All published articles of this journal are available on ScienceDirect.

Determinants of Women Access to Healthcare Services in Sub-Saharan Africa
Abstract
Background:
The study examined the socio-economic determinants of women access to healthcare services in Sub-Saharan Africa for the period 1995-2015.
Methods:
The study adopted the dynamic panel model and estimated it using the System Generalized Method of Moments in a bid to overcome the endogeneity problem inherent in the model of study.
Result:
The study harmonized the theoretical strands in the literature by describing the measure of access determinants as three main components; i. Health service availability, ii. Health service utilization and iii. Health service decision.
Conclusion:
The indicators of health service availability such as community health workers, physicians, nurses and midwives and hospital beds improve women's access to healthcare facilities in Africa. Also, health service utilization indicators such as population density worsen the quality of healthcare services available to women while electricity access and private health expenditure enhance women’s access to quality healthcare delivery. Health service decision indicators such as female bank account ownership, female labour force participation, attainment of basic education and female household headship were important in enhancing women's access to healthcare facilities. Generally, women's health outcomes were more responsive to health service utilization; implying that service utilization is an important proof of healthcare access in Africa.
1. INTRODUCTION
Good health is basic to human welfare and fundamental to socio-economic development. Incidentally, people in Sub-Saharan Africa (SSA) face limited healthcare choices leading to poor access and reduction on the benefits of medical technology and efficacy of medical interventions leading to pains and suffering among the population. Access to public healthcare practices often results in the elimination of deadly diseases among the communities. The health of mothers is very crucial because it affects the health of every member of the household, particularly that of children and aged persons. The increasing burden of poor institutional healthcare delivery service presents mothers with multiple challenges during pregnancy and delivery; leading to high maternal mortality in developing countries particularly among countries in the region of Sub-Saharan Africa (SSA). The situation is even grave in countries where the poverty level is high; the healthcare system is poor and overstretched [1]. According to a study [2], the health of mothers and children is closely related to the general health of the community. According to a study [3], developing regions accounted for approximately 99% (302000) of the global maternal deaths in 2015, with SSA alone accounting for roughly 66% (201000), followed by Southern Asia (66000). The majority of these deaths could be avoided if women had access to quality medical care during pregnancy, childbirth and postpartum [4]. For instance, in Nigeria, the government rolled out the Integrated Maternal, Newborn and Child Health (IMNCH) strategy as part of measures aimed at reducing maternal and infant mortality [5]. The study [6] noted that the trend in developing countries is much worse, as studies from various countries of SSA indicate that maternal mortality has not only continued to be high, but is indeed increasing after the launch of the Safe Motherhood Initiative (SMI) in Kenya in 1987. This limitation is greater in the SSA region, where a large proportion of deliveries take place at home [7]. In developing countries, less than 50% of deliveries occur in health facilities therefore skilled birth assistance is not utilized in such deliveries. Access to and use of health services is low in Africa, and this is reflected in the poor maternal health indicators [8].
Insufficient or poor use of maternal healthcare services is largely responsible for the high rate of maternal deaths in the sub-region. According to the study [9], maternal mortality and morbidity can be reduced through access to appropriate healthcare during pregnancy and delivery; however, in SSA women continue to face limited access to such services. Similarly, the study [10] concludes that lack of access to appropriate obstetric care, especially during labor, compounds the risk of adverse fatal outcomes such as death or disability. Improving maternal and infant health continues to be a major challenge such that a woman living in Sub-Saharan Africa has a 1 in 31 chance of dying during pregnancy or childbirth, as compared to 1 in 4,300 in a high-income country [11]. The study [12] opined that in order to reduce the risk of maternal and infant morbidity and mortality, especially in places where the general socio-economic status is low, access and utilization of the obstetric services is an effective way. Accessibility of maternal healthcare facilities is important in the use of essential maternal services, thereby ensuring the survival chances of mothers and children. The study [13] equally found that access and utilization of maternal health services in the health facilities have been linked with improved maternal and neonatal health outcomes. Low uptake of Antenatal Care (ANC) is an important determinant of high maternal mortality rate in developing countries and is one of the basic components of maternal care on which the life of mothers and babies depend [14]. According to the WHO, 536000 women die every year in the world from causes relating to pregnancy, childbirth or postpartum. Ninety- nine percent of these deaths occur in developing countries. The ANC services help pregnant women by identifying complications associated with pregnancy or diseases that might adversely affect the pregnancy [15].
