All published articles of this journal are available on ScienceDirect.

The Effectiveness of Tai Chi Exercise in Improving Balance and Preventing Falls Among Older Adults
Abstract
Background:
Accidental falls in older adults cause serious health problems, therefore, Tai Chi exercise (TC) is important to help older adults regain body balance and prevent falls.
Objective:
This study aimed to assess: 1) the effect of a 12-week TC intervention on lower extremity strength and body balance in older adults, 2) recent falls within 12 weeks, and 3) participants’ satisfaction toward TC exercise.
Methods:
A quasi-experimental study was conducted, and the participants were older adults, aged 60 and above. One hundred participants were selected by a purposive sampling technique and were divided into 2 groups: the experimental group (n=50) performing the TC exercise, and the control group (n=50) not performing TC. The lower-extremity strength was measured by using a dynamometer, and the body balance was measured by using a timed single leg stance procedure.
Results:
The findings revealed that lower-extremity strength was not significantly different in three time periods: pre-TC, after 6 weeks, and after 12 weeks within the experimental group and also after 12 weeks between the experimental group and control group. The body balance within the experimental group in the three time periods was significantly different (p<.001). Multiple pair comparisons by using the Bonferroni test indicated that phase 3 (a 12-week) was significantly higher than phase 1, and phase 2 (p<.05).
However, the effect of a 12-week TC intervention on the body balance of the experimental group was significantly higher than that of the control group (p<.001). The number of recent falls and near falls within 12 weeks in the control group was 14%, with 10% falls occurring outdoors and 4% occurring indoors, whereas the experimental group did not report any falls and showed satisfaction towards the TC exercise.
Conclusion:
The findings of the study confirm that TC exercise improves body balance and helps reduce the risk of falls in older adults, while the group of older adults who did not undergo TC exercise suffered an increased risk of falls. These results should be applied and implemented among older adults and other groups of populations in different geographic locations and other clinical settings who are at the risk of falls. Also, the study on TC exercise should be extended to 6-12 months so that concrete results from improving lower-limb strength and body balance can be observed.
1. INTRODUCTION
Nowadays, the number of older adults is significantly increasing worldwide with a change in their mental and physical health, including Thailand. Older adults tend to suffer from falls with more than one in four older adults falling accidentally each year. Falls appear serious because they lead to morbidity, disability and deaths [1]. During 2007-2016, unintentional injuries were reported as the seventh leading cause of death among older adults in the U.S [2]. Similarly, in Thailand, accidental falls in older adults have been the second cause of death. A national survey of Thai older adults aged 60 and above found that 18.7% had one or more falls with 21.5% of female older adults falling more often than their male counterparts with 14.4% [3]. A previous study found that older adults fell in the past by tripping (55%), and slipping (28.7%), and 48% of the falls occurred outdoor rather than indoor (30.4%) [3]. Injuries from falling may include bruising, fractures, traumatic brain injury, secondary complications, and losing the independence. There are a number of risk factors that are responsible for falling in older adults [3, 4], including a lack of exercise which can lead to weakness and an increase in the chances of falling. Various studies have found that the effect of Tai Chi exercise or Tai Chi Chuan (TC) may reduce the incidence of falls and injurious falls in older adults. TC exercise is recommended as a safe and known form of physical activity among older adults [5, 6] because it can improve lower extremity strength and body balance [5, 7]. It can improve mobility, knee extension and confidence in performing functional tasks [8]. Moreover, it increases psychological well-being, cardio functioning, and sleep enhancement in older adults [9]. TC intervention is a series of slow, gentle, and low-impact movements that integrate the breath, mind, and physical activity to achieve greater awareness and a sense of inner peace and well-being [5].
