All published articles of this journal are available on ScienceDirect.

Association of Household Fuel Type, Kitchen Characteristics and House Structure with Child Size at Birth in Wolaita Sodo, Southern Ethiopia
Abstract
Background:
Small sized child at birth is associated with household fuel use particularly from biomass fuel type. Household air pollution is believed to affect the fetus directly through trans-placental exposure or indirectly by adversely impacting birth outcome which resulted from a small-sized child at birth. It is an important predictor of children's health and is associated with higher risk of infant and child mortality due to various contributing factors. This study ascertained the association between household fuel types, kitchen characteristics and house structure with child size at birth in Wolaita Sodo, Southern Ethiopia.
Methods:
A cross-sectional study among 1042 mothers paired with their child aged between 0-59 months was employed. Participants were selected using systematic random sampling from 6 Kebeles. The size of a child at birth was determined based on the mother’s report. Data were entered using Epi Data version 3.1 and analyzed using SPSS version 21.
Results:
The prevalence of small size at birth was 16.3%, (95% CI 14.2%-18.6%). Children were relatively equally distributed by age. The mean age of the children was 23.74 ± 14.93 months. Sixty-one percent of households used charcoal followed by biomass fuel (23.4%) for cooking activities. About 322 (30.9%) houses had one room, 504 (48.4%) houses had one door and 431 (41.4%) houses had only one window. Biomass fuel type (AOR, 3.83, 95% CI, 1.95-15.35), cooking place inside the house (AOR, 2.27, 95% CI 1.88-5.88, house without window, (AOR, 4.79, 95% CI 1.56-14.69), time spent for three or more hours in cooking, (AOR, 2.45, 95% CI 1.16-5.21) were significantly associated with child size at birth.
Conclusion:
Small size child at birth is still the concern of the study area. Using biomass fuel, cooking inside the house, more time spent in cooking and houses without window were determinants. Therefore, we recommend to the concerned stakeholders to work on clean fuel technologies and improving house designs to assuage related problems.
1. BACKGROUND
Household Air Pollution (HAP) caused by inefficient use of solid fuels and kerosene for cooking accounts for 3.8 million to 4 million premature deaths per year worldwide [1]. Early life exposure to household air pollution has been linked to a range of adverse child health outcomes, including low birth weight and pneumonia. Household air pollution affects the poorest households that are unable to afford clean, efficient cooking practices [2]. Nearly three billion of the world's population continues to rely on solid fuel, including biomass fuels (wood, animal dung, and crop waste) to meet their energy needs [3]. Institute for Health Metrics and Evaluation (IHME), has identified household air pollution from solid fuels as the 8th leading risk factor for Global Burden of disease worldwide [4].
It is now recognized that health is affected by air pollution that primarily occurs in the rural indoors, from pollutants released during the incomplete combustion of solid fuels in households [5]. African nations alone accounted for 32% of the total attributable burden of disease related to HAP [2]. Global estimate indicated that approximately 21 million infants are born with low birth weight each year. The incidence of low birth weight varies significantly across countries, ranging from 6 to 18% [6].
Type of high pollution cooking fuels (such as biomass, coal, and kerosene) used in the household is the second leading cause of low birth weight next to maternal smoking and exposure to environmental tobacco smoke [7]. The use of biomass fuels in rural areas subjects the population to high household air pollution, due to incomplete combustion in traditional stoves produces high levels of household air pollutants. This smoke contains a range of health deteriorating substances that, at varying concentrations, can pose a serious threat to human health [8, 9].
Housing characteristics were determined to indicate ventilation in Honduran communities which showed that designing kitchens with proper ventilation structures could lead to improved household environments, especially important in areas where biomass will continue to be the preferred and necessary cooking fuel for some time [10].
Household air pollution, particularly NO2 in Butajira, Ethiopia, has been studied recently, and the concentration levels showed that large groups in the rural population of Ethiopia are exposed to NO2 concentrations more than double the currently proposed annual mean of WHO air quality guideline, that is regarded as potentially harmful [11].
