All published articles of this journal are available on ScienceDirect.

Social Support and Breast Cancer Recurrence: Is there any Association?
Authors Info & Affiliations
Abstract
Background:
Breast cancer is the most prominent cause of women's mortality due to cancer and is one of the most serious and commonly diagnosed cancers among Iranian women. Also, social support plays a vital role in breast cancer patients' lives and their diagnosis and treatment processes. This study aimed to determine the associations between social support status and the recurrence of breast cancer in women breast cancer referred to the Breast Diseases Research Center in Motahari Clinic in Shiraz, Iran in 2018.
Methods:
This was an applied and descriptive-analytic study on women with breast cancer referred to the Breast Diseases Research Center in Motahari Clinic in Shiraz, Iran in 2018. A sample of 221 patients in two groups of 117 non-recurrence patients and 44 patients with recurrence and metastasis were selected randomly. A localized standard questionnaire was used to collect the required data. The collected data were analyzed using SPSS 24.0.
Results:
Based on the results, there were significant differences between the two studied groups of patients with and without recurrence in terms of the means of social support and all of its dimensions (P-value<0.05); the means of social support and all of its dimensions in the group of patients without recurrence were higher than those in those with recurrence. Also, 88.6% of patients in the group without recurrence received high social support, while in the group of patients with recurrence, only 11.4% of them received high social support.
Conclusion:
The results showed that the breast cancer patients studied without recurrence had higher social support. Therefore, to improve the studied patients' health, we recommend providing the patients with a safe and secure environment, giving accurate and complete responses to the patients' questions, providing continuous psychological counseling, etc.
1. INTRODUCTION
In recent decades, there are significant advances in the field of health and medical sciences, and the pattern of diseases has become different compared to the past due to the identification of the biological causes of diseases, access to health facilities, and transition from acute and infectious diseases to chronic ones [1].
“Cancer” refers to a group of diseases with a variety of about 100 different types [2], which puts considerable pressure on both individuals and society [3]. According to the results of a study, there were about 17.5 million cases of cancer worldwide in 2015 which caused more than 8.7 million deaths, as the second leading cause of death in the world after cardiovascular diseases. In the mentioned study, breast cancer, with 2.4 million new cases, had the highest rate of cancer among women in the world [4]. In 2018, breast cancer alone accounted for 30% of total new diagnoses of cancers in the United States and was the most common type of cancer in American women [5]. Overall, it can be said that this disease is the most common cancer and also the most prominent cause of cancer deaths among women at the global level [4].
Breast cancer has also been one of the most commonly diagnosed cancers among Iranian women in the past few decades and has been prevalent in recent years [6]. According to the results of a study, breast cancer in Iran (between 2005 and 2015) has had the second-highest cancer incidence and mortality rate [4].
Breast cancer is the result of an uncontrollable and malignant growth of the epithelial cells of the lobules (which are the milk-producing glands), ducts (which are the passages that drain milk from the lobules to the nipple), and the stromal tissues (which include the fatty and fibrous connective tissues of the breast). Although it mainly affects women, in rare cases, men can get breast cancer as well [2, 7].
In medicine, the disease relapse is used to evaluate the outcome of the treatment. In general, in cancers, the disease can return as a recurrence in the same organ or as metastasis in another organ [8]. Based on the results of a study, more than 50% of breast cancer recurrence occurs in women after 5 years of their initial diagnosis [9]. Studies have shown that surgery and postoperative therapies reduce the risk of recurrence and significantly increase disease-free survival [10].
On the other hand, some researchers in their studies have demonstrated the positive effects of social support on the patients' general health [11], so that having a high level of social support has been associated with patients' good health behaviors and better health outcomes [12]. In women with breast cancer, also social support plays a vital role in their lives, diagnosis and treatment processes, and is also an important component in providing them with good care. Therefore, although providing appropriate medical treatments for breast cancer patients is necessary, social support can increase the effectiveness of treatments because it helps women to have positive attitudes towards their health condition and cope with their illness [13, 14].
