All published articles of this journal are available on ScienceDirect.

Determinants of Health Literacy and Healthy Lifestyle against Metabolic Syndrome among Major Ethnic Groups of Sarawak, Malaysia: A Multi-Group Path Analysis
Abstract
Introduction:
Non-communicable diseases like metabolic syndrome can be prevented and controlled by practicing healthy lifestyle.
Although health literacy is a critical factor in lifestyle modification to prevent non-communicable diseases and its complications, its role on metabolic syndrome prevention is still understudied.
Objective:
The main aim of this study was to identify the determinants of health literacy and healthy lifestyle practice against metabolic syndrome among multi-ethnic group of Sarawak based on health literacy skills framework.
Methods:
Using a stratified multistage sampling, a total of 1006 respondents were recruited to represent the major ethnic groups in Sarawak, Malaysia. Moderator variables, mediator variables and outcome variable (healthy lifestyle practice) were tested using path analysis to examine multiple and interrelated dependence relationships. Multi-group analysis was performed to compare structural models between major ethnic groups in Sarawak, namely Malay/Melanau, Native groups and Chinese.
Results:
Female respondents and those with higher education status were more likely to have better healthy lifestyle practice. Greater level of health literacy was positively significant with both disease knowledge and healthy lifestyle practice. Participants with good understanding of disease knowledge can directly influence healthy lifestyle. Simultaneously, health literacy and metabolic syndrome knowledge can mediate the relationship between sociodemographic variables, service accessibility, medical and family history with practice of healthy lifestyle. Multi-group path analysis indicated differences in causal pathway leading to healthy lifestyle practice among the ethnic groups.
Conclusion:
Health programs or interventions to increase health literacy skills and better understanding of metabolic syndrome will improve practice of healthy lifestyle. Culturally sensitive multidimensional approaches are needed to ensure health-related information can be delivered effectively across the state.
1. INTRODUCTION
The burden of Non-Communicable Diseases (NCD) is rising due to their risk factors. Sedentary lifestyle behaviours such as physically inactive, unhealthy food intake, alcohol consumption and use of tobacco products are the known risk factors. The World Health Organization stated that in 2016, more than 2/3 (40.5 million) deaths were contributed by non-communicable diseases [1]. Metabolic syndrome is a clustering of at least 3 to 5 diseases which are associated with the risk of developing type II diabetes and cardiovascular disease [2]. A secdentary lifestyle has been established as the main culprit [3, 4].Presently, people are more inclined towards unhealthy lifestyles, which contributed to the rise in the prevalence of metabolic syndrome globally [5, 6]. National Health Morbidity Survey Malaysia (NHMS) reported a worrying trend of unhealthy lifestyle practice among the general population of Malaysia [7]. The survey findings of the Department of Statistics, Malaysia reported ischemic heart disease as the principal cause of death regardless of ethnicity and gender among Malaysian population in 2017, [8]. In the early years, most of the models that describe health literacy were in the context of individual health literacy level. Freedman et al. (2009) in their article Public Health Literacy Defined discussed about the importance of public health literacy and how it is also vital to focus on primary prevention of diseases rather than just on the secondary and tertiary prevention [9]. Health or disease knowledge means information, facts, and skills developed throughout the course of life either via experience or education [10]. It allows us to have a greater understanding of health-related matters. Nutbeam (2000) proposed a model of health literacy which consists of three levels [11]. Firstly, the functional health literacy requires a person to possess a basic skill in reading and writing. This is the basic stage of health literacy and its assessment involves tools such as printed health materials or documents. The second level, communicative health literacy, requires more advanced skills than the functional components as it is necessary to extract information and applying it depending on the situations. In the meantime, the third level of critical health literacy is a skill that enables us to analyse health information critically and applying it to employ a better control of any situation. Prevention of Metabolic syndrome, like other similar chronic diseases, has been proven to be effective with the intervention on nutritional intake, promotion of physical activity, psychosocial care and education. The objective of this study was to identify the determinants of healthy lifestyle practices against metabolic syndrome among the multi-ethnic population of Sarawak, Malaysia. we studied the relationship between sociodemographic characteristics, service factor, medical history, health literacy and metabolic syndrome knowledge using path analysis to determine the causal pathway which contributed to healthy lifestyle practice. The following hypotheses were tested: (1) The level of health literacy will influence the practice of healthy lifestyle. (2) Disease knowledge can mediate health literacy and practice of healthy lifestyle to prevent metabolic syndrome.
