
Investigating the Contributing Risk Factors toward Sarcopenia Prevalence and its Development in Human Immunodeficiency Virus (HIV) Patients
Authors Info & Affiliations
Abstract
Background
Human Immunodeficiency Virus (HIV) causes immune system impairment, and antiretroviral therapy (ART) given for HIV may increase the risk of morbidity and adverse health outcomes, including sarcopenia. The prevalence of sarcopenia in patients with HIV in non-Asian countries has been well-documented, but not in Asian countries.
Objective
The study aimed to investigate the prevalence of sarcopenia and its association with HIV in Thai patients.
Methods
A cross-section study was designed. This study included 114 patients with HIV from a specialized infectious disease hospital aged 20-75 years and receiving ART for more than a year. Gait speed, muscle strength, and muscle mass were measured using the 6-m walking test, handgrip dynamometer, and bioelectrical impedance analysis, respectively. Patient medical records and Global Physical Health Questionnaire scores were assessed. Logistic regression analysis was used to determine the risk of sarcopenia occurrence.
Results
The prevalence of sarcopenia was 21.93%. Risk factors for sarcopenia included duration of ART (odds ratio [OR]=16.55), advanced age (≥60 years, OR=13.50), duration of living with HIV (OR=9.44), and female sex (OR=3.79). Besides, low physical activity, which is a modifiable behavioral, had an OR of 2.78.
Conclusion
The prevalence of sarcopenia in people with HIV was 21.93%. The duration of ART was the most prominent risk factor for sarcopenia in patients with HIV. Patients with HIV should increase their physical activity levels to reduce sarcopenia risk.
1. INTRODUCTION
According to the joint United Nations Programme on Human Immunodeficiency Virus (HIV) and Acquired Immune Deficiency Syndrome (AIDS), the prevalence rate of HIV infection in the Thai population aged 15 to 49 was 1.1 in 2022 [1]. Approximately 86% (range: 78–94%) of individuals with HIV are on antiretroviral therapy (ART) [1]. The impact of HIV is a huge issue in Thailand as patients with HIV have a weakened immune system and are inclined to chronic inflammation. Living with chronic inflammation caused by oxidative stress can lead to poor physical function and loss of muscle mass.
Sarcopenia in individuals with HIV is a health problem and is related to adverse health outcomes. It is the degeneration of muscle mass and is associated with poor physical function and/or muscle strength. Sarcopenia can be categorized into two types: primary sarcopenia, which is related to age, and secondary sarcopenia [2]. Secondary sarcopenia is linked to chronic and inflammatory diseases such as HIV infections. Several studies in Western countries have reported on sarcopenia in patients with HIV, with a prevalence of approximately 20% [3-5]. However, in Asia, the prevalence of sarcopenia was reportedly only 8% in Malaysia [6]. Moreover, there are limited studies on sarcopenia in other Asian countries, including Thailand. Therefore, this study aimed to investigate the prevalence of sarcopenia in patients with HIV and their associations in Thailand.
2. MATERIALS AND METHODS
This cross-sectional study was designed to investigate the prevalence of sarcopenia in patients with HIV at the Bamrasnaradura Infectious Disease Institute, Thailand, which is a specialized hospital for infectious diseases, including HIV. The study protocol and consent form were given to the participants prior to the test.
The following formula is used to calculate the size of the required sample. N = (z)2 p (1 – p) / d2 where N is the sample size, z is the level of confidence according to the standard normal distribution (for a level of confidence of 95%, z = 1.96), p is the estimated proportion of the population that presents the characteristic. According to a previous study, the prevalence of sarcopenia in patients with HIV was 8% [6]. Therefore, our study included 114 participants were enrolled in the study. Participants living with HIV and receiving ART for at least one year were included, having ages between 20 and 75 years). Individuals with a history of neurological problems, such as stroke, head injury, or musculoskeletal disorders that affect the test or walking were excluded from sampling. The staff included physical therapists who were trained in the standard protocols of the tests. Medical history, such as comorbidities, period since HIV diagnosis, duration of ART, and Cluster of differentiation 4 (CD4) count were recorded.