Considering the fact that researchers conducting the present study did not find any research in this field in Iran studying and comparing the social support status among two groups of breast cancer patients with and without recurrence, this study aimed to determine the associations between social support status and the recurrence of breast cancer in women referred to the Breast Diseases Research Center in the Motahari Clinic in Shiraz, Iran in 2018.
2. METHODS
This was an applied, cross-sectional and descriptive-analytic study conducted on women with breast cancer referred to the Breast Diseases Research Center in the Motahari Clinic in Shiraz, Iran in 2018. The studied patients in the present study were only in stages I, II and III.
These patients were divided into two groups of those with and without recurrence. The first group included patients who had a relapse and/or metastasis in the first 10 years after the diagnosis, and the second group consisted of those who did not have any relapse up to 10 years after the diagnosis. Therefore, in the present study, the recurrence time for patients with relapse was considered in the first 10 years of the onset and diagnosis of the disease.
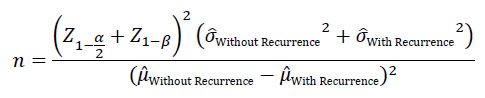
According to the results of the pilot study on the studied patients conducted prior to the present study and based on the following formula [15], assuming α=0.05, β=0.1,
 Without Recurrence=1.32, ,
Without Recurrence=1.26,
Without Recurrence=1.32, ,
Without Recurrence=1.26,
 Without Recurrence=3.5,
Without Recurrence=3.1 as as well as according to the results of a previous study [16] reporting that the average number of patients without recurrence was about four times to that of those with recurrence [16], and considering the probability of 10% patient dropout, the sample size was determined as 175 patients in the group of patients without recurrence and 44 in those with recurrence. The determined samples were selected randomly in each group of patients with and without recurrence referred to the Breast Diseases Research Center, using the simple random sampling method through the use of the random numbers table.
Without Recurrence=3.5,
Without Recurrence=3.1 as as well as according to the results of a previous study [16] reporting that the average number of patients without recurrence was about four times to that of those with recurrence [16], and considering the probability of 10% patient dropout, the sample size was determined as 175 patients in the group of patients without recurrence and 44 in those with recurrence. The determined samples were selected randomly in each group of patients with and without recurrence referred to the Breast Diseases Research Center, using the simple random sampling method through the use of the random numbers table.
The required data were collected using the Persian and localized version of the Social Support Measurement Questionnaire used by Denewer and colleagues in their study (2011) [17]. This questionnaire was first translated from English into Persian and then back-translated; its reliability was confirmed (α=0.79) and its validity was also approved by getting the experts' opinions. The questionnaire consisted of two parts. The first part included items related to the studied patients' demographic data, and the second part included 33 items to assess the social support dimensions, including psychological support (9 items), material support (8 items), medical support (8 items), and family and friends' support (8 items). A five-point Likert scale was used to measure the social support dimensions, 1 referring to “strongly disagree” and 5 to “strongly agree”. Also, the inverse items were scored reversely. In general, the mean of social support higher than 4 was considered as high social support, between 3 and 4 as medium social support, and lower than 3 was considered as low social support.
The collected data were analyzed through SPSS 24.0 software using some statistical tests, including Shapiro-Wilk, Chi-Square, Fisher’s exact test, Independent-Samples T-Test and One-Way ANOVA tests, as well as the Pearson Correlation coefficient. A P-value<0.05 was considered statistically significant.
4. RESULT
The demographic and clinical characteristics of the studied patients are shown in Table 1. As displayed in Table 1, there was no significant difference between demographic and clinical characteristics of the studied patients in the two groups of patients with and without recurrence (P-value>0.05). Also, the mean age of patients without recurrence and those with recurrence was, 51.16±10.01 and 54.59±13.14, respectively, indicating no significant difference between them (P-value=0.112).
Moreover, the results of the Shapiro-Wilk test showed that social support and its dimensions were normal (P>0.05). The results showed that there were no significant associations between the social support and its dimensions and the demographic and clinical characteristics of the studied patients in each group of patients with and without recurrence (P>0.05).