To establish the relation of HAP with birth weight and stillbirth, systematic reviews with meta-analyses were conducted. The study revealed that, IAP was associated with increased risk of low birth weight (OR = 1.38, 95% CI: 1.25, 1.52) and stillbirth (OR= 1.51, 95% CI: 1.23, 1.85) and reduced mean birth weight (−95.6 g, 95% CI: −68.5, −124.7) [12]. Household combustion of solid fuels resulted in 86.43 g (95% CI: 55.49, 117.37) reduction in birth weight [13], significantly increased risk of low birth weight was reported in the studies with odds ratio ranging from 1.1–1.86 [14].
The rates of low birth weight reach up to 50% in some developing countries, the prevalence of low birth weight in Nigeria was 20.5% [15], in India 20% [16], in Assam (India) 21.8% [17], in Pakistan 60.5% [18], and in Bangladesh 17.7% [19].
According to the report of Ethiopian demographic and health survey among children born in five years before the survey, the reported value of child size at birth was smaller than the average size which was 26% [20]. Ethiopia is a country which is found in sub-Saharan Africa, where, 84% of the population are found in rural areas who have no access to electrical power for heating houses, cooking foods and lighting. Studies were limited to point out the relationship between household fuel types, house structure and kitchen characteristic and child size birth. Therefore, the main aim of this study was to ascertain the relationship between household fuel type, housing structure and kitchen characteristics with reported child size at birth in Wolaita Sodo, Southern Ethiopia.
2. METHODS
2.1. Study Context
The study was conducted in Wolaita Sodo town in February 2017, which is situated 329 km from Addis Ababa in the Southern part of Ethiopia. Wolaita Sodo town is the administrative capital city of Wolaita zone. The town has three sub-cities and 11 Kebeles (the smallest administrative unit in the country). The town has a population of 111,616 and also has 22,777 households. The number of mothers whose age between 15-49 years old was 3829 and the number of under-five year children was 17,421. The town has one private and one government hospital. There are three health centers, many private clinics and drug vendors in the town. The most important source of fuel used in the households of Wolaita Sodo was firewood 94.6%, charcoal 96.6%, kerosene 11.5%, electricity 14.2%, crop residue 2.02%, dung cake 6% and sawdust 23.7% [21].
2.2. Study Design
A cross-sectional study design was used to ascertain the relationship between cooking fuel types, kitchen characteristics and housing structure with child size at birth in children aged between 0-59 months.
2.3. Source Population
All mothers who paired with their under-five years of age child participated in the study. In a random selection, 1042 mothers were included. Eligible mothers were all mothers of age 15-49 years, available during the survey time, being the residents of Wolaita-Sodo town (living at least six months in Wolaita-Sodo town). Seriously ill mothers were excluded from participation in the study. If two or more children were available in a house, one child was randomly selected.
2.4. Sample Size and Sampling Procedure
The sample size was determined based on analytic cross-sectional study design. We used a single population proportion formula considering a confidence level of 95%, the population size of mothers was 3829 during the survey period; the absolute precision of 5% and hypothesized proportion of small size at birth in the community was 50%. The sample size was calculated by the Open Epi, Version 3.03, open source calculator. Having considered a design effect of 3, the final sample size was 1048. Six Kebeles were selected from two sub-cities. Kebeles were further sub-classified in clusters. All sample sizes were allocated based on Probability Proportional to Size (PPS) of the population in each selected Kebele. Then, each household was selected using Systematic Random Sampling (SRS) technique.
2.5. Data Collection Procedure and Tools
Mothers with their child were identified using systematic random sampling technique. Mothers were interviewed about socio-demographic variables, child profile, the exposure related questions, fuel use, stove type, housing characteristics, type of kitchen, cooking practice, smoking history, occupational history, and medical history. The questionnaire was adopted from WHO and Ethiopian Demographic Health Survey (EDHS) household survey questions [22]. The child size at birth was determined based on mother’s report and labeled as “small” or “large or larger than the average.” Similar procedures have been applied in the literature [7, 20, 23-25]”.
Variables: The dependent variable was child size at birth and independent variables were socio-demographic status; housing and kitchen characteristics; household cooking fuels and stoves and maternal and child health questions.
