

RESEARCH ARTICLE
Distal Forearm Bone Mineral Density Among Hill Tribes in the Omkoi District, Chiang Mai Province, Thailand
Sompong Sriburee, Montree Tungjai, Suratchanee Padngam, Tarika Thumvijit, Pongsiri Hongsriti, Monruedee Tapanya, Utumma Maghanemi, Kwanchai Ratanasthien, Suchart Kothan*
Article Information

Identifiers and Pagination:
Year: 2019Volume: 12
First Page: 1
Last Page: 6
Publisher ID: TOPHJ-12-1
DOI: 10.2174/1874944501912010001
Article History:
Received Date: 9/9/2018Revision Received Date: 24/12/2018
Acceptance Date: 10/1/2019
Electronic publication date: 29/1/2019
Collection year: 2019

open-access license: This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International Public License (CC-BY 4.0), a copy of which is available at: (https://creativecommons.org/licenses/by/4.0/legalcode). This license permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Background:
Osteoporosis is a major public health issue in several countries worldwide because it increases healthcare costs, and is a risk for mortality. There have been several studies that have examined BMD among the various Thai people and the regions that they inhabit.
Objective:
This study examined the distal forearm Bone Mineral Density (BMD) in men and women over 40 years of age among members of various Karen hill-tribes located in the Omkoi District, Chiang Mai Province, Thailand.
Methods:
Two hundred and sixty-two subjects (180 women, 82 men), ranging from 40 to 83 years old were recruited in this study. The non-dominant distal forearm bone mineral density was assessed by using peripheral dual-energy X-ray absorptiometry (pDEXA).
Results:
The results showed that the BMD were 0.530 ± 0.065, 0.508 ± 0.087, 0.461 ± 0.098, and 0.438 ± 0.124 g/cm2 for men age 40-49 years, age 50-59 years, age 60-69 years, and ages 70-83 years, respectively. For women, the BMD were 0.392 ± 0.051, 0.337 ± 0.063, 0.232 ± 0.065, and 0.212 ± 0.069 g/cm2 among women age 40-49 years, age 50-59 years, age 60-69 years, and ages 70-83 years, respectively. BMD had decreased in post-menopause as a function of duration time after menopause.
Conclusion:
We determined the prevalence of osteoporosis of men and women of Karen hill-tribes in the Chiang Mai Province, Thailand. These findings provided important information regarding bone health in Karen hill-tribes for any healthcare planning done in the immediate future.
1. INTRODUCTION
Osteoporosis is a major public health issue in several countries worldwide because it increases healthcare costs, and is a risk for mortality [1-5]. This disease is characterized by Bone Mineral Density (BMD) and bone architecture data. Osteoporosis is associated with increased risks of bone fracture. Common fracture sites include the spine, and forearm [6-8]. The disease has no symptoms until complications due to fracture occur. Thus, BMD measurement is important for osteoporosis prevention. BMD is strongly related to many factors such as ethnicity, body mass index, age, sex, physical activity, previous fracture history, parental fracture history, alcohol and tobacco use, arthritis, and lifestyle [9-12]. These factors may change considerably between different areas within the same country. There have been several studies that have examined BMD among the various Thai peoples and the regions that they inhabit [13-18]. The findings of this research support the hypothesis that different demographic characteristics can impact BMD within the same country. It is noteworthy that subjects of this former research were chosen from urban areas. In contrast, this present study collected subjects from rural mountainous areas surrounding Chiang Mai, Thailand. In our study, the distal forearm bone mineral density among men and women over 40 years of age of Karen hill-tribes in the Omkoi District, Chiang Mai Province, Thailand was investigated by using peripheral dual-energy X-ray absorptiometry. Karen hill-tribe people inhabit the mountainous areas surrounding Chiang Mai.
2. MATERIALS AND METHODS
The present study was a retrospective study that was carried out by examining the demographic characteristic information and BMD data obtained from the Community Services Project at Omkoi District, Chiang Mai Province, Thailand. All procedures were approved by the Ethics Committee of the Faculty of Associated Medical Sciences, Chiang Mai University, Chiang Mai, Thailand.