2. MATERIALS AND METHODS
2.1. Development of the Model
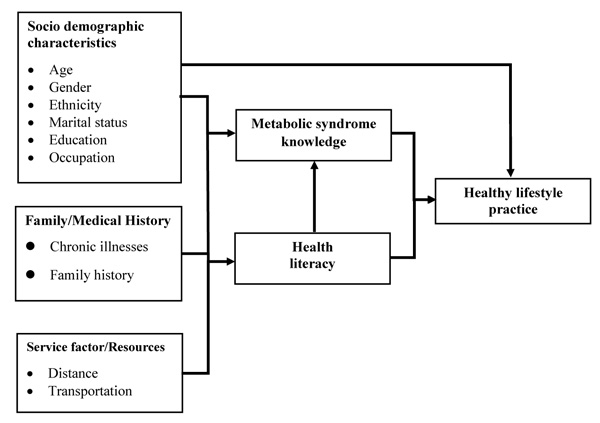
Reference was made to the conceptual model on health literacy skills framework [12]. The principle of the model indicates the competencies related to the process of accessing, understanding, appraising and applying health-related information. In this case, health-related information was specifically based on metabolic syndrome. Health literacy component was based on Nutbeam (2000) theory of health literacy. This model demonstrates the relationship between determinants and preventive care of metabolic syndrome with health literacy and knowledge as a potential mediator. Existing evidence also suggested that variables such as age and gender have a strong direct and moderation effect on healthy lifestyle practice [13, 14]. Thus, a direct arrow was added linking socio-demographic construct and healthy lifestyle practice (Fig. 1).
2.2. Sample and Procedure
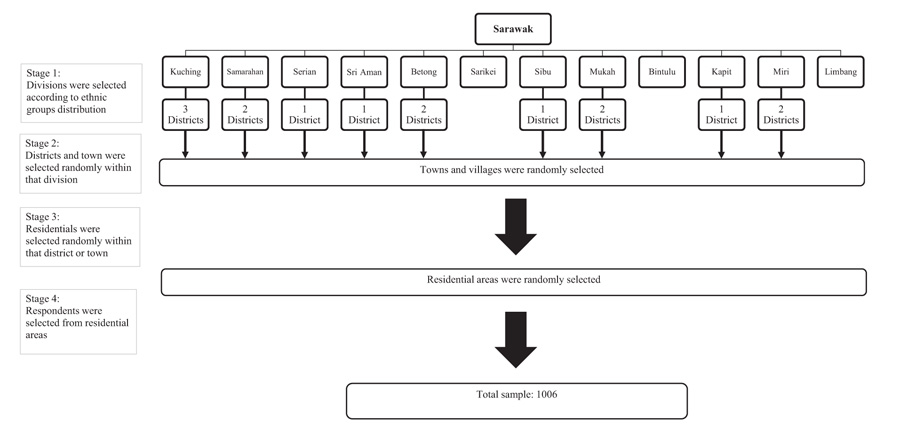
Study participants were citizens of Sarawak, which is one of the fourteen states of Malaysia. This is the largest state of Malaysia which consists of numerous major ethnic groups. This project was carried out between April 2017 and October 2018 (488 days). The respondents were 18 years old and above and recruited from the whole state through stratified multistage sampling. Medical and health personnel were excluded from these cross-sectional population surveys. The estimated sample size was 1200 calculated based on the prevalence of adequate physical activity in Sarawak (59.2%) from the National Health Morbidity Survey Malaysia in 2015 [7]. A total of 1119 respondents were recruited with response rate of 93.3%. After data cleaning and missing data analysis, a total of 1006 subjects were included for analysis. The state of Sarawak, located in the third largest island in the world, Borneo is divided into 12 divisions. It is known to have an ethnically diverse population. Multistage stratified sampling technique was used to select divisions and districts for data collection (Fig. 2).
2.3. Measures
Interviewer-assisted questionnaire was used. The first part of the questionnaire assessed socio-demographic variables and past medical illness. For health literacy, a three-level health literacy model was developed by Suka et al. (2013) which included five items for functional HL, five items for communicative HL, and four items for critical HL [15]. Participants were required to rate each item on a 5-point Likert scale ranging from 1(strongly disagree) to 5 (strongly agree). Reversed scoring was required for functional health literacy component. Total scores of health literacy were calculated and higher scores signify better health literacy. Disease knowledge section consisting of 20 questions focused on metabolic syndrome. For every question, the respondents were required to select one correct answer out of 3 options (True, False or Don’t Know). Metabolic syndrome knowledge was assessed based on a 3 points likert scale (True, False or Don’t Know) questionnaire adopted from Yahia N. et al. (2014) [16]. A total of 20 questions focused on risk factors, complications and prognosis of metabolic syndrome. Simple Lifestyle Indicator Questionnaire (SLIQ), developed by Godwin et al. (2008) was used to assess healthy lifestyle practices on non-communicable diseases [17]. In total, there were five constructs: Diet (3 questions), activity (3 questions), alcohol consumption (3 questions), smoking (2 questions), and stress (1 question). Subsequently, a raw score was obtained for every construct. Overall SLIQ scores ranged from 0 to 10. The higher the score, the healthier the lifestyle.