Mother exposure level was assessed by five variables, namely, level of house ventilation, cooking place, fuel type, stove type and time spent in cooking variables (Table 1).
| HAP Exposure Index | HAP Exposure Assessment Variables |
|---|---|
| High exposure practices (H) | a) Living in low ventilated houses* b) Cooking inside the living house c) Using biomass fuel for cooking d) Using an open/traditional type of stoves and e) Spent three or more hours in cooking |
| Moderate exposure practices (M) | a) Living in medium ventilated houses* b) Cooking in a separate house/kitchen c) Using charcoal fuel for cooking d) Using an improved type of stoves and e) Spent only two hours on cooking |
| Low exposure practices (L) | a) Living in high ventilated houses* b) Cooking outside the living house c) Using electric fuel for cooking d) Using electric stoves and e) Spent one hour or less in cooking |
| Highly exposed mothers | • If exposed to a combination of at least three high exposure practices in any order (≥3H); or • If exposed to a combination two high, two moderate and one low exposure practice variables (2H+2M+1L) |
| Moderately exposed mothers | • If exposed to a combination of at least three moderate exposure practices in any order (≥3M); or • If exposed to a combination two high, two low and one moderate exposure practice variables (2H+2L+1M) |
| Lowest exposed mothers | • If exposed to a combination of at least three low exposure practices in any order (≥3L); or • If exposed to a combined two moderate, two low and one high exposure practice variables (2M+2L+1H) |
2.6. Data Quality Assurance
Ten data collectors (environmental health, nurse, and public health profession) and two supervisors (Masters in Public Health) were engaged. A three days training was provided. To assure the quality of the data, high emphasis was given to designing data collection instrument. Prior to the data collection, a pre-test was conduted on 5% of the total sample size in non- selected Kebele. Regular supervision and follow-up were made by supervisors and the principal investigator. The filled questionnaire was collected and signed by supervisors after being checked for any missing value, correctness and consistency.
2.7. Data Management and Analysis
Cleaned and a coded questionnaire was entered into computer software program for analysis, in Epi Data version 3.1 and SPSS 21. Frequencies were run for checking of outliers and to clean the data. Crude odds ratio with 95% confidence intervals and Chi-squared tests were calculated. Multi-collinearity was checked using cutoff point Variance Inflation Factor (VIF) < 10 and tolerance test > 0.1. Bivariate and multivariate logistic regression analyses were conducted using enter method. The cut-off point for P-value was <0.05 for both bivariate and multivariate model.
2.8. Ethical Consideration
Permission to undertake the study was taken from Addis Ababa University, College of health sciences, Institutional Review Board Office. Mothers were consented before conducting the interview. For the consent, one-page subject information sheet and informed consent letter were attached to each questionnaire and it explained that participation was voluntary, confidential, and no risk or harm, every cultural value, norms and any demanding privacy were respected. The right of the respondent to withdraw from the interview or not to participate was respected. Identification of an informant was possible only through specific identification numbers.
3. RESULTS
3.1. Socio-Demographic Characteristics of Respondents
A total of 1042 biological mothers were involved in the study. More than half, (59.9%) of the mothers' age were between 25-34 years with a mean of age 26.39 years with standard deviation of 4.79 years. Regarding educational status, 305 (29.3%) of mothers and 274 (26.3) of fathers were engaged in primary level education. Seventy-three percent of the households had a family of 5 or less. Households had access to an improved water source in their yard, 985 (94%), and pit latrine 885 (84.9%) (Table 2).
