All published articles of this journal are available on ScienceDirect.

Correlation Between the Well-Being of Children and Caregivers
Abstract
Background:
Well-being relates to the quality of life of people; such as the knowledge and behavior of caregivers regarding the health and care of their children, personal welfare and benefits for the environment, which are indicators of health planning for children and caregivers in the community.
Objective:
The purpose of this study was to explore the personal and environmental well-being of children and caregivers and examine the correlation between their well-being in a northern-Thai suburban community.
Methods:
The study comprised of two phases, which developed and examined the content validity and reliability of the questionnaires used on the well-being of children and caregivers, and interviewed participants by using the questionnaires. The participants included thirty Thai children aged 3-6 years and twenty-nine caregivers.
Results:
The results indicated that 8 behavioral items (38.10%) of well-being were presented by the children, and 13 (61.90%) not, while 9 behavioral items (28.13%) of well-being were presented by the caregivers, and 23 (71.87%) not. The Pearson’s coefficient of correlation of well-being and personal well-being between the children and caregivers had a significant relationship (r = 0.423, p = 0.040 and r = 0.383, p = .022, respectively). However, it did not correlate significantly in terms of environmental well-being.
Conclusion:
There was a significant correlation between the well-being of children and their caregivers, particularly in personal well-being. This study provided an understanding that can be used as fundamental information that enables healthcare teams to perceive the well-being of caregivers and their children, which relates to achieving healthy behavior.
1. INTRODUCTION
Health information has been surveyed generally at the national level for the purposes of planning and policy making [1]. The health of people is related to well-being, which not only means happiness, but also personal development, fulfillment, and contribution to the community [2]. The meaning of well-being is referred usually to satisfaction with life in daily activities. In addition, well-being relates to the quality of life of people. The World Health Organization (WHO) defined quality of life as an individual’s perception of their position in life in the context of culture and value systems in which they live, and in relationships to their goals, expectations, standards and concerns. It is a wide -ranging concept with complex effects by way of the person’s physical health, psychological state, personal beliefs, social interaction and the relationship they have with salient features of their environment [3]. However, the well-being of children is more complex than that of adults because children are dependent. Participation in daily life activities and the environmental context are important factors of children’s health and well-being [4]. Their daily activities and environment are limited by their parents, families, caregivers and teachers, as shown in the study of Prachaya-arporn [5], in which the knowledge and behavior of caregivers are related to the health and well-being of children. Children with difficulties, in particular, those experiencing the need to receive healthcare services from healthcare professionals during their development, require more care from their caregivers [6]. As children are a group of dependent people, their caregivers need to adapt and restructure their responsibilities over time. Caring for children takes more time and demands more attention for safety and health concerns, and while some caregivers can manage this well, others cannot [4]. Therefore, the well-being of children should be studied together with that of their caregivers. Characteristics relating to the well-being of children and caregivers include socio-economic factors and the environmental context. In other words, the well-being of children and that of caregivers relate to personal and environmental factors. Personal well-being is a feeling of happiness within a person. It includes physical strength with healthy behavior and psychological strength with emotion and stress management. Environmental well-being involves the physical and social environment. Both types of well-being influence occupational performance, including self-care, work or education, leisure or play and social participation [7].
The study of well-being in children and caregivers is still limited, particularly in the community. This study applied the Person Environment Occupation (PEO) model, which explains the relationships between Person, Environment, and Occupation. This model can be approached systematically for considering issues of occupational performance in human functioning and experience. Therefore, many therapists apply the PEO model as a tool for analyzing and encouraging clients to engage successfully in meaningful occupations in their environment. Indeed, children will perform occupations such as self-care, education, play and social participation that are influenced by their physical, institutional, social and cultural environment. In turn, caregivers also will perform their occupation in line with their personal, cultural and environmental contexts [8]. Moreover, the International Classification of Functioning, Disability and Health (ICF) was applied in this study. The ICF is a WHO framework that classifies health and health-related domains for measuring health, disability and environmental factors at both individual and population levels [9]. Consideration of the PEO model and ICF framework in this study could ensure that well-being covers health and function in the context of children and caregivers. Therefore, this study aimed to explore the personal and environmental well-being of children and caregivers, and examine the correlation between their well-being in a northern Thai suburban community. This objective can provide useful information for health service providers in developing local policy and encouraging good health and well-being.
