All published articles of this journal are available on ScienceDirect.

A Cross-Sectional Study: Predicting Health Risks Among Female University Students
Abstract
Background:
Good health is very important in our lives and plays a significant role. Many health risks are associated with an unhealthy lifestyle. These risks are responsible for raising the risk of chronic heart diseases and other health complications. Females are not exempted from these issues.
Objective:
To identify the obesity-associated health risks of female students by using selected anthropometric measurements.
Methods:
A cross-sectional study was conducted including 300 females aged 20.82 ± 5.23 years from the college of applied medical sciences, Imam Abdulrahman bin Faisal University. The anthropometric measurements (body mass index, percentage of body fat, visceral fat area, waist circumference, waist-hip ratio,and waist-height ratio) were taken with the help of an auto-calibrated bioelectric impedance device. The waist-height ratio was determined by dividing waist circumference with height. Cross tabulation was done to scrutinize the participant’s levels at risk and high risk. Linear regression analysis was done to see the relationship and prediction between selected anthropometric measurements.
Results:
The finding showed that BMI level was high in 55% of participants, Waist-height ratio over the average level was 46.67% and 21% of participants had a visceral fat area on risk. Linear regression analysis showed a strong association among body mass index, percentage of body fat, visceral fat area, waist circumference, waist-hip ratio,and waist-height ratio and statistically significant to each other at the 0.01 level.
Conclusion:
The selected anthropometric measurements can be used to identify health-related risks. Though, when any anthropometric measurement dichotomized as standard or high, BMI is the best measure to predict health risk.
1. INTRODUCTION
Health is a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity [1]. For better health, a person needs to have a balanced diet and regular exercise. Health is affected by many factors-those linked to poor health, disability, disease, and injury are known as health risks. A health risk might be associated with many factors like genetic conditions, lifestyle factors, specific sports or activities, and some situations or incidence [2]. Health risks often coexist and interact with one another. The weight gain, high blood pressure, and high cholesterol are the result of inactiveness. These significantly enhance the chance of developing chronic heart diseases and other health problems. Contemporary threats of health are primarily the consequence of risk behavior and related outcome such as enhanced Body Mass Index (BMI), Percentage of Body Fat (PBF), Visceral Fat Area (VFA) Waist Circumference (WC), Waist-hip Ratio (WHR), Waist-height Ratio (WHtR). All these measures are also associated with increased risk of chronic disease morbidity-namely disability, depression, type 2 diabetes, cardiovascular disease, certain cancers-and mortality.
The BMI used to determine the level of body fat and a good measure of health risk that can appear with enhanced body fat. BMI categorization is being universally used in many survey-based kinds of research to assess the mortality risk in a different classification [3]. The high BMI may predict health risk for many diseases as type 2 diabetes, heart disease, high blood pressure, breathing problems, certain cancer, and elevated mortality risk [4]. Body fat percentage is also related to the risk of metabolic syndrome [5]. Enhanced abdominal fat is a notable risk factor for disease as excess body fat. Harvard University observes that 10% of total fat is probable to store as visceral fat. Visceral fat developed by excess intra-abdominal adipose tissue accumulation. Visceral fat considered as more significant health risk than the waist, hip, and thigh fat, not only for diabetes but for many other diseases too [6]. Ding et al. found that visceral fat area was correlated with a higher thirty-day morbidity rate after surgery and hence more appropriate and precise than BMI [7].
Many anthropometric measurements have been studied earlier to find out the leading causes of metabolic syndrome. Lean et al. suggested that WC used as a clinical tool for assessments and interpretation of health risks associated with obesity [8] and associated with cardiovascular disease risk factors independent of BMI [9]. WC indicated as a symptom of adiposity-related morbidities [10]. Waist-hip ratio is the most common measure of visceral adipose tissue, as it revealed a strong correlation with increased risk of various health outcomes as well as mortality in most of the population [11]. WHR is a valid parameter to establish the obesity level. The value of WHR on Myocardial Infarction (MI) risk varies as per gender differences. The high WHR increase MI risk and higher WHR values were strongly predictive of MI in women than men [12]. Many types of research have demonstrated the superiority of WHtR to WC as an anthropometric measure associated with many diseases as diabetes, CVD, hypertension, chronic kidney disease and metabolic syndrome [13].