| Sociodemographic characteristics of mothers | Child size at birth, n (%) | Total, n(%) | |||
|---|---|---|---|---|---|
| Small | Medium | Large | |||
| Age of Mother | 15-24 years | 60 (18.5) | 214 (66.0) | 50 (15.4) | 324 (31.1) |
| 25-34 years | 93 (15.0) | 430 (69.2) | 98 (15.8) | 621 (59.6) | |
| 35-49 years | 17 (17.5) | 71 (73.2) | 9 (9.3) | 97 (9.3) | |
| Mother Educational level | No education | 61 (21.0) | 198 (68.3) | 31 (107) | 290 (27.8) |
| Primary level | 57 (18.7) | 204 (66.9) | 44 (14.4) | 305 (29.3) | |
| Secondary level | 21 (9.1) | 168 (73.0) | 41 (17.8) | 230 (22.1) | |
| Higher level | 31 (14.3) | 145 (66.8) | 41 (18.9) | 217 (20.8) | |
| Father Educational level | No education | 41 (20.7) | 137 (69.2) | 20 (10.1) | 198 (19.0) |
| Primary level | 56 (20.4) | 183 (66.8) | 35 (12.8) | 274 (26.3) | |
| Secondary level | 39 (13.4) | 203 (69.5) | 50 (17.1) | 292 (28.0) | |
| Higher level | 34 (12.2) | 192 (69.1) | 52 (18.7) | 278 (26.7) | |
| Family size | ≤5 Families | 122 (15.9) | 533 (69.7) | 110 (14.4) | 765 (73.4) |
| >5 Families | 48 (17.3) | 182 (65.7) | 47 (17.0) | 277 (26.6) | |
| Wealth status | Reach | 55 (14.6) | 245 (64.8) | 78 (20.6) | 378 (36.3) |
| Middle | 88 (16.7) | 373 (70.9) | 65 (12.4) | 526 (50.5) | |
| Poor | 27 (19.6) | 97 (70.3) | 14 (10.1) | 138 (13.2) | |
3.2. Mother and Child Health Descriptions
Children were relatively equally distributed by age. The mean age of the children was 23.74 months with Standard Deviation (SD) of 14.93. Males accounted to be 567 (54.4%) of the total children. The majority of children 1011 (97%) were born after completed ANC follow up and only 91 (8.7%) children had been delivered at home, while the rest, 875 (84%) had been delivered at government health facilities. Half of the children 518 (49.7%) were first birth to their mothers, and 583 (56.0%) of the children had a birth order of 2 years or less (Table 3).
| Mother and child-related variables | Child size at birth, n (%) | Total, n (%) | ||
|---|---|---|---|---|
| Small | Medium or large | |||
| Sex of the child | Female | 103 (21.7) | 372 (78.3) | 475 (45.6) |
| Male | 67 (11.8) | 500 (88.2) | 567 (54.4) | |
| Full-term birth | Yes | 152(15.0) | 864(85.0) | 1016 (97.5) |
| No | 18 (69.2) | 8 (30.8) | 26 (2.5) | |
| ANC follow up | Yes | 159 (15.7) | 852 (84.3) | 1011 (97.0) |
| No | 11 (35.5) | 20 (64.5) | 31(3.0) | |
| Place of delivery | Home delivery | 25 (27.5) | 66 (72.5) | 91 (8.7) |
| Gov’t health facility | 135 (15.4) | 740 (84.6) | 875(84.0) | |
| Private health facility | 10 (13.2) | 66 (86.8) | 76 (7.3) | |
| Birth order | First child | 84 (16.2) | 434 (83.8) | 518 (49.7) |
| Second child | 50 (18.1) | 227 (81.9) | 277 (26.6) | |
| Third plus child | 36 (14.6) | 211 (85.4) | 247 (23.7) | |
| Birth spacing | ≤2 years | 105 (18.0) | 478 (82.0) | 583 (56.0) |
| >2 years | 65 (14.2) | 394 (85.8) | 459 (44.0) | |
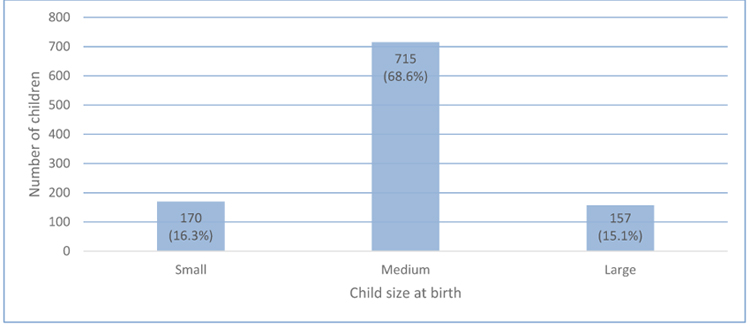
3.3. The Magnitude of Child Size at Birth
According to mother’s report of child size at birth, the number of small sizes at birth in the study area was 170, which accounted to 16.3% (95% CI 14.2%-18.6%), while 872 (83.7%) had medium and above size (more explicitly, medium size was 715 (68.6%) and larger than the medium size was 157 (15.1%) (Fig. 1).
