All published articles of this journal are available on ScienceDirect.

Effect of Knowledge About Cardiovascular Diseases on Healthy Lifestyle Behavior Among Freshmen of Zagazig University: An Intervention Study
Abstract
Background:
Educating the younger population about cardiovascular diseases (CVDs) and promoting their healthy lifestyle behavior are essential preventive approaches.
Objective:
To assess the knowledge about CVDs and healthy lifestyle behavior among freshmen college students, before and after the application of an educational program.
Methods:
A pre-test/post-test 6-month interventional educational study was conducted on first-year, Faculty of Science, Zagazig University students. Cardiovascular Disease Risk Factors Knowledge Level (CARRF-KL) and Healthy Lifestyle Behavior (HLSBS-II) scales were completed by the students before and after the intervention. The intervention included lectures, group discussions, and the participants’ preparation of action plans to change unhealthy lifestyle behaviors.
Results:
In the pre-intervention phase, 58.3% of the participants had “adequate” knowledge about CVDs and their mean total HLSBS-II score was 98.35 ± 6.50. Following the intervention, 99.2% of the participants acquired “adequate” knowledge about CVDs, with significant improvement in all aspects of the CARRF-KL score, p < 0.001. The “health responsibility” and “nutritional habits” subscale scores of the HLSBS-II improved significantly, p < 0.01. Participants with CVDs and/or positive family history had significantly higher total mean CARRF-KL scores than those without personal or family history of CVDs, p < 0.05. The total CARRF-KL showed a significant positive correlation with “health responsibility” and “nutritional habits” HLSBS-II subscales (p < 0.05).
Conclusion:
The applied educational program effectively improved the participants’ knowledge about CVDs and empowered them to improve their health responsibility and nutritional habits. Health education and promotion programs should be implemented and integrated within the curriculum of university students.
1. INTRODUCTION
Cardiovascular Diseases (CVDs) include groups of pathological disorders that affect the heart and/or blood vessels [1]. Over the last few decades, CVDs have become a priority on the public health agenda as they have been found to be one of the primary causes of premature death and disability. They are considered the third leading cause of death among individuals 35-44 years of age, and rank as the fifth leading cause of death among those 15-35 years of age [2-5]. The CVDs are responsible for over 17.3 million deaths worldwide annually, representing 30% of global deaths in 2008. This number is expected to increase to approximately 25 million deaths and CVDs are projected to be the leading cause of death by 2020 [6], with over 80% of CVD-related mortality occurring in low- to middle-income countries (LMIC). In Egypt, as a LMIC, CVD mortality for all ages and both sexes accounts for 46% of total deaths [1, 7].
The origin of CVDs is multi-factorial in nature with a synergistic effect. The World Health Organization (WHO) has identified different risk factors for CVDs that are classified into two groups: behavioral risk factors, such as tobacco use, physical inactivity, and poor dietary patterns; and clinical risk factors, such as hypertension, diabetes mellitus, high body mass index, and hyperlipidemia [8]. Early detection and prevention of these risk factors can help reduce the impact of CVDs [9].
Although CVDs are considered diseases of the elderly, multiple studies have shown that they can begin early in life, as their risk factors are often present during childhood and adolescence, resulting in increased prevalence of health risks among today’s university students [10]. Accordingly, there is a major need to increase knowledge and awareness about CVDs among this young population, and target CVD prevention programs to this audience with an aim to reduce CVD-related complications and mortality later in life [11].
University years are a major transitional period for students because they are away from parental supervision and have to make independent lifestyle decisions. University students obtain a considerable amount of knowledge that establishes a base for their lifestyle choices and health knowledge during college years. Many of them adopt unhealthy lifestyle behaviors like poor dietary choices, smoking, use of illicit drugs, and physical inactivity [12, 13]. Thus, the university setting offers a unique opportunity to reach many young adults and study their CVD risks, as well as inform, empower, and motivate them to adopt healthier lifestyle behaviors [14].
Research that focuses on the effects of education programs on knowledge about CVDs among university students in Egypt, as well as other countries in the region, is lacking. Moreover, there is no structured university-based program concerned with promoting healthy lifestyle behaviors among students. In addition, evaluating freshmen would provide baseline knowledge and lifestyle behavior regarding CVDs, before possible exposure to relevant knowledge and behavioral changes during subsequent college years. Therefore, the current study was designed to assess the knowledge about CVDs and healthy lifestyle behavior among freshmen of the Faculty of Science at Zagazig University, before and after the application of an educational program.