The BMI less than 18.5 is consider as a low level of health, the range of BMI between 18.5-24.9 is consider as healthy, and BMI over 25 is indicated as health at risk. The PBF between 19.0-29.0 is indicated as healthy. The waist circumference less than 88 cm. signifies healthy students. The visceral fat area is considered normal as range 40-80. The waist circumference of more than 88 cm is considered as a health risk factor. For the waist-hip ratio, the range 0.70-0.85 was considered normal, and the waist-height ratio range 0.42-0.48 implied as normal for female students. In this research, we outline the prevalence and trends of obesity, which can be associated with anthropometric measurements that lead the life at risk.
2. METHODOLOGY
This cross-sectional study was conducted including 300 female participants. The sample has randomly chosen from the College of Applied Medical Sciences. The sample size was considered appropriate to identify risk factors with 95% confidence and a precision rate of 4.5%. There was no pregnancy period and no specific medical problems reported in these participants. Before conducting the tests, all participants were informed of the data would be used for the research. The participants were completely aware of the importance of precision of information during assessment taken. The deanship approved this study of research from Imam Abdulrahman bin Faisal University, Dammam, Saudia Arabia.
2.1. Anthropometric Measurements
All participants were instructed to take off their shoes, jewelry, heavy clothing items and wrap their hair correctly that does not alter the effect to measure height and weight before step on the devices. An auto-calibrated digital scale (Detecto model-750, USA) was used to measure height and weight at the nearest 0.1 cm. and 0.01 kg, respectively. An auto-calibrated bioelectric impedance (BIA) device (iOi 253, Jowan Medical, SK) ran to measure BMI, PBF, VFA, WC, and WHR. To measure all these anthropometric measurements, participants stepped on to the foot electrodes of a BIA device. The measurement carried out was as follows: All participants came to the lab in the morning with empty stomach. The necessary personal details of participants such as age, gender, and height were inputted to the device via a digital keyboard. Participants were asked to be griped hand-held electrodes at 300 angles of the arms and press the button attached to it. Hand-held electrodes send a low and safe electric current through the hand and body to the leg. The participant stands erect and does not talk during measurement. The measurement completes within 1-2 minutes. The waist-height ratio was determined by dividing waist-circumference with height.
2.2. Statistical Analysis
The Statistical Package for Social Science (SPSS V-21) used for data analysis. The data screened for normality and outliers, and descriptive statistics expressed with means and Standard Deviation (SD) for all outcome measures. Levene’s test used to assess the equality of variance for the variables prior to proceed to further statistical analysis. Cross tabulation was done to scrutinize the participant’s level at risk and high risk. Linear regression analysis was done to assess the relationship between selected anthropometric (percentage of body fat, body mass index, visceral fat, waist circumference, waist-hip ratio, and waist-height ratio) variables obtained through BIA. To understand the association between the measured variable, scatter plots are also drawn.
3. RESULTS
Most of the female students were young with an average age 20.8±5.23 years; Height was 157.07±5.78cm, body mass 57.45±13.25kg, BMI 23.18±4.7kg/m, PBF 30.10±6.58%, VCA 59.12±34.20cm2, WC 76.87±8.88cm, WHR .78±.06, WHtR .49±.06.
Fig. (1) shows the categories of anthropometric measurements on the basis of their levels. The light gray bar depicts the below optimal range, green bar stands for the optimal range, and red bar denotes for beyond optimal range i.e., participants at risk. The figure shows that BMI was the highest risk factor, with 165 female students. WHtR on second highest risk factor with 140 female students.VFA on the third highest risk factor with 63. While WC, WHR, and PBF, were on risk with 40, 39, and 33, respectively.
