All published articles of this journal are available on ScienceDirect.

The Analysis of Socio-Economic and Demographic Factors Associated with Contraceptive Use Among Married Women of Reproductive Age in Rwanda
Abstract
Background:
Contraceptive use is seen as pivotal for protecting women’s health and rights, influencing fertility and population growth, and helping to promote economic development. The main objective of this study was to identify the socio-economic and demographic factors associated with contraceptive use among married women of childbearing age in Rwanda.
Methods:
The current study used survey logistic regression model in order to account for the complexity of sampling design and heterogeneity between the observations from the same cluster. The 2014/2015 Rwanda Demographic and Health Survey data was used as application.
Results:
The findings from this study revealed that education level of the woman, wealth quintile of the household, woman’s province of residence, woman’s age at first cohabitation, current age of the respondent, woman’s working status, number of living children, husband’s desire for more children compared to the wife or partner, religious affiliation, health facilities, exposure to contraceptive information in media and by family planning workers, and current age of husband or partner were significant determinants of contraceptive use among ever married women of reproductive age.
Conclusion:
The findings from this study suggest improvement of exposure to the information of contraceptive use in health centres, empowerment of women for access to quality contraceptive use services and religious affiliation to play an important role to explain and inform their adherents on the importance of using a contraceptive method.
1. BACKGROUND
Contraceptive use is seen as pivotal for protecting women’s health and rights, influencing fertility and population growth, and helping to promote economic development especially in Sub-Saharan Africa. It also helps to prevent unwanted pregnancies and abortions and helps to determine the number of children in the family and enhances adequate child spacing [1, 2]. Globally, contraceptive use helps to prevent approximately 2.7 million infant and maternal deaths [3]. Some contraceptive methods such as condoms help to prevent HIV transmission and other sexually transmitted infections. The findings from various studies showed that satisfying a woman’s need for contraception, especially in family planning, may reduce the fertility rate by a considerable amount [4, 5]. But young women face many problems for utilizing contraceptive methods, especially family planning services, such as fear of side effects, cost, and lack of knowledge [6]. In general, contraception and family planning are known as the key for improving the health of the population because of their benefits. Even though many United Nations member countries, particularly those in the developed world, have strong family planning programmes, this is not the case in most sub-Saharan African countries, in some sub regions of Asia and Latin America and Caribbean, where despite a rise in contraceptive prevalence, many women continue to have unmet needs for contraceptives [7, 8].
The Government of Rwanda has piloted many initiatives, such as community based health insurance commonly known in Rwanda as Mutuelle de santé, Rwanda 2020 vision, and Economic Development and Poverty Reduction Strategy (EDPRS) among others and these have helped to make tremendous developments in the health sector that has also helped to assist in the demand for contraception and family planning and this has helped to achieve the fifth Millennium Development Goal (MDG). The prevalence of contraception use among current married women or women living with their husband or partner has improved in the last fifteen years. It was 35% in 2005, 52% in 2010, and 53% in 2014 [9]. This may be also attributable to various strong contraceptives method use and family planning programmes installed by the government of Rwanda, stakeholders and health care infrastructures. This is an indicator of progress in improving maternal and child health. Contraceptive use and the various initiatives and policies in the health sector have helped to improve maternal health and this is mostly the main goal of family planning. The maternal mortality rate in Rwanda has declined tremendously over the period of 15 years. As shown by Rwanda Demographic and Health Survey (RDHS), in 2000, 2005, 2010 and 2014 there were 1071, 750, 476 and 210 deaths per 100000 live births respectively [9]. Despite the improvement of increasing contraceptive use among women of reproductive age in Rwanda, there is a need to improve the use of modern contraceptive methods among married women in order to reach the targeted modern contraceptive use of 70% [10]; since the prevalence of modern contraceptive methods (pill, Intrauterine device (IUD), injection, condom, sterilization, the Lactational Amenorrhea Method (LAM), standards days method, emergency contraception) use among married women of reproductive age was 48% in 2014/2015 RDHS [9].