Due to the prevalence of falls among older adults, the disability and dependency in older adults is increased. Unfortunately, no study has assessed the effect of TC exercise on body balance and lower extremity strength among older adults, specifically in the Northeastern region of Thailand. Therefore, this study aims to assess 1) the effect of a 12-week Tai Chi intervention on lower extremity strength and body balance in older adults, 2) the number of recent falls and near falls in the experimental group and control group within 12 weeks, and 3) the experimental group’s satisfaction towards TC exercise.
2. MATERIALS AND METHODS
2.1. Study Design and Subject
This study used a quasi-experimental research design. The participants were recruited from Thart Phanom municipality of Nakhon Phanom province and Park Chong municipality of Nakhon Ratchasima province, Northeastern Thailand. The experimental group was selected from the Thart Phanom municipality of Nakhon Phanom province, whereas the control group from the Pak Chong municipality of Nakhon Ratchasima province. The participants were selected by a purposive sampling technique. Moreover, both the experimental and control groups were matched by sex. The samples size was calculated by G*Power 3.1 program with test power (β)= .80, (α)= .05 and effect size = .50. The required sample size was 51 older adults per group.
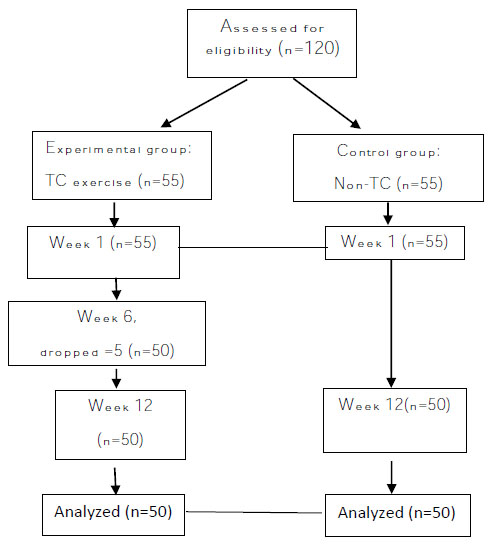
The inclusion criteria included: adults aged ≥ 60 years who were physically active, not cognitively impaired, able to communicate and with a Barthel Activity Daily Life (ADL) index of 18-20. They did not show any symptoms of diseases, such as headache, vertigo, back pain, and did not have a history of surgery for lower extremity, as well as with a blood pressure controlled at a normal level (no ≥ systolic BP 130 mmHg, no ≥ diastolic BP 100). Therefore, they were willing to participate in TC exercise. Exclusion criteria included: Difficulty in walking, ADL index lower than 18, with cognitive impairment, visual and hearing impairment,uncontrolled blood pressure and a history of surgery for lower extremities. Sixty participants fulfilled the eligibility criteria of each group. Five participants in the experimental group were excluded before the program began due to back pain, joint pain, knee surgery, and high blood pressure. Therefore, there were fifty-five participants in the experimental group, and an equal number of participants in the control group, with a total of 110 older adults in both the groups. Afterward, five participants dropped out of the program in the sixth week. Finally, fifty participants completed the TC program. This study was also found to be similar to a study by Cho and An [10]. This study was divided into: 1) three time periods (Pre-TC, after 6 weeks, and after 12 weeks) of the experimental group, 2) two time periods of the control group. The enrollment and study flow for the TC exercise program are shown in Fig. (1).
This study protocol was approved by the Institutional Review Board of Suan Sunandha Rajabhat University (SSRU), Thailand (COA.1-008/2018). All the participants were informed of the study purpose, process, confidentiality, risk, benefits, and their right. Also, they could withdraw from the study at any time. After the participants agreed to participate, they were asked to sign a consent form. This study took place between April- July 2018.
2.2. Measurement and Materials
2.2.1. Materials
Materials included 5 instruments: ● A personal demographic questionnaire was used to obtain each participant’s age, gender, marital status, educational level, history of illness, and falling accident.
The Barthel activity daily life (ADL) index is a standard tool by the Ministry of Public Health, Thailand which is widely used for the assessment of physical activity.
