All published articles of this journal are available on ScienceDirect.

Non-Adherence Related Factors to Antihypertensive Medications Among Hypertensive Patients on Follow up at Nedjo General Hospital in West Ethiopia
Abstract
Background:
Hypertension is an overwhelming global challenge. Increasing awareness and diagnosis of hypertension, and improving control of blood pressure with appropriate treatment are considered critical public health initiatives to reduce cardiovascular morbidity and mortality.
Objective:
To assess non-adherence-related factors to antihypertensive medications among hypertensive patients on follow up at Nedjo General Hospital.
Methods:
A cross-sectional study was conducted among hypertensive patients on follow up at Nedjo General Hospital from March 15 to May 5, 2015. A total of 172 hypertensive patients who were available during study period were included in the study. To identify the independent non-adherence-related factors, backward logistic regression analysis was used.
Results:
Only 54 (31.4%) of the study participants were adherent to their treatment. On multivariable logistic analysis non-adherence was more likely to occur among those with age of >55 years (Adjusted odds ratio (AOR) = 0.10, 95% CI = 0.01-0.85, p=0.035), illiteracy (AOR = 6.76, 95% CI = 1.01-45.08, p=0.049), income status of <500 Ethiopian birr (AOR = 18.51, 95% CI = 1.95-176.06, p=0.011), duration of treatments of >5 years (AOR = 5.41, 95% CI = 1.08-27.22, p=0.041), physical inactivity (AOR = 34.51, 95% CI = 4.66-255.89, p=0.001) and knowledge deficit about hypertension and its treatment (AOR = 7.67, 95% CI = 2.48-23.73, p<0.001).
Conclusion:
A finding of this study revealed that an adherence status of study participants was low. Thus, greater effort is needed to improve patient adherence to antihypertensive medications.
1. INTRODUCTION
Hypertension (HTN) is an overwhelming global challenge [1, 2]. Hypertension is defined as persistently elevated arterial Blood Pressure (BP) and it is identified as one of the most significant risk factors for Cardiovascular (CV) disease. Increasing awareness and diagnosis of hypertension, and improving control of BP with appropriate treatment are considered critical public health initiatives to reduce CV morbidity and mortality [3].
A study done on global burden of blood-pressure-related disease revealed that Worldwide, 7·6 million premature deaths (about 13·5% of the global total) and 92 million Disability-Adjusted Life Years (DALYs) (6·0% of the global total) were attributed to high blood pressure [2]. Even though there are medications that are used to treat hypertension, because of large proportion of patients not taking these medicines as prescribed the benefits of these drugs are not being realized and this indirectly raises the issue of therapeutic adherence among hypertensive persons [4].
The most frequently used definition of adherence is “the extent to which a person’s behavior – taking medication, following a diet, executing lifestyle changes – follows medical advice” [5]. Adherence has also been defined as “the extent to which patient behavior corresponds with recommendations from a health care provider” [5]. A review from the 2095 articles identified that therapeutic non-adherence occurs when an individual’s health-seeking behavior lacks similarity with the recommendations as prescribed [6].
Non adherence to treatment medication and lifestyle modification is a complicated issue affecting patients’ health, health expenditure, and resources’ utilization while adherence to Antihypertensive Treatment (AHT) has been associated with improved blood pressure (BP), decreased hospitalizations rates, and lower medical care costs [7-9]. Survey conducted 2003-2004 showed only 37% of hypertensive patients have their blood pressure controlled [10]. Uncontrolled high blood pressure indirectly raises the issue of therapeutic adherence among hypertensive persons [11]. According to the WHO, poor adherence to treatment is the most important cause of uncontrolled blood pressure and only 20 to 80% of patients receiving treatment for hypertension in real life situations are considered to be “good compliers” [5].
Different studies had identified factors determining the levels of antihypertensive drug adherence such as; the complexity of the treatment, the drugs’ side effects, the balance between established medical guidelines and their own convictions, communication between patient and doctor, patient’s satisfaction with the healthcare system, socio-economic factors, socio-demographic factors, the cost of treatment and lack of medical insurance [3, 6, 7, 12-25].