In addition to other specific country initiatives, there have been several strategic measures towards reduction in maternal mortality since 1980s, such as the International Safe Motherhood Initiative (SMI), launched in 1987, in Kenya; the International Conference on Population and Development (ICPD), 1994, Cairo in Egypt; the Fourth World Conference on Women, Beijing, 1995, in China; United Nations MDGs 2000 and SDGs 2015. In spite, the worrisome aspect of this situation is that in SSA as a whole, there has been no discernible or perceptible change over the past two or more decades. Scholars have suggested that socio-economic and health-related factors are responsible for high maternal deaths among mothers in SSA; the factors maternal education, husband’s education, employment status, and cost of healthcare services, household income, access to health information, inadequate healthcare providers and availability of service [16-21]. Incidentally, not many studies have examined critically these factors and how they influence access to healthcare services in SSA. Hence, the present study will facilitate understanding the reasons behind the poor access to and use of healthcare services and generate strategic interventions to address the problem of high maternal mortality in the sub-region. The main objective of this study is to determine the influence of socio-economic factors on access to and use of maternal health care services in SSA.
2. CONCEPTUALIZATION OF HEALTH ACCESS
The concept of access has long occupied the literature with vast debate in an attempt to unravel the constituent of access to healthcare services. Yet theoretical direction on what constitutes health access is still shrouded with ambiguity. The description available in academic literature and public policies is limited access to healthcare affordability and geographical proximity. This implies that healthcare access basically centers on issues regarding health insurance coverage and healthcare providers’ distance to patients. According to researchers [22-24], these measures are the easy way out for regulatory agencies charged with ensuring access, as they are readily understandable and relatively simple to measure. An attempt to conceptualize access should entail a broader perspective. A study [24] described access in four approaches, namely; definitions, measures, barriers and framework. Conceptualizing access by definitions basically reviews the various theoretical explanation of the concept in the existing literature. For example, another study [25] described access as the use of services and not simply the presence of the facility. A study [22] sees it as the ability of a population or a segment of the population to obtain health services. In the same manner, another study [26] considered it in terms of four key aspects: availability, utilization, relevance and effectiveness, and quality.
Another theoretical strand in access conceptualization is centered on access measures – this illustrates access as performance (access performance). It essentially considers the process, measures and how the system works to deliver expected results. Examples of such process measures include: the length of time it takes to secure an appointment, proximity to a usual source of care, the availability and ease of contacting a provider, likelihood of delaying healthcare due to facility deficiency or dysfunctional support services and the possibility of having a regular source of care [27-29].
Furthermore, the theoretical strand espoused by some studies [30, 31] conceptualized access as the removal of barriers to health service delivery. Access to health services is often limited by inadequate cash to pay for health services, high cost of health services, long distance to service provider, absence of transportation options, limited hours of providers operation, physical inaccessibility, personal preference for alternate sources, inability to make independent health decisions etc. However, the study [30] proposed three types of barriers to access conceptualization which include: structural barriers, financial barriers and personal barriers. In the same manner [31], extended the concept by introducing cognitive barriers.
The last theoretical strand as proposed by Donabedian [25] and propagated by Ricketts et al [32] and Mackinney et al [24], viewed access as developing a coordinated, effective and rich framework of interaction between multiple access influences and system characteristics. This strand extensively emphasized the ‘framework’ in describing access. The study [25] emphasized that though the presence of providers is necessary but the ultimate proof of access is the use of services. Also, adequate access would not only generate use but also provide equal health potential to different social classes and geographic locations. The framework that will impact access must consider the following: i. temporal match between providers’ care delivery schedule and patients’ work/play schedules, ii. Spatial distribution of service care recipients and health facilities, iii. The socio-organization of an area considering the patients’ socioeconomic class, gender, ethnicity, mental health status, and iv. The level of health care financing available will influence access.
