All published articles of this journal are available on ScienceDirect.

Factors Associated with Suicidal Ideation, and Attempt Among Cancer Patients in Ayder Comprehensive Specialized Hospital: Cross-Sectional, Mekelle, Ethiopia
Abstract
Background:
Cancer patients are at high risk for suicide, particularly, when they are informed about the cancer diagnosis. However, there is a limited study in Ethiopia therefore, assessing suicidal ideation, attempt, and its associated factors are needed for intervention.
Methods:
An institutional-based cross-sectional study was conducted from March to June 2019 at Ayder comprehensive specialized hospital with a total of 297 participants. Suicide module of the World Mental Health (WMH) survey initiative version adopted from the World Health Organization (WHO) and used to assess suicidal ideation and attempt. Binary logistic regression analysis employed to identify factors associated with suicidal ideation and attempt. Odds ratio with 95% CI and P-value <0.05 was applied to identify significantly associated factors.
Results:
The lifetime prevalence of suicidal ideation and the attempt was found to be 27.9% [95%CI (22.3, 31.6)] and 8.4% [95%CI (5.2, 10.3)] respectively. Being female [AOR= 2.23, 95%CI (1.27, 3.92)], stage IV cancer [AOR=2.08, 95%CI(1.47, 3.81)], having depression and anxiety [AOR=2.31, 95%CI(1.24,4.32)], poor social support [AOR=3.70, 95%CI(2.01,6.78)], and level 4 performance status [AOR=3.73, 95%CI(1.71, 8.13)] were the factors associated with lifetime suicidal ideation. While being in level 4, performance status was also significantly associated with suicidal attempt.
Conclusion:
Both suicidal ideation and attempt among cancer patients are high. The suicidal ideation had a statistical association with sex, stage of cancer, having depression and anxiety, social support, and level of performance. Therefore, health education for early screening and treatment for depression and anxiety, and giving social support are crucial for the reduction of suicide.
1. INTRODUCTION
Suicide means the act of a person intentionally causing his or her death. A suicide attempt is a known habitual act with the nonfatal outcome that is deliberately initiated and performed by the individual [1,2]. Cancer is a disease with abnormal cells growth, reproducing uncontrollably and invading nearby tissue by spreading to other parts of the body through bloodstreams and lymphatic systems. Worldwide, about 25 million people are living with cancer. Each year, 7 million people die from it. The World Health Organization (WHO) estimated in 2011 that 34% of the Ethiopian population is dying from a non-communicable disease, with a cancer prevalence of 40%[3-6].
Cancer patients are at high risk for suicide, particularly when they are informed about the cancer diagnosis or hospitalized for cancer treatment [7]. The risk of attempted and completed suicide among cancer patients is much higher than the general population [8,9]. Various studies have reported that the diagnosis of cancer is two to five times the risk factor for suicide when compared to the general population [5,6,9,10], with 8.5% to 26% of terminal cancer patients have a higher level of the “desire for hastened death [11].
A study conducted in the United Kingdom showed that 7.8% of cancer outpatients have suicidal ideation [12], while 10.9% of breast cancer patients undergoing surgery in Korea [9], and 8.6% of terminal cancer outpatients in Japan [13] have suicidal ideation, with its variation, ranging from 0.8 to 71% in non-psychiatric populations of cancer patients compared to 1.1 and 19.8% suicidal ideation in the general population [14].
The finding of this study shows that 15.3% cancer inpatients of Chinese general hospitals in the Tianjin area reported having suicidal ideation the previous month [7]. The prevalence found in Chinese cancer inpatients is similar to that reported in other cohorts, including the 17.7% prevalence in a population-based sample of American cancer patients [15], the 15% prevalence in Japanese patients with unrespectable lung cancer in Japan [13], the 18.1% prevalence in Chinese gynecological cancer patients [7], Korean stomach cancer survivors (34.7%)[9], and another study in Korea 20.1% [11] have suicidal ideation. While a study conducted in Turkey showed the prevalence of suicide attempts in cancer patients was 12.74% [5].
A study was carried out in Turkey including 102 patients who were under treatment in the oncology department and the control group included 100 individuals with similar socio-demographic features shows suicide attempts were correlated with depression, anxiety, low level of perceived social support, and advanced stage cancer. Multi-center study performed in Korea showed that poor performance status and having co-morbidity were associated with suicidal ideation and attempt. Performance Status (PS) is a standard functional classification in oncology research and practice. Performance status scores are based on a patient’s ability to perform daily activities and are designed to provide a measure of impairment as a function of cancer. Poor Performance status (defined as Performance status on Eastern Cooperative Oncology Group (ECOG) 2-4 on a 0-4 scale) was determined among cancer patients.