2.1. Subjects and Demographic Characteristic Information
Two hundred and sixty-two subjects (180 women, 82 men) from Karen hill-tribes, 40-83 years of age, from the Omkoi District, Chiang Mai Province, Thailand were recruited for this study. Subjects were recruited through advertisements in Omkoi District area such as village, and community. The Omkoi District is located about 179 km southwest of Chiang Mai city. Demographic characteristics information was obtained by self-administered questionnaires. The questions related to risk factors for osteoporosis determined the following information: Age, height, weight, parent’s history of osteoporosis, parent’s history of spinal deformity, coffee/tea intake, alcohol intake, smoking, milk intake, eating habits (fish, beans, and vegetable), and exercise. Body Mass Index (BMI) was calculated from weight (kg) and height (m) by using the following equation: BMI = kg/m2. The subject’s demographic characteristics information is summarized in Tables 1 and 2.
| Variables | Age Groups (Men) | |||
|---|---|---|---|---|
| 40-49 years | 50-59 years | 60-69 years | 70-83 years | |
| Age | 45.47 ± 2.64 | 55.44 ± 2.98 | 64.44 ± 3.18 | 74.40 ± 3.02 |
| Weight (kg) | 56.73 ± 6.51 | 58.54 ± 10.70 | 53.42 ± 11.16 | 52.73 ± 8.42 |
| Height (cm) | 163.47 ± 4.81 | 163.33 ± 5.48 | 159.08 ± 6.25 *,** | 161.17 ± 5.81 |
| BMI (kg/m2) | 21.25 ± 2.43 | 21.88 ± 3.48 | 20.99 ± 3.56 | 20.32 ± 3.23 |
| Variables | Age Groups (Women) | |||
| 40-49 years | 50-59 years | 60-69 years | 70-83 years | |
| Age | 45.42 ± 2.71 | 54.53 ± 2.90 | 63.47 ± 2.65 | 77.28 ± 3.83 |
| Weight (kg) | 60.92 ± 10.89 | 57.19 ± 10.99 | 52.68 ± 8.77 | 47.67 ± 13.00 |
| Height (cm) | 153.60 ± 4.80 | 152.56 ± 4.86 | 151.79 ± 5.13 | 149.02 ± 5.29 *,** |
| BMI (kg/m2) | 25.77 ± 4.12 | 24.51 ± 4.27 | 22.88 ± 3.75 * | 21.43 ± 5.80 *,** |
| Risk factors | Prevalence (%) | |
|---|---|---|
| Men | Women | |
| Parent history of osteoporosis or low-trauma fractures | 10.98 | 13.33 |
| Parent history of spinal deformity | 17.07 | 8.94 |
| Coffee/tea intake | 84.15 | 34.64 |
| Alcohol intake | 39.02 | 9.44 |
| Smoking | 63.41 | 32.96 |
| Milk intake | 43.90 | 65.00 |
| Eating habits (fish, beans, and vegetable) | 93.90 | 98.33 |
| Exercise | 68.29 | 58.33 |
| Menopause | - | 71.67 |
| Men | ||||
|---|---|---|---|---|
| Variables | Age Groups | |||
| 40-49 years (n =15) |
50-59 years (n =27) |
60-69 years (n= 20) |
70-83 years (n =14) |
|
| BMD, (g/cm2) | 0.530 ± 0.065 | 0.508 ± 0.087 | 0.461 ± 0.098 | 0.438 ± 0.124 |
| T-score | -0.857 ± 1.088 | -1.212 ± 1.448 | -2.001 ± 1.630 | -2.376 ± 2.064 |
| Women | ||||
| Variables | Age Groups | |||
| 40-49 years (n=55) |
50-59 years (n=62) |
60-69 years (n=34) |
70-83 years (n=29) |
|
| BMD, (g/cm2) | 0.392 ± 0.051 | 0.337 ± 0.063 | 0.232 ± 0.065 | 0.212 ± 0.069 |
| T-score | -1.414 ± 0.853 | -2.330 ± 1.049 | -4.091 ± 1.069 | -4.408 ± 1.151 |
2.2. BMD at Distal Forearm Measurement
The BMD of a non-dominant distal forearm of all subjects was measured using peripheral dual-energy X-ray absorptiometry (pDEXA) scan (EXA 3000; Osteosys Corp, Seoul, Korea) according to standard protocol. All subjects were requested to remove all items (e.g. bracelet, wristwatch, etc.) from their non-dominant distal forearm before being measured for BMD at distal forearm. All subjects were asked to place their non-dominant distal forearm into a lateral position between the X-ray source and detector of the pDEXA machine. The results of BMD measurements were grouped into three categories based on the World Health Organization (WHO) guidelines. These three categories are normal bone mass (T-score ≥ -1), low bone mass or osteopenia (T-score between -1 and - 2.5), and osteoporosis (T-score≤ -2.5) [19, 20].