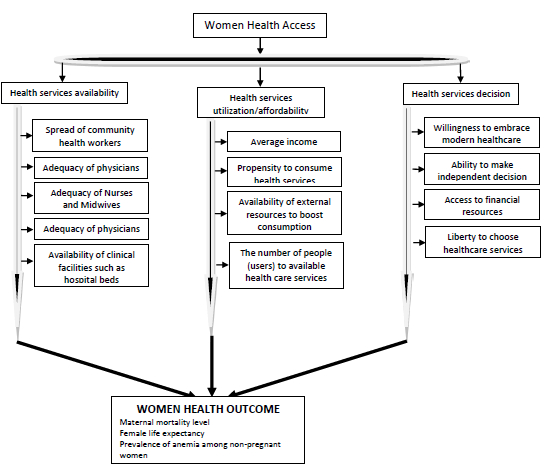
The foregoing has extensively identified the available theoretical positions on the concept of access to health services. From the origin of this discourse in the literature to date, diverse views have emerged to how best to conceptualize health access. This present examination harmonized the existing strands into three major components to capture important determinants of women's access to healthcare services (Table 1); these determinants include: i. Health service availability, ii. Health service utilization, and iii. Health services decision.
| Health Services Availability | Health Service Utilization/affordability | Health Services Decision |
|---|---|---|
| Community health workers (per 1000 people | Per Capita income | Education (Female) |
| Physicians (per 1000 people) | Out-of-pocket health expenditure | Female household |
| Nurses and Midwives (per 1000 people) | External resources for health | Account at financial institutions (Female) |
| Hospital beds (per 1000 people) | Population density | Labour force participation rate (Female) |
3. ANALYTICAL FRAMEWORK AND METHODOLOGY
Following the several attempts by the erstwhile theoretical strands in conceptualizing health access determinants, the study expatiates on the existing relations by constructing an analytical framework to depict how the determinants of women access transmit to influencing woman health outcomes. We diagrammatically identify the pathways and links from health access to health outcomes. Basically, the study sees the determinants of women's healthcare services as premised on three factors, including health services availability, health services utilization and health service decision. The first component bothers on the availability of healthcare services such as personnel and facilities. The second is a measure of the extent of use – the ability of the healthcare receivers to access the healthcare services which can be hindered by the functionality of the healthcare services and the elasticity of its demand effectiveness (ability to pay). The third factor considers the independent ability of healthcare receivers to make an independent decision on the choice of healthcare.
Globally, women have been considered to dominate the healthcare decisions for themselves and families. According to the US Labour Department, women are responsible for making about 80 percent of healthcare decisions for their families. Certainly, this trend differs in some regions, as a certain aspect of culture tends to traditionally overwhelm the ability of women to take independent decisions on matters that affect them. Though, the dominance of this limitation could be dependent on the literacy and financial independence of women. Evidence abound that women in SSA often have limited autonomy and control over their reproductive health decisions, implying that intra-familial decision-making affects women’s ability to access and use maternal health services.
The functional form of the relationship between access and health outcomes can be presented as:
 |
(1) |
Where HLTotc is women's health outcomes (a proxy for women access to healthcare services),
The model can be further structured into three to capture the different categories of determinants of women's health access services. This is illustrated as follows:
Health Services Availability Model:
 |
(2) |
Health Services Utilization Model:
 |
(3) |
 |
(4) |
Where CHW denotes community health workers,
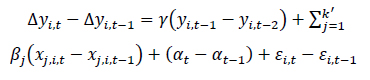
The estimation technique adopted is based on a dynamic panel data model with country fixed effects, and is estimated using the System Generalized Method of Moments (SGMM). This is necessary in order to overcome the problem of reverse causation inherent in the model. In this model, all predetermined and endogenous variables are instrumented by their appropriate lags, to avoid introducing a spurious correlation between these variables and the error term. The SGMM is dynamic in nature and thus preferable to the static panel data models in which the regressors are correlated with the country-specific effects and are usually estimated using the so-called Fixed Effects (FE) estimator. The class of GMM estimators [33-35] proposed the use of extra moment conditions that rely on certain stationarity conditions of the initial observation. When these conditions are satisfied, the SGMM tends to have much better finite sample properties in terms of bias and root mean squared error than other variants of GMM such as Difference GMM. The relative importance of System GMM makes it an estimator of choice in many applied panel data settings.