2. MATERIALS AND METHODOLOGY
This study comprised of two phases, of which the first developed and examined the content validity and reliability of the research instruments that comprised questionnaires on the well-being of children and caregivers, as constructed by the researchers. The questionnaires were based on the Person Environment Occupation (PEO) model, with their items developed from the International Classification of Functioning, Disability and Health (ICF) framework, as shown in Table 1. The children’s well-being questionnaire consisted of 2 parts, including 11 items of personal and 10 of environmental well-being. The caregivers’ well-being questionnaire also comprised of 2 parts, including 21 items of personal and 12 of environmental well-being. The items were scored on a dummy scale: 0 = No and 1 = Yes. The questionnaires were processed for content validity by suggestions from five related specialists. The consistency of internal reliability was tested and the results revealed the acceptable internal consistency of α = .73 and α = .70 for the children’s and caregivers’ well-being questionnaire, respectively.
| Well-being Domains | ICF Domains | Chapter Inclusions |
|---|---|---|
| Personal well-being of the children | Activities and participation | Chapter 4 Mobility Chapter 5 Self-care Chapter 7 Interpersonal interactions and relationships |
| Environmental well-being of the children | Activities and participation | Chapter 9 Community, social and civic life |
| Environmental factors | Chapter 2 Natural environment and human-made changes to the environment |
|
| Chapter 3 Support and relationships | ||
| Personal well-being of the caregivers | Activities and participation | Chapter 1 Learning and applying knowledge |
| Chapter 2 General tasks and demands | ||
| Chapter 5 Self-care | ||
| Chapter 6 Domestic life | ||
| Chapter 7 Interpersonal interactions and relationships | ||
| Chapter 8 Major life areas | ||
| Chapter 9 Community, social and civic life | ||
| Environmental well-being of the caregivers | Activities and participation | Chapter 9 Community, social and civic life |
| Environmental factors | Chapter 2 Natural environment and human-made changes to the environment | |
| Chapter 3 Support and relationships |
The second phase consisted of interviews with the participants by using the questionnaires in San Klang sub-district of San Kamphaeng district, Chiang Mai, Thailand. The participants comprised thirty Thai children aged 3-6 years, who were studying in schools in this area, including Ban Morn School and San Klang Neour School, and twenty-nine caregivers. Only Thai citizens living in that area were included in this study, which obtained approval from the Research Ethics Committee of the Faculty of Associated Medical Sciences, Chiang Mai University. The participants were then contacted by the researchers and asked to sign informed consent and assent forms. After that, they were interviewed by the researchers using the children’s and caregivers’ well-being questionnaire. Data were analyzed by descriptive analysis, including number and percentage of behavioral items. In addition, the well-being of the children and caregivers was analyzed to examine the Pearson product-moment correlation.
3. RESULTS
General information on the well-being of the children and caregivers was received after the interviews. The child participants comprised of 15 females and 15 males. Many were aged 4–4.11 years old (33.33%), underweight (BMI of less than 18.5) (70.00%), and most of them lived in extended families (53.33%). In addition, the caregivers consisted of 12 females and 17 males. Only 2 of them were not parents, and many were aged 20-30 years old (48.27%), graduated from high school (48.28%) and employed (75.86%), as shown in (Table 2).
| Characteristics | Number | Percentage |
|---|---|---|
| Gender of the children | ||
| Male | 15 | 50.00 |
| Female | 15 | 50.00 |
| Gender of the caregivers | ||
| Male | 12 | 41.38 |
| Female | 17 | 58.62 |
| Age of the children (years old) | ||
| 3 – 3-11 | 4 | 13.33 |
| 4 – 4-11 | 10 | 33.33 |