The Asian Working Group of Sarcopenia Revision 2019 defined sarcopenia as poor physical performance or/and decreased muscle strength combined with low muscle mass [7]. In this study, muscle strength was measured using a digital handgrip dynamometer (TKK 5401 Grip-D; Takei Scientific Instruments Co, Ltd, Tokyo, Japan); the cut-offs for low muscle strength for sarcopenia diagnosis were <28 kg for men and <18 kg for women [7]. All participants were required to stand upright with full extension of the hand; the dynamometer was held in the dominant hand, and the greater result of two trials was recorded [7]. Physical performance was measured as gait speed using the 6-meter walking test, which was at a normal pace for two trials; the average speed was recorded. Low physical performance was defined as a speed of <1.0 m/s for the 6-meter walk for both men and women [7]. Bioelectrical impedance analysis (BIA: Omron Healthcare Co., Ltd., Japan) was used to measure muscle mass. All participants were required to void their bladder before the exam of the body mass. Low muscle mass was considered as <7.0 kg/m2 in men and <5.7 kg/m2 in women [7]. Besides, only those patients with slow speed and decreased handgrip strength underwent muscle mass evaluation.
The Global Physical Activity Questionnaire (GPAQ) was administered to determine physical activity. The GPAQ was developed by the World Health Organization and is now widely translated into many languages [8]. The GPAQ is divided into three categories: <600 metabolic equivalents (MET)*min*week−1 is defined as low physical activity, 600–1499 MET*min*week−1 is defined as moderate activity, and ≥1,500 MET*min*week−1 is defined as high activity [8].
Descriptive statistics using the t-test or chi-square test was performed as appropriate to compare individuals with and without sarcopenia. Logistic analysis with a 95% confidence interval (CI) was used to analyze the risk of developing sarcopenia in patients with HIV. The SPSS program version 24.0 was used for statistical analysis, and a p-value of <0.05 was considered significant.
3. RESULTS
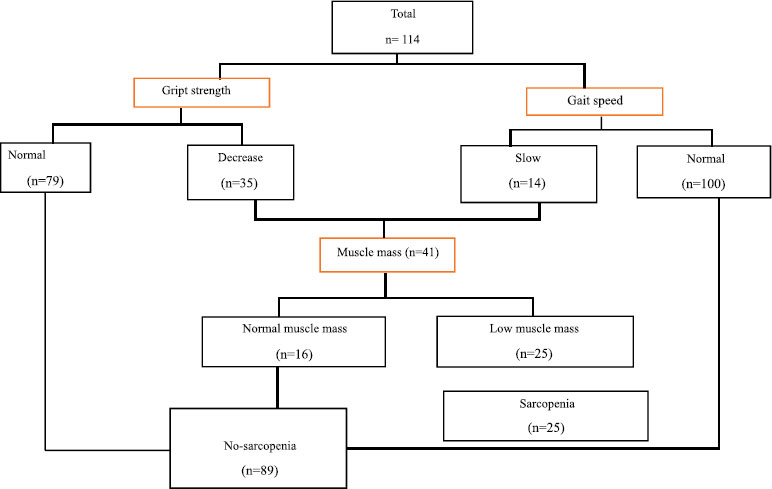
Fig. (1) displays the criteria for determining sarcopenia in participants with HIV. A total of 114 participants (60 men and 55 women) with an average age of 46.79±10.43 years were enrolled. Fourteen participants showed slow gait speed, and 35 participants had low handgrip strength; however, five participants showed both slow gait speed and decreased grip strength. Therefore, the muscle mass of 41 patients was evaluated by using BIA. Consequently, 25 participants (21.93%) were determined to have sarcopenia; 20 patients had sarcopenia and 5 patients had severe sarcopenia, which is defined as low muscle mass, decreased muscle strength, and poor physical performance. Further, significant differences in ART duration (p=.001), the period since HIV diagnosis (p=.001), CD4 cell count (p=.027), and history of dyslipidemia (p=.004). In addition, a low physical activity (defined as GPAQ scores less than 600 MET*min*week−1) was also reported in the sarcopenia group (p=.025; Table 1).