*Ethnicity was used as a reference point for multi-group analysis
2.4. Statistical Analysis
Data were assessed using the Statistical Package for Social Science (SPSS) IBM version 23. All the data were thoroughly checked and cleaned prior to analysis. Missing data analysis was performed to identify the percentage of missing data for all the variables and items. Prior to major analysis, outliers were removed. Once outliers were detected, they were first checked for coding errors. Descriptive statistics was used to describe the fundamental features of the data in this study. It provides simple summaries about the sample and the measures such as percentage and mean scores with standard deviation. Pearson correlation was run to determine the relationship between health literacy and preventive lifestyle practice. Independent t-test and one-way ANOVA were used to detect differences between the healthy lifestyle practice across the socio-demographic variables. For analysis involving ANOVA, Bonferroni adjustment was used. For every analysis, the significance level was set at 0.05.
2.5. Data Modelling
The main purpose of path analysis in this study was to examine multiple and interrelated dependence relationships [18]. Amos software version 23 was used to run the maximum likelihood to obtain an estimation of the coefficient. Firstly, the correlations of the main study variables were examined. Gender, education, chronic illness, family history of ischemic heart disease and distance of health care facilities were dummy coded. Subsequently, path analysis was conducted to test the associations between socio-demographic variables, health literacy, health knowledge and healthy lifestyle practice. In the presence of non-normality, bootstrapping was performed as a remedy. Bootstrapping analyses were done by replicating 3000 samples to obtain reliable 95% confidence intervals of not normally distributed parameters [19] Subsequently, a multi-group analysis was conducted and the respondents were stratified into 3 groups, namely Malay/Melanau, Native and Chinese. For model fit, the Comparative Fit Index (CFI), Adjusted Goodness-of-Fit Index (AGFI), Root-Mean-Squared Error of Approximation (RMSEA), (TLI) and chi-square statistics were generated. The cut-off point was 0.07 and below for RMSEA [20], and 0.90 and above for AGFI, TLI and CFI [21, 22]. The acceptable range for CMIN/df was 1 – 5. The chi-square statistics was generated by bootstrapping sampling distribution and Bollen-Stine statistics [23].
2.6. Ethical Consideration
Medical Research Ethics Committee of Universiti Malaysia Sarawak (UNIMAS) granted approval to conduct this research. Respondents were briefed about this project and participation was voluntary. Formal written consent was obtained, and confidentiality of information was assured.
3. RESULTS
3.1. Respondents’ Characteristics
The age range of our respondents was 18 to 93 years old with the mean age of 36.8 (14.53) years (Table 1). Majority of the respondents were married and obtained a secondary education. Out of 1006 respondents, the majority were employed, living within 5 to 10 km from the nearest health care facilities and without any chronic illnesses. In term of ethnic group distribution, 16.9% of them were Malays, 18.9% were Ibans, 19.1% from the Chinese ethnic group, 16.4% were Melanau, 15.6% were Bidayuh and Orang Ulu were13.1%. Prior to performing path analysis, a correlation among the variables was tested. Table 2 shows correlations between sociodemographic variables, health literacy components, metabolic syndrome knowledge and healthy lifestyle practices. Healthy lifestyle practice was positively correlated with gender, health literacy and metabolic syndrome knowledge. Advancement in age decreased healthy lifestyle practice. The ethnic groups were categorised into Malay/Melanau, Native and Chinese for multi-group analysis.