| 5 – 5-11 | 8 | 26.67 |
| 6 – 6-11 | 8 | 26.67 |
| Age of the caregivers (years old) | ||
| 20 – 30 | 14 | 48.27 |
| 31 – 40 | 13 | 44.83 |
| 41 – 50 | 1 | 3.45 |
| > 50 | 1 | 3.45 |
| BMI* of the children | ||
| Underweight (BMI < 18.50 kg./m2) | 21 | 70.00 |
| Normal weight (BMI = 18.50 – 22.90 kg./m2) | 7 | 23.33 |
| Overweight (BMI = 23.00 – 24.90 kg./m2) | 2 | 6.67 |
| Family type of the children | ||
| Single family | 14 | 46.67 |
| Extended family | 16 | 53.33 |
| Education of the caregivers | ||
| not educated | 4 | 13.79 |
| primary school | 7 | 24.14 |
| high school | 14 | 48.28 |
| undergraduate | 4 | 13.79 |
| Occupation of the caregivers | ||
| own business | 3 | 10.34 |
| employee | 22 | 75.86 |
| housewife | 4 | 13.80 |
| Relationship of caregivers to the children | ||
| parents | 27 | 72.41 |
| not parents | 2 | 6.90 |
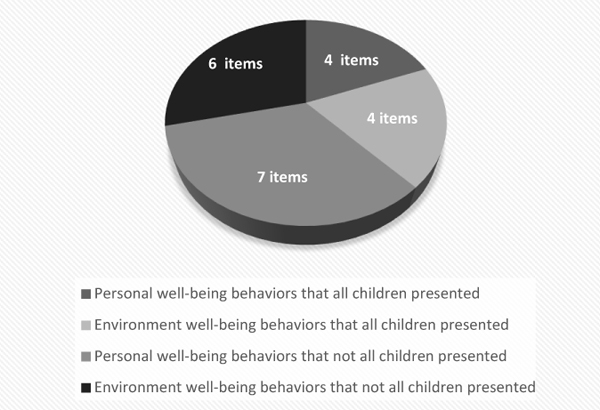
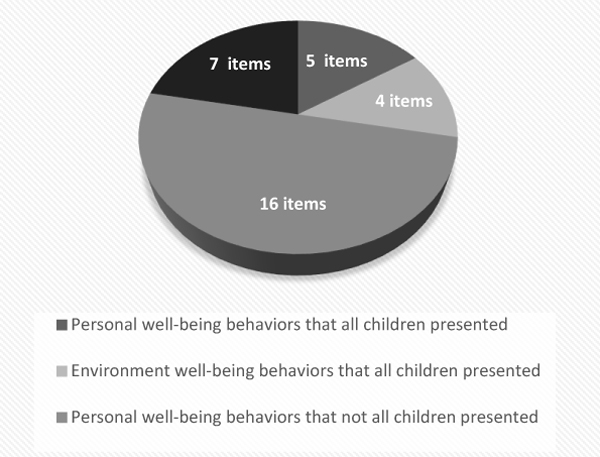
In terms of the personal and environmental well-being of the children, the results presented 4 (36.36%) and 4 (40.00%) behavioral items of personal and environmental well-being, respectively. Overall, 8 behavioral items (38.10%) of well-being were presented by the children, and 13 (61.90%) not. In terms of the personal and environmental well-being of the caregivers, the results presented 5 (23.81%) and 4 (36.36%) behavioral items of personal and environmental well-being, respectively. Overall, 9 behavioral items (28.13%) of well-being were presented by the caregivers, and 23 (71.87%) not, as shown in (Figs. 1-2).
In terms of the personal well-being domain of the children, brushing teeth twice daily was the item mostly unperformed by the children (26.67%). In terms of their environmental well-being domain, some children (6.67%) indicated that they did not live in a place that provided necessary facilities such as water, electricity or waste management, and they did not participate in outdoor activities with their family at least twice a week, as shown in (Table 3).
| Behavioral Items | Yes | No |
|---|---|---|
| Personal well-being domain | ||
| 1. Sleep for 8-10 hours per day | 30 (100.00) | / |
| 2. Do movement or outdoor activities 3-4 days/week | 29 (96.67) | 1 (3.33) |
| 3. Shower twice daily | 25 (83.33) | 5 (16.67) |
| 4. Brush teeth twice daily | 22 (73.33) | 8 (26.67) |
| 5. Clean and wash hands every time after toileting | 29 (96.67) | 1 (3.33) |
| 6. Receive educational preparation | 30 (100.00) | / |
| 7. Enroll in school at an appropriate age | 30 (100.00) | / |
| 8. Adjust or control emotion when feeling angry | 25 (83.33) | 5 (16.67) |
| 9. Participate in home activities as a family member | 28 (93.33) | 2 (6.67) |
| 10. Be responsible for mistakes and apologize to others | 29 (96.67) | 1 (3.33) |
| 11. Participate with peers | 30 (100.00) | / |
| Environmental well-being domain | ||
| 1. Live in the place that supports and enables him/her to do daily life activities independently | 29 (96.67) | 1 (3.33) |
| 2. Have enough area around their home for playing and learning | 29 (96.67) | 1 (3.33) |
| 3. Live in place that provides necessary facilities such as water, electricity, waste management, etc. | 28 (93.33) | 2 (6.67) |
| 4. Live in place that has no pollution | 29 (96.67) | 1 (3.33) |
| 5. Receive care from family when sick or facing problems | 30 (100.00) | / |
| 6. Live in a loving and harmonious family | 29 (96.67) | 1 (3.33) |
| 7. Participate in leisure activities with their family | 30 (100.00) | / |
| 8. Participate in outdoor activities with their family at least twice a week | 28 (93.33) | 2 (6.67) |
| 9. Receive educational support from family members | 30 (100.00) | / |
| 10. Live in a peaceful community | 30 (100.00) | / |
Furthermore, in terms of the personal well-being domain, many caregivers indicated that they neither ate substantial meals every day (48.28%) nor exercised 3-4 days per week (44.83%). In terms of the environmental well-being domain, some caregivers (13.79%) did not live in a stable or clean environment or community that arranged health promotion, as shown in (Table 4).