There are various studies in literature done on contraceptive use in Rwanda. However, many of them concentrate only on modern contraceptive use especially in family planning [11-13] and some of these methods can also help to prevent HIV and sexual transmitted infections but forget traditional methods. Therefore, the current study addresses this problem by combining all the contraceptive methods use among married women of reproductive age, nationwide. In addition, women from the same cluster may share common exposure to the practice of contraception and this violates the assumption of independence of observations. Consequently, the current study uses survey logistic regression model in order to account for complexity of sampling design and possible heterogeneity between observations from the same cluster. The main objective of this study was to identify the socio-economic and demographic factors associated with contraceptive use among married women of childbearing age in Rwanda. To the best of our knowledge, there was no study in literature identifying socio-economic and demographic determinants of contraceptive use among married women in Rwanda and using survey logic regression model to account for clustering and heterogeneity among observations from the same cluster. It was hoped that the findings from this study would help the public health related institutions and family planning services to enhance the knowledge of socio-economic and demographic factors associated with contraceptive use among married women of reproductive age and consequently contribute to improving contraceptive usage amongst all women.
2. MATERIAL AND METHODS
2.1. Source of Data
The present cross-sectional study used secondary data from the 2014/15 Rwanda Demographic and Health Survey (RDHS), the most recent national dataset on current contraceptive use. This survey was conducted from 9th November 2014 to 8th April 2015, where 12793 households were selected. The sampling used in this survey was a two-stage stratified method; in the first stage, 113 primary sampling or enumeration areas were selected from urban areas and 379 from rural areas. The sampling was done with probability proportional to the number of households residing in the village. In the second stage, systematic sampling was used for all households existing in the selected village and 26 households were selected in each village. This survey had three types of questionnaires: a questionnaire for households, a questionnaire for men and a questionnaire for women. Women’s questionnaire was used to collect information for all women aged 15-49 residing in the selected household on background characteristics, fertility preferences, contraception, reproduction, marriage and sexual activities and pregnancy among others and the data from this questionnaire were considered in the present study. The current study considered only currently married women or women living with partner. The eligible women response rate was 99.5% ; more details on sampling techniques and data collection can be found in [9].
2.2. Response Variable-Contraceptive Methods
There are different methods of contraceptive use, such as pill, IUD, injection, male condom, female condom, female sterilization, male sterilization, periodic abstinence, withdrawal, implants/Norplant, lactational amenorrhea (LAM) and standard days method. In the survey women were asked whether they used any of these methods. In the current study, a woman is considered as current contraceptive use if she uses at least one of the above mentioned methods and non-contraceptive use if otherwise and this was coded as “1” and “0” for contraceptive use and non-contraceptive use respectively.
2.3. Independent Variable
The dependent variables used in this study have been used elsewhere [7, 14-17]. These variables are classified as socio-economic and demographic factors: current age of the respondent, the age at first cohabitation (recorded as: <15, 15-17, 18-22, 22-49), woman’s level of education (no education, primary, secondary, tertiary), heard about family planning in last few months in newspapers/magazine (yes, no), heard about family planning in the last months on television (yes, no), visited by family planning worker during last 12 months (yes, no), husband’s or partner’s desire of children compared to the wife or partner (same, husband wants more, husband wants fewer, don’t know), wealth index of her household (poorest, poorer, middle, richer, richest), province of residence (Kigali, south, west, north, east), place of residence (urban, rural), currently working (yes, no), religious affiliation (Catholic, Protestant, Seventh Day Adventist, others), husband’s or partner’s education level (no education, primary, secondary, tertiary), decision-making for using contraceptive (mainly respondent, mainly husband or partner, joint decision, others), person who usually decides on health care (respondent alone, respondent and husband/partner, respondent and other person, husband/partner alone, someone else, others), number of living children (0, 1, 2, 3, 4 and more), size of the family (continuous) and age of the husband or partner (continuous).
2.4. Statistical Methods
Based on the sampling design used when collecting the data in Demographic Health Survey, the current study uses survey logistic regression model in order to account for the complexity of sampling design and account for heterogeneity between observations from same cluster.