2. MATERIALS AND METHODS
2.1. Design and Setting
A pre-test/post-test interventional educational study was conducted over a 6-month period from October 2016 until the end of March 2017 at the Faculty of Science, Zagazig University.
2.2. Study Population and Sampling
Zagazig University comprises 20 colleges. These colleges are categorized into practical non-health-related, theoretical, and practical health-related colleges. The practical health-related and theoretical colleges were excluded from the present study. The practical health-related college students are exposed to health information relating to CVDs through their educational curriculum. This would have affected the results of the study. The theoretical colleges were also excluded, as most of those students do not attend the college campus regularly, which would make the implementation of our education program infeasible.
The faculty of science was selected out of six practical non-health related colleges of Zagazig University by a simple random sampling technique. According to the objectives of the current study, the first-year students (freshmen) of the Faculty Science comprised the study population.
2.2.1. Sample Size Calculation
A sample of 128 first-year students was calculated using the Epi Info software program version 7, based on the following criteria: the change in knowledge was assumed to reach up to 27% based on the findings of our pilot study; a statistical level of significance set at p < 0.05; power of 80.0%; and expected dropout rate of 10%.
2.2.2. Recruitment
According to the Faculty of Science students registry, the total number of first-year students during the academic year 2016/2017 was 1300. The name of each student had a number in the list of the college registry. The calculated sample was drawn by a simple random sampling technique using the Excel software program 2013. The selected students were invited to participate in the study, and the response rate was about 97%. The students who did not respond were replaced by others from the generated Excel program random list.
2.3. Data Collection Tools
The following data were collected using self-administered pre-test/post-test questionnaires.
2.3.1. General Characteristics of the Study Population
A general questionnaire was developed to address socio-demographic characteristics of the students under evaluation. The CVD risk factors included age, gender, residence, parental educational level and occupation, family income, smoking habits, and disease status in the student and family.
2.3.2. Cardiovascular Disease Risk Factors Knowledge Level (CARRF-KL) Scale
A standardized, valid and reliable (Cronbach’s α = 0.76) scale that was developed by Arikan et al. [15] was used to assess knowledge about CVDs. The scale is composed of 28 items that are presented as sentences investigating knowledge about CVD manifestations, prevention, the role of age, different risk factors, and the effect of changing risky behaviors. Responses to these items included “yes,” “no,” or “I do not know.” Correct responses were given a score of 2; wrong answers, a score of 1; and “I don't know” was given a score of 0. This resulted in a total score of 56. Knowledge level increased as the score increased. A score > 28 (> 50%) was considered an “adequate” knowledge level, whereas a score ≤ 28 (≤ 50%) was considered an “inadequate” knowledge level. In this study, the Cronbach’s α was 0.79.
2.3.3. Healthy Lifestyle Behaviors Scale II (HLSBS-II)
The scale was developed by Walker, Sechrist, and Pender [16]. It is used to evaluate health behaviors associated with an individual's healthy lifestyle. The scale consists of six subscales, including: “health responsibility” (which assesses the level of the individual’s responsibility regarding their health); “physical activity” (which assesses the individual’s physical activity practices); “nutritional habits” (which assesses the individual’s food choices); “spiritual growth” (which assesses the attainment of self-actualization and fulfillment); “interpersonal relationships” (which assesses continuous communication of the individual with the surrounding social environment); and “stress management” (which assesses sources of stress, as identified by the individual and stress coping mechanisms).
The scale consists of 52 items (nine items for “health responsibility;” eight items for “physical activity;” nine items for “nutritional habits;” nine items for “spiritual growth;” nine items for “interpersonal relationships;” and eight items for “stress management.”) Each item was scored on a four-point Likert scale, where “never” = 1; “sometimes” = 2; “often” = 3; and “regularly” = 4. Thus, the scores obtained ranged from 52 to 208. Higher scores indicated more health-promoting behaviors. Cronbach’s α for this scale was 0.81.
The items of both CARRF-KL and HLSBS-II scales were translated from English to Arabic by a professional translator experienced in translating health survey questionnaires. The scales were also reverse translated back into English to check for possible discrepancies and make appropriate changes. The study was preceded by a pilot study on 12 students, to assess the feasibility and time required to complete the questionnaire and conduct the health education sessions. The selected pilot subjects were excluded from the main sample of the study. The collected pilot data were analyzed and the necessary modifications were done.