Risk factors for sarcopenia were determined using logistic regression analysis. Age, sex, history of dyslipidemia, time since HIV diagnosis, ART, and low physical activity were revealed to be the risk factors for sarcopenia. Participants with HIV who received ART for ≥20 years (OR = 16.55, 95%CI = 4.02-68.12, p<.001) had the greatest risk of developing sarcopenia, followed by those aged ≥60 years (OR = 13.50, 95%CI = 2.17-84.03, p=.005), time since HIV diagnosis of ≥20 years (OR = 9.44, 95%CI = 2.41-36.98, p =.001), female sex (OR =3.79, 95%CI =1.44-9.99, p=.007), having dyslipidemia (OR = 3.02, 95%CI = 1.07-8.52, p=.037) and low physical activity (OR = 2.78, 95%CI = 1.12-6.92, p =.028); in Table 2.
| - | Total (n = 114) |
Sarcopenia (n = 25) |
No Sarcopenia (n = 89) |
χ2 | p-value | - |
|---|---|---|---|---|---|---|
| Sex | - | - | - | 7.793 | .005 | - |
| Male (%) | 60 (100.00) | 7 (11.67) | 53 (88.33) | - | - | - |
| Female (%) | 54 (100.00) | 18 (33.33) | 36 (66.67) | - | - | - |
| Underlying diseases | - | - | - | - | - | - |
| Hypertension (%) | 20 (100.00) | 7 (35.00) | 13 (65.00) | 2.420 | .140 | - |
| Diabetes mellitus (%) | 13 (100.00) | 4 (30.77) | 9 (69.23) | 0.670 | .477 | - |
| Dyslipidemia (%) | 20 (100.00) | 8 (40.00) | 12 (60.00) | 4.626 | .041 | - |
| - |
Total (n = 114) Mean ± SD |
Sarcopenia (n = 25) Mean ± SD |
No Sarcopenia (n = 89) Mean ± SD |
t (112) | p-value | 95% CI |
| Age (years) | 46.79 ± 10.43 | 52.12±10.04 | 45.29 ±10.10 | 2.991 | .003 | 2.30 to 11.35 |
| BMI (kg/m2) | 22.86 ±3.49) | 20.14 ±2.78 | 23.62± 3.30 | -4.800 | <.001 | -4.91 to -2.04 |
| Duration of HIV (years) | 13.44 ±7.74 | 17.92 ±7.16 | 12.14±7.37 | 3.486 | .001 | 2.49to 9.07 |
| Received antiretroviral drugs (years) | 12.21 ±7.16 | 17.76 ±7.05 | 10.81±6.56 | 4.602 | <.001 | 3.96 to 9.94 |
| CD4 (cells/mm3) | 598.14 ± 310.13 | 718.88 ±424.19 | 564.22 ±262.93 | 2.242 | .027 | 17.98 to 291.33 |
| Gait speed (m/s) | 1.31 ± 0.32 | 1.16±0.27 | 1.35±0.32 | -2.687 | .008 | -0.33 to -0.05 |
| Grip strength (kg) | 27.44 ± 9.41 | 18.18±5.50 | 30.04±8.61 | -6.514 | <.001 | -15.47 to -8.26 |
| Skeletal mass index (kg/m2) | 6.53 ± 1.34 | 5.10 ±0.77 | 6.94±1.18 | -7.335 | <.001 | -2.34 to -1.34 |
| PA (MET*min*week−1) | 920.07 ± 1015.72 | 520.40 ± 625.28 | 1032.34 ± 1077.04 | -2.267 | .025 | -959.36 to -64.52 |
| Risk Factors | OR (95% CI) | P-value |
|---|---|---|
| Age | Reference < 40 years | |
| Age 40-49 years | 4.500 (0.888-22.793) | .069 |
| Age 50-59 years | 3.724 (0.725 – 19.117) | .115 |
| Age ≥ 60 years | 13.500 (2.169 – 84.033) | .005 |
| Sex | Reference male | |
| female | 3.786 (1.435-9.989) | .007 |
| Comorbidities | Reference no history of Hypertension | |
| Hypertension | 2.274 (0.793 – 6.515) | .126 |
| Comorbidities | Reference no history of Dyslipidemia | |
| Dyslipidemia | 3.020 (1.070 – 8.521) | .037 |
| Comorbidities | Reference no history of Diabetes mellitus | |
| Diabetes mellitus | 1.693 (0.475 – 6.041) | .417 |
| Duration of living with HIV | Reference duration <10 years | |
| Duration 10-19 years | 2.144 (0.513 – 8.963) | .296 |
| Duration ≥20 years | 9.444 (2.412 – 36.979) | .001 |
| Received antiretroviral drugs | Reference duration <10 years | |
| Duration 10-19 years | 2.667 (0.658 – 10.805) | .169 |
| Duration ≥20 years | 16.545 (4.019 – 68.118) | <.001 |
| Physical activity | Reference moderate to high physical activity | |
| Low physical activity | 2.781 (1.117-6.923) | .028 |
