All published articles of this journal are available on ScienceDirect.

Knowledge of Non-communicable Disease Risk Factors among Community Health Workers in South Africa
Abstract
Introduction:
Community Health Workers play an important role in supporting patients with chronic non-communicable diseases (NCDs), therefore they need to be constantly updated with current knowledge to enable them to perform their activities effectively. The purpose of this study was to assess the knowledge of NCDs risk factors among Community Health Workers (CHWs) in South Africa.
Methodology:
A triple “A” approach (assessment, analysis, and action) was used among 40 CHWs working with patients with chronic non-communicable diseases. All CHWs gave voluntary, informed consent in writing and verbally before they were allowed to participate in the study. For the initial assessment, CHWs completed a questionnaire to assess knowledge about the knowledge of NCDs. The questionnaire was analysed to determine their baseline performance. The findings of the assessment identified shortcomings in the knowledge of CHWs, specifically on diabetes and hypertension knowledge. Feedback was given to the CHWs followed by a short training on healthy living, focusing on the risk factors associated with NCDs (diabetes and hypertension). Training of CHWs was conducted using an adapted national training programme together with CHW prevention of healthy lifestyle modules designed by experts from the School of Public Health, University of the Western Cape. All statistical tests were two-tailed, and p<.05 was considered statistically significant.
Results:
The majority (97.5%) of the CHWs who had their knowledge assessed were women. Fifty-five percent (55%) were within age 30-45 years, while 45% were between the ages 46-60 years. The majority of the participants had secondary school education (92.5%) and 1-15 years of experience (97.5%) as CHWs. The results of the post-training assessment revealed that 48.5%, 63.6%, 42.4%, 72.7%, 42.5%, 57.6%, and 18.2% had poor knowledge of diabetes, hypertension, diabetes complications, hypertension complications, advice for diabetic patient, advice for hypertension, and nutrition advice of NCDs, respectively. Regression analysis showed that those with higher education levels were significantly highly likely to be knowledgeable about hypertension complications (OR=19.6, CI=1.14, 336.0).
Conclusion:
There was poor knowledge of risk factors for NCDs among CHWs. An association exists between the knowledge of risk factors for NCDs and education levels among the participants. There is a need for regular refresher training programs for CHWs to upscale their knowledge about NCDs, coupled with frequent review of CHWs program and curriculum.
1. INTRODUCTION
Non-communicable Diseases (NCDs) are a public health concern globally. Some of the most prominent NCDs are hypertension, diabetes mellitus, Cardiovascular Disease (CVD), cancers, injuries, and chronic respiratory disease [1]. Numerous factors have been cited as contributing to the development of NCDs. These, among others, include unhealthy dietary practices that are influenced by the food environment, physical inactivity, obesity, smoking, and heavy alcohol consumption [2].
The increasing number of people with NCDs has a negative impact to the health system which is already overwhelmed due to the demands of those affected by infectious diseases, lack of human resources, lack of infrastructure and training, thus affecting the system’s ability to adequately counsel people about NCDs and associated risk factors. This situation suggests a need to use an alternative cadre of health workers to fulfil this role. Community Health Workers (CHWs) who are more accessible to community members can play an important role in assisting patients with disease self-management [3]
CHWs are persons who live and work in their community, selected by their community, and accountable to their community [4-9]. CHWs may include skilled nonprofessional workers, health unpaid workers, community health representatives, customary birth helpers, and communal midwives [3, 4]. However, the Sustainable Development Goals (SDGs) have re-positioned fresh importance on scaling up the reduction of NCDs globally, especially in low-to-middle income countries [4]. In many countries, CHWs have been saddle with the responsibility to intervene and render certain basic health services in bettering the health conditions of many individuals. On the other hand, the use of CHWs has been acknowledged as one of the strategies to address the ever-increasing scarcity of health personnel most, especially in the low-to-middle income countries [3]. Puoane et al. [6] pointed out that CHWs could assist many individuals by effectively educating them on several illnesses. This could assist patients and families in lowering healthcare expenses, have access to the relevant information about their illnesses, and help them take necessary precautions by themselves.
The South African government has adopted the Primary Health Care (PHC) re-engineering strategy as a means of strengthening the effectiveness of the current health system. This approach has the potential to address NCDs comprehensively as its focus was on health promotion, disease prevention and referral for curative care to improve health outcomes. This approach could also assist in building the capacity of CHWs in the management of chronic conditions and provide support to CHWs through a professional nurse, health promoter, and environmental officer who form part of the PHC outreach team. Studies have shown that patients exposed to the health education delivered by CHWs had better knowledge when compared to others who had no exposure to CHWs [10-12].