This study aimed to examine adherence to antihypertensive medication and to assess factors associated with non-adherence to medications at Nedjo General Hospital. Identification of non-adherence related factors will help the healthcare professionals and patients to work on those factors to improve non-adherence. The findings of the study will also suggest strategies for improving non-adherence. As there was no study done in West Ethiopia, this study will help as a base to perform further studies.
2. METHODS AND PARTICIPANTS
2.1. Study Setting and Period
The study was conducted in Nedjo General Hospital (NGH), Nedjo town, Western Wollega zone, Oromia region, western Ethiopia which is found 496 km from Addis Ababa, a capital city of Ethiopia. The study was conducted from March 15 to May 5, 2015.
2.2. Study Design
The study was conducted using hospital based descriptive cross–sectional study design which involves quantitative methods.
2.3. Study Population
All adult hypertensive patients attending the facility on out-patient basis during the study period and attended the chronic care department for hypertension care at least for one year and volunteered to take part in the study were used for the study. A total of 172 hypertensive patients were included in the study. Patients who are critically ill, psychotic and/or unable to communicate with data collector due to other underlying medical disorder were excluded.
2.4. Data Collection Process and Quality Assurance
Data were collected using a questionnaire consisting of the 8- item morisky medication adherence scale [26] which was adapted to our set up and self-reported medication adherence questions relating to medication use and major reasons for non-adherence which were designed-based on an extensive literature review of similar studies [12, 21, 24, 27]. The questionnaire was presented to each patient with proper explanation and face to face interviews were conducted when patients came for follow up checkup. Patient medication charts were also reviewed carefully for assessing the characteristics of hypertension and antihypertensive treatment. Data collection was conducted with appropriate training of the data collectors and continuous advices to keep the quality of the data. Close supervision was made by the investigators and the collected data were checked for completeness every day.
For completeness and consistency, standardized questionnaire of English version was translated to local language Afaan Oromoo. Then, it was again translated to English and checked.
Medication adherence: Adherence to antihypertensive medications was measured using the 8-item Morisky medication adherence scale. Individual item scores were summed and those with a score of 8 were considered adherent to medication. Medium adherence corresponded to a score of 6–8, while a score of <6 was considered low adherence [26]. Medication non-adherence referred to a score of <8 (i.e., medium or low adherence).
Extra salt intake was defined as “Patients who report the addition of salt in food on table”.
2.5. Data Analysis and Interpretation
After data collection, data were entered into the Statistical Package for the Social Sciences (SPSS) version 20 for analysis. Odds ratio with 95% confidence interval, along with binary and multiple logistic regression was used to assess the significance and strength of association. All factors with a p-value <0.25 in the bivariable logistic regression analysis were further entered into the multivariable model to control confounding effects. A significance level of alpha = 5% was used to identify statistically significant association.
| Variables | Categories | n (%) |
|---|---|---|
| Sex |
Male | 76 (44.2) |
| Female |
96 (55.8) | |
| Age |
18-34 |
19 (11.0) |
| 35-54 |
85 (49.4) |
|
| 55 | 68 (39.5) |
|
| Marital status | Single | 17 (9.9) |
| Married | 119 (69.2) |
|
| Divorced | 21 (12.2) | |
| Widowed |
15 (8.7) |
|
|
Occupation |
Employed | 36 (20.9) |
| Unemployed | 26 (15.1) |
|
| Student | 12 (7.0) |
|
| Farmer | 84 (48.8) | |
| Business man or Woman |
14 (8.1%) |
|
|
Place of residence |
Urban | 78 (45.3) |
| Rural |
94 (54.7) |
|
| Level of education | Illiterate | 75 (43.6) |
| Elementary | 42 (24.4) |
|
| Secondary | 22 (12.8) | |
| College/University |
33 (19.2) |
|
|
Income status (Monthly income in Birr) |
<500 | 70 (40.7) |
| 500-1000 |
49 (28.5) |
|
| 1000-2000 | 21 (12.2) |
|
| >2000 | 32 (18.6) |
3. RESULTS
A total of 172 hypertensive patients out of the 184 cases were included in the study. Twelve of the respondents were excluded by the exclusion criteria. Of this 5 were not volunteer to participate while 7 patients, even though they are volunteer they did not fulfill the inclusion criteria because they were newly diagnosed for hypertension and medication initiation was less than one year. So the response rate was 93.5%. Majority of the respondents were females (55.8%). The mean age of the respondents was 51.5 + 12.1 years. Out of the study participants 49.4% were in the age range of 35-54 years. More than half of the study participants 119 (69.2%) were married and 84 (48.8%) were farmers (Table 1).