2.4. Data Collection Phases
- Phase 1 (pre-intervention)
After obtaining informed consent, and before the health education sessions were conducted, the prepared questionnaire and scales were self-administered by the students. The responses were then collected by the researchers.
- Phase 2 (intervention)
Our intervention was divided into two parts:
a). Health Education Session
Health education regarding basic knowledge about CVDs and aspects of a healthy lifestyle was delivered by the researchers, who conducted 10 sessions over 4 weeks. Each session featured specific educational content and lasted 50 min. Two sessions were conducted on CVD risk factors, manifestations, and prevention; two sessions on proper nutritional habits (e.g., not skipping breakfast, eating less fats and sugary foods, eating fruits and vegetables); two sessions on physical activity/stress management techniques/interpersonal relationships; two sessions on spiritual growth/health responsibility; and the last two sessions were on planning a healthy lifestyle (e.g., how to identify problems and needs, set a goal, select strategies, implement steps of the selected strategy, and monitor and evaluate the plan). In addition to the distribution of brochures to the students, PowerPoint was used as a supportive audiovisual tool.
The students who agreed to participate and completed all phases of the study were offered follow-up cards for general medical checkups and basic laboratory tests (complete blood count and random blood sugar). These checkups and tests were performed at the Zagazig University Internal Medicine outpatient clinic. Almost all participants completed the study. Those who did not attend 20% of the educational activities during the intervention phase were considered dropouts.
b). After completing the health education sessions, the students were divided into six groups. The researcher met each group once over two weeks. During these meetings, group discussions were conducted and videos about healthy lifestyle behavior were displayed. Moreover, the participants were encouraged to discuss any personal experience of CVD risk factors and complications relating to their families. Each group was then asked to prepare a plan to improve one unhealthy lifestyle behavior. Two weeks later, each group presented and discussed their plans with the researcher.
- Phase 3
This was a wash-out period of two months, during which no education sessions were conducted.
- Phase 4 (post-intervention)
The post-test questionnaire and scales (similar to the pre-test) were completed after obtaining the students’ verbal consent.
2.5. Ethical Considerations
The study protocol was approved by the ethical committee of the Faculty of Medicine - Zagazig University institutional review board. Written informed consent was obtained from the participants. Furthermore, participants were assured about the confidentiality of their data, and that the study results would be used only for the purpose of research.
2.6. Statistical Analysis
Data were coded, entered, and analyzed by the SPSS program version 19. Mean and Standard Deviation (SD) were computed to summarize the scores of the scales. The paired t-test was applied to assess the differences between the mean scores in the pre- and post-tests. Pearson’s correlation was used to determine the correlation between the measurements of different scales. Furthermore, linear regression analysis was performed to predict the effects of the different characteristics of participants on the acquisition of “adequate” knowledge. Statistical significance was considered at p < 0.05.
3. RESULTS
Table 1 presents the general characteristics of the students under investigation. The results showed that 51.7% were male participants; 55.0% were from rural areas; the parents of 85.0% had university-level education and above; the parents of 81.7% had a professional career; the family income of 48.3% was considered adequate; 73.3% were non-smokers; 93.3% had no CVDs; 90.0% had no other diseases; and 71.7% had no family history of CVDs. Their ages ranged from 16.50 to 17.50 years with a mean of 17 + 0.35 years.
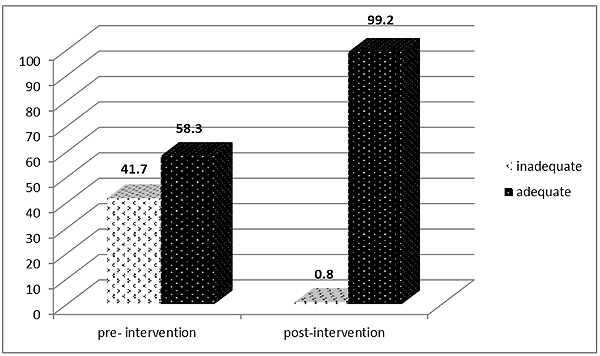
Following comparisons of the total CARRF-KL scores between the pre- and post-intervention phases, 58.3% of the participants showed “adequate” knowledge in the pre-intervention phase, which increased to 99.2% in the post-intervention phase (Fig. 1).