3.2. Path Analysis
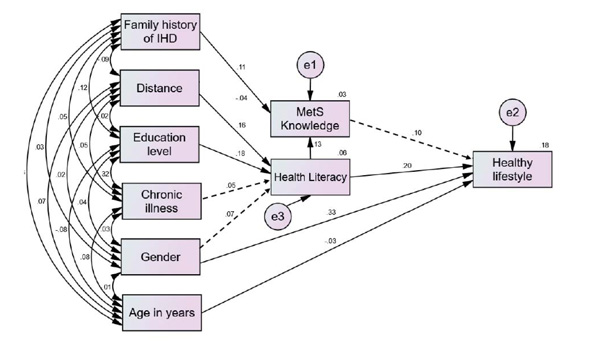
A final path model was constructed after the removal of non-significant constructs and mediation analysis. Overall, the constructs accounted for 11 percent of the total variance in healthy lifestyle practice among the population of Sarawak (Fig. 3). As shown in Table 3, Gender directly influenced healthy lifestyle practice. Female respondents were more likely to practice better lifestyle behaviours compared to the male respondents we (beta = 0.277, 95% CI: 0.229 - 0.324, p = 0.002). Younger respondents reported to have better healthy lifestyle practice than older respondents (beta= -0.071, 95% CI: -0.119, -0.019, p =0.019). Service factor, the distance of nearest health care facilities also significantly affected health knowledge level. Individual who were living nearer to health care facilities (within 5km radius) reported to have better metabolic syndrome knowledge compared to those staying more than the 5km radius from the nearest health care facilities (beta= 0.085, 95% CI: 0.031 - 0.138, p = 0.010). Respondents who lived more than 5km from the health care facility reported to have better health literacy status compared to those who lived nearer to the health care facility. Respondents with chronic illnesses were more likely to have a higher level of metabolic syndrome knowledge. (beta= 0.087, 95% CI: 0.041 - 0.140, p = 0.003). Metabolic syndrome knowledge was reported to be positively significant with the practise of healthy lifestyle (beta= 0.080, 95% CI: 0.021- 0.139, p = 0.037).
| Characteristics | Frequency (%) |
Healthy Lifestyle Practice, Mean (SD) |
p value |
|---|---|---|---|
|
Age Young adults [18 – 25] Adulthood [26 – 40] Middle age [41 – 60] Elderly [>60] Mean (SD) |
281(28) 369(37) 278(28) 78(8) 36.8(14.53) |
7.5(1.33) 7.4(1.35) 7.1(1.45) 7.1(1.46) |
0.023 |
|
Gender Male Female |
461(46) 545(54) |
6.9(1.49) 7.7(1.18) |
<0.001 |
|
Marital status Married Unmarried |
658(65) 348(35) |
7.3(1.41) 7.3(1.35) |
0.574 |
|
Education Primary and lower Secondary Higher |
245(24) 575(57) 186(19) |
7.2(1.47) 7.3(1.37) 7.5(7.34) |
0.057 |
|
Employment Employed Unemployed Housewives |
717(71) 98(10) 191(19) |
7.2(1.44) 7.5(1.40) 7.5(1.15) |
0.089 |
|
Ethnicity Malay/Melanau Natives Chinese |
335(33) 479(48) 192(19) |
7.3(1.40) 7.3(1.45) 7.3(1.21) |
0.816 |
|
Distance to health care facilities Within 5km More than 5km |
327(33) 366(36) |
7.3(1.42) 7.3(1.38) |
0.903 |
|
Chronic illnesses Yes No |
324(32) 682(68) |
7.2(1.39) 7.3(1.39) |
0.366 |
|
First degree relative with history of heart disease Yes No |
260(26) 746(74) |
7.3(1.40) 7.3(1.36) |
0.981 |
Dummy coding:
Gender: male=0, female= 1
Education: primary and below= 0, Secondary and above= 1
Distance: less than 5 km= 0, more than 5 km = 1
Chronic illness, family history of IHD: no= 0, yes= 1
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
|---|---|---|---|---|---|---|---|---|---|
| Age | 1.00 | - | - | - | - | - | - | - | - |
| Gender | -0.076* | 1.000 | - | - | - | - | - | - | - |
| Family history of IHD | 0.016 | 0.010 | 1.000 | - | - | - | - | - | - |
| Distance | 0.026 | -0.029 | -0.029 | -0.029 | - | - | - | - | - |
| Chronic Illness | 0.076* | -0.019 | 0.098* | 0.042 | 1.000 | - | - | - | - |
| Education | 0.047 | -0.006 | 0.049 | -0.062* | -0.253* | 1.000 | - | - | - |
| Health Literacy | 0.010 | 0.066* | 0.015* | 0.062 | 0.028 | 0.147** | 1.000 | - | - |
| MetS Knowledge | -0.001 | 0.018* | 0.070 | -0.068* | 0.009 | 0.042** | 0.223* | 1.00 | - |
| Healthy Lifestyle | -0.091* | 0.292* | 0.012 | 0.011 | 0.007 | 0.012 | 0.130* | 0.118* | 1.00 |
| Parameters | Unstandardized | SE | Standardized Estimate | 95% CI | P-value | ||
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| Health literacy | Education | 3.089 | 0.584 | 0.170 | 0.115 | 0.222 | 0.001 |