3.4. House and kitchen characteristics
About 322 (30.9%), 504 (48.4%) and 431 (41.4%) of children lived in the house of one room, one door, and one window, respectively, while 960 (92.1%) of the houses have at least one window. About 667 (64%) of the households used a kitchen separated from the main house and 311 (29.8%) of households used kitchen inside the living house. Regarding house ventilation, about 418 (40.1%) of the households had poor ventilation, 346 (33.2%) of the house had moderate ventilation, and but only 278 (26.7%) of the house had good ventilation (Table 4).
| House and kitchen characteristics | Child size at birth, n (%) | Total, n (%) | ||
|---|---|---|---|---|
| Small | Medium or large | |||
| Number of rooms | 1 room | 69 (21.4) | 253 (78.6) | 322 (30.9) |
| 2 rooms | 61 (14.3) | 366 (85.7) | 427 (41.0) | |
| ≥3 rooms | 40 (13.7) | 253 (86.3) | 293 (28.1) | |
| Number of doors in the house | 1 door | 97 (19.2) | 407 (80.8) | 504 (48.4) |
| 2 doors | 48 (13.0) | 322 (87) | 370 (35.5) | |
| 3+ doors | 25 (2.4) | 143 (85.1) | 168 (16.1) | |
| Number of windows in the house | No window | 23 (34.8) | 43 (65.2) | 66 (6.3) |
| 1 window | 77 (17.9) | 354 (82.1) | 431 (41.4) | |
| 2 windows | 54 (14.5) | 319 (85.5) | 373 (35.8) | |
| 3+ windows | 16 (9.3) | 156 (90.7) | 172 (16.5) | |
| House ventilation | Poor | 85 (20.3) | 333 (79.7) | 418 (40.1) |
| Moderate | 51 (14.7) | 295 (85.3) | 346 (33.2) | |
| Good | 34 (12.2%) | 244 (87.8) | 278 (26.7) | |
| Cooking place | Inside the house | 99 (31.8) | 212 (68.2) | 311 (29.8) |
| Separate house | 62 (9.3) | 605 (90.7) | 667 (64) | |
| Outdoor space | 9 (14.1) | 55 (85.9) | 64 (6.1) | |
3.5. Fuel Types, Ptove Types, and Home Practice
Majority of the households, 877 (84.1%) of children were living in households that used polluting fuel for cooking (charcoal 60.7% and biomass fuel 23.4%), but only 165 (15.8%) of the households used clean fuel energy (i.e. electricity, LPG, natural gas and biogas).
The most common type of stoves used were open-fire stoves, 764 (73.3%). The time spent on cooking by the households was calculated in hours per day, and therefore, 290 (27.8%) of them spent three hours or more, while the rest were less than two hours. The mean time spent on cooking was 2.24±1.06 hours. More than two-thirds 706 (67.8%) of the households used incense, but only 19 (1.8%) of the households have at least one of the family member as cigarette smoker (Table 5).
