All published articles of this journal are available on ScienceDirect.

Reproductive Health Choices Among Adolescents in Secondary Schools: A Case Study of Selected Schools in Limpopo, South Africa
Abstract
Objectives:
This study was conducted to determine the knowledge, opinions and practices of female adolescents in selected secondary schools in Limpopo Province of South Africa about reproductive health issues and assess the level of parental involvement in their choices.
Materials and methods:
A quantitative, exploratory, survey design was adopted. A total of 512 learners from grades 8 (first year of secondary school) and 12 (final year) were conveniently sampled from 24 randomly selected secondary schools in Limpopo Province. Data was collected with a structured, self-administered questionnaire and analysis was done using the Statistical Package for Social Sciences (SPSS) version 20.0.
Results:
Sixteen (3.9%) of the learners attained menarche at or before the early age of 8 years and 102 (29.3%) experienced sexual debut before age 14 years. More than half of grade 12 (n =84, 52.5%) and 49 (14%) of grade 8 learners were sexually active and 80% (n = 444, 86.7%) of them were unaware of contraceptives when engaging in sexual intercourse for the first time. Only 116 (22.7%) of the respondents admitted to having knowledge about contraceptives before engaging in sex for the first time and more than a third (n = 172, 33.6%) have been pregnant at least once before the study was conducted. Parental involvement in Sexual and Reproductive Health (SRH) education was found to be low and many obtained the little information they have mainly through friends.
Conclusion:
Many adolescents are lacking in vital information regarding their SRH and some hold wrong opinions about contraception. Parents are advised to initiate and sustain discussions regarding SRH with their children to help them make informed reproductive health choices.
1. INTRODUCTION
The World Health Organization defines an adolescent as a young person aged between 10 and 19 years [1]. The stage of adolescence is the transitional stage between childhood and adulthood and it is a period of rapid physical, emotional and psychological changes which is also associated with the decisions to engage in risky behaviors including sexual activities and consumption of harmful chemical substances [2]. Adolescents often engage in these behaviors to “try them out” or “experiment with them” without an adequate consideration of what the consequences may be. This exposes them to adverse reproductive health consequences including sexually transmitted infections, unwanted pregnancies, unsafe abortions and maternal health complications [3]. Many adolescents are facing different problems as a result of wrong choices they have made regarding their reproductive health and the females are usually more affected than their male counterparts [4].
Approximately 90% of global adolescents’ population are found in the developing countries as compared with developed countries due to a higher fertility rate in the former [5]. However, in many developing countries, access to reproductive health services is largely fragmented and inadequate [2]. In 2016, it was reported that an estimated 21 million adolescent pregnancies occurred in the developing countries with almost half of the pregnancies unplanned and unwanted [6]. About half of pregnancies in this age group usually end up in induced abortion resulting in approximately 17,000 deaths of young women from complications arising from the pregnancies or childbirth [6]. Incidences of teenage pregnancies are higher in Africa (130/1,000 girls) where sexual issues are not openly discussed as compared with Asia (58/1,000 girls) and Europe (29/1,000 girls) where there are more open discussions regarding reproductive health issues [7].
There is a prevalence of early and unprotected sexual activities as well as misconceptions about contraception and sexually transmitted diseases among adolescents in the developing countries, especially in the rural areas where discussions about sexual activities are generally considered as a taboo [8, 9]. Yet, the lack of sex education aggravated by a perceived or real peer pressure to engage in sexual activities has been identified as a very important factor in the increase in the rate of teenage pregnancies [9, 10].