Therefore, regular upscale training to improve CHWs knowledge on NCDs risk factor seems necessary. Although training to increase CHWs knowledge about Cardiovascular Disease (CVD) risk has been previously conducted [6, 13], the knowledge of those who care for the patients must be assessed periodically so that remedial training is given to bridge the identified shortcomings if any. This study assessed the knowledge and practices of CHWs who are working with patients diagnosed with NCDs and their related risk factors, focusing on diabetes and hypertension in Western and Eastern Cape Province of South Africa with the aim of implementing a short training to close the identified gaps in knowledge.
2. MATERIALS AND METHODS
2.1. Research Design
We used a triple‘A’ approach of (i) Assessment (ii) Analysis, and (iii) Action to assess the knowledge of CHWs about risk factors for NCDs before and after the training. The CHWs in the current study were employed by the Non-Government Organisation (NGO) that employs CHWs who are working in Langa, a peri-urban site in Cape Town, and those employed by the Department of health in Mount Frere, a rural site in the Eastern Cape.
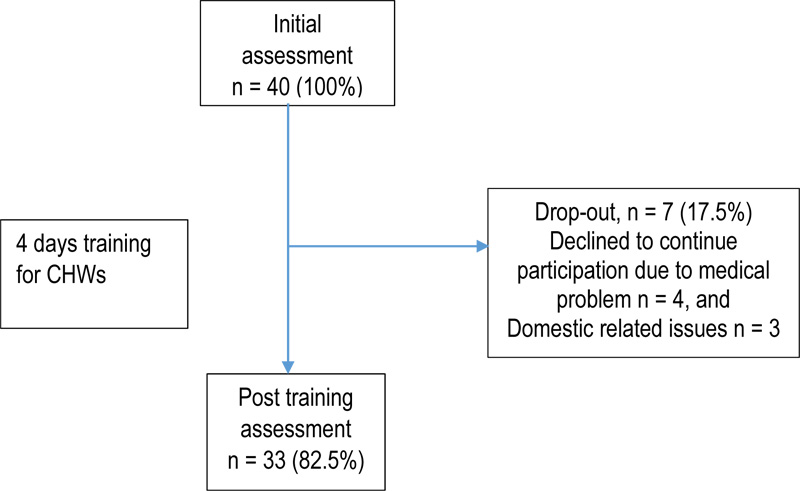
These sites were purposely selected because the researchers have an existing cohort of the PURE study in these communities and have already established a relationship with the CHWs and community members and the researchers are familiar with the setting. A total of 40 (men, n =1; and women, n =39) participants with an average age of 44.8-year-old volunteered to participate in the study. Of the total of 40 participants that were initially assessed, only 33 completed the training, while 7 participants dropped out. All the participants gave voluntary, informed consent in writing and verbally before they were allowed to participate in the study.
2.1.1. Development and Implementation of the Training Programme
2.1.1.1. Training of CHWs
CHWs received four days training programme on healthy living, focusing on the risk factors associated with NCDs (diabetes and hypertension) between 13th and 17th March 2017. In the absence of standardised training curriculum for CHWs in South Africa [6], training of CHWs was conducted using the adapted national training programme together with CHW training manual on the prevention of healthy lifestyle modules developed by the experts from the School of Public Health, University of the Western Cape, to train CHWs in order to strengthen the section on the risk factors associated with chronic diseases, so that it is in line with the study objectives. The training of CHWs focused on the following areas: Chronic illness; Wellness; Healthy lifestyle focusing on nutrition; and Physical activity. In addition to the above, CHWs were trained on using simple motivational interviewing techniques to improve communication with clients. Motivational interviewing is described as a client-centered approach to behaviour change by enhancing intrinsic motivation to change through exploring and resolving ambivalence. This method is based on the principles of evocation and support for personal autonomy [14]. These sessions were conducted in the local vernacular, isiXhosa. Handouts were also provided to the CHWs to help them revise what had been taught in the sessions. Culturally, appropriate educational text messages were also developed by the researcher with the CHWs in line with the national training programme. The goal was to equip and empower the CHWs knowledge of NCDs risk factors to better advise the community members with one or more chronic diseases, especially diabetes and hypertension (Fig. 1).
Data was collected through interviews using an NCDs risk factors knowledge questionnaire. Data collected includes socio-demographic characteristics (age, gender, education, year of employment, training on NCDs, refresher training attended, client counselling and communication), and knowledge of NCD risk factors (Knowledge of diabetes risks, Knowledge of hypertension risks, Knowledge of diabetes complications, Knowledge of hypertension complications, Knowledge of advice for diabetes, and Knowledge of advice for hypertension). All the data were collected in face-to-face interviews by specially trained researchers (Table 1).