2.3. Statistical Analysis
All data were analyzed using a Microsoft Excel 2010 program for Windows and Origin 8.0 software (Origin-Lab, Northampton, MA, USA). The results of the statistical analysis were expressed as mean values ± standard deviation. The student t-test was used to compare the mean between these two groups. Linear correlation analysis was carried out using a Pearson correlation. A p value of < 0.05 was considered as statistically significant.
3. RESULTS
The demographic characteristics information is shown in Table 1. The variables including height, weight, and Body Mass Index (BMI) were compared among the various age groups. For men, the heights of the 60-69 years old group were statistically significantly different (p< 0.05) than that of the 40-49 years old group. For women, the weight and BMI of the 70-83 years group were statistically significantly different (p<0.05) from the 40-49 and 50-59 years groups. The 60-69 years group were statistically significantly different (p<0.05) from the 40-49 years groups, as well.
Table 3 shows the age-group distal forearm BMD and T-scores. For men, the BMD was the highest in the 40-49-year age-group and lowest in the 60-69 and 70-83 year age-group. The average T-score at the distal forearm was also highest in the 40-49-year age-group and lowest in the 60-69 and 70-83 year age-group. For women, the BMD was the highest in the 40-49-year age-group and lowest in the 70-83 year age-group. The average T-score at the distal forearm was also highest in the 40-49-year age-group and lowest in the 70-83 year age-group.
The BMD at distal forearm plotted against the age of men and women is shown in Figs. (1 and 2), respectively. The BMD at distal forearm of both men and women decreased as a function of age (p<0.05, r = -0.41 for men and p<0.05, r = -0.72 for women).
The percentage of prevalence osteopenia and osteoporosis of men and women is shown in Figs. (3 and 4), respectively. The percentage of osteopenia and osteoporosis increases as a function of age in both men and women, while normal bone density had decreased in that same category.
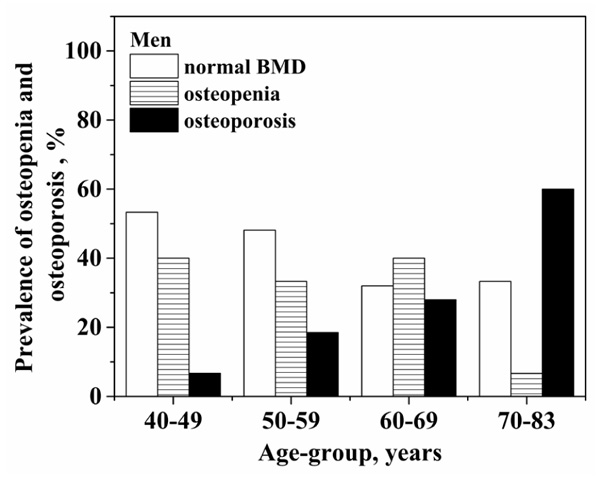 |
Fig. (1). BMD at distal forearm plotted against age of men. |
 |
Fig. (2). BMD at distal forearm plotted against age of women. |