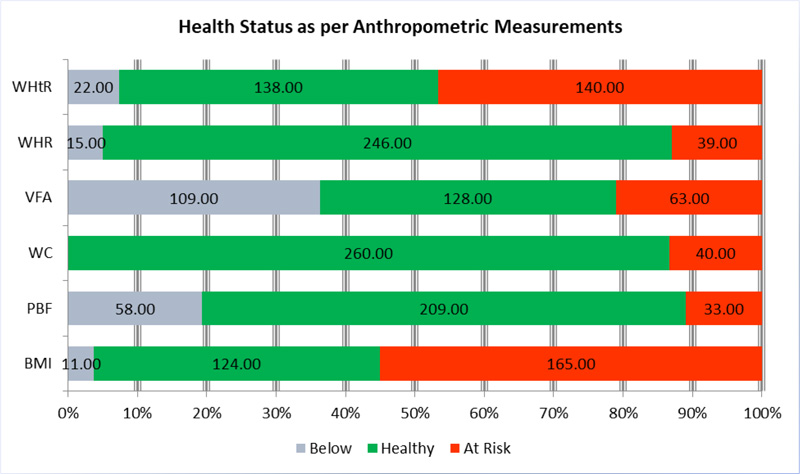
According to the WC, most females (260) were healthy, whereas WHR indicate 246 healthy females, and PBF also indicate 209 females with no health risk. Whereas, WHtR, VFA, and BMI showed more than 50% females were on the health risk either by below or high level of measurement Table 1.
According to Table 2, among all female students for selected variables, 55 participants fell at risk and 33 participants at a high-risk category of BMI as well as for PBF, WC, VFA, WHR, and WHtR. While there are many participants, who also are at-risk category according to a particular parameter such as 174(58%) for PBF, 40(13.33%) for WC, 63(21%) for VFA, 189(63%) for WHR, and 140(46.67%) for WHtR.
Table 3 shows that the p-value is .000 for all variables; the association between BMI and other variables is significant. From the R column in the table, the correlation coefficient, R, is .938, .963, .762, .907, .917 and .941 for PBF, WC, HC, VFA, WHR and WHtR, respectively. Therefore, we can conclude that BMI is positively associated with other variables, and the association is strong (R is positively and very closed to 1). From column B, we can conclude that on average for every number of BMI, they get 1.305, 1.809, .747, 6.562, .012, and .011 chance of health risk for other variables.
4. DISCUSSION
The present study investigated how anthropometric parameters (WC, VFA, PBF, and WHR) were associated with BMI (Fig. 2). Elevated BMI level or other anthropometric parameters is the alarm for different health complications and cardiovascular diseases such as diabetes, hypertension, types of cancer, sleep apnea, fatty liver, and kidney disease. In this study, we found a positive, strong association between BMI and WHR in female students, and the association between BMI and anthropometric parameters was positively significant.
| Anthropometric Measure | n | Mean | SD |
|---|---|---|---|
| Age (Year) | 300 | 20.80 | 5.23 |
| Height (cm) | 300 | 157.07 | 5.78 |
| Body Mass (kg) | 300 | 57.45 | 13.25 |
| BMI | 300 | 23.18 | 4.70 |
| PBF (%) | 300 | 30.10 | 6.58 |
| VCA (cm2) | 300 | 59.12 | 34.20 |
| WC (cm) | 300 | 76.87 | 8.88 |
| WHR | 300 | 0.78 | 0.78 |
| WHtR | 300 | 0.49 | 0.06 |

| Participants' Risk Status in Line with Body Mass Index and Selected Variables | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| - | BMI | Total | ||||||||
| Under Weight | Healthy | At-Risk | At High Risk | |||||||
| PBF | Under | 9 | 2 | 0 | 0 | 11 | ||||
| Ideal | 35 | 80 | 0 | 0 | 115 | |||||
| At-Risk | 1 | 87 | 55 | 31 | 174 | |||||
| Total | 45 | 169 | 55 | 31 | 300 | |||||
| WC | Under | 45 | 162 | 11 | 0 | 218 | ||||
| Healthy | 0 | 7 | 33 | 2 | 42 | |||||
| At-Risk | 0 | 0 | 11 | 29 | 40 | |||||
| Total | 45 | 169 | 55 | 31 | 300 | |||||
| VFA | Low | 45 | 64 | 0 | 0 | 109 | ||||
| Adequate | 0 | 104 | 22 | 2 | 128 | |||||
| At-Risk | 0 | 1 | 33 | 29 | 63 | |||||
| Total | 45 | 169 | 55 | 31 | 300 | |||||
| WHR | Under | 18 | 2 | 0 | 0 | 20 | ||||
| Healthy | 27 | 64 | 0 | 0 | 91 | |||||
| At-Risk | 0 | 103 | 55 | 31 | 189 | |||||
| Total | 45 | 169 | 55 | 31 | 300 | |||||
| WHtR | Under | 18 | 3 | 1 | 0 | 22 | ||||
| Healthy | 27 | 109 | 2 | 0 | 138 | |||||
| At-Risk | 0 | 57 | 52 | 31 | 140 | |||||
| Total | 45 | 169 | 55 | 31 | 300 | |||||
| - | PBF | WC | VFA | WHR | WHtR |
|---|---|---|---|---|---|
| R | .938 | .963 | .907 | .917 | .941 |
| Adjusted R Squares | .879 | .928 | .823 | .884 | .941 |
| F | 2174.37 | 3856.14 | 1390.51 | 1578.47 | 2290.73 |
| Significant | .000 | .000 | .000 | .000 | .000 |
| B | 1.305 | 1.809 | 6.562 | .012 | .011 |
| Std. Error | .028 | .029 | .176 | .000 | .000 |
This research reported that WHtR was the second-highest risk factor for 140 female students, and it confirmed is from Fig. (1) and Table 1. Earlier researches indicated that WHtR was better than the WC and BMI in predicting blood lipid abnormalities in the Chinese population [14]. A cross-sectional study indicated that WHtR was the strongest predictor for CKD, followed by BMI and WC [15]. A meta-analysis supported that WHtR significantly better than WC for CVD, hypertension, and another outcome for women and men [16].