2.5. Model Formulation
Let yijk denote the contraceptive use status of woman i from stratum j and cluster m, with i = 1, 2, 3, ... ,6841, j = 1, 2, 3, ... ,60 and m = 1, 2, 3, ... ,492. The dependent variable is defined as a dichotomous variable such that yijm = 1 if the women i is using any type of contraceptive methods and yijm if the women i is not currently using any type of contraceptive methods. It is assumed in the present study that the response variable yijm is Bernoulli distributed as yijm|μijm~Bernoulli (μijm), where μijm is known as the mean and is given by E(yijm) = μijm. It is related to the explanatory variables as:
g(μijm) = X'ijmβ + U'ijmδ
where g(.) is the logit link function, β is a p-dimensional vector of regression of categorical explanatory variables, namely, woman’s education level, wealth quintile of the household, visited health facility last 12 months, respondent currently working, woman’s age at fist cohabitation, religion, woman’s current age, heard about family planning on the radio last few months, heard about family planning on the TV last few months, heard about family planning in the newspaper/magazine, province, husband desires children, husband/partner’s education level, age of the husband/partner) and δ is a q-dimensional vector of regression of continuous covariates (age of the husband/partner, size of the family).
2.6. Model Fitting and Testing
The analysis in this study was done utilizing Proc Survey logistic from SAS software version 9.4. The Taylor series method was used in this study as variance estimator and this is the default in SAS. The model fit statistics in survey logistic was assessed based on Akaike Information Criteria (AIC), the Schwarz Criterion (SC) and -2 Log-Likelihood (-2LogL) principles. The model test was done based on Likelihood ratio, score and the Wald test principles.
3. RESULTS
3.1. Descriptive Analysis
Table 1 presents the descriptive statistics of the participants. Out of 6841 married women or women living with their husband or partner 52.7% of them were currently using any type of contraceptive methods, where 5.9% and 46.8% were traditional and modern contraceptive methods respectively. The mean age of the respondents was 32.81, minimum was 16 and maximum was 49. The mean of the size of the household was 5.0; minimum was 1 and maximum was 15 members. The mean age of the husband or partner was 37.39, minimum was 18 and maximum was 95 years old. It is observed from the Table that 83.0% of the respondents were from rural areas whereas 17.0% were from urban areas. It is also observed that 16.5% of the respondents had no level of education, 70.5% had primary level, 10.3% had secondary education level and only 2.7% of them had tertiary education level. It can be seen from the Table that 55.0% of respondent heard about family planning on the radio, 7.1% on the TV and 6.1% in newspapers or magazines.71.8% of respondents visited health facilities in last 12 months before the period of survey, and 46.3% of them were told about family planning at health facilities. It is observed from Table 1 that 38.2% of the respondents were Catholic, 45.2% were Protestant, 12.8% and 3.2% were from religions other than Catholic, Protestant or Seventh Day Adventist.
| Variable | Categories | % or M or Range |
|---|---|---|
| Current contraceptive use | Yes No |
52.7(traditional=5.9%; modern=46.8%) 47.3 |
| Respondent current age | Continuous | M=32.81(Minimum=16, maximum=49) |
| Size of the family | Continuous | M=5.0(Minimum=1, maximum=15) |
| Current age of partner | Continuous | M=37.39(Minimum=18, maximum=95) |
| Place of residence | Urban Rural |
17.0 83.0 |
| Respondent education level | No education Primary Secondary Tertiary |
16.5 70.5 10.3 2.7 |
| Wealth index | Poorest Poorer Middle Rich Richest |
18.8 21.2 20.9 19.9 19.3 |
| Heard about family planning on the radio last few months | Yes No |
55.0 45.0 |
| Heard about family planning on the TV last few months | Yes No |
7.1 92.8 |
| Heard about family planning in newspaper/magazine last few months | Yes No |
6.1 93.9 |
| Visited by family planning worker last 12 months | Yes No |
29.2 70.8 |
| Visited health facility last 12 months | Yes No |
71.8 28.2 |
| At health facility, told of family planning | Yes No |
46.3 53.7 |
| Respondent currently working | Yes No |
86.8 13.2 |
| Husband/partner education level | No education Primary Secondary Tertiary Don’t know |
16.9 70.1 9.2 3.5 .2 |
| Number of living children | 0 1 2 3 4 and more |
5.2 17.9 45.2 17.4 37.4 |
| Religion | Catholic Protestant Seventh Day Adventist Others |
38.2 45.6 12.8 3.2 |
The model fit is tested based on the Akaike Information Criterion (AIC), the Schwarz Criterion (SC) and the negative of twice the log likelihood (-2LogL). AIC and SC are used to compare the model of intercept only and the model of intercept and covariates. It is noted that the smaller the value of AIC and SC the better the model fit. It was observed from Table 2 that fitting the model with covariates and intercept had a small AIC and SC compared to model with intercept only. Consequently it was used in the analysis. The global null hypothesis was tested based on Likelihood ratio test and Score test and these two tests were found to be significant (Table 3) therefore the global null hypothesis stating that the slope parameters are zero is rejected.