There is a growing concern to address adolescent reproductive health problems worldwide and many programs targeting reproductive health among adolescents have expanded their focus to involve more stakeholders including parents, guardians, teachers and the community. Parental involvement is much desired because their strong and supportive involvement is an essential factor in the emotional and social development of their children [3]. A review of many studies in sub-Saharan Africa showed that the contribution of parents to their adolescents’ reproductive health knowledge is minimal. While many parents agreed that sex education should be given to their children in the schools, most of them never discuss these issues with their children because “such a discussion is forbidden by their culture”, others refrain from such discussions because they feared it may increase their children’s quest for sexual activities and the few parents who dared to hold discussions about reproductive health issues with their adolescents were usually selective, placing an emphasis on abstinence, sexually transmitted infections and unwanted pregnancies while avoiding the issue of contraceptive use. Most parents who give this information will only do so if they were asked by their children, rather than initiate the discussion [11]. In a study among Indian adolescents, mothers were reported to be the major educators of their female adolescents on the issues of menstruation only, while information regarding sexual activities, contraception and abortion were mainly obtained from friends [12].
In 2007, a study conducted in four out of the nine provinces of South Africa showed that 19.4% of females between the ages of 12 - 19 years have had at least one pregnancy; majority of which were unwanted [13]. The same study showed that more than half (55.5%) of the adolescents got pregnant for the first time due to a lack of understanding of how pregnancy happens and the risks involved in unprotected sex; 74.1% of the respondents indicated that their pregnancies were unwanted; only 19% claimed to have got pregnant in order to prove their maturity or reveal their identity as women [13].
In the Youth Risk Behaviour survey conducted in 2008 among South African adolescents, it was reported that 30% of their female subjects reported ever having sex while 24% have been pregnant before and about 15% of the sexually active female learners were not using contraceptives [14, 15]. A progressive decline in the use of condoms (the most widely available contraceptive device in South Africa) was noticed among adolescents according to two nationally representative surveys carried out in South Africa in 2008 and 2012. The studies reported that the rate of use of condoms had reduced from 66.5% to 49.8% among females [16]. Lack of knowledge, perceived adverse side effects and difficulty with access have been identified as reasons among others for a reduced use of contraceptives [17].
Many initiatives have been developed by the South African government aimed at addressing the sexual health issues of adolescents including national campaigns and policies on Health education and reproductive health issues including sexually transmitted infections, especially HIV. Many non-governmental organizations have also made attempts to assist the government in this regard [16]. However, the implementation and efficacy of government policies regarding the youth sexual and reproductive health have faced many challenges and the interventions seem not to have made a significant impact on the adolescents. Three years after the loveLife programme was initiated, a baseline study in all South African provinces revealed no significant differences in Sexually Transmitted Infections (STIs) prevalence between youth living in communities with loveLife youth centres and National Adolescent Friendly Initiative (NAFCI) interventions compared with those in communities with no interventions [18].
Also, a qualitative study on the NAFCI in the Greater Tzaneen subdistrict in Limpopo Province showed that even though some adolescents used the NAFCI services at the clinic, especially contraception, STI and pregnancy services, yet, pregnancy and STI rates in the area did not decrease and HIV Counselling and Testing (HCT) services were under-utilised [19, 20]. An increasing number of adolescent pregnancies in South Africa has also been reported despite the government’s effort in providing contraceptives for all [21].
With the stage of adolescence experiencing a rapid change in shape evidenced by a decreasing age of onset of puberty, Sawyer, et al. [22] have proposed that a greater attention must be placed on this age group for many public health goals to be achieved. Other studies have shown that mothers are very critical in the decision making of their daughters as far as sexuality is concerned [23, 24] and that adolescents who discuss sexual issues with their parents tend to be less sexually active and are more likely to use more appropriate contraceptives [3]. An open communication on sexual issues at home coupled with effective sex education in school are protective factors in the prevention of adolescent pregnancy [25].
Many previous studies conducted in South Africa regarding reproductive health issues among youths have been focused on urban centers and usually involved the youth/adolescents in the community rather than in schools. This study was conducted to determine the knowledge, opinions and practices of the female adolescents in selected rural secondary schools in Limpopo Province of South Africa about important reproductive health issues and assess the level of parental involvement on the learners’ choices. The learners selected for this study were drawn from grade 8 (first year of secondary school, with learners usually between 13 - 15 years of age) and grade 12 (final year of secondary school, with learners usually between 17 - 19 years of age).