| Behavioral Items | Yes | No |
|---|---|---|
| Personal well-being Domain | ||
| 1. Have good health, especially no serious health problems | 23 (79.31) | 6 (20.69) |
| 2. Have three meals daily | 27 (93.10) | 2 (6.90) |
| 3. Eat substantial meals daily | 15 (51.72) | 14 (48.28) |
| 4. Exercise 3-4 days per week | 16 (55.17) | 13 (44.83) |
| 5. Sleep for 6-8 hours per day | 27 (93.10) | 2 (6.90) |
| 6. Perform self-hygiene activities independently | 29 (100.00) | / |
| 7. Manage risks of accidents | 26 (89.66) | 3 (10.34) |
| 8. Receive health services from government benefits | 23 (79.31) | 6 (20.69) |
| 9. Have no chronic stress or anxiety | 25 (86.21) | 4 (13.79) |
| 10. Feel no anger in minor situations | 23 (79.31) | 6 (20.69) |
| 11. Control or manage angry feelings in any situation | 27 (93.10) | 2 (6.90) |
| 12. Solve problems by acceptable strategies | 25 (86.21) | 4 (13.79) |
| 13. Be happy to work | 27 (93.10) | 2 (6.90) |
| 14. Be responsible in work or jobs | 29 (100.00) | / |
| 15. Manage stress by acceptable strategies | 24 (82.76) | 5 (17.24) |
| 16. Be happy and satisfied with life | 27 (93.10) | 2 (6.90) |
| 17. Understand and offer help to others who are facing problems | 29 (100.00) | / |
| 18. Help others when they request it | 28 (96.55) | 1 (3.45) |
| 19. Listen respectfully to other opinions | 29 (100.00) | / |
| 20. Be responsible for mistakes and apologize to others | 28 (96.55) | 1 (3.45) |
| 21. Forgive other people unconditionally | 29 (100.00) | / |
| Environmental well-being Domain | ||
| 1. Live in a stable and clean environment | 25 (86.21) | 4 (13.79) |
| 2. Live in place that provides necessary facilities such as water, electricity, waste management, etc. | 28 (96.55) | 1 (3.45) |
| 3. Live in a safe place that is far away from pubs, shops selling alcohol and illegal drugs | 26 (89.66) | 3 (10.34) |
| 4. Live in a safe community that has no local conflicts or crime | 29 (100.00) | / |
| 5. Live in place that has no pollution | 28 (96.55) | 1 (3.45) |
| 6. Live in a community that arranges areas of health promotion | 25 (86.21) | 4 (13.79) |
| 7. Live in a loving and harmonious family | 29 (100.00) | / |
| 8. Participate in family activities at least twice a week | 27 (93.10) | 2 (6.90) |
| 9. Receive care from family when sick or facing problems | 29 (100.00) | / |
| 10. Have family members that respect each other’s opinions and decisions | 29 (100.00) | / |
| 11. Live in a peaceful community | 28 (96.55) | 1 (3.45) |
Finally, the well-being of children and caregivers was analyzed for examining the Pearson product-moment correlation. The result indicated that the mean and standard deviation scores of well-being for the children and caregivers were 19.97 + 1.50 and 28.93 + 2.60, respectively. The correlation between the well-being of children and caregivers was a significantly moderate relationship (r = 0.383, p = 0.04). Furthermore, in terms of personal well-being, the result also showed a significantly moderate relationship between the children and caregivers (r = 0.423, p = 0.022). On the other hand, in terms of environmental well-being, the result showed that the relationship between the children and caregivers was weak and insignificant (r = 0.383, p = 0.04), as shown in (Table 5).