| Criterion | ||
|---|---|---|
| AIC | 9433.526 | 8673.849 |
| SC | 9440.353 | 8960.604 |
| -2 Log L | 9431.526 | 8589.849 |
| Test | F Value | Number of degree of Freedom | Pr>F |
|---|---|---|---|
| Likelihood Ratio | 19.33 | 35.5079 | <.0001 |
| Score | 13.94 | 41 | <.0001 |
| Wald | 9.28 | 41 | <.0001 |
Table 4 provides the unadjusted and adjusted odds ratios of survey logistic regression model, used to identify the determinants of contraceptive use among women of childbearing age. Wealth index of household, woman’s education level, woman’s age at first cohabitation and her age at the period of survey, her religious affiliation, size of the family, whether the woman heard about family planning on the radio, on TV or in newspapers/magazine, her province of residence, whether she was working or not at the period of survey, whether she was visited by family planning worker in the last 12 months prior to the survey, number of living children, husband/partner’s desire for more children and current age of the husband or partner were found to be significantly associated with the contraceptive use among married women of childbearing age in Rwanda. The results of fixed effect are summarized in Table 4 and the results of interaction effect are summarized in Table 5 and Fig. (1).
| Variables | Unadjusted | Adjusted | ||
|---|---|---|---|---|
| Odds ratios(OR) | P-value | Odds Ratio (OR) |
P-value | |
| Intercept | 0.898 | 0.1342 | 1.328 | 0.5445 |
| Woman’s education level (no education =ref) Tertiary level Secondary level Primary level |
1.477 1.293 1.283 |
0.0140 0.0011 0.0176 |
58.694 2.489 3.003 |
<.0001 0.1126 0.0150 |
| Wealth quintile of the household (richest=ref) Richer Middle Poorer Poorest |
1.012 0.944 0.786 0.745 |
0.8883 0.5241 0.0033 0.0016 |
0.954 0.866 0.752 0.743 |
0.6490 0.2030 0.0068 0.0146 |
| Visited health facility last 12 months (no=ref) Yes |
1.169 | 0.0065 | 1.379 | <.0001 |
| Respondent currently working (yes=ref) No |
0.766 | 0.0003 | 0.769 | 0.0014 |
| Age of first cohabitation (23-49=ref) <15 15-17 18-22 |
0.632 1.246 1.163 |
0.0470 0.0123 0.0069 |
0.595 1.050 1.035 |
0.0235 0.6055 0.5975 |
| Number of living children (4 and more=ref) 0 1 2 3 |
0.013 0.811 1.071 1.108 |
<.0001 0.0035 0.3368 0.1744 |
0.007 0.495 0.768 0.902 |
<.0001 <.0001 0.0058 0.2368 |
| Religion (others=ref) Catholic Protestant Seventh Day Adventist |
1.151 0.790 1.249 |
0.4035 0.1505 0.2119 |
2.409 1.564 2.549 |
0.0233 0.2431 0.0194 |
| Woman’s current age (35-49=ref) 25-34 15-24 |
0.783 1.088 |
0.0014 0.1267 |
1.584 1.222 |
0.0007 0.0125 |
| Heard about family planning on the radio last few months (yes=ref) No |
0.762 | <.0001 | 0.859 | 0.0077 |
| Heard about family planning on TV last few months (yes=ref) No |
0.721 | 0.0020 | - | - |
| Visited by family planning worker last 12 months (yes=ref) No |
1.169 | 0.0065 | 0.784 | 0.0001 |
| At health facility, told of family planning(yes=ref) No |
0.937 | 0.2821 | - | - |
| Heard about family planning in newspaper/magazine (yes=ref) No |
0.614 | <.0001 | 0.682 | 0.0030 |
| Province (West=ref) Kigali South North East |
1.362 1.282 1.797 1.340 |
0.0025 0.0064 <.0001 0.0013 |
1.268 1.237 1.590 1.331 |
0.0621 0.0288 <.0001 0.0024 |
| Husband desires children (same number=ref) more fewer don’t know |
1.295 1.268 0.876 |
0.0033 0.0094 0.2305 |
1.319 1.278 0.957 |
0.0033 0.0094 0.7107 |
| Husband’s education level (no education=ref) Don’t know secondary level Higher level Primary level |
0.822 1.055 0.822 1.027 |
0.7456 0.7188 0.0690 0.7571 |
- | - |
| Place of residence (Urban=ref) rural |
0.867 | 0.0696 | - | - |
| Age of the husband/partner | 0.999 | 0.6203 | 0.985 | 0.0002 |