A survey of consecutive patients who attended the outpatient clinics of a regional cancer center in Edinburgh, United Kingdom, shows significant emotional distress, substantial pain, and older age, were associated with a positive response for suicide. Alcohol use, previous suicide attempts, metastatic cancer, palliative care, being male, single, unemployed, diagnoses of more severe types of cancer were significantly associated with suicidal ideation. Additionally, a higher risk of suicidal behavior or ideation was observed during the first 5 years following the initial diagnosis of cancer, and with emotional distress such as depression, hopelessness, anxiety, post-traumatic stress disorder [2, 5, 11, 12, 14, 16-18].
Male patients seem to have a higher suicide risk than females [13]. Cohort studies were carried out among Danish cancer patients which revealed the risk of suicide increase immediately after cancer diagnosis [17 , 19]. Commuting suicide was highest during the first 3 months after the cancer diagnosis for men and from 3 month to 1 year after the diagnosis for women [19].
Patients with terminal cancer have the highest level of hopelessness [15], a powerful predictor of suicidality in cancer patients [8]. In some previous studies, cancer site is also reported to be associated with an increased risk of suicidality [20 , 21].
Despite the rapidly increasing morbidity of cancer [2], to the best of our knowledge, there have been no published studies on the prevalence and associated factors of suicidality among cancer patients in Ethiopia. Therefore, this study assesses the prevalence of Suicidal ideation, attempt, and associated factors among cancer patients.
2. METHODS AND MATERIALS
2.1. Study Design and Area
Institutional based cross-sectional study was conducted from March to June 2019, at Ayder comprehensive specialized hospital, Mekelle, Tigray, Ethiopia. Ayder comprehensive specialized hospital is one of the biggest teaching and referral hospitals in the Tigray region.
2.2. Sampling Technique and Sample Size Determination
We surveyed the cancer patients who are available during the study period. The total numbers of participants were 297 cancer patients available during the data collection period. Data were collected by psychiatric nurses with interviewing clients by using a semi-structured questionnaire and clinical factor-related questioners.
2.3. Operational Definitions
2.3.1. Suicidal Ideation
Is defined as if the respondent answers the question have you ever seriously thought about suicide? If the answer is yes, the respondent has suicidal ideation.
2.3.2. Suicidal Attempt
Is defined as if the respondent answers the question, have you ever attempted suicide? If the answer is yes, the respondent has a suicidal attempt.
2.3.3. Depression and Anxiety
Hospital Anxiety and Depression Scale (HADS) score ≤ 10 shows no or borderline depression or anxiety and score ≥ shows the presence of depression and anxiety.
2.3.4. Social Support
Individuals who scored ≥ 9 (moderate and strong social support) on the Oslo 3-item social support scale.
2.4. Data Collection Instrument
The presence of suicidal ideation and attempt among cancer patients was assessed by using the World Mental Health (WMH), adapted from the World Health Organization (WHO) Composite International Diagnostic Interview (CIDI). Depression and Anxiety were assessed using HADS (Hospital Anxiety and Depression Scale).
Social support was assessed by using the Oslo-3 social support scale. Performance status was assessed using the Eastern Cooperative Oncology Group (ECOG). A semi-structured questionnaire was used to collect socio-demographic characteristics and some clinical factors.
2.5. Data Collection Tools and Quality Controls
Data was collected by interviewing patients during a routine follow-up visit. Training for data collectors was given on how to collect data. A pre-test was conducted on 5% of the sample size. The collected data were checked daily for completeness and consistency.
2.6. Data Processing and Analysis
The coded data were entered, checked, and cleaned with Epi data 3.1 and analyzed using Statistical Package for the Social Sciences (SPSS) version 20. Descriptive summary using frequencies, percentages, and graphs were used to present study results. Bivariate analysis was done for Crude Odds Ratio (COR) and multivariate analysis was employed to calculate Adjusted Odds Ratio (AOR).
The strength of the association was presented by the odds ratio with a 95% Confidence Interval (CI). P-value < 0.05 was considered statistically significant in our study.
3. RESULTS
3.1. Socio-Demographic Characteristics
A total of 297 cancer patients were included in the study with a response rate of 98%. Among respondents, 150(50.5%), 227(76.43%), 244(82.13%), and 184(61.95%) were male, orthodox, Tigrian, and married respectively (Table 1).