| Fuel and stove types | Child size at birth, n (%) | Total, n (%) | ||
|---|---|---|---|---|
| Small | Medium or large | |||
| Fuel for cooking | Biomass fuel | 49 (20.1) | 195 (79.9) | 244 (23.4) |
| Charcoal | 104 (16.3) | 529 (83.6) | 633 (60.7) | |
| Electricity | 17 (10.3) | 148 (89.7) | 165 (15.8) | |
| Type of stove | Open-fire | 142 (18.6) | 622 (81.4) | 764 (73.3) |
| Improved | 11 (7.2) | 142 (92.8) | 153 (14.7) | |
| Electricity | 17 (13.6) | 108 (86.4) | 125 (12) | |
| Time spent in cooking per day | 1 hour | 23 (9.2) | 228 (90.8) | 251 (24.1) |
| 2 hours | 81 (16.2) | 420 (83.8) | 501 (48.1) | |
| ≥3 hours | 66 (22.8) | 224 (77.2) | 290 (27.8)) | |
| HAP Exposure index of mothers | High | 75 (33.9) | 146 (14.0) | 221 (21.2) |
| Moderate | 67 (13.9) | 415 (86.1) | 482 (46.3) | |
| Low | 28 (8.3) | 311 (91.7) | 339 (32.5) | |
| Smoke incense frequently | Yes | 132 (18.7) | 574 (81.3) | 706 (67.8) |
| No | 38 (11.3) | 298 (88.7) | 336 (32.2) | |
| Family member smokes a cigarette | Yes | 3 (15.8) | 16 (84.2) | 19 (1.8) |
| No | 167 (16.3) | 856 (83.7) | 1023 (98.2) | |
3.6. Bivariate Analysis
Wealth status, childbirth order, and child spacing didn't show any significant associations in the bivariate analysis, but mother and father education; sex of the child, number of windows, level of house ventilation; cooking place, type of fuels and stoves, time spent on cooking and HAP exposure of mothers showed significant associations with child size at birth in the bivariate analysis. While, only mother education, child sex, number of windows, cooking place, type of fuels and stoves and time spent on cooking showed significant associations in a multivariable analysis.
Children who were born in households who used biomass fuel as the main source of fuel for cooking [AOR, 3.83, 95% CI, 1.95-15.35] had more likely to be small size at birth as compared to children who were born in households who used electricity. Cooking place inside the house [AOR, 2.27, 95% CI 1.88-5.88] were more likely to be leading to small size at birth as compared to a child from a mother who had a cooking place outside the house. Children from houses of no window were of small size at birth than children born in houses having three or more windows [AOR, 4.79, 95%CI, 1.56-14.69] (Table 6).
| Predictor variables | Child size at birth | COR (95% CI) | AOR (95% CI) | ||
|---|---|---|---|---|---|
| Small | Medium or Large | ||||
| Mother education | No education | 61 | 229 | Reference | Reference |
| Primary level | 57 | 248 | 0.86 (0.58-1.29) | 1.06 (0.65-1.72) | |
| Secondary level | 21 | 209 | 0.38 (0.22-0.64)* | 0.52 (0.28-0.97)* | |
| Higher level | 31 | 186 | 0.63 (0.39-1.01) | 1.22 (0.65-2.29) | |
| Father education | No education | 41 | 157 | 1.87 (1.14-3.08)* | 1.31 (0.69-2.50) |
| Primary level | 56 | 218 | 1.84 (1.16-2.93)* | 1.78 (1.00-3.18) | |
| Secondary level | 39 | 253 | 1.10 (0.68-1.81) | 1.14 (0.65-2.01) | |
| Higher level | 34 | 244 | Reference | Reference | |
| Wealth status | Reach | 55 | 323 | 0.70 (0.42-1.16) | --- |
| Middle | 88 | 438 | 0.83 (0.51-1.33) | --- | |
| Poor | 27 | 111 | Reference | --- | |
| Sex of a child | Female | 103 | 372 | 2.07 (1.48-2.89)* | 2.27 (1.58-3.27)* |
| Male | 67 | 500 | Reference | 1.00 | |
| Birth order | First child | 84 | 434 | 1.13 (0.74-1.73) | --- |
| Second child | 50 | 227 | 1.29 (0.81-2.06) | --- | |
| Third plus child | 36 | 211 | Reference | --- | |
| Birth spacing | ≤2 years | 105 | 478 | 1.33 (0.95-1.87) | --- |
| >2 years | 65 | 394 | Reference | --- | |
| Number of windows in the house | No window | 23 | 43 | 5.22 (2.53-10.73)* | 4.79 (1.56-14.69)* |
| 1 window | 77 | 354 | 2.12 (1.20-3.75)* | 2.12 (0.82-5.44) | |
| 2 windows | 54 | 319 | 1.65 (0.92-2.98) | 1.83 (0.84-4.01) | |
| ≥3 windows | 16 | 156 | Reference | Reference | |
| House ventilation level | Poor | 85 | 333 | 1.83 (1.19-2.82)* | 1.37 (0.67-2.82) |
| Moderate | 51 | 295 | 1.24 (0.78-1.98) | 1.03 (0.58-1.83) | |
| Good | 34 | 244 | Reference | Reference | |
| Cooking Place (kitchen arrangement) | Inside the house | 38 | 255 | 2.85 (1.36-6.01)* | 2.27 (1.88-5.88)* |