The GMM specification can be illustrated as follows:
 |
(5) |
As clearly observed in equation 5, regressors may also be correlated with the error term, such that
The empirical models to be estimated are specified in the GMM structural form presented as follows:
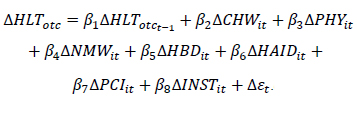 |
(6) |
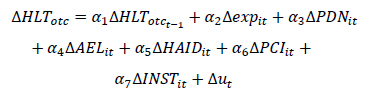 |
(7) |
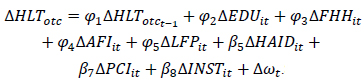 |
(8) |
The data for the empirical investigations were obtained from reputable databases including, World Development Indicators (WDI) and World Governance Indicators (WGI), both of World Bank publications for the period 1995 to 2016.
4. RESULT AND DISCUSSION
The study assesses the determinants of women's access to healthcare facilities in Africa. The determinants were categorized into three categories namely: i. Service availability; ii. Service utilization/affordability; and iii. Service decision ability. The empirical procedure analyzed how these categories of determinants influence women's access to healthcare facilities in Africa. The study captured women's health access using health outcomes such as maternal mortality rate, female life expectancy and prevalence of anemia among non-pregnant women.
The results of the estimation were presented in sequence with adequate explanation. The estimation was completed using the two-step SGMM (xtabond2 specification). The two-step system GMM uses a consistent estimator of the weighing matrix, though could yield standard errors that are downward biased. Also, the Arellano-Bond test for autocorrelation was applied in order to purge the unobserved and perfectly autocorrelated idiosyncratic errors. The results were presented as AR(1) and AR(2) in the lower panel of the result tables and suggest no cases of serial correlation at 1% significance level. Also, a test of instrument validity was conducted using the Sargan test. The results do not reject the over-identifying restriction, implying that instruments are considered valid. Finally, the F-test in the results is considered satisfactory at 1% significance level, implying that the exogenous variables are all jointly significant.
Table 2 (see appendix) comprises the regression results indicating the effect of healthcare services availability on women's health outcomes in Africa. From the result in Table 2, the provision of community health workers and health physician were significant in improving female life expectancy and also these factors reduce the prevalence of anemia among non-pregnant women in Africa. The result implies that a unit increase in the number of community health workers and physicians raises female life expectancy by 1.5 units and 0.9 units respectively. Likewise, a unit increase in the number of community health workers and physicians causes the prevalence of anemia among non-pregnant women to fall by 2.49 and 3.36 units, respectively. The results are consistent with the study [36-38] which suggests that CHWs enable people to access and navigate the healthcare system and better manage their health conditions, coordinate services for people with multiple chronic conditions, and lead community-wide efforts to identify and address underlying causes of poor health. Similarly, available evidence from Table 2 show that the availability of nurses and midwives enhances women's access to healthcare facilities. The number of nurses and midwives significantly impacts women's health outcomes in Africa; as a unit increase in nurses and midwives reduces maternal mortality by about 17.4% while enhancing female life expectancy by about 0.1 units.
The availability of nurses and midwives is more significantly potent in reducing the maternal mortality rate. This would not be unconnected to the fact that most of the life-threatening maternal mortality diseases (especially the anti and postnatal complications) are largely preventable when early diagnosed and treated, given that maternal deaths in Africa arise mainly from these complications. Healthcare services interventions targeted at women would appropriately address the challenges as seen in Table 2. The result supports evidence from studies [39-42], implying that the provision of affordable, acceptable, high-quality health services leads to better access to necessary care and improved population health, particularly for growing numbers of vulnerable individuals and communities. Also, the result considers the effect of per capita income on women's healthcare access in Africa. Average income exerts no significant contemporaneous effect on women's health outcomes in Africa, basically because of the extent of income inequality in the region. This evidence contradicts the assertion by the relative income hypothesis which proposes that the distribution of income within societies is an important determinant of that population’s health consumption. The contradiction could be linked to the reality that African states (especially the SSA economies) have the highest income disparity in the world, with about 5% of the population sharing over 90% of the region’s wealth and heavily based bottom billion.
Conversely, official development assistance significantly improves women’s health outcomes in the African region. It reduces maternal mortality rate and incidence of anemia among non-pregnant women by 24.1 units and 0.2 units respectively and raises life expectancy by 0.2 units. Similarly, female basic education and institution significantly impact women health outcomes. Generally, foreign intervention assistance (ODA), and availability of midwives (NMW) and institutions (INST) were most important in enhancing women's health outcomes in Africa. It is necessary to note that the maternal mortality rate (as a health outcome) is more responsive to health services factors. This is due to the fact that it encompassed a larger weight of women's health outcomes, as low female life expectation and prevalence of anemia among pregnant women could be a major contributor to maternal mortality rate.