2. MATERIALS AND METHODS
2.1. The Study Design and Setting
This study was conducted at twenty-four randomly sampled secondary schools in Limpopo province of South Africa between March and May 2014, using a quantitative, exploratory, descriptive, and survey research design.
2.2. Population and Sampling
A total of 512 female learners were conveniently sampled for this study from the randomly selected secondary schools. Learners were purposively selected from grades 8 and 12, being the first and the last grades in the secondary schools in South Africa. All the female learners from grades 8 and 12 who were present in the school on the day the researcher and her assistants visited the school were involved in the study, except those who did not volunteer to participate. Learners from grade 8 constituted 352 (68.8%) of the sample while 160 (31.2%) were grade 12 learners.
2.3. Data Collection and Measurement
A structured questionnaire was employed for data collection in this study. It was designed to obtain information concerning the common reproductive health issues of adolescents in relation to their knowledge, practices, opinions and parental involvement. The reproductive health issues of concern include sexual exposures and education, teenage pregnancy and parenting, knowledge and use of contraceptives, primary health centers and legal abortions. The questionnaires were distributed to the learners to complete after having given their consents by signing on the consent forms. Explanations were given to those who indicated a need for clarity on some of the questions asked and the completed questionnaires were collected immediately.
2.4. Statistical Analysis
Data obtained were analyzed with Statistical Package for the Social Sciences (SPSS), version 20.0. Descriptive statistics were performed on the data and the results were summarized using frequency distribution tables and figures. Chi-square tests were performed to identify the relationships between the responses of grades 8 and 12 learners. A p-value of less than 0.05 was set to be statistically significant.
3. ETHICS AND CONSENT
Ethical approval was obtained from the University of Venda Research and Publication Committee. The permission to conduct the study was obtained from the Provincial Department of Education, Strata South Africa and Democratic Nursing Organization of South Africa (DENOSA). A detailed explanation of the purpose and method of the study was given to each learner and informed consent was obtained from all the learners before they were given the questionnaires to complete. Other ethical issues like voluntary participation, the right to withdraw, confidentiality, anonymity and minimization of risk of harm to participants were also strictly adhered to.
4. RESULTS AND DISCUSSION
4.1. Sample Characteristics
All the respondents in this study were within the adolescent age category. The term “teenager” also applies to them and will be used for them at some relevant points in the discussion. Most of the respondents were rural dwellers with varying religious denominations though most of them belonged to the Christian religion. Although 418 (89.3%) of them were never married, as expected, interestingly, 24 (5.1%) and 10 (2.1%) of them admitted being married and divorced respectively. This is probably because the marriage of young females is practiced by some African cultures and some religions like Islam to which some of the respondents might belong to (captioned under “others” in the “religious denomination column in Table 1. Overall, 194 (37.9%) of the study adolescents lived with both parents while 104 (20.3%) and 182 (35.5%) live with father or with mother, respectively (Table 1).