 |
Fig. (3). The percentage of prevalence osteopenia and osteoporosis of men. |
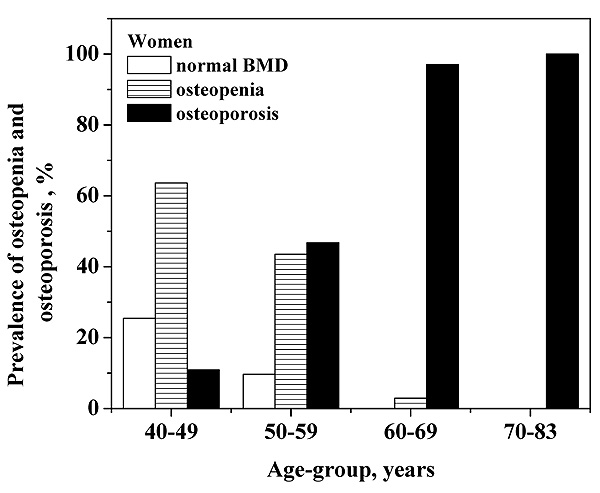 |
Fig. (4). The percentage of prevalence osteopenia and osteoporosis of women. |
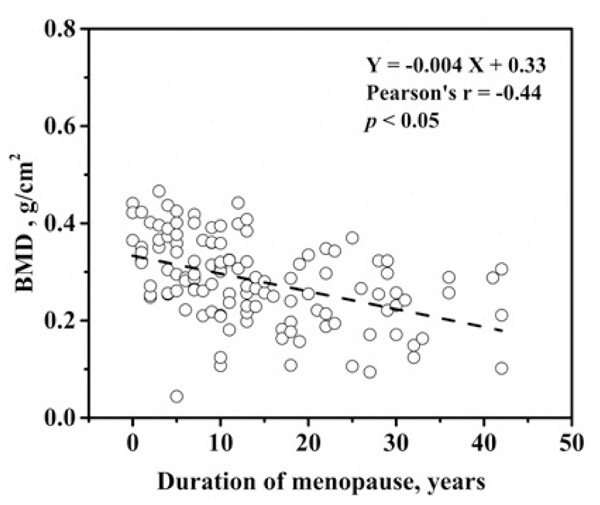 |
Fig. (5). BMD at distal forearm plotted against duration of menopause of women. |
In addition, the BMD of distal forearm plotted against duration of menopause of women is shown in (Fig. 5). The BMD at distal forearm decreased when the duration of menopause increased (p<0.05, r = -0.44).
4. DISCUSSION
Osteoporosis is a common health problem in Thailand. It is characterized by deficits in Bone Mineral Density (BMD) and micro-architectural deterioration that can result in an increase in bone fragility and fractures [13, 17]. The prevalence of BMD and osteoporosis in men and women are still being studied. When comparing the BMD at distal forearm of each age-group, the BMD was found to be higher in men. Moreover, the BMD at distal forearm of both men and women decreased with advanced aging. In contrast, a previous study showed that the BMD at distal forearm (radius) of women significantly decreased when age-group increased, but the BMD at distal forearm (radius) of men did not change when age-group had increased [21]. However, the BMD at distal forearm of each age-group of men was higher than that of each age-group of women; and these results were similar to our findings.
A previous study conducted on the bone mineral density at distal forearm in men over 40 years of age in Mae Chaem district, Chiang Mai Province, Thailand showed that BMD in Thai men aged 40-49, 50-59, 60-69, and 70-87 years were 0.571 ± 0.071, 0.560 ± 0.075, 0.500 ± 0.126 and 0.418 ± 0.093 g/cm2, respectively [13]. In this present study, the results showed that the BMD were 0.530 ± 0.065, 0.508 ± 0.087, 0.461 ± 0.098, and 0.438 ± 0.124 g/cm2 for men ages 40-49, 50-59, 60-69, and 70-83 years. The average BMD of men who resided in the Omkoi District was lower than that of men who resided in Mae Chaem District. The risk factors for osteoporosis in both the Omkoi District and Mae Chaem District were evaluated. We found that the percentages of each risk factor were rather different between these two districts.