The regression results in Table 3 (see appendix) describe women's access to healthcare facilities as a function of the capability to utilize the available healthcare services. These capability/utilization factors include: i. The population density of the area where such health services are available; ii. Access to electricity/energy services in an area for effective utilization of health services; and iii. Out of pocket expenditure on health services. Available evidence from the regression procedure show that population density worsens women's health outcomes in Africa. This indicates that the population per square km of land area in Africa region seems larger than the available facilities, hence limiting the utilization per person. This is not farfetched, as most African states have the smallest number of physicians per population. In addition, electricity access reduces maternal mortality ratio (per 100, 000 live births) in Africa; as a unit increase in access to electricity significantly dwindles maternal mortality by about 5.64 units. This implies that the introduction of off-grid electricity services in homes and health facilities in the region contributes significantly to reducing maternal mortality as necessary health intervention services are quickly provided when emergencies occur. Also, women are less exposed to the strenuous act of fetching firewoods and biomass for cooking and heating purposes and generally less susceptible to the health hazards from using traditional biomass. Similarly, the results suggest that electricity access significantly enhances the life expectancy of women, implying that access to efficient and clean energy services improves women's health outcomes in Africa. Women are mostly at the disadvantaged end in the utilization of dirty energy resources. They engage in biomass gathering, spending the time that would have been put into productive uses and continually exposed to the de-humming and hazardous flames from the use of traditional biomass.
On the other hand, Table 3 indicates that private health expenditure significantly influences female life expectancy and incidences of anemia among non-pregnant women in Africa. This implies that individuals’ private expenditure on health improves life expectancy by 0.002 units and reduces incidences of anemia among non-pregnant women by 0.009 units. This result indicates that women's health outcomes in Africa are less responsive to out-of-pocket expenditure. To support this point, the out-of-pocket expenditure does not significantly influence the maternal mortality ratio. The result is not surprising, given the low per capita income in the region; health services (especially complications surrounding postnatal care) can better be provided by the government public health spending.
The regression results in Table 3 (see appendix) describe women's healthcare access as depending on the capability of women to take independent decisions in accessing healthcare facilities. In this study, we consider women’s social and economic capabilities including; number of women account holders at financial institutions, female labour force participation rate, female basic education and number of households headed by women. The evidence from Table 3 reveals that the number of female accounts at financial institutions and the female labour force participation rate were important factors enhancing women's access to healthcare facilities in Africa. In the same manner, female education and household headship improve health outcomes by reducing the ratio of maternal mortality per 100,000 live births and the proportion of non-pregnant women with anemia by 0.4 units and 0.1 units, respectively. The result suggests that the capability to make an independent decision and unhindered access to appropriate financing improves women's access to healthcare facilities in Africa.
The regression result in Table 1 (see appendix) comprises the index values for the categories of the determinants of women's health outcomes in Africa. These indexes are health services availability index, health services utilization index and health services decision index. The indexes are developed using the principal component analysis [43] of several health services variables. For instance, the health services availability is an index of four health service variables, namely: community health workers (per 1000 people), physicians (per 1000 people), nurses and midwives (per 1000 people) and hospital beds (per 1000 people). The health service utilization index comprises per capita income, out-of-pocket health expenditure, population density and access to electricity. Also, the health service decision index comprises of female education, female household headship, female labour force participation rate and female account at financial institutions. Evidence from the regression Table 1 show that the health services availability index induced an important variation on women's health outcomes as maternal mortality diminishes. This implies that as more health personnel and facilities become available, the number of women mortality from birth complications dwindles by seven units in Africa. Similarly, health services affordability/utilization exerts a more significant variation on health outcomes. The result implies that as utilization access improves, maternal mortality rate and anemia among non-pregnant women reduce by 49.4 units and 2.8 units, respectively while women's life expectancy improves by 0.63 units. The result suggests that the utilization and affordability of health services is an important determinant of women's health outcomes. In places where public health services are unavailable, access to the facilities remains a critical challenge due to population density or inadequate provisions. In cases where access is possible, the effective functioning of these services is limited due to social and economic challenges.