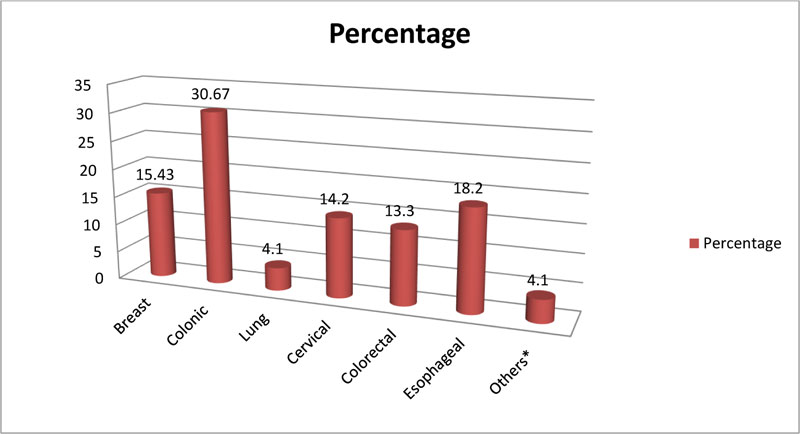
3.2. Clinical Characteristics of the Respondents
Of the participants, 23(7.8%), 132(44.4%), 59(19.9%), and 83(27.9%) of respondents were found to have stage I, II, III, and IV cancer, respectively. More than half of study participants; 184(61.95%) had a duration of illness ≤ 1 year. One hundred eighteen (39.7%) of participants were on chemotherapy treatment (Table 2). Regarding the type cancer, 46(15.43%) of participants had breast cancer (Fig.1).
3.3. Prevalence of Suicidal Ideation and Attempt
The prevalence of suicide ideation and attempt among 297 respondents was 83(27.9%) and 25(8.4%), respectively. Of the respondents, 28(37.73%), and 8(32.0%) reported to have suicide ideation, and attempted for ≤ 6 months, respectively (Table 3).
| Variables | Category | Frequency(n=297) | Percent (%) |
|---|---|---|---|
| Age | 18-27 28-37 38-47 >=48 |
44 68 78 107 |
14.8% 22.9% 26.2% 36.1% |
| Sex | Male Female |
150 147 |
50.50 49.50 |
| Religion | Orthodox Muslim Other |
227 58 12 |
76.43 19.52 4.05 |
| Ethnicity | Tigrigna Amhara Afar |
244 32 23 |
82.13 10.17 7.70 |
| Marital status | Single Married Divorced Widowed |
54 184 38 23 |
18.18 61.95 12.79 7.08 |
| Education status | Non -educated Reading and writing Primary Secondary Diploma and above |
18 97 78 45 59 |
6.10 32.65 26.26 15.13 19.86 |
| Occupation | Unemployed Governmental Private Farmer Student Other |
25 60 110 42 48 12 |
8.41 20.21 37.04 14.14 16.16 4.04 |
| Living status | With family Alone |
238 59 |
80.13 19.87 |
| Monthly income | <1500 1500-4000 4001-7000 >7001 |
78 75 96 48 |
26.26 25.25 32.33 16.16 |
| Variables | Category | Frequency(n=297) | Percent (%) |
|---|---|---|---|
| Type of treatment | Chemotherapy Surgery Combined |
118 122 57 |
39.70 41.10 19.20 |
| Duration of illness | ≤1years 1-5years ≥5years |
184 90 23 |
61.95 30.30 7.75 |
| Duration of treatment | ≤1month 1-3month 3-6month 6-12month ≥12month |
21 40 114 92 30 |
7.10 13.46 38.37 30.97 10.10 |
| Do you have pain | Yes No |
168 129 |
56.56 43.44 |
| If yes did it interfere with daily activity | Yes No |
63 105 |
37.5 62.5 |
| Comorbid medical illness | Yes No |
38 259 |
12.80 87.20 |
| Family history of suicide | Yes No |
31 266 |
10.43 89.57 |
| Depression and anxiety | No, and Borderline* Has depression and anxiety |
25 272 |
8.42 91.58 |
| Ever use substance | Yes No |
43 254 |
14.47 85.53 |
| Which substance? | Alcohol Cigarette Chat Other |
20 9 10 4 |
46.51 20.93 23.26 9.30 |
| Ever use the substance within this three month | Yes No |
29 268 |
9.76 90.24 |
| Which substance | Alcohol Chat Other |
12 13 4 |
41.37 44.84 13.79 |
| How many people are you so close to counting on them during great personal problem? | None 1-2 3-5 ≥5 |
32 132 112 21 |
10.74 44.45 37.71 7.10 |
| How much interest do people show in what you do? | very little Little Uncertain Some A lot |
30 52 21 122 72 |
10.10 17.50 7.10 41.10 24.20 |
| How easy is to get practical help from neighbors if you should need it? | Very difficult Difficult Possible Easy Very easy |
50 70 58 84 35 |
16.82 23.57 19.53 28.30 11.78 |
| Oncology performance status | Fully active Restricted in some 50% or more working hour Limited activities |
88 148 40 21 |
29.63 49.83 13.47 7.10 |
| Variables | Category | Frequency(n=146) | Percent (%) |
|---|---|---|---|
| Ever serious thought about commuting suicide | Yes No |
83 214 |
27.94 72.06 |