4. DISCUSSION
This study aimed to investigate the prevalence of sarcopenia and its risk in Thai patients with HIV. In 114 individuals with an average age of 46.79±10.43 years, the prevalence of sarcopenia was 21.93%. The risk factors of sarcopenia were longer duration of ART, longer time since HIV diagnosis, advanced age ≥60 years, female sex, history of dyslipidemia and low physical activity.
It was found that the prevalence of sarcopenia was 25.7% in people with HIV and was higher in patients aged >50 years and significantly higher in women than in men [3]. Similarly, a systematic review and meta-analysis from 13 studies and 2267 participants with HIV reported the prevalence of sarcopenia as 24.1% [9]. However, some studies have reported a low prevalence of 5–8% in patients with HIV [6, 10]. This difference may be because of different definitions or diagnosis criteria (e.g., defined by the European and Asian Working Group for Sarcopenia, the Asian Working Group for Sarcopenia), measurements (e.g., measured muscle mass by the dual-energy X-ray absorptiometry or bioelectrical impedance), and clinical settings (e.g., hospital, community).
In addition, according to the systematic review, the prevalence of sarcopenia may be 6.1 times greater in patients with HIV than in those without [9]. The prevalence of sarcopenia in community-dwelling older adults was 9.9–18.6%, according to the definition of sarcopenia by the European Working Group on Sarcopenia, the Asian Working Group for Sarcopenia, and International Working Group on Sarcopenia [11]. Similarly, the prevalence was 10%–27% in older adults aged ≥60 years in another study [12]. The prevalence of sarcopenia in patients with cardiovascular conditions, such as pre-operative open cardiac surgery patients, was 26.9% [13], and that in patients with heart failure was 10–69%, according to a systematic review and meta-analysis of Zhang et al. [14]. Besides, another systematic review and meta-analysis reported the prevalence of sarcopenia as 31.4% in patients with cardiovascular disease (i.e., heart failure with preserved ejection fraction and stroke), 16.2% in patients with diabetes mellitus (i.e., type 1 and type 2 diabetes mellitus), and 13.3% in patients with respiratory disease (i.e., chronic obstructive pulmonary disease and restrictive lung disease) [15]. The prevalence of sarcopenia in patients with cirrhosis was 43% [16]. Consequently, the prevalence of secondary sarcopenia is higher than that of primary sarcopenia, and the presence of chronic inflammatory disease, including immunodeficiencies, increases the risk of developing sarcopenia.
Sarcopenia in patients with HIV can be explained by the prolonged inflammation that results in changes in muscle fibers and mitochondrial dysfunction [17, 18]. Chronic inflammation causes the release of proinflammatory mediators, malfunction of T-regulatory cells, deregulation of senescent T cells, and increased muscle protein catabolism; therefore, these lead to increased loss of muscle mass [17]. Further, declining physical function in patients receiving ART can be attributed to low insulin-like growth factor (IGF)-1 levels. Decreased IGF-1 level is mediated via increasing central adiposity, low muscle mass, and reduced bone mineral density; therefore, these result in function impairment [19]. In addition, a long time since HIV diagnosis related to long duration of ART decreases skeletal muscle mass [20, 21].