Most of the respondents, 109 (63.4%) were taking a single antihypertensive medication and 48 (27.9%) respondents were taking two antihypertensive medication. Among 172 study participants, 72 (41.9%) respondents were treated for less than two years and 51 (29.7%) were treated for > 5 years. Regarding knowledge of the study participants about hypertension and its treatment, more than half of the study participants 112 (65.1%) had inadequate knowledge about hypertension and its treatment (Table 2).
| Variables | Categories | n (%) |
|---|---|---|
| Number of antihypertensive medication | 1 | 109 (63.4) |
| 2 | 48 (27.9) | |
| 3 |
15 (8.7) |
|
|
Duration of treatments |
<2 Years |
72 (41.9) |
| 2-4 Years | 49 (28.5) |
|
| >5 Years | 51 (29.7) | |
|
Physical activity |
Inactive |
63 (36.6) |
| Minimally active | 76 (44.2) | |
| Vigorously active |
33 (19.2) |
|
| Extra salt intake |
Yes | 59 (34.3) |
| No | 113 (65.7) | |
| Cigarette smoking status |
Yes |
24 (14.0) |
| No |
148 (86.0) |
|
| Knowledge about hypertension and treatment Adherence Status |
Yes |
60 (34.9) |
| No |
112 (65.1) | |
| Adherent |
54 (31.4) |
|
| Non-adherent |
118 (68.6) |
Most of the study participants 118 (68.6%) were non-adherent to antihypertensive medications, whereas 54 (31.4%) were adherent (Table 2). For non-adherent respondents 118 (68.6%), the major reasons for non-adherence were forgetfulness 81 (47.1%), followed by inability to buy medications 29 (16.9%) (Table 3).
| Variables | n (%) |
|---|---|
| Forget to take medications |
81 (47.1) |
| Cannot afford to buy the medications always | 29 (16.9) |
|
Don’t believe in the medication |
5 (2.9) |
|
Patient cannot swallow medication(s) |
2 (1.2) |
| The schedule of patients work makes it impossible | 1 (0.6) |
| Adherent | 54 (31.4) |
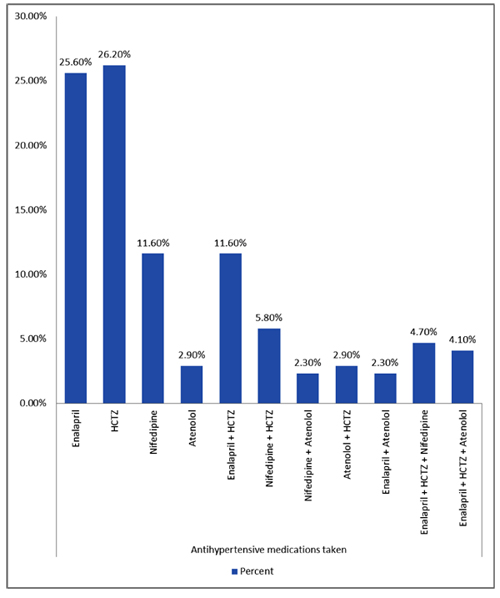
In our study regarding antihypertensive medications Hydrochlorothiazide, 45 (26.2%) and Enalapril, 44 (25.6%) were the commonly prescribed antihypertensive medications followed by Nifedipine 20 (11.6%) and a combination of Enalapril plus Hydrochlorothiazide 20 (11.6%) Fig. (1).
The bivariable analysis showed that non-adherence was associated with marital status, occupation, place of residence, level of education, income status, number of antihypertensive medication, physical activity, extra salt intake and knowledge of hypertension. However, other factors did not show statistically significant association with non-adherence (Table 4). Majority of patients with age > 55 years, patients who live in rural, patients who are illiterate and their level of education was elementary and patients with low level of Knowledge about hypertension and treatment were non-adherent to their antihypertensive medication (Table 4).