Table 2 shows a significant increase in the mean score of both the total and each individual CARRF-KL scale aspects in the post-intervention phase, p < 0.001. Regarding the HLSBS-II scale, insignificant changes were noted in the mean scores of the total HLSBS-II and its subscales among the participants, with the exception of “health responsibility” (18.57 ± 2.82 to 18.63 ± 2.75, p < 0.05) and “nutritional habits” (15.71 ± 2.05 to 17.25 ± 2.51, p < 0.01) in the post-intervention phase.
Regarding the correlation between the mean scores of the total CARRF-KL and HLSBS-II scales among the participants in the post-intervention phase, Table 3 shows significant positive correlations between the total CARRF-KL, and “health responsibility” (r = 0.202, p < 0.05) and “nutritional habits” HLSBS-II subscales (r = 0.617, p < 0.01).
Table 4 shows that participants with CVDs and/or a positive family history were significantly more likely to acquire “adequate” total CARRF-KL scores than those without personal or family history of CVDs (p < 0.05).
| Variables | No (%) |
|---|---|
|
Gender: Male Female |
62 (51.7%) 58 (48.3%) |
|
Age (X+SD) Range |
17+0.35 16.50 -17.50 |
|
Residence: Urban Rural |
54(45.0%) 66 (55.0%) |
|
Parent education Illiterate Primary Secondary University and above |
4 (3.3%) 4 (3.3%) 10 (8.3%) 102 (85.0%) |
|
Parent occupation Skilled worker Professional |
22 (18.3%) 98 (81.7%) |
|
Family income Not enough Enough Enough and more |
54 (45.0%) 58 (48.3%) 8 (6.7%) |
|
Smoking status: Non-smoker Ex- smoker Smoker |
88(73.3%) 4(3.3%) 28 (23.3%) |
|
Presence of CVDs: No Yes |
112 (93.3%) 8 (6.7%) |
|
Presence of other diseases: None Diabetes Rheumatoid Arthritis |
108 (90.0%) 10 (8.3%) 2 (1.7%) |
|
Family history of CVDs No Yes |
86 (71.7%) 34 (28.3%) |
| Total* | 120 |
4. DISCUSSION
4.1. Pre-Intervention Phase
The present study revealed that the level of knowledge about CVDs of 58.3% of the participants during the pre-intervention phase was deemed “adequate.” This value is lower than that reported among Gulf Medical University students in Ajman, UAE, where most of the participants (95.5%) had an adequate knowledge level about CVD risk factors and prevention [17].
| Items | Min- max | Pre-intervention | Post intervention | *p | ||
|---|---|---|---|---|---|---|
| Min- max | X ±SD | Min- max | X ±SD | |||
| CARRF-KL | ||||||
| CVDs manifestations, CVD prevention, and the role of age. | 0-8 | 0-8 | 3.91±1.10 | 3-8 | 6.42±1.12 | 0.000 |
| CVDs risk factors | 0-30 | 1-27 | 16.75±4.92 | 12-30 | 23.59±3.64 | 0.000 |
| Effect of changing risky behaviors | 0-18 | 0-16 | 9.14±2.61 | 8-18 | 14.11±2.16 | 0.000 |
| Total CARRF-KL scale score | 0-56 | 5-45 | 29.81± 8.15 | 21-55 | 44.15±4.76 | 0.000 |
| HLSBS-II | ||||||
| Health responsibility | 9-36 | 14-26 | 18.57±2.82 | 14-29 | 18.63±2.75 | 0.019 |
| Physical activity | 8-32 | 8-15 | 11.60±1.59 | 10-16 | 11.61±1.59 | 0.319 |
| Nutritional habits | 9-36 | 11-20 | 15.71±2.05 | 11-24 | 17.25±2.51 | 0.000 |
| Spiritual growth | 9-36 | 10-19 | 14.85±2.02 | 10-21 | 14.84±2.02 | 0.657 |
| Interpersonal relationships | 9-36 | 15-30 | 22.78±2.86 | 17-35 | 22.80±2.84 | 0.158 |
| Stress management | 8-32 | 9-21 | 14.82±2.47 | 11-23 | 14.88±2.50 | 0.190 |
| Total HLSBS-II scale score | 52-208 | 81-110 | 98.35± 6.50 | 87-125 | 98.39±6.44 | 0.132 |
| – | Total CARRF-KL |
|---|---|
| Health responsibility | r=0.202 * |
| Physical activity | r=0.003 |
| Nutritional habits | r=0.617** |
| Spiritual growth | r=0.112 |
| Interpersonal relationships | r=0.067 |
| Stress management | r=0.039 |
| Total HLSBS-II | r=0.097 |
| Items | B | S.E. | p value | Expected (B) | 95.0% C.I. for Exp B | |
|---|---|---|---|---|---|---|
| – | – | – | – | – | Lower | Upper |
| Presence of CVDs | 1.064 | 0.503 | 0.034 | 2.897 | 1.082 | 7.757 |
| Family history of CVDs | 1.113 | 0.464 | 0.016 | 3.043 | 1.227 | 7.550 |
This difference could be attributed to the medical background of the Gulf Medical University students. However, our results were more favorable than those reported by multiple studies among young adults and college students using various CVD knowledge assessment tools [18-20].