| Health literacy | Chronic Illness | 1.153 | 0.536 | 0.069 | 0.018 | 0.118 | 0.033 |
| Health literacy | Distance | 1.194 | 0.518 | 0.072 | 0.019 | 0.122 | 0.026 |
| Health literacy | Gender | 1.110 | 0.486 | 0.071 | 0.020 | 0.120 | 0.026 |
| MetS Knowledge | Health Literacy | 0.099 | 0.013 | 0.227 | 0.180 | 0.274 | 0.001 |
| MetS Knowledge | Distance | -0.589 | 0.223 | -0.081 | -0.134 | -0.028 | 0.012 |
| MetS Knowledge | Family history of IHD | 0.506 | 0.239 | 0.065 | 0.016 | 0.112 | 0.026 |
| Healthy Lifetyle | MetS Knowledge | 0.038 | 0.012 | 0.093 | 0.035 | 0.150 | 0.009 |
| Healthy Lifetyle | Health Literacy | 0.016 | 0.005 | 0.092 | 0.040 | 0.141 | 0.002 |
| Healthy Lifetyle | Gender | 0.777 | 0.083 | 0.279 | 0.240 | 0.333 | 0.001 |
| Healthy Lifetyle | Age | -0.007 | 0.003 | -0.071 | -0.119 | -0.019 | 0.019 |
| Type of Effect | Family History of IHD Effect (%) | Distance Effect (%) | Education Effect (%) | Chronic Illness Effect (%) | Gender Effect (%) | Age Effect (%) | Health Literacy (%) | MetS Knowledge (%) |
|---|---|---|---|---|---|---|---|---|
| Total | 0.006(100) | 0.001(100) | 0.019(100) | 0.008(100) | 0.287(100) | -0.071(100) | 0.113(100) | 0.093(100) |
| Direct | 0(0) | 0(0) | 0(0) | 0(0) | 0.279(97.2) | -0.071(100) | 0.092(810.4) | 0.093(100) |
| Indirect | 0.006(100) | 0.001(100) | 0.019(100) | 0.008(100) | 0.008(2.8) | 0(0) | 0.021(18.6) | 0(0) |
The construction of the path diagram revealed that age, gender, health literacy and metabolic syndrome knowledge have a direct effect on healthy lifestyle practice. Gender has both direct and indirect effect on healthy lifestyle practice. Table 4 displays the indirect, direct and total effects of the independent and intermediate variables towards healthy lifestyle practice. The beta coefficient for the direct effect of gender on healthy lifestyle practice in the model is 0.279 (p value <0.05). Gender was dummy coded as 0= Male and 1= Female in this path model. Thus, the positive relationship indicates that females are more likely to have healthier lifestyle practice compared to males. In this model pathway, gender has an indirect effect towards healthy lifestyle practice which is mediated by health literacy (beta= 0.008, p < 0.05). The total effect (direct & indirect) from gender to healthy lifestyle practice is 0.287 which is also statistically significant (p < 0.05). Age only has a direct effect on the practice of healthy lifestyle with beta coefficient of -0.071 (p < 0.001). Negative correlation suggested that with every unit increase in age, healthy lifestyle practice is lowered. This was an expected direction in this relationship and and is statistically significant. An increase in the unit of family history of ischemic heart disease will improve metabolic syndrome knowledge. Health literacy has both direct and direct effect on healthy lifestyle practice. The direct effect of health literacy towards healthy lifestyle practice has the coefficient of 0.092 which is statistically significant (p < 0.05). This means every unit increase in health literacy will improve healthy lifestyle practice of an individual. Health literacy indirect effect towards healthy lifestyle practice is mediated by metabolic syndrome knowledge with the beta coefficient of 0.021 and is statistically significant. This shows that every unit increase in health literacy will indirectly improve healthy lifestyle practice. The total effect of this structural relationship is 0.113 (p < 0.005). This, illustrates the importance of better understanding of disease knowledge in order to practice a healthy lifestyle. Lastly, the direct effect of metabolic syndrome knowledge towards healthy lifestyle practice is 0.093 which is statistically significant (p < 0.05). This finding suggests that an increase in every unit of metabolic syndrome will positively impact healthy lifestyle practice.