| Size of the family | 1.118 | <.0001 | - | - |
| Variables | Unadjusted | Adjusted | ||
|---|---|---|---|---|
| Odds ratio (OR) | P-value | Odds ratio (OR) |
P-value | |
|
Education*religion (no education and other religions =ref) Tertiary and Catholic Tertiary and Protestant Tertiary and Seventh Day Adventist Secondary and Catholic Secondary and Protestant Secondary and Seventh Day Adventist Primary and Catholic Primary and Protestant Primary and Seventh Day Adventist |
0.091 0.097 0.084 0.439 0.496 0.390 0.392 0.427 0.409 |
0.0380 0.0380 0.0366 0.1292 0.1928 0.1112 0.0303 0.0542 0.0457 |
0.021 0.028 0.016 0.527 0.518 0.568 0.357 0.402 0.397 |
<.0001 <.0001 <.0001 0.2861 0.2649 0.4046 0.0250 0.0495 0.0509 |
The odds of contraceptive use decreases with wealth quintile of the household. A woman from poorer and poorest household was 0.752(p-value=0.0068) and 0.743 respectively (p-value=0.0146) times less likely to use a contraceptive method compared to a woman from richest family. The present study did not find a significant difference between a woman from middle and richest household and association with contraceptive use among women of childbearing age.
It is noted from the results that the age at first cohabitation was found to be significantly associated to contraceptive use. A woman who had her first cohabitation at age less than 15 years old was 0.595 (OR=0.595, p-value=0.0235) times less likely to use a contraceptive method than a woman who had her first cohabitation from age group 22-49 years old. However, there was no significant difference in the current contraceptive use among woman who had her first cohabitation at the age 15-17, 18-21 and a woman who had her first cohabitation at 22-49 years old.
It was observed from the analysis that the working status of the woman was significantly associated with current contraceptive use among married woman or woman living with her partner. A woman who was not working at the period of survey was 0.769 (OR=0.769, p-value<.0001) less likely to use contraceptive method compared to a woman who was working at the period of the survey.
It is observed from the Table that the current age group of the woman had a significant effect on current contraceptive use among women. A woman who was in age group 25-34 and 15-24 at the period of survey was 1.584 and 1.222 respectively (OR=1.584, p-value=0.0007 and OR=1.222,p-value=0.0125) times more likely to use a contraceptive method than a woman who was in the age group 35-49 years old.
A woman who was not visited by a family planning worker in the last 12 months prior to the survey was 0.784 (OR=0.784, p-value=0.0001) times less likely to use contraceptive than a woman who was visited by a family planning worker in the last 12 months prior to the survey. The use of contraceptive varied with the woman’s province of residence. A woman from Eastern, Northern and Southern province was 1.331, 1.590 and 1.237 respectively (OR=1.331, p-value=0.0001, OR=1.590, p-value <.0001, OR=1.237, p-value=0.0288) times more likely to use contraceptive methods than a woman from Western province. But a woman from Kigali did not show any statistical difference compared to a woman from Western province.
The number of living children was significantly associated with the use of contraceptive method. The results revealed that a woman who had one child was 0.495 (OR=0.495, p-value <.0001) less likely to use contraceptive method compared to a woman who had four children or more. It was also found that a woman who had two children was 0.768 (OR=0.768, p-value=0.0058) less likely to use any type of contraceptive method compared to a woman who had four children or more.