Based on the results, the highest and lowest means of social support dimensions in the group of patients without recurrence were related to the family and friends' support (3.96±0.53) and the material support (3.69±0.61), respectively; also, in those with recurrence, the minimum and maximum dimensions were related to the psychological support (3.69±0.36) and material support (3.42±0.61) (Table 2). Also, as shown in Table 2, there were significant differences between the two studied groups in terms of the means of social support and all of its dimensions (P-value<0.05), so that the means of social support and all of its dimensions in the group of patients without recurrence were higher than those with recurrence.
On the other hand, Table 3 shows that 88.6% of patients without recurrence received high social support, while in the group with recurrence, only 11.4% of patients received high social support. On the contrary, 71.4% of patients in the group with recurrence, compared with 28.6% of those without recurrence, received low social support.
Table 1.
| Patients' Characteristics | Without Recurrence | With Recurrence | Results | |
|---|---|---|---|---|
| Frequency (%) | Frequency (%) | |||
| Marital Status | Married | 143 (80.8) | 34 (77.3) | χ2=0.274 P-value=0.601 |
| Single | 34 (19.2) | 10 (22.7) | ||
| Employment Status | Employed | 16 (9) | 7 (15.9) | F*=7.767 P-value=0.124 |
| Retired | 26 (14.7) | 8 (18.2) | ||
| Housewife | 133 (75.1) | 28 (63.6) | ||
| Home Jobs | 2 (1.1) | 1 (2.3) | ||
| Education | Under the Diploma | 84 (47.5) | 19 (43.2) | χ2=0.387 P-value=0.824 |
| Diploma | 52 (29.4) | 13 (29.5) | ||
| Academic Degrees | 41 (23.2) | 12 (27.3) | ||
| Types of Basic Health Insurance | Iran Health Insurance | 68 (38.5) | 14 (31.8) | F*=3.054 P-value=0.672 |
| Social Security Insurance | 71 (40.1) | 18 (40.9) | ||
| Rural Health Insurance | 13 (7.3) | 5 (11.4) | ||
| Other Health Insurance (including banks, corporations, etc.) | 12 (6.8) | 2 (4.5) | ||
| Armed Forces Health Insurance | 11 (6.2) | 5 (11.4) | ||
| Without any Health Insurance Coverage | 2 (1.1) | 0 (0) | ||
| Having Supplementary Health Insurance | Yes | 93 (52.5) | 31 (70.5) | χ2=0.572 P-value=0.107 |
| No | 84 (47.5) | 13 (29.5) | ||
| Having the Family History of the Breast Cancer | Yes | 85 (48) | 18 (40.9) | χ2=0.717 P-value=0.250 |
| No | 92 (52) | 26 (59.1) | ||
| Place of Residence | City | 106 (59.9) | 26 (59.1) | χ2=0.617 P-value=0.734 |
| Town | 53 (29.9) | 15 (34.1) | ||
| Village | 18 (10.2) | 3 (6.8) | ||
| Stage | I | 32 (18.1) | 12 (27.3) | χ2=3.927 P-value=0.140 |
| II | 117 (66.1) | 22 (50) | ||
| III | 28 (15.8) | 10 (22.7) | ||
*Fisher’s exact test value
5. DISCUSSION
The social support and its dimensions, especially psychological and family and friends' support, are very important for coping with the diseases, particularly breast cancer [18]. Studies have also shown that social and economic inequalities have an impact on the risk of recurrence in breast cancer patients and the opportunity for getting future proper care [19]. Furthermore, according to the results of a study (2017) conducted in Italy in 2003-2005, among the factors affecting the mental health and quality of life of breast cancer patients, social support plays a major role [20].