| Variables | Categories | Adherence status | P-value | COR (95% CI) for Non-adherence status | |
|---|---|---|---|---|---|
| Adherent | Non-adherent | ||||
| Sex | Male | 28 | 48 | 1.00 | |
| Female | 26 | 70 | 0.172 | 1.57(0.82-3.00) | |
| Age | 18-34 | 9 | 10 | 0.231 | 1.00 |
| 35-54 | 27 | 58 | 0.201 | 1.93(0.70-5.31) | |
| >55 | 18 | 50 | 0.087 | 2.50(0.88-7.14) | |
| Marital status | Single | 10 | 7 | 0.096 | 1.00 |
| Married | 34 | 85 | 0.017 | 3.57(1.26-10.15) | |
| Divorced | 5 | 16 | 0.033 | 4.57(1.14-18.41) | |
| Widowed | 5 | 10 | 0.154 | 2.86(0.67-12.11) | |
| Occupation | Employed | 26 | 10 | 0.000 | 1.00 |
| Unemployed | 6 | 20 | 0.000 | 8.67(2.69-27.89) | |
| Student | 8 | 4 | 0.714 | 1.30(0.32-5.29) | |
| Farmer | 11 | 73 | 0.000 | 17.26(6.57-45.35) | |
| Business person | 3 | 11 | 0.003 | 9.53(2.19-41.47) | |
| Place of residence | Urban | 40 | 38 | 1.00 | |
| Rural | 14 | 80 | 0.000 | 6.02(2.93-12.37) | |
| Level of education | Illiterate | 11 | 64 | 0.000 | 26.18(8.79-78.00) |
| Elementary | 4 | 38 | 0.000 | 42.75(10.99-166.22) | |
| Secondary | 12 | 10 | 0.034 | 3.75(1.11-12.69) | |
| College/University | 27 | 6 | 0.000 | 1.00 | |
| Income status (Monthly income in Birr) | <500 | 11 | 59 | 0.000 | 13.71(5.02-37.41) |
| 500-1000 | 11 | 38 | 0.000 | 8.83(3.18-24.53) | |
| 1000-2000 | 9 | 12 | 0.038 | 3.41(1.07-10.85) | |
| >2000 | 23 | 9 | 0.000 | 1.00 | |
| Number of antihypertensive medication | 1 | 27 | 82 | 0.001 | 1.00 |
| 2 | 25 | 23 | 0.001 | 0.30(0.15-0.62) | |
| 3 | 2 | 13 | 0.336 | 2.14(0.45-10.09) | |
| Duration of treatments | <2 Years | 27 | 45 | 0.174 | 1.00 |
| 2-4 Years | 16 | 33 | 0.585 | 1.238(0.576-2.66) | |
| >5 Years | 11 | 40 | 0.062 | 2.18(0.96-4.96) | |
| Physical activity | Inactive | 12 | 51 | 0.000 | 7.44(2.88-19.19) |
| Minimally active | 21 | 55 | 0.001 | 4.58(1.92-10.93) | |
| Vigorously active | 21 | 12 | 0.000 | 1.00 | |
| Extra salt intake | Yes | 8 | 51 | 0.001 | 4.38(1.90-10.08) |
| No | 46 | 67 | 1.00 | ||
| Knowledge about hypertension and treatment | Yes | 41 | 19 | 1.00 | |
| No | 13 | 99 | 0.000 | 16.43(7.43-36.35) | |
| Cigarette smoking status | Yes | 6 | 18 | 0.469 | 1.44(0.54-3.86) |
| No | 48 | 100 | 1.00 | ||
Multivariable logistic regression have shown that variables such as age, level of education, monthly income status, duration of treatment, physical activity status and knowledge about hypertension and treatment were associated with non-adherence to antihypertensive medications. Factors like marital status, occupation, place of residence, number of antihypertensive medication and extra salt intake have shown significant association in bivariable analysis but the effect was absent after controlling for confounding factors (Table 5).