| Characteristics | Grade 8 | Grade 12 | Total | |||
|---|---|---|---|---|---|---|
| Age | Freq. | % | Freq. | % | Freq. | % |
| ˂ 13 years | 316 | 89.8 | 0 | 0 | 316 | 61.8 |
| 13-18 years | 36 | 10.2 | 159 | 100 | 195 | 38.2 |
| Total | 352 | 100 | 159 | 100 | 511 | 100 |
| Residence | ||||||
| Urban | 40 | 11.5 | 12 | 7.5 | 52 | 10.2 |
| Rural | 290 | 83.3 | 124 | 77.5 | 414 | 81.5 |
| City | 10 | 2.9 | 6 | 3.8 | 16 | 3.1 |
| Township | 8 | 2.3 | 18 | 11.3 | 26 | 5.1 |
| Total | 348 | 100 | 160 | 100 | 508 | 100 |
| Religious denomination | ||||||
| African religion | 119 | 35.6 | 22 | 14.1 | 141 | 28.8 |
| Catholic | 10 | 3.0 | 26 | 16.7 | 36 | 7.3 |
| Anglican/Protestant | 8 | 2.4 | 6 | 3.8 | 14 | 2.9 |
| ZCC | 76 | 22.8 | 48 | 30.8 | 124 | 25.3 |
| Apostolic | 108 | 32.3 | 28 | 17.9 | 136 | 27.8 |
| Others | 13 | 3.9 | 26 | 16.7 | 39 | 8.0 |
| Total | 334 | 100 | 156 | 100 | 490 | 100 |
| Marital status | ||||||
| Never married | 274 | 85.6 | 144 | 97.3 | 418 | 89.3 |
| married | 20 | 6.3 | 4 | 2.7 | 24 | 5.1 |
| divorced | 10 | 3.1 | 0 | 0 | 10 | 2.1 |
| Others | 16 | 5.0 | 0 | 0 | 16 | 3.4 |
| Total | 320 | 100 | 148 | 100 | 468 | 100 |
| Who are you living with | ||||||
| Father | ||||||
| Yes | 82 | 23.3 | 22 | 13.8 | 104 | 20.3 |
| No | 270 | 76.7 | 138 | 86.3 | 408 | 79.7 |
| Total | 352 | 100 | 160 | 100 | 512 | 100 |
| Mother | ||||||
| Yes | 140 | 39.8 | 42 | 26.3 | 182 | 35.5 |
| No | 212 | 60.2 | 118 | 73.8 | 330 | 64.5 |
| Total | 352 | 100 | 160 | 100 | 512 | 100 |
| Both Parents | ||||||
| Yes | 108 | 30.7 | 86 | 53.8 | 194 | 37.9 |
| No | 244 | 69.3 | 74 | 46.3 | 318 | 62.1 |
| Total | 352 | 100 | 160 | 100 | 512 | 100 |
| Grandparents | ||||||
| Yes | 32 | 9.1 | 34 | 21.3 | 66 | 12.9 |
| No | 320 | 90.9 | 126 | 78.8 | 446 | 87.1 |
| Total | 352 | 100 | 160 | 100 | 512 | 100 |
4.2. Reproductive Health Issues
4.2.1. Sexual Exposure
Sixteen (3.9%) of the respondents attained menarche at age 8 years or younger and 210, (51.2%) attained menarche between age 13 and 14 years indicating early exposure to the risk and consequences of unsafe sexual practices such as unwanted pregnancies and Sexually Transmitted Infections (STIs). This finding supports the fact that the age of onset of puberty is reducing, making the number of adolescents to increase rapidly [22]. An early sexual debut is a call for a deliberate and early onset of sex education for adolescents.
A total of 49 (13.9%) respondents from grade 8 and 90 (56.3%) from grade 12 admitted they have ever engaged in sexual intercourse, while 27 (7.7%) and 6 (3.7%) from grades 8 and 12 respectively did not answer the question. At least, 102 (29.3%) of them had an early sexual debut (sexual intercourse experience at or before age 14), while 30 (8.6%) learners reportedly had their first sexual intercourse experience between the age of 14 and 15 years.
Though 26 (8.2%) learners claimed that their first sexual intercourse was as a result of rape, 44 (13.9%) indicated that they planned it with their partners, 40 (12.7%) said they felt like doing it, 24 (7.6%) engaged in it out of curiosity, while 74 (23.4%) claimed “it just happened”. However, after the first experience, many of them continued in this risky behavior to the extent that as many as 82 (26.2%) were practicing it as frequently as two or more times every week. This shows that an appreciable number of these young learners are engaging in sex and affirms the report of the previous studies among the youth in South Africa regarding learners being sexually active [14, 15].