Source: Authors’ compilation.
| variable | Description | Measurement | Source |
|---|---|---|---|
| HLTotc | Health outcomes – Index of maternal mortality, female life expectancy and prevalence of anemia among non-pregnant women | Index | Data on variables were sourced from WDI |
| chw | Community health workers (per 1,000 people) | Number | WDI |
| phy | Physicians (per 1,000 people) | Number | WDI |
| nmw | Nurses and midwives (per 1,000 people) | Number | WDI |
| Hbd | Hospital beds (per 1,000 people) | Number | WDI |
| gdpk | GDP per capita (constant 2010 US$) | Monetary | WDI |
| exp | Out-of-pocket expenditure (% of current health expenditure) | Percentage | WDI |
| pdn | Population density (people per sq. km of land area) | Number | WDI |
| Ael | Access to electricity (% of population) | Percentage | WDI |
| fhh | Female headed household (% of household with a female head) | Percentage | WDI |
| Afi | Account ownership at a financial institution or with a mobile-money service provider, female (% of population 15+) | Percentage | WDI |
| fp | Labour force participation rate, female (% of female population ages 15+) | Percentage | WDI |
| Haid | Total official development assistance for health | Number | Institute of Health Metric Evaluation (IHME) |
| Inst | Average of the six indicators including: control of corruption, government effectiveness, political stability and absence of violence & terrorism, regulatory quality, rule of law and voice and accountability | Scale | World Governance Inductor of World Bank Publication (2016) |
| Health Outcomes | |||
|---|---|---|---|
| VARIABLES | mmr | lxp | npa |
| gdpk | 0.00139 | 0.000596*** | -0.000687*** |
| (0.00433) | (6.08e-05) | (0.000191) | |
| haid | 0.340 | 0.242*** | -0.162*** |
| (1.686) | (0.0179) | (0.0348) | |
| afi | 3.600*** | -0.0351*** | 0.0299 |
| (0.442) | (0.0107) | (0.0191) | |
| fp | -4.823*** | 0.0447*** | 0.0927*** |
| (0.550) | (0.00737) | (0.0181) | |
| fpri | -0.277 | 0.00101 | -0.0290*** |
| (0.370) | (0.00146) | (0.00322) | |
| inst | -43.89** | -0.868*** | -1.291*** |
| (17.06) | (0.0514) | (0.190) | |
| pdn | 0.225** | 0.0191*** | 0.0103* |
| (0.0949) | (0.00302) | (0.00557) | |
| ael | -5.639*** | 0.0204*** | 0.110*** |
| (0.468) | (0.00425) | (0.0179) | |
| poc | -0.176 | 0.00151* | -0.00979*** |
| (0.218) | (0.000897) | (0.00222) | |
| L.mmr L.lxp |
0.691*** (0.0261) |
0.860*** | |
| (0.0107) | |||
| L.npa | 1.082*** | ||
| (0.0190) | |||
| Constant | 565.0*** | -0.438 | -7.850*** |
| (57.31) | (0.840) | (2.081) | |
| Observations | 599 | 622 | 622 |
| Number of id | 42 | 43 | 43 |
| F-stat (p-values) | 0.0000 | 0.0000 | 0.0000 |
| Sargan | 0.8703 | 0.8780 | 0.9404 |
| AR(1) | 0.0071 | 0.0401 | 0.0308 |
| AR(2) | 0.0006 | 0.0634 | 0.0390 |
| No. of instruments | 18 | 18 | 18 |
The indicator of socio-political crisis impacts women's health outcomes negatively, increasing maternal mortality rate and reducing women's life expectancy by 16.4 units and 0.37 units, respectively. This implies that the prevalence of political instability, violence and terrorism progressively worsens women's health outcomes in Africa. In the same manner, evidence obtained for institutions were similar to that of the socio-political crisis. This would not be unconnected to the weak quality of institutions in Africa, which has posed a major deterrent to economic prosperity and quality of life in Africa.