3.3. Multi Group Analysis
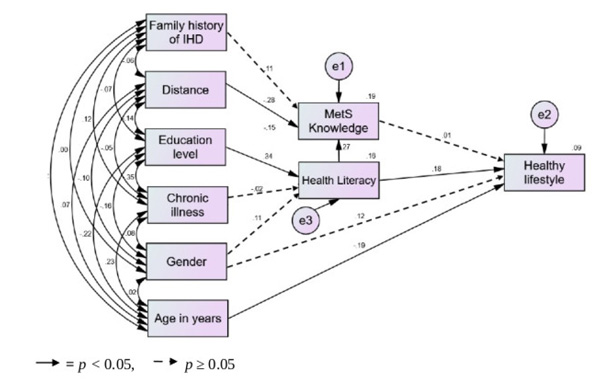
A multi-group path analysis was developed to produce separate subgroup models based on ethnicity, which were divided into Malay/Melanau, Native and Chinese Figs. (4-6) Female respondents from Malay/Melanau and Native groups have a better healthy lifestyle practice than the male. However, there was no significant difference between gender for Chinese respondents towards the practice of a healthy lifestyle. For all 3 ethnic groups, the only sociodemographic factor that significantly affects health literacy was education level. Correspondingly, health literacy status positively influenced knowledge of metabolic syndrome. Age was reported to be negatively associated with healthy lifestyle practice for Malay/ Melanau and Chinese respondents. Distance of health care facility was a significant factor affecting health literacy for Malay/ Melanau respondents. Influence of having a chronic illness on health literacy was only significant among the Native respondents. Health care service factor (distance) influenced health literacy for Malay/Melanau ethnic group and metabolic syndrome knowledge for the Chinese respondents. Family history with ischemic heart disease only improved knowledge of metabolic syndrome of the Malay/Melanau respondents. Good health literacy was vital for respondents from Malay/ Melanau and Chinese ethnic group to practice a healthier lifestyle. For the Natives, knowledge of metabolic syndrome was an important determinant of healthy lifestyle practice.

Dummy coding:
Gender: male=0, female= 1
Education: primary and below= 0, Secondary and above= 1
Distance: less than 5 km= 0, more than 5 km = 1
Chronic illness, family history of IHD: no= 0, yes= 1

Dummy coding:
Gender: male=0, female= 1
Education: primary and below= 0, Secondary and above= 1
Distance: less than 5 km= 0, more than 5 km = 1
Chronic illness, family history of IHD: no= 0, yes= 1
Dummy coding:
Gender: male=0, female= 1
Education: primary and below= 0, Secondary and above= 1
Distance: less than 5 km= 0, more than 5 km = 1
Chronic illness, family history of IHD: no= 0, yes= 1
| Index | Overall Model | Multi Group |
|---|---|---|
| Chi-square | 12.083 | 69.829 |
| Degree of freedom | 8 | 32 |
| Chi-square p value | 0.148 | 0.000 |
| Normed chi square χ2/df | 1.510 | 2.182 |
| Root Mean Square Error of Approximation (90% CI) |
0.023 (0.000, 0.047) | 0.024 (0.016, 0.032) |
| Comparative fit index | 0.986 | 0.945 |
| Adjusted goodness-of-fit index | 0.987 | 0.962 |
| Tucker-Lewis coefficient | 0.950 | 0.809 |
In summary, for all three ethnic groups, education status positively influenced health literacy status. Correspondingly, health literacy status positively affects knowledge of metabolic syndrome. Gender differences and history of chronic illness has no significant influence on health literacy for all the ethnic groups. However, being female was a strong determinant to practice a healthy lifestyle for Malay/Melanau and Native groups, but not for Chinese respondents. We observed different determinants influencing the practice of healthy lifestyle among the ethnic groups. For Malay/Melanau respondents, gender and health literacy status influenced healthy lifestyle practice. Knowledge of metabolic syndrome and gender were reported to contribute significantly on the practice of a healthy lifestyle for the Natives. For Chinese respondents, health literacy is the only factor that influences healthy lifestyle practice.
3.4. Model Fit
(Table 5) goodness of fit for both overall and multi group pathway model. Model fit for overall pathway model was reported to be good with AGFI = 0.987, CFI = 0.986 and TLI = 0.950. Additionally, χ2 (8) = 12.083, p = 0.148 and RMSEA = 0.023 (90% CI: 0.000 - 0.047). For multi group analysis, the model fit was also reported to be acceptable with AGFI = 0.962, CFI = 0.945 and TLI= 0.809. Additionally, χ2 (32) = 69.829, p < 0.001 and RMSEA= 0.024 (90% CI: 0.016 - 0.032). Table 5 contains the indirect, direct and total effects of the independent and intermediate variables towards healthy lifestyle practice.