4.2.2. Knowledge about Contraception and Consequence of Sexual Intercourse
Despite the number of the learners who indicated that they were sexually active, 248 (74.3%) respondents did not know that it is possible to get pregnant with the first sexual experience and 272 (80%) did not know about contraception while engaging in their first sexual intercourse. This shows a paucity of information about teenage pregnancy and contraception among the learners [17]. About half of those who claimed to know about contraception (n = 220, 49.3%) got the information from their friends, while others got the information from parents (n = 52, 11.7%), teachers (n = 28, 6.3%), nurses/doctors (n = 80, 17.9%) and others (n = 66, 14.8%). This suggests that adolescents discuss sexual issues more with their peers and supports the statement that adolescents usually feel more comfortable discussing sexual issues with their peers rather than their parents [7]. However, it was obvious that many of them do not have information regarding these issues and they end up with unwanted pregnancies for lack of information. Of the 172 learners who have been pregnant at least once before this study was conducted, only 64 (37.2%) reported that they ever used any form of contraception before they got pregnant. The reason for this poor knowledge could be associated with the fact that parents avoid having discussions about contraception with their children because of the fear that it may lead them to initiate sexual intercourse. Many parents who attempt to discuss reproductive health issues with their children would rather emphasize on abstinence and the dangers of unwanted pregnancies and sexually transmitted infections [11]. However, adolescents whose parents have engaged in reproductive health discussions are more likely to use effective means of contraception [3].
4.2.3. Knowledge About and Use of Contraceptives
Aside from the male condom, only a negligible number of the respondents affirmed that they know anything about contraceptives. Their “knowledge” of the male condom is probably restricted to the identification of the device since it is provided freely by the South African government and is available in the secondary schools. Many of them do not have the correct information on the use of the male condom as 186 (64.6%) of grade 8 learners and 78 (54.2%) of grade 12 learners said “condoms do not have expiry dates” and 188 (63.1%) and 70 (58.3%) of grades 8 and 12 learners respectively disagreed with the statement that new condoms should be used always. Only 154 (39.1%) of all the learners agreed that a condom should be used only once and afterward discarded. This suggests that some of them could have been using expired condoms or keeping used condoms for subsequent use which could adversely affect their health. Worse responses were recorded concerning other forms of contraceptives, including oral contraceptive pills, intrauterine devices and sterilization methods (Table 2). Only 4 (1.1%) respondents from grade 8 and 18 (11.3%) from grade 12 learners claimed to know about the side effects of contraceptives, while the others knew nothing about them. In spite of this poor knowledge, 98 (41.5%) of the learners reportedly did use contraceptives occasionally and 88 (35.5%) indicated that they preferred the male condom. This result is in consonance with the report of a previous study of contraceptive uses among South African youths where the male condom was found to be the most common form of contraceptive being used (57.6%) as opposed to others like the pills (5.2%) and the female condoms (8.9%) [26]. The vast majority of adolescents who engage in sexual intercourse without using contraceptives is of a great concern since contraceptives help to reduce the incidence of unwanted pregnancies.