● The dynamometer was used for measuring the strength of lower-limbs.
● The procedure of timed single leg stance for body balance.
● The questionnaire of satisfaction towards TC. The researchers adapted a tool from the literature review. All the items used a 5-point Likert scale from 1= Least to 5=The most, with the possible scores ranging from 15 to 75. The tool was validated by 3 experts. CVI .89 was examined for reliability using α Cronbach 0.87.
● The intervention tool of this study was used for training TC exercise program VTR.
Additionally, the TC sessions were taught to participants by three experts in every TC session. The experimental group performed TC exercise for twelve weeks, six days a week, and 45 minutes in each session, that was divided into 3 phases:
Phase 1; Pre-TC: including a) Demographic questionnaire was used to obtain each participant’s age, gender, marital status, educational level, history of illness. b) Test of the lower-limb strength and body balance pre-TC exercise and during TC workshops.
Phase 2; After completion of 6 weeks of TC: Test of lower-limb strength and body balance after TC practice in 6 weeks.
Phase 3; After completion of 12 weeks of TC: Test of lower-limb strength and body balance after completion of TC practice in 12 weeks and the evaluation of participants’ satisfaction towards TC practice.
The control group performed daily activities without TC practice, that had 2 phases:
Phase 1; First week: Test of lower- limb strength and body balance for the first time, including the collection of demographic data.
Phase 2; Twelfth week: Test of lower- limb strength and body balance after 12 weeks (for the second time), (Fig. 1).
2.2.2. Measurement
Measurement: The lower-limbs strength and body balance were measured by four sports scientists. The TC exercise was taught to participants by three experts in every TC session. Evaluators evaluated the outcomes independently, and they did not know the results of other evaluators.
After obtaining their permission, participants who met the criteria agreed to participate in this program. They were at the training workshop program, which included the assessment of lower-limb, body balance, demographic questionnaire. The intervention was performed on the group that performed TC exercise.
Assessed for eligibility (n=120)
2.3. Statistical Analyses
Descriptive statistics was used to determine the demographic data. The difference of lower-limb strength and body balance among 3 phases was tested using repeated measures ANOVA. The independent t-test was used to test the difference of lower- limb strength and body balance after 12 weeks between the experimental group and the control group.
3. RESULTS
The participants’ demographic characteristics, comorbid diseases, and the history of falling accidents are demonstrated in Table 1.
The repeated measures ANOVA was used for the comparison of the mean difference of lower-limb strength of the experimental group among 3 phases and the results revealed that it was not different (Table 2). The body balance with opened eyes and closed eyes among 3 phases of the experimental group was compared. The results showed that it was significantly different, p<.001 (Table 3). Post-hoc pair comparison by using the Bonferroni test indicated that phase 3 (a 12-week) was higher than phase 1 and phase 2and had a value of p<.05 (Table 4). The effect of a 12-week TC intervention on lower extremity strength between the experimental group and the control group was not different (Table 5). However, the effect of a 12-week TC intervention on body balance with opened eyes and closed eyes of the experimental group was significantly higher than the control group with p<.05 and p<.001, respectively (Table 6). The number of recent falls and near falls within 12 weeks in the control group was 14%, with 10% of falls occurring outdoors and 4% occurring indoors, whereas the experimental group did not report any falls (Table 7) and showed satisfaction towards TC exercise.
The recent fall and near falls in participants within 12 weeks; no falls were observed in the experimental group, whereas falls and near falls of 14% were observed in the control group (Table 7).