A woman who did not hear about family planning in newspaper/magazines was 0.682 (OR=0.682, p-value=0.0030) times less likely to use contraceptive method compared to a woman who heard about family planning in newspapers/magazines. A woman whose husband desired more children or fewer children than her was 1.319 and 1.278 respectively (OR=1.319, p-value=0.0033, OR=1.278, p-value=0.0084) times more likely to use a contraceptive method compared to a woman whose husband/partner desired the same number of children as her.
A woman who did not hear about family on the radio last few months prior to the survey was 0.859 (OR=0.859, p-value=0.0077) times less likely to use contraceptive method compared to a woman who heard about family planning on the radio last few months prior to the survey.
It was also noted from the results that the age of the partner has an important significant effect on his wife or partner’s current contraceptive use. The results revealed that for a unit increase in age of the husband, the odds of contraceptive use by his wife or partner reduced by 1.5% (OR=0.985, P-value=0.0002).
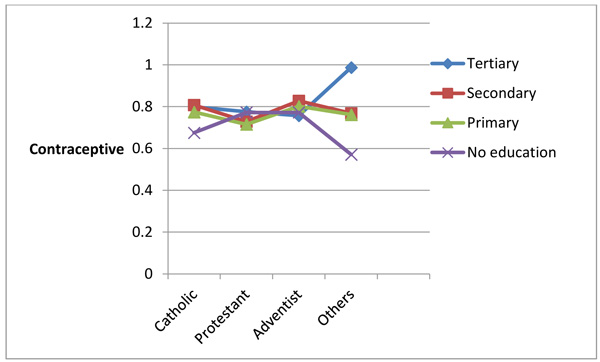
3.2. Interaction Effects
The current study considered various two-way interaction effects but only women’s education level and her religious affiliation was significant and therefore used in the analysis. The results are summarized in Table 5 and Fig. (1). It is observed from Fig. (1) that contraceptive use increases with level of education among women from Catholic and women from religions other than Catholic, Protestant and Seventh Day Adventist. It is also observed from the Figure that there is a big gap between women with tertiary education level and women with no education level on contraceptive use among women from religions other than Catholic, Protestant and Seventh Day Adventist. It is observed from the Figure that contraceptive use is higher among Seventh Day Adventist women with secondary education, followed by women with primary education. It is also observed from the figure that contraceptive use was higher among Protestant women with no education and tertiary education followed by women with secondary education.
4. DISCUSSION
The findings from this study showed that the prevalence rate of contraceptive use among married women or women living with their partner was 52.7% and 30.9% respectively among all women of childbearing age.
The findings from multivariate survey logistics regression showed that the current use of contraceptive methods increases with increasing household wealth quintile. This finding was found in similar researches [11, 16-20]. This may be due to the fact that women from richest family have more exposure to the use of contraceptive methods information than women from poorest and poorer households.
The findings from the current study highlighted the disparities in the use of contraceptive method by women according to their province of residence. It was noted from the results that married women from Northern Province use contraceptive methods more than women from any other provinces in Rwanda. This finding was found elsewhere by [9]. The findings from this study revealed that older women were less likely to use contraceptives. This may suggest a need to educate older women about the importance of the use of contraceptive methods. The contraceptive use increases with age group up to 25 and 34 and then decreases afterwards. This finding was found elsewhere by [11, 16, 17, 21]. This may be due to the fact that the majority of women of this age group are working and they have a number of children such that they want to limit births or undesired pregnancy and at the same time save their jobs. In addition, the women from this age group are mostly studying and this may help them to access the information in mass media or from their studies.
Generally, contraceptive use is commonly influenced by factors such as education, place of residence and wealth index where the poor are the most disadvantaged and less likely to use contraceptives [16, 22]. However in the present study, in multivariate analysis, the study found no significant difference in the use of contraceptive methods among women of childbearing age from urban areas and those from rural areas. The results from the present study also revealed an interaction effect between women’s education level and her religious affiliation and this was a surprising finding of the current research. To the best of our knowledge there was no other research in literature that studied this interaction effect. In most of the research, it was found that contraceptive use increases with increasing the woman’s level of education [15, 16, 23] among others. However, the findings from this research revealed that the effect of education on contraceptive use is affected in one way or another by religious beliefs. In most cases, religious teaching and preaching opposes contraceptive use and for this reason some of their members choose for themselves what seems good to them between contraceptive use and non-contraceptive use. This may be the reason why in some religions contraceptive use increases with the level of education and in others decreases with increasing the level of education and yet in others there is no clear relationship.