4. DISCUSSION
This study examined theories on factors influencing healthy lifestyle practice among multi-ethnic Sarawakian adults. Two important mediation pathways between socio demographic variables, service factor, history of chronic illness and healthy lifestyle practice were discovered discovered in our study. Health literacy and metabolic syndrome knowledge significantly mediates pathway between independent variables and healthy lifestyle practice. Current study reported age gender differences, health literacy, and knowledge on metabolic syndrome are direct determinants of healthy lifestyle practice to prevent metabolic syndrome. Health literacy requires a combination of basic literacy skills, communication ability and critical thinking. The result is consistent with previous literature which emphasized on the importance of health literacy towards healthy lifestyle habits [24]. Our study also reported that a better level of health literacy will improve the understanding of disease knowledge and subsequently leads to the practice of healthy lifestyle. The relationship between health knowledge, health literacy and the practice of healthy lifestyle habit has been widely established in other parts of the world [25-27]. This finding is beneficial since health literacy and knowledge are modifiable determinants of health. interventions can be administered on both components. We found that good socioeconomic status, such as education is associated with possessing a higher level of health literacy. Several existing studies reported similar findings [28-30]. This should support the policy of focusing on developing health literacy and integrating the teaching of knowledge of specific diseases in school curriculum. These health-related knowledges should be delivered extensively since childhood to prevent lifestyle related disease. The Protection Motivation Theory which was developed and later revised by Ronald W. Rogers, offers a theory on influential communication, inducing fear that focused on the cognitive processes mediating change of behaviour [31]. Its main aim is not only to create preventive awareness but also induce fear on lifestyle related diseases. The clear understanding of diseases, its severity, complication and prognosis could deter sedentary lifestyle such as being physically inactive, eating healthy and avoiding or reducing alcohol and tobacco usage.
The current study reported that comorbidity leads to improvement of health literacy and a better understanding of disease knowledge contributed by having a family history of medical illnesses. A similar scenario was reported by Song Y. et al. (2013) [32]. However, the distance of the health care facility negatively affects metabolic syndrome knowledge. In contrary to our finding, He et al. (2016) in their community study among the elderly in China reported that the greater the distance of health care facility, the poorer the health knowledge [33]. This eventually led to an unhealthy lifestyle practice. Deficiency of knowledge is expected in the rural part of any country, but an effective method of delivering proper health information to the general public is vital. Health and disease-specific knowledge could be delivered in various ways. Currently, the most effective tool for information dissemination is social media. Malaysians prefer to spend time online than listening to radio, watching television and reading printed materials [34]. Additionally, Malaysian social network users reported to have the highest number of friends on social network in the world [35].
As public health personnel, our goal should focus on creating awareness and understanding of ailments among healthy population, instead of acquiring disease knowledge when they are ill. Failure to tackle underlying determinant will not improve the pattern of health problems. Burden and cost of curative care services will skyrocket. In this study, healthy lifestyle practices were made up of the following components: physical activity, dietary status, tobacco and alcohol consumption and stress level. Therefore, the score of every component counts in determining the level of healthy lifestyle status of the respondents. A more sedentary lifestyle will result in a lower score of Simple Lifestyle Indicator Questionnaire (SLIQ). Available literature demonstrated the effectiveness of healthy-lifestyle such as adequate fruits and vegetables consumption, not smoking regular physical activity and ability to maintain ideal body weight towards the prevention of metabolic syndrome. Under the principle of health promotion, health behavior is modifiable by addressing factors. Female respondents reported to have better healthy lifestyle practice than male respondents. Similar findings have been reported elsewhere [36, 37]. Female participants practice better nutritional intake and higher physical activity compared to male participants. Women were more attentive towards information and worldwide issues related to health and diseases than the men. This is a vital discovery since numerous studies reported a higher prevalence of metabolic syndrome in women than men [6, 38]. Nevertheless, it is vital for both men and women to have healthy lifestyle practice. In this model, age has moderation effects on healthy lifestyle practice. Advancing age turned lifestyle into more motionless and riskier forms [39, 40]. However, the biological and social process of aging is likely to encourage discordant behaviours. Biologically, exercise becomes more difficult with age as cardiovascular function and balance decline, and the prevalence of joint problems increases. Older age individuals with inadequate health literacy status are less likely to utilise the written media as a source of health information. This leads to a serious and challenging problem where written information is the main method of information communication in health care settings. This situation is worrying since aging was also proven to elevate the risk of metabolic syndrome. Increasing in age deteriorate lipid profile in both men and women, a condition which is known as dyslipidaemia and can lead to ischemic heart diseases and stroke [41].