| Duration of ever serious thought | <=6monthg 6-12month 1-5years >5years |
28 38 10 7 |
33.73 45.78 12.05 8.44 |
| Ever thought of suicide within this 1 month | Yes No |
17 280 |
5.72 94.23 |
| Ever made a plan for commuting suicide | Yes No |
29 268 |
9.76 90.23 |
| Duration of an ever made plan for commuting | <6month 6-12month |
12 17 |
41.37 58.63 |
| Ever attempt of suicide | Yes No |
25 272 |
8.42 91.58 |
| Method used | Hanging Poisoning Jumping from a high place |
6 10 9 |
24.0 40.0 36.0 |
| Duration of ever attempting suicide | <=6month 6-12month >5years |
8 10 7 |
32.0 40.0 28.0 |
| Number of suicide attempted | Once Twice |
14 11 |
56.0 44.0 |
| Ever attempt suicide with this 1 month | Yes No |
7 290 |
2.35 97.65 |
| Reason for attempting suicide | Economic problem Death in the family Mental illness Physical illness |
2 5 8 10 |
8.0 20.0 32.0 40 |
3.4. Bivariate Analysis
On bivariate logistic regression, sex, stage of cancer, having pain, depression and anxiety, social support, and performance status were statistically significant at p-value < 0.05 for suicidal ideation and attempted into multivariate binary logistic regression analysis.
3.5. Multivariate Analysis
During the multivariate analysis, sex, stage of cancer, having depression and anxiety, social support, and performance status were found to be statistically significant. Being female was more than two times more likely to have suicidal ideation as compared to male patients with the odds of [AOR=2.23, 95%CI (1.27, 3.92)]. Current stage IV cancer was two times more likely to have suicidal ideation as compared to stage I cancer patients with the odds of [AOR=2.08, 95%CI (1.47, 3.81)] (Table 4).
4. DISCUSSION
Cancer is associated with an increased rate of suicidal acts, suicidal attempts, and suicidal ideation. This leads to commuting complete suicide. The prevalence of suicidal ideation and attempt was 27.9% 95%CI [22.3-31.6], and 8.4% 95%CI [5.2-10.3], respectively. The prevalence of suicidal ideation was higher than the result from studies in the United Kingdom 7.8%[10], Korea 10.9, and 20.1[7,9], Japan 8.6%[14], and 15%[15], Chinese 15.3%[5], and 18.1% [20] the United States 17.7%[18], and lower than a study conducted in Korean 34.7%[7]. The finding of suicidal ideation was lower than the study conducted in Turkey at 12.74%[3].
The prevalence difference in these studies may be due to the difference in sampling methods and design (i.e., case-control, correlation), in the type of cancer (i.e., patients with one type of cancer only vs. various types of cancer), and the study settings (i.e., institutional-based vs. community-based), and in developed countries like Turkey screen early for suicide which gives an increase in prevalence.
Regarding factors associated with suicidal ideation, the result of this study shows that being female was 2.23 times more likely to have suicidal ideation when compared to males. This finding was supported by studies conducted in Korea (26). This might be because females have high suicidal ideation than male counterparts as supported by DSM 5 and other psychiatry books.
The odds of suicidal ideation among stage IV cancer patients were found to be 2.08 times more likely to have suicidal ideation when compared with stage I cancer. This finding was in line with the study conducted in Turkey [3], and Japan(27). This could be due to as the stage of the disease progresses the patient becomes hopeless and end the hope of living.