| - | Grade 8 | Grade 12 | Total | |||
|---|---|---|---|---|---|---|
| Knowledge of Female condom | Freq. | % | Freq. | % | Freq | % |
| Yes | 94 | 29.4 | 14 | 9.1 | 108 | 22.8 |
| No | 226 | 70.6 | 140 | 90.9 | 366 | 77.2 |
| Total | 320 | 100 | 154 | 100 | 474 | 100 |
| Knowledge of male condom | ||||||
| Yes | 130 | 42.2 | 50 | 32.5 | 180 | 39.0 |
| No | 178 | 57.8 | 104 | 67.5 | 282 | 61.0 |
| Total | 308 | 100 | 154 | 100 | 462 | 100 |
| Do condoms have expiry dates? | ||||||
| Yes | 102 | 35.4 | 66 | 45.8 | 168 | 38.9 |
| No | 186 | 64.6 | 78 | 54.2 | 264 | 61.1 |
| Total | 288 | 100 | 144 | 100 | 432 | 100 |
| Should new condoms be used always? | ||||||
| Yes | 110 | 36.9 | 50 | 41.7 | 160 | 38.3 |
| No | 188 | 63.1 | 70 | 58.3 | 258 | 61.7 |
| Total | 298 | 100 | 120 | 100 | 418 | 100 |
| Should condoms be used only once? | ||||||
| Yes | 100 | 34.7 | 54 | 50.9 | 154 | 39.1 |
| No | 188 | 65.3 | 52 | 49.1 | 240 | 60.9 |
| Total | 288 | 100 | 106 | 100 | 394 | 100 |
| Knowledge about female sterilization | ||||||
| Yes | 2 | 0.6 | 2 | 1.3 | 4 | 0.8 |
| No | 346 | 99.4 | 156 | 98.7 | 502 | 99.2 |
| Total | 348 | 100 | 158 | 100 | 506 | 100 |
| Knowledge about male sterilization | ||||||
| Yes | 2 | 0.6 | 2 | 1.3 | 4 | 0.8 |
| No | 350 | 99.4 | 158 | 98.7 | 508 | 99.2 |
| Total | 352 | 100 | 160 | 100 | 512 | 100 |
| Knowledge about IUCDs | ||||||
| Yes | 2 | 0.6 | 0 | 0 | 2 | 0.4 |
| No | 348 | 99.4 | 160 | 100 | 508 | 99.6 |
| Total | 350 | 100 | 160 | 100 | 510 | 100 |
| Knowledge about oral contraceptives | ||||||
| Yes | 4 | 1.1 | 16 | 10.0 | 20 | 3.9 |
| No | 348 | 98.9 | 144 | 90.0 | 492 | 96.1 |
| Total | 352 | 100 | 160 | 100 | 512 | 100 |
| Knowledge about side effects of contraceptives | ||||||
| Yes | 4 | 1.1 | 18 | 11.2 | 22 | 4.3 |
| No | 344 | 98.9 | 142 | 88.8 | 486 | 95.7 |
| Total | 348 | 100 | 160 | 100 | 508 | 100 |
4.2.4. Teenage Pregnancy and Parenting
As at the time of data collection, 46 (11.1%) learners were suspecting that they might be pregnant due to signs ranging from missed periods to vomiting, especially breast changes. Out of the 172 respondents who have been pregnant in the past before this study was conducted, 106 (61.6%) have been pregnant once and 66 (38.4%) have been pregnant two or three times. Only 50 (20.5%) of these claimed to be ready for their first pregnancy while 130 (53.3%) reported that they were not ready and 36 (14.8%) indicated that they wished to get an abortion. This confirms the report that there is a high rate of unwanted pregnancy among South African young women [14]. For those who had babies (124 learners), their children were living with their mothers (n = 170, 68.5%), grandmothers (n = 26, 10.5%) or other people (n = 52, 21.0%). While this will afford the learners the opportunity to continue with their education, it will put an extra pressure and stress on the mothers (or, sometimes grandmothers or other relatives that were catering for the babies). Almost 80% of the grade 12 respondents indicated that they had received some information on teenage pregnancy while only a few of those in grade 8 (18.2%) gave a similar report. However, 288 (81.8%) Grade 8 and 34 (21.3%) Grade 12 learners stated that they had no information on teenage pregnancy. This discrepancy suggests that learners in grade 8 were probably considered too young for such an information, which is not the case considering that many of them were also sexually active.