| Variables | Categories | P-value | AOR (95% CI) for Non-adherence status |
|---|---|---|---|
| Age | 18-34 | 0.075 | 1.00 |
| 35-54 | 0.255 | 0.34(0.05-2.21) | |
| > 55 | 0.035 | 0.10(0.01-0.85) | |
| Level of education | Illiterate | 0.049 | 6.76(1.01-45.08) |
| Elementary | 0.002 | 21.62(3.17-147.38) | |
| Secondary | 0.971 | 0.97(0.17-5.62) | |
| College/University | 0.007 | 1.00 | |
| Income status (Monthly income in Birr) | <500 | 0.011 | 18.51(1.95-176.06) |
| 500-1000 | 0.071 | 7.19(0.85-61.12) | |
| 1000-2000 | 0.401 | 2.52(0.29-21.71) | |
| >2000 | 0.031 | 1.00 | |
| Duration of treatments | <2 Years | 0.119 | 1.00 |
| 2-4 Years | 0.825 | 1.15(0.33-4.08) | |
| >5 Years | 0.041 | 5.41(1.08-27.22) | |
| Physical activity | Inactive | 0.001 | 34.51(4.66-255.89) |
| Minimally active | 0.005 | 8.49(1.91-37.84) | |
| Vigorously active | 0.002 | 1.00 | |
| Knowledge about hypertension and treatment | Yes | 0.000 | 1.00 |
| No | 7.67(2.48-23.73) |
4. DISCUSSION
Despite the availability of effective treatments, studies have shown that in many countries less than 25% of patients treated for hypertension achieve optimum blood pressure. Poor adherence has been identified as the main cause of failure to control hypertension [5]. In this study, only 31.4% of the study participants were adherent to their medication. This is comparable to studies reported from hospitals in Ghana and Nigeria 33.3%, Kenya 31.8%, Palestine 36.2%, Nepal 35.4% [17, 28-30]. When we compare the current finding to other studies done in Ethiopia, adherence to antihypertensive treatment was lower than studies done in University of Gondar Referral Hospital 64.6%, Black Lion Hospital 69.2%, Northern Ethiopia 52.9%, Adama Referral Hospital 59.5% [13-16]. Similarly the adherence to antihypertensive treatment found in current study was lower than studies done in Ghana 68.7%, Nigeria 44.7%, Zambia 83%, Malaysia 48.7%, Brazil 52.9%, Italy 48.6%, USA 57.6%, Pakistan 77%, United Arab Emirates 54.4% [12, 18-25]. The reason for the difference might be due to better access and skilled health care professionals for the patients in these regions and countries. It could also be due to participants’ better knowledge toward hypertension and its management than the current study area. The results of this study suggest that greater effort is needed to improve patient adherence to antihypertensive medications at Nedjo General Hospital. To improve adherence the following intervention should be done: education on the use of medicines, management of disease and treatment in conjunction with patients, adherence education, multidisciplinary care, training in monitoring adherence, more intensive intervention by increasing the number and duration of contacts [5]. In addition involving the patient's family members and friends in providing education on the importance of adherence to antihypertensive medications and telling them the consequences if the patient is not adherent to his medication should also be targeted/ adopted.
The results obtained from multivariable logistic regression analysis of the present study revealed that younger age, being illiterate, income status of <500 Ethiopian birr, duration of treatments of >5 years, physical inactivity and knowledge deficit about hypertension were associated with non-adherence.
In this study, age was significantly associated (p=0.035) with non-adherence observed in younger age. The present finding is consistent with that reported by other studies from Adama Referral Hospital [16], in hospitals of Ghana and Nigeria [17], Nigeria [18] and Pakistan [24]. A probable reason for better adherence in elderly might be because of a better care given by the family members for patients in this age group. The other reason could be patients with younger age could be reluctant for their medication. Older people might have more concern about their health than younger patients, so that older patients’ non-compliance is non-intentional in most cases. As a result, if they can get the necessary help from healthcare providers or family members, they may be more likely to be compliant with therapies [6].
Present study revealed that participants who were illiterate (p=0.049) and participants whom educational status was elementary (p=0.002) were significantly associated with non-adherence. Similar results were reported from studies in hospitals of Ghana and Nigeria [17], Zambia [19], Pakistan [24] and Nepal [30]. This could be due to lack of awareness about hypertension, its management and medications for this condition in this study area. It may be expected that patients with higher educational level should have better knowledge about the disease and therapy and therefore be more compliant [6]. To improve adherence in illiterate patients and patients with low level of education, interventions to optimize adherence must go beyond the provision of advice and prescriptions; supplementing oral teaching with written materials are required to improve adherence [5]. Using simple, everyday language, when explaining about the disease and giving instructions will also improve their adherence.