Regarding comorbidities, a history of dyslipidemia was a risk factor for sarcopenia in patients with HIV in the present study, but not diabetes mellitus. Several studies have reported that participants with underlying diabetes mellitus or type 2 diabetes mellitus showed a higher risk of sarcopenia than older adults without diabetes mellitus [22, 23]. One mechanism that can explain the relationship between the duration of underlying dyslipidemia and sarcopenia in patients with HIV is taking ART. Patients with HIV who are on suppressive ART show risks for increasing the prevalence of dyslipidemia [24]. Thus, long-duration living with HIV is associated with ART and therefore, risk of dyslipidemia [25]. Previous studies found that ART aggravated oxidative stress and skeletal muscle loss that may, in part, play an important role in muscular dysfunction [26]. Therefore, it seems that a longer duration of ART results in high dyslipidemia and decreased muscle mass loss.
HIV-infected individuals with low physical activity had a 2.78 higher risk of sarcopenia than individuals with moderate to high physical activity. A sedentary lifestyle or physical inactivity with sarcopenia has been extensively documented in older adults and those with chronic illness [27-29]. With a systematic review of 14 studies and 2592 people with HIV, an increase in physical activity related to reduced risks for sarcopenia in people with HIV [30]. In addition, exercise could enhance antioxidant status and decrease mitochondrial dysfunction and inflammation [18]. Besides, exercise can potentially reverse sarcopenia; therefore, increasing physical activity or engaging in exercise can be a protective effect against muscle mass loss or physical impairment [17, 18].
To our knowledge, this is the first study in Thailand to investigate the prevalence of sarcopenia in patients with HIV. Further, all participants were enrolled in the infectious disease institute, which is a specialized hospital for patients with infectious diseases. However, the study has some limitations that should be noted. All participants were recruited at the outpatient department, so, participants were able to walk and were clinically stable. Laboratory investigations, such as inflammatory biomarkers or ART types, were not recorded. Therefore, further studies should explore the mechanism of sarcopenia and determine how to reduce the risks of sarcopenia in patients with HIV. Lastly, the single case site was conducted in the present study; therefore, the generalizability of this study is limited by the characteristics of the participants.
CONCLUSION
In the study sample, the prevalence of sarcopenia was 21.93% in individuals infected with HIV.
Longer duration of HIV and ART were associated with sarcopenia and the risk of developing sarcopenia. Low physical activity or physical inactivity is a modifiable risk factor for sarcopenia in patients with HIV. Therefore, an assessment of sarcopenia should be considered in people with HIV and promote physical activity in people with HIV.
KEY MESSAGE
• The prevalence of sarcopenia was 21.93 in Thai people living with HIV.
• Long duration of antiretroviral therapy is the greatest risk factor for sarcopenia.
• Physical inactivity is a modifiable health behavioral risk factor of sarcopenia.
ABBREVIATIONS
| IGF | = Insulin-like Growth Factor |
| HIV | = Human Immunodeficiency Virus |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The protocol was approved by the Institutional Review Board of Bamrasnaradura Infections Diseases Institute, No. S043h/63; Thai Clinical Trials Registry is TCTR20210701006.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committees and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Participants who received the information sheet were required to sign the consent form before participating in the study.
STANDARDS OF REPORTING
STROBE guidelines were followed.
AVAILABILITY OF DATA AND MATERIAL
All the data and supporting information are provided within the article.
FUNDING
This study was supported by Thammasat University Research Fund, Contract No TUFT 40/2565.
CONFLICT OF INTEREST
The authors have no conflict of interest in the study.
ACKNOWLEDGEMENTS
Declared none.
DECLARATION OF FIGURES AUTHENTICITY
All figures submitted have been created by the authors, who confirm that the images are original with no duplication and have not been previously published in whole or in part.