| Separate house | 115 | 562 | 0.63 (0.30-1.33) | 0.65 (0.28-1.51) | |
| Outdoor space | 17 | 55 | Reference | Reference | |
| Fuel types for cooking | Biomass fuel | 49 | 195 | 2.19 (1.21-3.95)* | 3.83 (1.95-15.35)* |
| Charcoal | 104 | 529 | 1.71 (0.99-2.95) | 3.47 (0.99-12.24) | |
| Electricity | 17 | 148 | Reference | Reference | |
| Type of stoves | Open-fire | 136 | 735 | Reference | Reference |
| Improved | 22 | 65 | 0.34 (0.18-0.64)* | 0.31 (0.14-0.67)* | |
| Electricity | 12 | 72 | 0.69 (0.40-1.19) | 3.12 (0.79-12.32) | |
| Time spent in cooking per day | ≥3 hours | 62 | 261 | 2.92 (1.76-4.86)* | 2.45 (1.16-5.21)* |
| 2 hours | 78 | 398 | 1.91 (1.17-3.12)* | 1.53 (0.86-2.70) | |
| 1 hour | 30 | 213 | Reference | Reference | |
| HAP exposure status of mothers | High | 75 | 146 | 5.71 (3.54-9.19)* | 1.62 (0.46-5.77) |
| Moderate | 67 | 415 | 1.79 (1.13-2.86)* | 1.37 (0.58-3.23) | |
| Low | 28 | 311 | Reference | Reference | |
4. DISCUSSION
Child size at birth is an indicator of multifaceted public health problem including poor health service and lack of awareness of mothers. Small size at birth is a national concern in Ethiopia. The prevalence of small size at birth in this study area was 16.3%. The result was more or less similar to the report of EDHS 2016, which accounted to 20.1% in urban residence of Ethiopia [20], Nigeria, 20.5% [15], Bangladesh, 17.7% [19], India, 20% [16] and Assam (India), 21.8% [17]. But it was by far smaller than the Pakistan being 60.5% [18]. Less significant differences with EDHS figure were due to the fact that EDHS data is a national survey which included all districts of the country. In contrary, large discrepancies were observed in a study conducted in Pakistan, which could be due to the socioeconomic and cultural differences among these countries.
Type of fuel used for cooking had been explored as one of the main determinants of small weight in most studies. Similarly, the current study revealed that using biomass fuel as the main source of fuel for cooking was important predictors of small size at birth as compared to electric stove users. This study consistently agrees with the study conducted in India in conclusion that solid fuel in cooking in household was a higher risk of low birth weight [19, 26]; similarly in Pakistan, exposure to biomass fuel during pregnancy was significantly associated with low birth weight of a child [18, 25], and the type of cooking fuel was an explanatory variable to child size at birth [7], but the type of fuel used didn't show any significant association with birth weight in a study [23, 24], probably the sample size in the study was too small as compared to other mentioned in the literature.
Children who were born from mothers of improved stove users were less likely to be small in size at birth as compared to children born from mothers who were using an open-fire type of stoves. Most improved stoves were designed in the way to minimize fuel and to facilitate combustion to reduce particulate matter emissions. Therefore, mothers who used this improved stove could be prevented from high exposure of HAP.
Our study suggested that most of the households were cooking in the separate kitchen, which is a different report from a study of Devkota et al., in which more than 88% of the households were cooking in indoor kitchens [23]]. The possible explanation could be the participants were registered pregnant mothers who were following antenatal care in their small village. Cooking place inside the house was a risk factor for a size of a child at birth as compared to the cooking place at outdoor spaces. Our study is consistent with the study of Khan et al. [19], where children born to mothers of cooking inside the house were the most likely to report as very small size birth weight. This was a fact that those who were cooking inside the house could have more exposure to biomass and charcoal smoke in a poorly ventilated house. But in a study conducted by Haider et al. [26], the cooking place was not significantly associated with child size at birth.