| Domains | Children | Caregivers | p-value | r | ||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| Personal well-being | 10.23 | 1.17 | 18.48 | 2.05 | 0.022* | 0.423 |
| Environmental well-being | 9.73 | 0.58 | 10.45 | 0.95 | 0.393 | 0.165 |
| Total | 19.97 | 1.50 | 28.93 | 2.60 | 0.040* | 0.383 |
4. DISCUSSION
The results of this study showed that most of the children did not present behavioral items, in either personal or environmental well-being, although they performed basic health behavior like all children do. These results reflected on the need of children in this study for health promotion in order to encourage behavioral items of well-being. Although personal well-being was encouraged in areas of education, it lacked encouragement to carry out self-hygiene, particularly oral hygiene. This study found that parents usually focused on brushing teeth in the morning because their children had social activities all day in schools. However, they might not emphasize on brushing teeth at night because their children would not talk to others while asleep. This result indicates that parents pay attention to social participation and encourage children from an early age to care for themselves for social activities [2]. In addition, the children reflected that they did not find it necessary to brush their teeth before going to bed. Therefore, these children in this suburban community need to pay more attention to self-hygiene, especially dental care. The promotion strategy may provide information that will help parents and caregivers to understand correct methods and necessary dental care. Moreover, this study found that the caregivers performed personal well-being in self-hygiene, work and social participation, relating to human occupation of the occupational therapy practice framework [10]. However, some caregivers did not devote importance to having substantial meals because they lived in a suburban community and their low income restricted their choice of food [11, 12]. In terms of environmental well-being, both children and caregivers reflected the lack of health promotion in areas of the community, which could be multipurpose for exercising, playing, learning and doing outdoor activities. These results related to the PEO Model, which explains the relationships between personal factors, the physical and cultural environment, and daily activities of children and their caregivers [6].
In addition, this study found a significantly moderate relationship between the well-being of the children and caregivers that related to many studies, which indicated child well-being as being predictable by parent or family characteristics [13]. This meant that when the caregivers had quality well-being, child well-being was improved. In particular, the personal well-being of the children and caregivers also indicated a significantly moderate relationship because the children in this study were pre-school and needed more care in preparing self-care performance independently. Therefore, the caregivers might be a model in training their children. However, a weak relationship was found, and not significant, between the environmental well-being of children and caregivers. This might be because the environment of pre-school children is the home and kindergarten school that especially manage to encourage child development, while the caregivers’ environment is not only the home, but also communities and workplaces. Poor suburban communities and workplaces might not support complete facilities or arrange areas of health promotion. This information illustrates community problems to local policymakers and related health professionals and makes them aware and plan to improve well-being for the people.
Health service providers in the community must not only consider personal well-being, the environment, and health status of the children, but also focus on the same for caregivers. In fact, when children grow up in a healthy and well-being environment and are cared for by the caregivers concerned with it; they achieve a good quality of life. This study provided fundamental information for healthcare teams when performing their service plans and working with the community in order to encourage health and well-being. Caregivers should be provided with programs that cover personal health support and environmental well-being as well as psychological support, particularly for children with special needs [14].
5. LIMITATION
This research was conducted in a small village that had two local schools for preschool children, aged 3-6 years. They were small schools that had a minority of students because most local children were enrolled in private schools in the city, which had better educational facilities. Therefore, the sample size was small in this study, in which the results might have a limitation in generalizing to other villages with different contexts.
CONCLUSION
Well-being is related to the quality of life and level of participation in daily life activities of children and their caregivers. Personal and environmental factors were impacted into well-being because they influenced the occupational performances and social participation of children and their caregivers. However, the study of well-being in children and caregivers was limited in the community. This study applied the PEO model and ICF framework to measure personal and environmental well-being. The results indicated that both the children and caregivers needed health promotion services to encourage their personal well-being, particularly in oral hygiene and having substantial meals. In terms of environmental well-being, both the children and caregivers reflected the lack of areas in the community for exercising, playing, learning and doing outdoor activities. In addition, this study found a significantly moderate relationship between the well-being of the children and caregivers. These findings are useful for relating health service providers in the community to encourage children to grow up in a healthy and well-being environment and be concerned for the well-being of caregivers in achieving a good quality of life.
ETHICS APPROVAL AND CONSENT OF PARTICIPANTS
This study obtained approval from the Research Ethics Committee of the Faculty of Associated Medical Sciences, Chiang Mai University.
HUMAN AND ANIMAL RIGHTS
No animals/humans were used for studies that are the basis of this research.
CONSENT FOR PUBLICATION
Informed written consent was obtaind from all the participants.
CONFLICTS OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
This research was supplied with tools and equipment by the Department of Occupational Therapy, Faculty of Associated Medical Sciences, Chiang Mai University.