The findings from this study revealed that exposure to the use of contraceptive information played a crucial positive role in contraceptive use and family planning. This finding was also found in the studies by [13, 17, 24, 25]. This may be due, for example, to the fact that when a woman visits a health centre or is visited by a family planning worker, she is sensitized on the use of contraceptive methods and their importance on family planning, HIV and undesired pregnancy, among others. However, there was no significant difference with contraceptive use between a woman who did not hear about family planning on TV and a woman who heard about family planning on TV.
The findings from this study also highlighted the important role played by the age of the husband or partner on the use of contraceptive methods by his wife or partner; where the age of the husband or partner and current contraceptive use methods by his wife or partner are inversely proportional to each other. This may be due to the fact that older men tend to discourage contraceptive use methods especially when limiting births and may also resist modern contraceptive use because of cultural beliefs.
The study found that the number of living children is an important factor associated with contraceptive use. The contraceptive use increases with increasing the number of living children. This finding was found in similar studies by [14, 21, 26-29]. This is not surprising because a woman who has many children tends to limit births. It is known from literature that a small family allows for investment in each child, for instance by paying for their education and health care.
CONCLUSION
The main objective of this study was to identify the socio-economic and demographic factors associated with contraceptive use among married women or women living with their partners of reproductive age in Rwanda. The findings from this study revealed that education level of the woman, wealth index of the household, province of residence, age at first cohabitation, her current age, her working status, the number of living children, preference of number of children by husband or partner compared to that of the wife or partner, religious affiliation, exposure to information on family planning (such as hearing about family planning on the radio, reading newspaper or magazines, visiting health centre, visited by family planning worker, told about family planning at the health centre) were determinants of contraceptive use among married women or women living with partner of reproductive age. It was highlighted that women who listen to the radio, visited the health centre or were visited by the family planning workers and told about family planning, aged between 25-34, working at the period of survey, with higher education level had higher odds of using contraception. The study also considered various two- way interaction effects and only the interaction effect between religious affiliation and woman’s education level was significant. The findings from this study suggested that religious affiliation should also play an important role to explain and inform their adherents on the importance of using a contraceptive method; the findings also suggested improvement about exposure to the information of contraceptive use in health centres, the use of trained health workers in communities and in mass media especially radio, to empower women for access to quality contraceptive use services especially family planning, encourage spousal communication on contraceptive use and to continue improving women’s access to education. Further research is needed to identify the reasons for disparities of contraceptive use among provinces and why the prevalence of contraceptive use among women of childbearing age is higher in Northern province and this may help to address why the prevalence is low in Western province and to highlight the predictors that can increase the use of contraceptives among young women.
LIMITATIONS
The analysis in this study was mainly based on cross-sectional study and this may not draw the causal relationship or effect between contraceptive use and independent variables; only an association can be drawn from this study. A longitudinal study is suggested for future work to identify relevant trends and patterns over time.
AVAILABILITY OF THE DATA
RDHS data are freely available to registered users with permission at http:// dhsprogram.com.data /Rwanda_ Standard-DHS2015.cfm.
FUNDING
The authors received no funding for this study.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study does not involve any experiment or interaction with human or animal subjects. The study uses secondary data from 2014/2015 RDHS. The 2014/15 RDHS was reviewed and approved by Rwanda National Ethics Committee, National Institute of Statistics of Rwanda and International Review Board of ICF International. We were granted permission by ICF international, Inc. to use these de-identified data.
HUMAN AND ANIMAL RIGHTS
No animals/ humans were used for the studies that are bases of this research.
CONSENT FOR PUBLICATION
Not applicable.
CONFLICT OF INTEREST
The authors declare no potential conflicts of interest with respect to the research, authorship, and/ or publication of this article.
ACKNOWLEDGEMENTS
The authors acknowledge National Institute of Statistics of Rwanda (NISR) [Rwanda], Ministry of Health (MOH) [Rwanda], and ICF International for the data.