|
Patient Groups |
Patients Without Recurrence | Patients With Recurrence | P- value |
|---|---|---|---|
| Social Support Dimensions | Mean±SD | Mean±SD | |
| Psychological | 3.91±0.45 | 3.69±0.36 | 0.044 |
| Material | 3.69±0.61 | 3.42±0.61 | 0.009 |
| Medical | 3.81±0.51 | 3.48±0.88 | 0.001 |
| Family and Friends' | 3.96±0.53 | 3.67±0.71 | 0.003 |
| Social Support | 3.84±0.39 | 3.59±0.53 | <0.001 |
| Patient Groups | Without Recurrence (n=177) | With Recurrence (n=44) | Total |
|
Level of Social Support |
Frequency (%) | Frequency (%) | |
| Low (Mean<3) | 2 (28.6) | 5 (71.4) | 7 (100) |
| Medium (Mean between 3 and 4) | 113 (78.5) | 31 (21.5) | 144 (100) |
| High (Mean>4) | 62 (88.6) | 8 (11.4) | 70 (100) |
In the present study, women with breast cancer were divided into two groups without and with recurrence and/or metastases. This study aimed to determine the association between social support and recurrence of breast cancer in patients referred to the Breast Diseases Research Center in the Motahari Clinic in Shiraz, Iran in 2018. The results of the present study showed that patients with more social support had less recurrence. In other words, the means of social support and its dimensions, including psychological, instrumental, medical and family and friends' support, in women who had recurrence or metastases on average in the first 10 years after the first course of treatment were at a lower level. The results also showed that the number of non-recurrence patients at the high social support level (means higher than 4) (88.6%) and women with recurrence at the low level of social support (less than 3) (71.4%) was high. The results of the study by Orsini and colleagues in France (2016) [21], by Jalali-Farahani et al. in Iran (2018) [22], by Denewer and colleagues in Egypt (2016) [17], by Yang et al. in China (2017) [23], by Suwankhong and Liamputtong in Thailand (2016) [24], by Zhang and colleagues in China (2017) [25], by Gage-Bouchard in the United States (2017) [26], by Thompson and colleagues in the United States (2017) [27], by Faller et al. (2016) in Germany [28], by Kauffmann et al. in the United States (2016) [29], and by Hulbert-Williams et al. study (2018) [30]showed that social support and its dimensions had positive effects on patients' health, hope, quality of life, coping behavior, and body image, that are consistent with those of the present study.
The present study, like other studies, has several limitations, including the use of a cross-sectional design, collecting the required data using a single method (i.e. questionnaire), and the use of patients' self-report data. Also, the results of the present study are related to the studied clinic and their generalization to the entire country should be careful and conservative.
To the best of our knowledge, this study has been conducted in Iran for the first time and health policymakers and managers, as well as families of patients with breast cancer, can benefit from its results.
CONCLUSION
According to the results of the present study, social support has a significant association with the absence of recurrence in breast cancer patients. Therefore, specialists, authorities and families should take the importance of social support and its dimensions in the improvement of patients' health into consideration. Families should provide the patient with a safe and secure environment and help him/her to perform his/her activities and tasks and accompany the patient when visiting the health centers. Specialists also have to take into account cancer patients' distress and consider that their patience, support and accurate and complete responses to the patients' questions will be a major contribution to coping with diseases and their compliance with the professional advice. Moreover, because one of the patients' concerns is the costs of treatment, which, in some cases, even caused poverty, the authorities and policymakers should take the necessary measures to create financial and insurance funds to financially support such patients and establish centers to provide the patients and their families' access to cheap medicines. Furthermore, these patients, especially in the early stages, need continuous psychological counseling. By providing these services and facilities, effective steps can be taken to reduce the patients' depression and anxiety, and their fear of lack of timely and appropriate access to the necessary treatments and medicines due to lack of financial support.
AUTHORS’ CONTRIBUTIONS
RR, MD and LH conceived, designed, analyzed, and interpreted the data; LH, ST and MA performed data collection. NSh, RR and LH wrote the first draft and finalized it. All authors read and approved the final manuscript.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The present study was approved by the Ethics Committee of Shiraz University of Medical Sciences, Iran (Code: IR.SUMS.REC. 1397.316).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Informed consent was obtained from all patients participating in the study.
AVAILABILITY OF DATA AND MATERIALS
The data that support the findings of this study are with the corresponding author, [R.R], and can be made available on reasonable request.
FUNDING
This study was a research project supported financially by Iran, Shiraz University of Medical Sciences with the contract number 97-01-68-16935.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest, financial, or otherwise.
ACKNOWLEDGEMENTS
The researchers would like to thank the studied patients for their kind cooperation with the researchers in collecting and analyzing data.