Multi-group analysis demonstrated differences in the pathway leading to a healthy lifestyle among different ethnic groups. Health literacy plays an important role in predicting healthy lifestyle behaviors for Malay/Melanau and Chinese respondents. However, for the Natives, adequate knowledge on the disease itself will deter a sedentary lifestyle. Nevertheless, regardless of the ethnicity and cultural differences, intervention activities should be comprehensive, with emphasis on the cultural aspect of it. Cultural differences have a substantial effect on lifestyle. Studies have shown the importance of addressing issues related to health beliefs and practices of culturally diverse groups [42, 43]. Our path model supported eight determinants (age, gender, education, chronic illness, family history of ischemic heart disease, health care facility distance, health literacy and metabolic syndrome knowledge) for healthy lifestyle practice against metabolic syndrome. The interaction between these determinants explained 11 percent of the total variance. Our findings are comparable to other studies that assess complex structural relationship predicating a healthy lifestyle habit [44-46]. The current study assessed a combination of all five healthy lifestyle habit elements (physical activity, nutrition, stress, tobacco and alcohol consumption) that prevent metabolic syndrome. Participants fulfilling all criteria of healthy lifestyle habit were considered to have a good preventive lifestyle of metabolic syndrome. To our knowledge, this is the first study to identify the causal model on healthy behaviours against lifestyle-related disease specifically metabolic syndrome among different ethnic groups of Sarawak. Therefore, the current study has practical implications for designing health promotion programs according to the target group. Since the gap for practicing a healthy lifestyle has been identified, it is timely to handle this issue comprehensively. To date, health literacy is a well-established concept and outcome of health promotion [47, 48]. It can be nurtured through proper health education. Health education, in a broader understanding, aims to influence not solely on personal lifestyle choices, but also raises awareness of the determinants of health, and encourages individual and collective actions which might lead to an adjustment of these determinants. it is high time that health care professional be the driving force to ensure that health literacy flourish in both individual and community level. The objective of a traditional community-based approach is to create equitable corporations of everyone in a specific community by emphasizing on generating strengths and allocating resources within the community itself [49]. Health and disease knowledge can be nurtured through health education activities. The effort to increase the practice of healthy lifestyle is not just an individual problem, but also societal. Thus, it requires a culturally acceptable approach which can be applied to the population. Simultaneously a multi-disciplinary and multi-sectoral involvement is important to target a bigger audience.
CONCLUSION
Current study shows the mediation effect of health literacy and knowledge towards the practice of a healthy lifestyle. Poor lifestyle practice can be explained by a lack of information and understanding of certain diseases and deprived health literacy skills. Education to increase the knowledge of important specific diseases will provide better practice of a healthy lifestyle. Additionally, culturally sensitive health education is essential to ensure that information can be delivered effectively across the State which is diverse in term of population. Primordial prevention should target vulnerable groups to inhibit the development of risk factors. From Public Health perspective, the best method of primordial prevention is school-based. Continuous long-standing lifestyle modification and changes in children and adolescents can diminish the development of NCD risk factors and disease onset in later-life. The teaching of disease knowledge and recognising the danger of metabolic syndrome lifestyle risk factors should be integrated into school curriculum.
STRENGTH AND LIMITATION
This study is one of the first to demonstrate the mediation effect of health literacy and disease knowledge towards the practice of healthy lifestyle in Malaysia. Sarawak is diverse in ethnic groups. Thus, population study with multistage stratified sampling methods allows for the proper representation of subgroups within the population. Several limitations of this study should be addressed. Firstly, cross-sectional study only permits us to assess independent and dependent variables concurrently. Hence only association can be identified but causality cannot be inferred. Secondly, data were collected by using interviewer-assisted questionnaire which could lead to interviewer bias that can cause distraction and affect the respondent’s willingness to disclose sensitive information [50]. However, it is important to point out that face to face interview facilitates precise screening and evades false information.
AUTHOR'S CONTRIBUTION
All the authors contributed equally.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Medical Research Ethics Committee of Universiti Malaysia Sarawak (UNIMAS) granted approval to conduct this research.
HUMAN AND ANIMAL RIGHTS
No animals/humans were used for studies that are the basis of this research.
CONSENT FOR PUBLICATION
Formal written consent was obtained, and confidentiality of information was assured.
FUNDING
This work was supported by the Institute of Borneo Studies, Universiti Malaysia Sarawak (Unimas) with the reference number of F05/NRC/1636/2017.
CONFLICT OF INTEREST
The authors declare that they have no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The authors would like to thank all participants of this study; lecturers and staffs of Department of Community Medicine and Public Health, Universiti Malaysia Sarawak; Medical Research Ethics Committee of Universiti Malaysia Sarawak; Institute of Borneo Study for the project grant and our research assistants for the excellent work.