CONCLUSION
The theoretical strands in literature and the scant empirical evidence support the fact that accessibility of maternal healthcare facilities and general health facilities are important in ensuring that lives are saved through the provision of essential maternal services. In Africa, access to healthcare services directly translates to the use of these services but when people cannot access life-saving healthcare services due to a number of barriers, the use of such services will be limited. The study examined the socio-economic deterrent of women access to healthcare services in Sub-Saharan Africa using the dynamic panel model for the period 1995-2015. The study adopted the system generalized method of the moment in order to overcome the inherent challenges of endogeneity associated with the model in the study. The study harmonized the theoretical strands in the literature by developing three categories of indicators to measure components of women's healthcare access. This includes; i. Health services availability; ii. Health services utilization; and iii. Health services decision. Similarly, the study followed the theoretical framework of IOM (1993) in ascertaining the health access outcomes, this includes: morbidity (maternal mortality ratio), health status (female life expectancy), and patient satisfaction (prevalence of anemia among non-pregnant women).
The result indicates that health services availability improves women access to healthcare facilities in Africa. Specifically, provision of community health workers and physician improves female life expectancy and reduces the proportion of African non-pregnant women living with anemia. Similarly, the availability of nurses and midwives, and the provision of services such as adequate hospital beds space enhances the quality of healthcare service available to women in the region. Conversely, average income exerts a negligible contemporaneous effect on women's health outcomes in Africa. This would not be unconnected to the weak average income in Sub-Saharan African economies due to widening income inequality.
More so, socio-economic factors such as population density worsen health outcomes in Africa, reflecting the dense population of most African communities and the sparse distribution of healthcare facilities in these areas. Also, electricity access reduces maternal mortality ratio and enhances the life expectancy of women. This implies that enhanced provision of clean energy sources reduces the risk of exposure to dirty energy sources and enhances the effective use of support services in healthcare provisions. Private health expenditure, though improves life expectancy and reduces the prevalence of non-pregnant women living with anemia but does not exert any significant contemporaneous effect on maternal mortality ratio; thus, implying that the amount available as out-of-pocket spending on health is quite negligible to address complications arising from birth outcomes. Generally, women's health outcomes are less responsive to out-of-pocket expenditure.
Furthermore, the ability to make independent decisions in financing health access measured by female bank account ownership, female labour force participation, attainment of basic education, and female household headship was important in enhancing women's access by reducing maternal mortality ratio and prevalence of anemia among non-pregnant women. Most notably, in all categories of access determinants considered, health services utilization and/or affordability exert the most important effect on health outcomes in Africa. This is consistent with the assertion by Donabedian (1972) who argued that proof of health access is the use of services and not the presence of a provider. From the foregoing, it is obvious that critical attention is needed in developing a health access framework that will ensure the provision of healthcare facilities within the space and income of the people. The government of African economies needs to consciously improve health services availability and most importantly improve capital budgetary allocation in the provision of support services that are needed for efficient and effective healthcare service delivery.
In addition, other important determinants of health outcomes were considered including: total official health development assistance, institutions and prevalence of political instability, and violence and terrorism in Africa. The result shows that in virtually all cases, health aid and institutions improve women's health outcomes while the crisis worsens health outcomes in Africa. Hence, there is a need to further ensure that health development assistance is channelled into appropriate areas of healthcare provisions as evaluated from time to time. Also, the disbursement of aid fund should not be shrouded in secrecy, communities should be consulted and intimated on the appropriate and available healthcare provision plans, in order to own it and access as at when due. Finally, there is a need to strengthen institutions in order to ensure appropriate and adequate disbursement of health funds and ensure adequate discharge of healthcare services by providers.
ETHICAL APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
Not applicable.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of this research are available within the article
FUNDING
None declared.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.
Table 1.