The total HLSBS-II mean score of the participants was 98.35 ± 6.50 during the pre-intervention phase. This value was lower than that reported in studies conducted in other countries using the same assessment scale. Hacihasanoǧlu et al. [21] reported a value of 118.41 ± 20.90 among Turkish university students; Nassar and Shaheen [22] reported 127.24 ± 21.03 among Jordanian nursing students; Mehri et al. [23] reported 135.38 ± 15.21 among Iranian university students; and Suraj and Singh [24] reported 138.69 ± 14.50 among Indian university students.
Despite levels of “adequate” knowledge in more than half of the participants, their healthy lifestyle behavior was relatively low. This highlights the urgent need for the establishment and implementation of effective strategies to improve health promotion behavior among university students.
Regarding the HLSBS-II, the lowest score was observed in the “physical activities” subscale (11.60 ± 1.59), and the highest score in the “interpersonal relationship” subscale (22.78 ± 2.86) during the pre-intervention phase. This finding is consistent with the results of other studies conducted among Iranian university students and Health High School nursing students at a Turkish university [23, 25].
Low levels of physical activity among university students may be due to a greater focus on their time spent studying, using mobile devices and computers, as well as a lack of sporting facilities [26]. Moreover, from a socio-cultural perspective, regular exercise is not typically part of the daily Egyptian lifestyle, and sports is still considered, to some extent, a leisure activity.
The relatively high “interpersonal relationship” score was particularly interesting. College students usually have insufficient life experience and are susceptible to peer pressure, which may have a negative effect on their social and psychological health [27]. The findings of the current study suggest that our study population has a high a degree of social communication skills, which in turn, makes them both more receptive to interventions and more efficient disseminators of health promotion information.
4.2. Post-Intervention Phase
Following the implementation of our educational program, almost all (99.2%) of the participants acquired “adequate” knowledge scores, with significant improvement in the total, and each of the individual knowledge aspects of the CARRF-KL scale (p < 0.001). Similar findings have been observed in several educational intervention studies among healthy adults and school children using different types of knowledge assessment questionnaires [28, 29].
Another experimental randomized controlled study, conducted among university nursing students, showed a significantly higher level of knowledge about coronary artery disease in the intervention group, after the provision of a cardiac educational program. The intervention group had scores of 21 ± 2.32 and 20.20 ± 2.24 in the first and second follow-up post-tests, respectively; as compared to the control group, which had scores of 6.93 ± 1.15 and 7.12 ± 2.13 in the first and second post-tests, respectively [30].
Furthermore, after the implementation of our educational program, the participants showed significant improvement in their “nutritional habits” score. This finding is similar to those of other studies conducted among nursing students in Taiwan [31, 32]. Stice et al. [33] went further and evaluated the effect of a 15-week educational program on the dietary intake and Body Mass Index (BMI) of undergraduate students. The program included seminars and class discussions, and the results showed significant changes in the BMI of the participants [33]. The findings of the present study are promising, as the dietary habits of students during the university years could deteriorate. Such students are more likely to skip meals and consume fast foods and snacks [34]. Therefore, targeted nutritional education for students during their early university years is essential to improve their nutritional habits and overall health consciousness [35, 36].
We also observed significant improvement in the “health responsibility” scores of participants. This finding is consistent with those of other studies [32, 37]. “Health responsibility” describes the sense of accountability for one’s own health and educating oneself about health. College students are relatively young, and worry less about their health owing to low levels of health responsibility [38]. Thus, the improvement observed in our participants’ sense of responsibility after application of the program indicates that they are potentially able to change their unhealthy behavior, if they are supported by health promotion programs.