| Demographics |
Experimental group (TC) n=50 |
Control group (Non-TC) n=50 |
|---|---|---|
| Gender: Male Female | 46 | 46 |
| Age (years) Range Mean |
– 60-88 72.5 |
– 60-85 71 |
| Body mass index (BMI) | 18.0- 29.0 | 19.5-32.4 |
| Educational level Elementary Secondary Vocation Bachelor degree Master degree |
– 11 14 3 12 1 |
– 20 3 2 6 6 |
| Income (Thai Baht)/month Mean |
800-100,000 21,530 |
800-80,000 15,250 |
| Marital status Single Married Widowed |
– 2 23 24 |
– 3 15 35 |
| Co-morbid Disease Non Yes Hypertension (HT) Hypotension Heart disease (HD) Diabetes mellitus (DM) Hypothyroid Parkinson’s disease Allergy Musculoskeletal disease |
– 23 27 15 1 2 5 1 1 3 2 |
– 20 30 20 1 4 13 1 1 2 3 |
| Falling within 6 months Non Yes |
– 33 17 |
– 29 21 |
| Sources | SS | df | MS | F | p-value |
|---|---|---|---|---|---|
| TC practice (3 phases) | 2.052 | 1.006 | 2.040 | 2.435 | .125 |
| Error | 41.295 | 49.292 | 0.838 | – | – |
| Sources | SS | df | MS | F | p-value |
|---|---|---|---|---|---|
|
Opened eye TC practice (3 phases) |
244.910 | 1.130 | .655 | 21.49** | .000 |
| Error | 558.394 | 55.390 | 10.081 | – | – |
|
Closed eye TC practice (3 phases) |
42.927 | 1.418 | 30.263 | 36.527** | .000 |
| Error | 57.585 | 69.505 | 0.829 | – | – |
|
Body balance: Timed single leg stance (second) Opened eyes |
– | Phase 1 | Phase 2 | Phase 3 |
|---|---|---|---|---|
| – | 6.699 | 7.056 | 9.571 | |
| Phase 1 | 6.699 | – | 0.357 | 2.872* |
| Phase 2 | 7.056 | – | – | 2.515* |
| Phase 3 | 9.571 | – | – | – |
| Closed eyes | – | 2.983 | 3.134 | 4.186 |
| Phase 1 | 2.983 | – | 0.151 | 1.203* |
| Phase 2 | 3.134 | – | – | 1.052* |
| Phase3 | 4.186 | – | – | – |
| Groups | Mean | SD | t | p-value |
|---|---|---|---|---|
| Experiment | 1.12 | 1.13 | 0.880 | .381 |
| Control | 0.92 | 1.07 | – | – |
| Groups | Mean | SD | t | p-value |
|---|---|---|---|---|
|
Opened eyes Experiment Control |
9.57 6.43 |
8.69 6.21 |
2.075* |
.041 |
|
Closed eyes Experiment Control |
4.18 5.25 |
3.49 1.16 |
3.714** |
.000 |
| Group |
Experimental group Frequency (%) |
Control group Frequency (%) |
|---|---|---|
| Recent falls and near falls within 12 weeks Location of falls Outdoors Indoors |
0 0 0 |
7 (14) 5(10) 2 (4) |
The participants showed satisfaction toward TC exercise; mean=3.47 (SD=0.42).
The satisfaction was based on 15 items (1) perceived beneficial effects; mean= 3.63 (SD=0.49)
(2) using in daily life; mean=3.56 (SD=0.50) (3) improved sleep; mean=3.41 (SD=0.63)
(4) physically active; mean=3.56 (SD=0.50) (5) muscle relaxation; mean=3.48 (SD=0.50) (6) vigorous; mean=3.52 (SD=0.50) (7) decreased fear of falling; mean=3.41 (SD=0.57) (8) reduced muscle pain; mean=3.41 (SD=0.63) (9) less time consuming; mean=3.19 (SD=0.87) (10) favorable; mean=3.56 (SD=0.50) (11) desire to perform TC exercise often; mean=3.59 (SD=0.50) (12) no danger; mean=3.59 (SD=0.50) (13) will advise to family members and others; mean=3.44 (SD=0.50) (14) should provide for other community; mean=3.30 (SD=0.86) (15) joyful; mean =3.59 (SD=0.50).