Patients having depression and anxiety were 2.31 times more likely to have suicidal ideation as compared with those who don’t have borderline depression and anxiety. This finding was in line with various studies like the study conducted in China (20), Japan(15), and(14), USA(28), and the UK (12). This could be due to patients having depression and anxiety was at high risk of suicidal ideation.
| Explanatory Variables | Suicidal ideation | COR (95% CI) | AOR (95% CI) | ||
|---|---|---|---|---|---|
| Yes | No | ||||
| Sex | |||||
| Male | 40 | 84 | 1.00 | 1.00 | |
| Female | 107 | 66 | 3.40(2.09,5.93)*** | 2.23(1.27,3.92) ** | |
| Stage of Cancer | |||||
| Stage I | 9 | 14 | 1.003 | 1.00 | |
| Stage II | 59 | 73 | 1.70(1.03,2.73)* | 1.11(0.56,1.98) | |
| Stage III | 19 | 40 | 0.73(0.16, 3.40) | 0.47(0.24,0.86) | |
| Stage IV | 60 | 23 | 22(2.04,5.80)*** | 2.08(1.47,3.81)** | |
| Do you have pain | |||||
| Yes | 93 | 75 | 1.72(1.08,2.73)* | 1.53(0.82,2.84) | |
| No | 54 | 75 | 1.00 | 1.00 | |
| Depression and Anxiety | |||||
| No, and Borderline | 32 | 74 | 1.00 | 1.00 | |
| Have depression and anxiety | 115 | 76 | 2.65(1.60,4.35) *** | 2.31(1.24,4.32) ** | |
| Social support | |||||
| Yes | 41 | 108 | 1.00 | 1.00 | |
| No | 106 | 42 | 6.64(4.00,11.03)*** | 3.70(2.01,6.78)*** | |
| Oncology performance status | |||||
| Fully active | 26 | 62 | 1.00 | 1.00 | |
| Restricted in some | 24 | 124 | 2.16(3.60, 9.51) | 1.47(0.82, 2.66) | |
| 50% or more working hour | 20 | 20 | 1.38(0.74, 2.55)* | 1.45(0.67, 3.12) | |
| Limited activities | 8 | 13 | 8.09(4.39, 14,92)* | 3.73(1.71, 8.13)** | |
The odds of suicidal ideation among participants with poor social support were found to be3.7 times higher as compared to participants with good social support. This finding was supported by studies conducted in China (20), and Canada (29). Social support is one of the protection factors for any mental illness including depression. Therefore those who lack social support were at high risk of depression which leads to suicidal ideation.
Participants with limited performance status were 3.73 times more likely to develop suicidal attempts and ideation as compared with those having fully active status. This finding was in line with a study conducted in the USA(28), Japan (14), UK (12), Canada (29), and Korea(9). This might be due to the reason that a patient who was actively engaging in their daily life becomes dependent on others and they feel hopeless and thinking of ending their life.
CONCLUSION
The prevalence of suicidal ideation and attempt among cancer patients was found to be high, indicating how suicide in cancer patients is a public health problem. Being female, stage IV cancer, having depression and anxiety and lack of social support was associated with suicidal ideation while poor performance status has been associated with suicidal attempt and ideation. Therefore those patients have to find out professional help in early screening and treatment for depression and anxiety, giving social support, and health education on the identification of cancer before progression, especially on females, is crucial for the reduction of suicide.
LIMITATIONS
This study was a cross-sectional study design that cannot show the temporal cause-effect association between factors and suicide. Since this study surveys the whole patient during the study period its default to generalize outside of the study area.
LIST OF ABBREVIATIONS
| AOR | = Adjusted Odds Ratio |
| CI | = Confidence Intervals |
| COR | = Crude Odds Ratio |
| HADS | = Hospital Anxiety and Depression Scale |
| OSS-3 | = Oslo-3 Social Support Scale |
| SPSS | = Statistical Package for Social Sciences |
| W.H.O | = World Health Organization |
AUTHORS' CONTRIBUTIONS
TA has designed the study, contributed in analysis and draft of the manuscript, interpretation, and wrote up. WG has participated in data collection; write up, analysis, and interpretation. ZW contributed to data collection; write up, analysis, and interpretation. All authors have read and approved the final manuscript.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical approval was obtained from the ethical review board of Mekelle University, College of Health Science, Ethiopia.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
Written consent taken from the participants for their voluntary participation after a complete description of the study was provided to them. The participant's profile was omitted for confidentiality.
AVAILABILITY OF DATA AND MATERIALS
The authors confirm that the data supporting the findings of this study are available within the article.
FUNDING
Mekelle University has financially supported the process of data collection. The funder has no role in the design and outcome of the study.
CONFLICT OF INTEREST
The authors declare no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
ACKNOWLEDGEMENTS
We would like to give sincere thanks to Mekelle University for financial support in conducting the research. They also would like to extend their appreciation to data collectors and study participants.