The total HLSBS-II scores and other dimension scores showed no significant improvement after the implementation of our intervention. In contrast to this finding, other studies in Taiwan and Turkey have reported a positive impact of health education promotion programs on both the total and various aspects of healthy lifestyle behaviors of nursing and engineering students [31, 32, 37]. This difference could be attributed to variations in the content, duration, components, and approach of the intervention [39].
The considerable improvement observed in the participants’ knowledge about CVDs and some of the lifestyle dimensions (nutritional habits and health responsibility) could be attributed to the variety of health education methods used. These methods included interactive face-to-face lectures and group discussions, supported by various audiovisual tools. WHO stated that health education programs enhance the individual’s health awareness and enables them to make their decisions regarding healthy lifestyle behaviors [40]. Furthermore, the students created action plans, implemented problem solving techniques to develop solutions for various unhealthy lifestyle behaviors, and discussed their plans with the researchers. These methods led them to better understand the delivered educational messages, establish the relationship between their health and behavior, and equipped them with the tools for decision making and behavioral change [32].
The insignificant change in the total HLSBS-II and its other domains during the post-intervention phase could be attributed to the difficulty in changing human behavior [41]. Applying multi-factorial lifestyle program interventions, such as physical exercise training, dietary counseling, and behavioral change targets will provide a comprehensive approach for the modification of healthy lifestyle behavior [42].
A significant positive correlation was observed between the post-intervention total CARRF-KL score and both the “health responsibility” (r = 0.202, p < 0.05) and “nutritional habits” scores (r = 0.617, p < 0.01) of the participants. Many interventional studies have confirmed the positive effects of gaining knowledge and changing different lifestyle dimensions among adults and college students [30, 39, 43]. A study conducted by Jovanović et al. [44] showed that a higher level of knowledge about CVDs and cancer nutrition was significantly correlated with better food choices among medical students. Contrary to our findings, Kumsar et al. [25] reported a significant positive correlation between the CARRF-KL score and all HLSBS-II dimensions (p < 0.05), with the exception of health responsibility, physical activity, and nutritional habits among nursing students.
After evaluating the effects of different students’ characteristics on the acquisition of knowledge during the post-intervention phase, we noticed that participants with CVDs and/or a positive family history had significantly higher total mean CARRF-KL scores than those without personal or family history of CVDs, p < 0.05. These results are consistent with those of previous studies conducted among adults and university students [15, 25, 28]. This finding could be attributed to the desire of those with CVDs to cope with specific requirements to avoid complications and adopt a healthy lifestyle [30]. The existence of a family history of CVDs may motivate and empower individuals to adopt healthy lifestyle changes and follow clinician-recommended preventive changes [45, 46]. After our intervention, we expect those with a family history to acquire more knowledge than those without a family history of CVDs.
The results of our intervention are encouraging and highlight the importance of introducing an effective multi-dimensional university-based health promotion educational program. Such programs should be aimed at improving students’ knowledge about CVDs and promoting healthy lifestyle behaviors.
4.3. Limitations of the Study
We encourage investigators in their future research to recruit students of theoretical colleges and adopt quasi-experimental designs with a longer follow-up period. This study included neither a control group nor long-term follow-up of the participants. Moreover, students of theoretical colleges were not involved in the present study. Another limitation of the study was its use of self-administered behavior questionnaires, which have a tendency toward overreporting of socially acceptable behavior.
CONCLUSION
The applied educational program effectively improved the participants’ knowledge about CVDs and empowered them to improve their health responsibility and nutritional habits. Health education and promotion programs should be implemented and integrated within the curriculum of university students.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study protocol was approved by the ethical committee of the Faculty of Medicine - Zagazig University Institutional Review Board – ZU-IRB # 4849/10-8-2016.
HUMAN AND ANIMAL RIGHTS
No animals/ humans were used for the studies that are the basis of this research.
CONSENT FOR PUBLICATION
Written informed consent was obtained from the participants. Furthermore, participants were assured about the confidentiality of their data and that the study results would be used only for the purpose of research.
AVAILABILITY OF DATA AND MATERIALS
Not applicable.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
We would like to thank all participating students for their kind co-operation.