4. DISCUSSION
In this study, lower-limb strength of the older adults in the experimental group was not significantly different in the three time periods and also after the completion of 12 weeks in the experimental group and the control group. It could be observed that TC, in short term, may not affect the muscle strength of lower limbs. This is consistent with [7] a study that indicated that the strength of lower limbs related to TC practice within 4 months (16 weeks) affected muscle strength which was lower than walking and dancing. The practice extended to 8 months showed greater strength, and the completion of 12 months showed the greatest strength. In the experimental group, the body balance during the following periods: 1) pre- TC, 2) after 6 weeks, and 3) after 12 weeks with closed eyes and opened eyes, was significantly different in both the three time periods and after the completion of 12 weeks in the experimental group and the control group. Moreover, the body balance after 12 weeks was the highest. It could be observed that TC practice appeared to improve body balance. Also, it helped reduce falls and fear of falls in the elderly [7, 9]. TC exercise increased functional mobility, flexibility, psychological well-being, sleep enhancement in elderly individuals, and increased cardio functioning [9,11]. TC, which effectively improves the balance and reduces the fear of falling, could be considered as a practical and useful method for fall prevention among older adults and more suitable as a long term exercise, as its short term effects are not obvious [6, 7]. TC is a safe and known form of physical activity among older adults, and seems better than brisk walking for reducing several risk factors of cardiovascular disease and improving psychosocial well-being [9]. Therefore, it should be recommended for living a healthy life [6]. The recent falls and near falls of the control group were 14%, with 4% happening indoors and 10% outdoors, which indicated that the control group was at a high risk of falls and near falls [12], while the experimental group did not suffer from falls. Participants’ satisfaction was perceived by the TC benefits, intention to do TC exercise daily, strength improvement, relaxation, reduction of muscle pain, and a good night’s sleep. In addition, the findings indicated that TC affected not only the physical well-being but also the psychosocial well-being [13]. Since the elderly health care is a priority, there is a need to use an integrated model of care to improve the quality of life of older adults [14]. Therefore, TC exercise should be included in health promotion programs for older adults.
5. LIMITATIONS
This study focused on older adults in only two municipalities in Nakhon Phanom province and Nakhon Ratchasima province in the Northeast of Thailand. A small number of participants were selected through purposive sampling. Thus, the finding may not be generalized to older adults living in other regions of Thailand as well as in other countries. Also, the intervention was performed for only 12 weeks and could not improve the strength of lower limbs.
CONCLUSION AND IMPLICATIONS
The results confirmed that a 12-week TC intervention can improve the body balance of lower extremities and help reduce the risk of falls in older adults. However, it can not improve lower extremity strength in older adults. The recent falls and near falls within 12 weeks in the control group were 14%, with 4% falls happening indoors and 10% outdoors. Participants in the experimental group did not report falls, and had a good level of satisfaction towards the program of TC exercise. Therefore, it can be applied and implemented among older adults and other groups of populations in different geographic locations and other clinical settings who are at the risk of falls. Further study should focus more on high-quality trials with larger participants and extended TC practice in long term.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by the Institutional Review Broad of Suan Sunandha Rajabhat University (SSRU), Thailand. (COA. 1-008/2018)
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures were followed in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (http://www.wma.net/en/20activities/10ethics/10helsinki/).
CONSENT FOR PUBLICATION
Informed consent was obtained from all the participants to participate in this study.
AVAILABILITY OF DATA AND MATERIALS
Not applicable.
FUNDING
This study was funded by the National Research Council of Thailand and Suan Sunandha Rajabhat University.
CONFLICT OF INTEREST
The authors declared no potential conflicts of interest with respect to the research with other publications of this article Grant No. 1
ACKNOWLEDGEMENTS
The researchers would like to express sincere thanks and appreciation to all the parties concerned, including the participants, Suan Sunandha Rajabhat University and Bangkokthonburi University, that significantly contributed to the successful completion of this research.