| Health Outcomes | |||
|---|---|---|---|
| VARIABLES | npa | lxp | Mmr |
| loda_t | -0.0892*** | 0.262*** | -0.793 |
| (0.0222) | (0.0458) | (1.387) | |
| ht_ser_ind | 0.173** | -0.287*** | -7.060 |
| (0.0862) | (0.0895) | (5.187) | |
| htser_uti_ind | 2.841*** | 0.628* | -49.38*** |
| (0.843) | (0.374) | (12.90) | |
| htser_dec_ind | -0.570*** | -0.372** | 16.46*** |
| (0.0933) | (0.174) | (3.561) | |
| psv_2 | -0.0874 | 0.452*** | 55.97*** |
| (0.0879) | (0.101) | (7.470) | |
| Inst | 0.0194 | -0.926*** | 71.14*** |
| (0.276) | (0.248) | (7.335) | |
| L.npa L.lxp |
1.059*** (0.0100) |
0.892*** | |
| (0.0188) | |||
| L.mmr | 0.741*** | ||
| (0.0159) | |||
| Observations | 266 | 266 | 261 |
| Number of id | 23 | 23 | 23 |
| F-stat (p-values) | 0.0000 | 0.0000 | 0.0000 |
| Sargan | 0.9902 | 0.8681 | 0.9003 |
| AR(1) | 0.0011 | 0.0231 | 0.0042 |
| AR(2) | 0.0023 | 0.0004 | 0.0321 |
| No. of instruments | 18 | 18 | 18 |
*** p<0.01, ** p<0.05, * p<0.1
| Health Outcomes | |||
|---|---|---|---|
| VARIABLES | mmr | lxp | npa |
| Gdpk | 0.000253 | -0.000486*** | -0.000218 |
| (0.00950) | (0.000107) | (0.000149) | |
| loda_t | -24.11*** | 0.200*** | -0.190*** |
| (3.544) | (0.0424) | (0.0256) | |
| afi | -1.099*** | -0.0117** | 0.0950*** |
| (0.423) | (0.00503) | (0.0285) | |
| fp | -1.186*** | 0.0470*** | -0.0712*** |
| (0.422) | (0.0126) | (0.0120) | |
| fpri | 1.019*** | 0.00182 | -0.0182*** |
| (0.271) | (0.00245) | (0.00242) | |
| inst | -59.61** | -0.867*** | -0.239 |
| (25.49) | (0.203) | (0.315) | |
| chw | 97.76*** | 1.519*** | -2.488*** |
| (19.66) | (0.349) | (0.899) | |
| phy | 203.3*** | 0.915** | -3.359*** |
| (33.70) | (0.463) | (0.901) | |
| nmw | -17.38*** | -0.108** | 0.125 |
| (2.822) | (0.0456) | (0.0811) | |
| L.mmr L.lxp |
0.695*** (0.0224) |
0.954*** | |
| (0.0126) | |||
| L.npa | 1.021*** | ||
| (0.0207) | |||
| Constant | 517.1*** | -3.715** | 7.765*** |
| (47.23) | (1.475) | (1.701) | |
| Observations | 337 | 346 | 346 |
| Number of id | 29 | 29 | 29 |
| F-stat (p-values) | 0.0000 | 0.0000 | 0.0000 |
| Sargan | 0.9262 | 0.9601 | 0.7903 |
| AR(1) | 0.0010 | 0.0081 | 0.0102 |
| AR(2) | 0.0009 | 0.0754 | 0.0075 |
| No. of instruments | 18 | 18 | 18 |
| Health Outcomes | |||
|---|---|---|---|
| VARIABLES | Mmr | lxp | Npa |
| gdpk | -0.0167*** | 0.000908*** | 0.000636*** |
| (0.00500) | (0.000114) | (0.000226) | |
| haid | -2.891* | 0.489*** | -0.436*** |
| (1.746) | (0.0204) | (0.0408) | |
| afi | -2.873*** | -0.0469*** | 0.0142 |
| (0.487) | (0.0126) | (0.0227) | |
| fp | -2.288*** | 0.0842*** | -0.0386*** |
| (0.246) | (0.0117) | (0.0102) | |
| fpri | 0.374* | 0.00172 | 0.00481* |
| (0.196) | (0.00114) | (0.00286) | |
| inst | 15.03* | -1.311*** | -1.384*** |
| (7.740) | (0.108) | (0.192) | |
| fhh | 3.253*** | -0.0859*** | -0.110*** |
| (0.864) | (0.00633) | (0.0186) | |
| L.mmr L.lxp |
0.820*** (0.00644) |
0.869*** | |
| (0.00998) | |||
| L.npa | 1.019*** | ||
| (0.00985) | |||
| Constant | 265.3*** | -5.845*** | 9.079*** |
| (21.43) | (1.258) | (1.473) | |
| Observations | 522 | 542 | 542 |
| Number of id | 36 | 37 | 37 |
| F-stat (p-values) | 0.0000 | 0.0000 | 0.0000 |
| Sargan | 0.9622 | 0.6982 | 0.8853 |
| AR(1) | 0.0011 | 0.0231 | 0.0042 |
| AR(2) | 0.0023 | 0.0004 | 0.0321 |
| No. of instruments | 18 | 18 | 18 |