CONCLUSION
The results indicated that the visceral fat area was the third highest risk factor, with 63 female students according to Table 1 and Fig. (1). Visceral fat area is not only a predictor of hypertension but also a crucial factor of many severe diseases. A study revealed that a higher percentage of participants with VFA ≥100 cm2 had diabetes, hypertension, obesity, hypertriglyceridemia, and hypo-HDL cholesterolemia in the Romanian population [17]. Hayashi et al. investigated a study for 10-11 years with adult participants and found that an increase of VFA is associated with a 3.82 higher risk of developing impaired glucose tolerance. The association remained statistically significant after adjustment for the total subcutaneous fat area, total fat area, or abdominal subcutaneous fat area [18].
According to the findings of this research, Fig. (1) shows that 40 female students at risk. While Table 1 showed, only 80 female students were on health risk with WC. A meta-analysis and systematic review reported that WC is superior to WHR, and WHR is a more reliable measure for abdominal obesity and visceral fat [19]. World Health Organization recommended that the risk of cardiovascular disease and type II diabetes is better diagnosed when using both WC and BMI [20] while other studies showed that visceral fat is a more reliable predictor of hypertension than BMI [21].
It is demonstrated that 189 female students according to Table 1 and Fig. (1), only 39 female students were on health risk associated with WHR. A meta-analysis was conducted with twelve case-control studies in fourteen eligible trails and showed that higher WHR were more strongly prognostic of myocardial infarction risk in females [22]. Some studies suggested that WC, WHR, WHtR, and central obesity index are the risk factors for foreseeing myocardial infraction, which might additionally overcome the BMI limitation [23]. The WHR more clinically relevant than BMI and evidence increased attention, particularly in terms of the acute onset of disease, to reduce the risk of morbidity.
Percentage of body fat was the least health risk factor with only 33 female students as per Fig. (1) and Table 1 also indicated that 174 female students were on health risk. Bohn et al. found PBF and BMI were similar in predicting hypertension, but the correlation between blood pressure and BMI was stronger than PBF [24]. A study by Romero-Corral et al. indicated that individuals with high body fat but a healthy weight were more predisposed to diabetes mellitus II than those who were overweight but had average fat mass [25]. A study with two measures of obesity (BMI & PBF) performed on the Thai population. The study showed that Thai women have higher PBF and its associated with cardiometabolic risk profiles [26].
The study concludes that there is a positive strong association between BMI and other anthropometric variables, which is also statistically significant. All these anthropometric obesity variables might be the causes of many health risks such as cardiovascular disease, diabetes, hypertension, type of cancer, sleep apnea, fatty liver, and kidney disease for females. Despite the limitations of this study by gender, area, and population-specific, it provides further insight into the obesity-related health risks. This observation is not only essential to find out the level of anthropometric parameters but also to draw the attention of students and public health authorities involved in planning the prevention, management, and educate the communities.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by the Ethics Committee of Deanship of scientific research, Imam Abdulrahman bin Faisal University, Saudi Arabia with approval number IRB-2017-03-165.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
Written informed consent was obtained from each participants prior to the study.
AVAILABILITY OF DATA AND MATERIALS
Not applicaple.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