4.2.5. Sources of Information Regarding Sexually Transmitted Infections (STIs), Primary Health Care centers and Legal Abortion
Almost all respondents from grade 12 (n = 128, 84.2%) claim to know about HIV/AIDS, but less than half of those in grade 8 (n = 134, 42.9%) know about the disease. Their sources of information include nurses (n = 78, 23.5%), parents (n = 74, 22.3%) and public campaigns (n = 4, 1.2%). Many respondents said they were aware of the existence of a Primary Health Care centers in their area mainly through their parents (n = 100, 26.5%) and friends (n = 84, 22.2%). Others got the information through their boyfriends, nurses/doctors and other people. The information made available to the respondents might not have much to do with their reproductive health needs because many of them (n = 350, 78.5%) do not know about legal abortion and where they can access this service. Only 96 (21.5%) of the respondents claimed to know about legal abortions and 86 (34.7%) of them reported that their parents or grandmothers informed them about legal abortions. Others learnt about legal abortions through the nurses (n = 68, 27.4%), teachers (n = 50, 20.2%) and their boyfriends (n = 44, 17.7%). This paucity of information may be responsible for the high rate of unsafe abortions among adolescents resulting in dozens of maternal deaths yearly in South Africa despite the fact that abortion has been legalized in South Africa since 1996 and the number of Termination of Pregnancy (TOP) services is on the increase [21, 27]. South Africa has been listed among countries with less restrictive abortion laws and yet with high rates of unsafe abortions among adolescents alongside with Cambodia, Ethiopia, Guyana and Nepal [28].
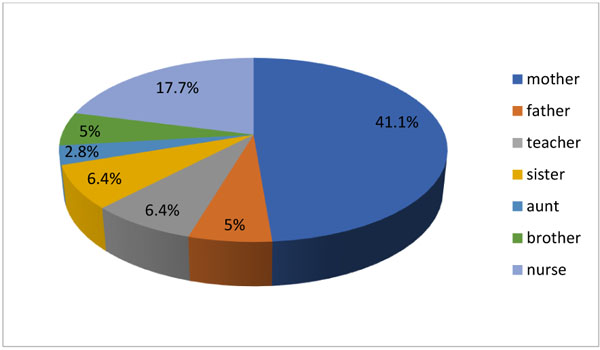
Only 38.9% of the respondents reported that they have someone they can confide in and discuss sexual issues with; most of them (n= 116, 41.1%) claim the person is their mother (Fig. 1). This finding is comparable to the report of the study conducted among the parents and adolescents of North Okkalapa Township where both male and female adolescents were found to be more comfortable in discussing reproductive health issues with their mothers rather than fathers. However, the same study stated that many adolescents are often unable to initiate the discussion about sexual issues with their parents.
Sadly, only 282 (55.1%) responded to this question; suggesting that the others feel they cannot discuss their sexual issues with anyone. This might be because of the cultural belief in many parts of Africa that open discussion about sexual issues is a taboo. Many respondents (n = 372, 80.5%) indicated that their parents have never initiated discussions with them regarding sexual issues and 348 (78.4%) do not bother to ask their parents about it because 182 felt parents were not supposed to talk about it (43.8%), 162 (38.9%) claimed that it is not culturally acceptable to discuss such matters with their parents while 72 (17.3%) ticked the option of “other reasons” [8, 9].
4.2.6. Opinions About Sex Education and Contraception
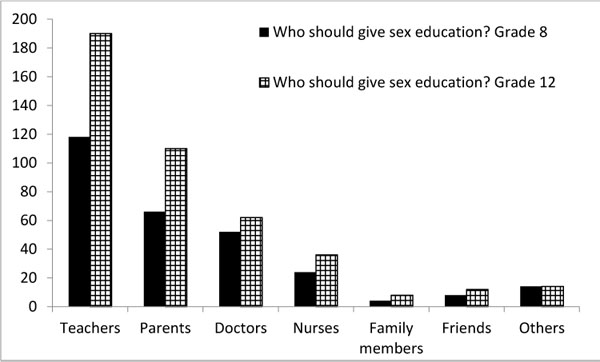
While being asked about their opinions about sex education and contraception, more than half (n = 286, 55.8%) of the respondents agreed that both boys and girls should receive formalized sex education; 118 (41.3%) grade 8 and 72 (49.3%) grade 12 learners think the teachers should be responsible for this, while 66 (23.1%) and 44 (30.1%) of the grades 8 and 12 learners accorded the responsibility to parents. Others chose other members of the public (Fig. 2). Only 72 (16.1%) respondents opined that sexually active teenagers should discuss family planning methods with their parents while 194 (43.3%) held an opposite opinion, saying teenagers do not have to discuss family planning methods with their parents. Though, 216 (53.5%) of the learners indicated that there are some periods in their schools whereby they can discuss sexual issues with their teachers, many of them might not make use of such an opportunity if there was not enough privacy or if they felt they had enough information from their friends. Less than half of the respondents admitted that they need more information about teenage pregnancy (n = 190, 37.1%), abortion (n = 146, 28.5%), HIV/AIDS (n = 214, 41.8%) and contraceptives (n = 134, 26.2%). Others claim they do not need further information about these issues. This shows that many of these adolescents may not initiate a discussion on these topics because they think they have all the information they needed, which is obviously not the case.