In addition, another previous study showed that BMD at distal forearm (radius) of men who resided in Muang District, Khon Kaen Province, Thailand were 0.42 ± 0.04, 0.40 ± 0.05, 0.36 ± 0.06, and 0.35 ± 0.07 g/cm2 for ages 40-49, 50-59, 60-69 and over 70 years of age, respectively. The BMD at distal forearm of women were 0.34 ± 0.05, 0.30 ±0.05, 0.25 ±0.05, and 0.21± 0.05 g/cm2 for ages 40-49, 50-59, 60-69, and over 70 years of age [22]. The BMD at distal forearm of men was lower than those determined in this present study. In the present study, BMD at distal forearm of women were 0.392 ± 0.051, 0.337 ± 0.063, 0.232 ± 0.065, and 0.212 ± 0.069 g/cm2 for ages 40-49, 50-59, 60-69, and 70-83 years. The average BMD of women age 40-49 years and ages 50-59 years who resided in the Omkoi District of Chiang Mai was rather higher than that of women age 40-49 years and age 50-59 years who resided in the Muang District, Khon Kaen Province. It seems reasonable that if each population had differences in demographic characteristics, then the BMD at distal forearm of each population would likely not be the same.
In post-menopause northern Thai women, BMD at distal forearm (1/3 radius) was 0.600 ± 0.086 g/cm2 [17]. The BMD at distal forearm of post-menopause in this present study was 0.284 ± 0.087 g/cm2. The average BMD of post-menopause women in this present study was lower than those of previous studies done at two separate times. The relationship between menopausal duration and BMD in the present study was in agreement with other studies [7, 22].
There was a positive correlation with the BMD found from various skeletal sites (i.e.; the lumbar spine, prox-imal femur, and 1/3 radius) in northern Thai women [17]. Thus, it was determined that the BMD of distal forearm in men and women decreased as a function of age (Figs. 1 and 2). The BMD of other skeletal sites involving the lumbar spine and proximal femur should have decreased as a function of age, as well. It is noteworthy that the nondominant distal forearm bone mineral density might be useful for BMD screening in people who reside in areas that are difficult to access for whole body BMD examinations such as the Omkoi District because distal forearm bone mineral density is correlated with BMD from various skeletal remains; as mentioned earlier.
The prevalence of osteoporosis of men and women in this present study increased as a function of age-group as indicated by other studies [13, 23-25]. Of note, the prevalence of osteopenia of men aged 70-83 years had decreased compared to other age-groups because the number of subjects in age 70-83 years was small.
Notable strength in this present study is that our subjects were Karen hill-tribe people, a member of an indigenous people that inhabits mountainous areas. This makes it notably different from other studies done on the BMD of Thai people [14, 18]. The lifestyles and culture of Karen hill-tribe people is quite different from urban populations. In addition, these results can be used as information on any large-scale bone mineral density studies of Karen hill-tribes at Omkoi District done in the future. However, a limitation of this present study was that the number of our subjects was rather small. Additionally, the questionnaires that asked about past history possibly resulted in some recall bias information, especially in older people. Also, some subjects may have not communicated their responses correctly. Additional information regarding biochemical bone turnover marker [9, 15] that is related to BMD might be needed, as well.
CONCLUSION
It is important to note that the results in this present study supported the hypothesis that different demographic characteristics can impact BMD in both men and women, even though these various groups reside in the same country. In summary, our study provided the demographic characteristics related to the distal forearm BMD, and we found a prevalence of osteopenia and osteoporosis in both men and women in the Karen hill-tribes of the Omkoi District, Chiang Mai Province, Thailand.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
All procedures were approved by the Ethics Com-mittee of the Faculty of Associated Medical Sciences, Chiang Mai University, Chiang Mai, Thailand.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2008 (http://www.wma.net/en/20activities/10ethics/10helsinki/).
CONSENT FOR PUBLICATION
Written informed consent was obtained from all the participants prior to publication.
CONFLICT OF INTEREST
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
ACKNOWLEDGEMENTS
We are thankful for the support we received from the Ban Yang Poa School, Omkoi District, Chiang Mai Province, Thailand. We also want to thank all the staff and students who participated in this study.




