding of these practices and apply them consistently will have a high level of ability to prevent infection and protect themselves, their patients, and the general public.
This study also highlights the importance of the Management Commitment sub-variable in establishing effective Safety Management Practices. Management Commitment involves the commitment and support provided by management in implementing workplace safety policies and practices [13]. Strong support from management can include the allocation of adequate resources, the implementation of regular training, effective supervision, and consistent enforcement of safety policies [14]. The important role of Management Commitment in establishing Safety Management Practices shows that safety in the workplace is not only an individual's responsibility but also depends on the commitments and policies implemented by management. Management that is committed to safety will create a work culture that prioritizes safety, encouraging employees to adopt good safety practices. Complications experienced by stroke patients can be mild to severe. This can have a dangerous impact on the patient. Long treatment periods can increase the risk of infectious complications, which will have an impact on socio-economic and other clinical risks. Every action taken on a patient while hospitalized has the potential to cause an adverse event for both the patient and the health worker.
Although the results of this study demonstrate the importance of safety management practices in infection prevention, there are still some challenges to their implementation. Some of these challenges include employee compliance with safety policies, availability, and accessibility of adequate personal protective equipment, as well as limited resources that may affect the effectiveness of implementing safety practices [15]. Therefore, organizations need to invest resources and efforts in the development and implementation of effective safety management practices to maintain the safety and health of their employees and the general public as a whole.
4.2. Effect of Safety Management Practices on Safety Prevention Infection through Safety Knowledge and Safety Motivation
Safety Management Practices have a significant influence on Safety Prevention Infection, with the variables, Safety Knowledge and Safety Motivation, being mediators that influence the relationship between Safety Management Practices and Safety Prevention Infection abilities. Effective Safety Management Practices can provide relevant knowledge to workers, including nurses, about the safety practices needed to prevent infection. Good safety training and high and comprehensive discipline can increase nurse safety knowledge, providing a better understanding of infection prevention measures, use of personal protective equipment, hand hygiene practices, and infection control [16, 17]. Compliance with the 5 moments of hand washing among the health workers and the public is a global strategy in efforts to prevent and reduce cross-infection [18]. With adequate knowledge, nurses can identify potentially dangerous situations and apply appropriate preventive measures, thus increasing their skills in Safety Prevention Infection [19]. In addition, Safety Management Practices that support and promote safety can influence the motivation of nurses to comply with safety practices [20]. With clear safety policies and procedures, strong management support, and recognition of successful safety practices, nurses tend to have higher motivation to implement safety practices consistently [21]. This motivation can stem from a desire to protect oneself, patients, and members of the healthcare team and to create a safe and infection-free work environment [20]. High safety motivation will encourage nurses to apply their knowledge and take active steps to prevent the spread of infection [22], considering the hand-washing behavior of nurses plays a major role in causing infections, such as phlebitis [23]. The long period of care in stroke patients is associated with the incidence of nosocomial pneumonia infections, which, through clinical findings and laboratory tests, can worsen the condition of the patient [24]. The impact of infection treatment in the stroke unit increased during the COVID-19 pandemic outbreak, thereby increasing efforts to prevent the spread of germs through the use of personal protective equipment and reducing the risk of infection [25].
In this context, Safety Knowledge and Safety Motivation function as mediators in the relationship between Safety Management Practices and Safety Prevention Infection. Nurses who have insufficient knowledge in preventing infection in stroke patients do not know enough about treatment procedures in the stroke unit, and low hand-washing compliance can lead to cross-infection [26]. The potential for cross-infection to occur is greater in hospitals than in patients undergoing treatment at home [27]. Good Safety Management Practices provide the knowledge and support needed to enhance Safety Knowledge and encourage Nurse Safety Motivation. Increased Safety Knowledge will increase their understanding of safety practices needed to prevent infection, while high Safety Motivation will encourage them to implement this knowledge in daily practice. Through these mediators, safety management practices can positively influence the Safety Prevention Infection abilities of the nurses. Moreover, the understanding of patient treatment management that is correct and safe can improve recovery for patients [28]. Further, hospital culture promotes safety for patients and health workers as the main strategy for reducing the incidence of nosocomial infections [29].
4.3. Nosocomial Infection Prevention Safety Model
The development of work safety models in companies and health service institutions is carried out as an effort to reduce the number of work accidents and the risk of nosocomial infections that have an impact on the socio-economic and safety of patients and health workers. The results of the model suitability test with the value of Average Full Collinearity VIF = 1.89 with the construction of the safety model for preventing nosocomial infections were reportedly well. This supports the results of Basahel's research (2021), which states that safety leadership, safety knowledge, safety attitudes, and safety motivation are able to shape safety performance in companies [30]. The findings of the model (Fig. 1) show that safety in preventing nosocomial infections in stroke patients is the effect of Safety Management Practices on Safety Prevention Infection through Safety Knowledge. This nosocomial infection prevention safety model can be recommended as an effort to improve quality in prevention, control, and reduce the incidence of infection and adverse events. Hospitals must contribute to increasing marketing, brand trust, and loyalty for patients to get safe and quality services in global competition [31].
CONCLUSION
There is a positive and significant influence between the variable paths of safety management practices, safety knowledge, safety motivation and safety prevention of nosocomial infection. Moreover, the influence of safety management practices on the formation of safety prevention of nosocomial infection through safety knowledge is evident. Therefore, the safety prevention model of nosocomial infection in stroke patients can be recommended as an effort to prevent and reduce the incidence of nosocomial infections in hospitals.
LIST OF ABBREVIATIONS
| HAIs | = Healthcare-associated Infections |
| SmartPLS | = Smart Partial Least Square |
| SEM | = Structural Equation Model |
| VIF | = Variance Inflation Factor |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Research involving human subjects received a research ethics permission number: 34/EA/KEPK/2022 from the Health Research Ethics Committee of Mardi Waluyo Hospital, which is affiliated with the Ministry of Health of the Republic and is declared “applicable”.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Research Ethics referred to the guidelines of the Declaration of Helsinki with the basic principles of respect for individuals (Article 8), their right to self-determination, and the right to make informed decisions (Articles 20, 21, and 22) regarding participation in research, both initially and during the course of the research.
STANDARDS OF REPORTING
STROBE guidelines were followed.
AVAILABILITY OF DATA AND MATERIALS
The datasets used and/or analysed during the current study are available from the corresponding author.
FUNDING
The funding support was provided by a research grant from The Research and Community Service Board, Universitas Brawijaya.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
We would like to express our gratitude to Dr. Endah Woro Utami, MMRS as Director of Mardi Waluyo Hospital Blitar. We would also like to express special thanks to the Institute for Research and Community Service (LPPM) at Brawijaya University for the 2022 University of Brawijaya Doctoral Grant.