Most respondents from grade 12 held the opinions that contraceptives can make the users fat or obese (n = 110, 77.5%) and they also contribute to infertility (n = 102, 73.9%). In contrast, only a few respondents from grade 8 held the same opinions [98 (37.1%) and 102 (37.2%) respectively]. The Chi-square test shows a statistically significant difference in their opinions concerning contraceptive (P-value < 0.0001).
It was observed that generally, a higher proportion of grade 12 learners hold more positive and correct opinions about the reproductive health issues raised in this study. This might be because more of them have received some form of sex education as a result of their advanced age or the past wrong choices they have made. More learners from grade 8 and lower grades may be better assisted to also have positive opinions and correct information on these issues if trusted people, most especially their parents and teachers take up the responsibility of engaging them in discussions regarding their reproductive health, thereby helping them to make better choices.
4.2.7. Parental Involvement on Reproductive Health Issues
This study, like other previous studies, has established that most parents do not actively participate in the education of their adolescents regarding their sexual and reproductive health [8, 9, 11]. Although many adolescents will be willing to discuss these issues with their parents, yet, many of them will rather seek information from their peers unless their parents initiate the discussion [12]; but, in cases where the parents are involved, the adolescents made better reproductive health choices [3, 24, 25]. This further buttress the importance of the roles of parents, especially mothers in this very important stage of their children’s lives.
CONCLUSION
From the findings of this research, which shows that though many learners in Limpopo Province are living with at least one of their parents and yet many of them are lacking in the essential information regarding their reproductive health, it can be concluded that parents in the Limpopo Province were not actively involved in providing reproductive health education to their children. This has rendered many learners highly susceptible to teenage pregnancies, sexually transmitted infections and unsafe abortion practices. The need for the adolescents to obtain correct information concerning their reproductive health at an early stage before puberty has made it necessary that the information has to be provided by the trusted people around them in their growing up years, which, for many of them are their parents. It is recommended that the parents deliberately initiate communications on reproductive health issues with their children especially the females, give proper answers to their questions in order to encourage them and be always ready to assist them in making positive choices regarding their reproductive health. This will ensure that they are well prepared to handle their reproductive health challenges and minimize the effects of wrong sexual decisions on the society.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical approval was obtained from the University of Venda Research and Publication Committee. The permission to conduct the study was obtained from the Provincial department of Education, Strata South Africa and Democratic Nursing Organization of South Africa (DENOSA).
HUMAN AND ANIMAL RIGHTS
No animals/humans were used for the studies that are bases of this research.
CONSENT FOR PUBLICATION
A detailed explanation of the purpose and method of the study was given to each learner and informed consent was obtained from all the learners before they were given the questionnaires to complete.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The authors wish to thank the University of Venda Research and Publication Committee for funding this project, the Provincial Department of Education, Strata South Africa and Democratic Nursing Organization of South Africa (DENOSA) for granting the permission to conduct the research and the learners who volunteered to complete the questionnaires.