Different studies have identified inability to afford the cost of medications as an important barrier to medication adherence [14, 17, 24, 29]; however these studies did not show association of medication adherence with level of income. Unlike thus studies, this study showed an association between level of income and non-adherence (p=0.011) with non-adherence 18.51 times more likely to occur in patients with low income than higher income. The reason could be because of patients with low income cannot able to afford the cost of medication.
In this study, duration of treatment was significantly associated (p=0.041) with non-adherence and patients on hypertension treatment for more than or equal to five years were 5.41 times more likely to be non-adherent than those with duration of treatments of less than two years. Similar finding was reported from study done in Black Lion Hospital [14]. This could be because long use of drugs would burden the patient and lead to forget their medication and discontinue medication too soon. Beside once the patient blood pressure had got stabilized they might felt to be in better condition.
A study done in Nigeria [27] revealed that exercise is a facilitator for adherence to antihypertensive medication. The result of present study showed that, physical inactivity was significantly associated (p=0.001) with non-adherence. Physicians should help patients find an activity that they enjoy, because enjoyment will increase their adherence [31].
In this study, lack of knowledge about hypertension and its treatment was significantly associated with non-adherence. The present finding is consistent with that reported by other studies from University of Gondar Referral Hospital [13], Adama Referral Hospital [16], in hospitals of Ghana and Nigeria [17], Pakistan [24], United Arab Emirates [25] and Congo [32]. Right knowledge about HTN and its treatment creates a clear understanding and avoids confusion about the treatment and the disease condition [5].
The present study revealed that the major reasons for non-adherence were forgetfulness followed by inability to buy medications. To improve non adherence related to forgetfulness we recommend the patients to use medication boxes with dates/times written on them (“Pill organizers”) or setting an alarm clock. For patients with lack of finance, we recommend the government to find a means in which patients with lack of finance that cannot afford the cost of medication can get the medications; for example providing medications for free for patients that cannot afford the cost of medication, creating drug discount cards that can be helpful to patients who can afford to pay part of their prescription costs.
Strengths of our study were that adherence to antihypertensive medications was measured by using the 8-item Morisky medication adherence scale and data were collected from patients’ card and by face to face interview with patients; this helped us to have more complete information. Limitations of our study were that, this study was conducted only in government District Hospitals in Nedjo Town and did not include patients who attended private Hospitals. Therefore results cannot be generalized to all hypertension patients in Nedjo woreda. However, the results have important insights for same hospitals within the same characteristics. Self-reporting was used for measuring adherence. This method has the disadvantages of recall bias and eliciting only socially acceptable responses and hence, may, lead to overestimation of some of the results, because they are self- reports by the patients which can be misleading.
CONCLUSION
In general, a finding of this study revealed that an adherence status of study participants was low. Thus greater effort is needed to improve patient adherence to antihypertensive medications. The major reasons for non-adherence among the study participants were forgetfulness, followed by inability to buy medications. Factors such as age, educational level, income status, duration of treatments, physical activity and knowledge deficit about hypertension and its treatment were significantly associated with non-adherence. We recommend that practitioners should always look for poor adherence and enhance adherence by emphasizing the value of a patient’s regimen, making the regimen simple, and customizing the regimen to the patient’s lifestyle. Health care professionals should assist hypertensive patients develop systems that will remind them to take their medications. There should be total collaboration between all the health professionals in the institution to promote patient education and medication counseling.
ETHICS APPROVAL AND CONSENT TO PARTCIPATE
Ethical clearance was obtained from the Ethical Review Committee of Wollega University, College of Medical and Health Sciences. This committee wrote a formal letter of permission to Nedjo General Hospital to seek its cooperation and access to the data. Permission was obtained from the medical director’s office of the hospital.
HUMAN AND ANIMAL RIGHTS
No Animals were used in this research. All human research procedures followed were approved by the Ethical Review Committee of Wollega University.
CONSENT FOR PUBLICATION
After obtaining the required permission from the hospital, patient’s written informed consent was obtained after explaining about the purpose and procedures of the study. Patients were expected to be fully voluntary to participate in the study. In addition all the responses were kept confidential.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
We are grateful to the department of pharmacy, Wollega University for their unreserved cooperation in making this study to be a fruitful work. We are also thankful for the outpatient department nurses of Nedjo General Hospital for their cooperation in collecting the data and the patients who willingly participate in this study.