Most studies indicated that women and young children spend much time in close proximity to the fire and in a cooking environment. Having spent much time leads to the higher risk of exposure to harmful chemical pollutants. This is also a proxy for higher exposure measurement. In this study, mothers spent a mean and standard deviation of 2.24 (±1.1) hours per day in cooking. This time is smaller than reported in the study of Clark et al., with a mean of 6.5±4.3 hours per day [10]. However, the time spent on cooking seem to be short in the current study, the risk of spending much time on cooking per day showed a significant association with reduced child size at birth as compared to a child born to mother who spent one hour or less on cooking per day. Biomass smoke exposure is the highest among women and children, as these groups generally spend more time in home and in areas designated for cooking [27]. As more time spent on cooking, exposure to smoke and particulate matter increases, therefore the risk of a small-sized child at birth is expected.
The number of windows is a powerful indicator of house and kitchen ventilation. In the current study, children in the houses with no windows showed a significant difference in child size at birth. Children born in the households with no window were 4.79 times more likely to be small-sized at birth as compared to their counters born in the houses having three or more windows. This is the fact that increased number of windows can facilitate house ventilation significantly [10]. As the number of windows in a house increases, the level of ventilation of a house greatly improves, hence the risk of HAP exposure radically declines.
Mothers who had secondary level of education as compared to non-educated mothers and had a male child, were found to have less risk of having a small size child at birth. Our study result is consistent with the study of Haider et al. [26]. Those mothers who were attending some level of education could have information on the predictors of small child size at birth and so as to take measures as early as possible. Meanwhile, a female child is smaller than the male child at birth in most studies [24, 26].
This study was conducted on large sample size which could help to make a plausible conclusion. Another important strength of our study is that participant mothers were only biological mothers who could provide a reliable response to their child. However, the limitation of this study is that the child size at birth was estimated based on the mother’s response, which is subjective and leads to overestimation of a large-sized child at birth, because most mothers want to have a larger size child at birth and may intend to respond to large size child at birth. Mother’s estimate was not ascertained with actual weight measurement, which could lead to social desirability bias and personal judgments of mother’s. Therefore, interpretation of this finding should be viewed with caution.
CONCLUSION
The present study revealed that small child size at birth is still a concern in Ethiopia. Using biomass fuels for cooking, cooking inside the house, houses without windows, three or more hours spent on cooking, using open-fire stoves, being a female child and lower level of mother’s education were risk factors of a small-sized child at birth. Therefore, we commend to local government, non-government, private sectors and all concerned stakeholders to provide accessible and affordable clean fuels and improved stoves; to design health initiatives and promote a separate kitchen and housing design so as to incorporate a sufficient number of windows in the house in the long-run. Findings of this study should be ascertained by actual measurements of childbirth weight in the future.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Permission to undertake the study was taken from Addis Ababa University, College of health sciences, Institutional Review Board Office.
HUMAN AND ANIMAL RIGHTS
No animals/humans were used for studies that are the basis of this review.
CONSENT FOR PUBLICATION
Mothers were consented before conducting the interview. For the consent, one-page subject information sheet and informed consent letter were attached to each questionnaire and it explained that participation was voluntary, confidential, and no risk or harm, every cultural value, norms and any demanding privacy were respected.
AUTHORS’ CONTRIBUTIONS
All authors involved in study protocol design and development. AA involved in data collection. AA and AW were involved in protocol design and data analysis. AA prepared the manuscript and edited by AK. AK and AW supervised and monitored the protocol. All authors read and approved the final manuscript.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGMENTS
The authors thank Addis Ababa University and Wolaita Sodo university for financial support to this study. We are also very grateful for the Wolaita Sodo town health office and Wolaita Sodo town administration for their cooperation. We all thank participants’, data collectors and supervisors of the study who devoted their time and used their effort to the success of this study meaningfully.