2.1.2. Ethical Clearance
Ethical approval was obtained from the University of Western Cape Research Ethics Committee (Ethics number: 15/7/99) before the commencement of the study. Permission to conduct the nested study from which this study was sourced was requested from the International Steering Committee (ISC) of the PURE study and the local Principal Investigators (PI). Data were collected from July to September 2017 by trained fieldworkers.
| Day 1 | Session 1: Introductions Project overview Session 2: • Obesity as a risk factor for chronic diseases • Diabetes and hypertension • Health and wellness(how to prevent chronic diseases) |
| Day 2 | Last sessions overview Session 3: Chronic diseases and exercise Session 4: The role of nutrition in the development of chronic diseases |
| Day 3 | Last session’s overview • Session 5: Motivational interviewing |
| Day 4 | • The way forward- work plan • CHWs will register participants and collect 24-hour dietary recall (Participants will be asked to recall all the food consumed in the last 24 hours). • Field workers will go with CHWs and collect food consumption data in the households. • CHWs will have one on one health education sessions with participants using Motivational Interviewing technique |
| Day 4 | • Re-enforcement of health education through SMS and this will be done weekly. Each month will have a theme, e.g., fat reduction. • Fieldworkers will collect data again on food consumption to ascertain if there have been any changes in nutrition knowledge and dietary intake. • Issuing of attendance certificates • Distribution of CHW manuals with all the sessions |
2.1.3. Data Analyses
Data analyses were carried out using the Statistical Package for Social Science (SPSS) software Version 25.0. All statistical tests were two-tailed, and p<.05 was considered statistically significant. Descriptive statistics, such as mean, SD, and percentages, were used to examine the baseline characteristics of the participants. Frequencies and percentages were calculated to identify the distribution of sociodemographic information. Chi-square test was performed for comparing proportions of categorical variables of the participant’s knowledge of risk factors for NCDs at pre-test and post-test. Multiple logistic regression was performed to identify the associations between the participant’s grade levels or educational status and the knowledge of NCDs risk factors. All sociodemographic and NCDs risk knowledge variables used for the regression analyses were dichotomised into two or three groups. For sociodemographic variables: age (30-45, 46-60); grade/education levels (primary, secondary). For NCDs risk knowledge, that is, knowledge of diabetes risks, knowledge of hypertension risks, knowledge of diabetes complications, knowledge of hypertension complications, knowledge of advice for diabetes, and knowledge of advice for hypertension were categorised into poor, average, and good.
3. RESULTS
Table 2 shows the demographic characteristics of CHWs. The participants studied had an overall mean age of 44.8±9.05 years. Fifty-five percent (55%) were within age 30-45 years, while 45% were between the age 46-60 years. The majority (92.5%) had secondary school education, while 97.5% had years of experience ranging between 1-15 years. The majority (60%) of the participants had previously received training on NCDs. Meanwhile, only 15% of the participants had undergone a refresher course at least one or two times since the last training, while the majority (85%) had never received any refresher training/course. Furthermore, 75% of the participants do discuss with clients to help them make informed choices about their ailment. Similarly, 87.5% always feel the need to tell their clients what to do (Table 2).
The results of the post-training knowledge of diabetes risk revealed that 48.5% of CHWs performed poorly, 45.5% had average knowledge, while only 6.1% had good knowledge. There was, however, no significant difference in the knowledge of diabetes risk among the participants (χ2=2.735; p>0.05). The majority (63.6%) of the participants performed poorly in the knowledge of risk factors for hypertension, 33.3% had average knowledge, while only 3.0% had good knowledge. Chi-square (X2) analysis showed that there were no significant differences in the participant performances for hypertension knowledge risk (χ2=1.399; p>0.05). Meanwhile, 42.4% of the participants performed poorly in the knowledge of diabetes complications, 45.5% had average knowledge, while only 12.1% had good knowledge. Chi-square (χ2) analysis showed that there were no significant differences in the participant performances on the knowledge of diabetes complications (χ2=0.044; p>0.05).
In the knowledge of hypertension complications, the majority of the participants (72.7%) had poor knowledge, while only 27.3% performed averagely. Chi-square (χ2) analysis showed that there were no significant differences in the participant's performances on the knowledge of diabetes complications (χ2=3.407; p>0.05). In terms of the knowledge of what advice to give to diabetic patients, most of the participants performed averagely (51.5%), while only 6.1% had good knowledge. Based on the chi-square (χ2) analysis, there were no significant differences in the participant's performances on the knowledge of advice for diabetic patients (χ2=0.433; p>0.05). Knowledge of advice for hypertension shows that more than half (57.6%) of the participants do not perform well, 36.4% performed averagely while only 6.1 had good performance with chi-square (χ2) analysis showing non-significant differences in the participant's performances (χ2=2.948; p>0.05). Based on the knowledge of nutrition advice for NCDs, the majority (66.7%) performed averagely, while 15.2% had a good performance. The chi-square (χ2) analysis also revealed a non-significant difference in the participant's performance on the knowledge of nutrition advice for NCDs (χ2=3.483; p>0.05) (Table 3).
Table 4 shows the multiple logistic regression analysis of the association between grade levels and the knowledge of the risk factors for NCDs. The results showed that those with higher grade levels were significantly highly likely to be knowledgeable about hypertension complication (OR=19.6, CI=1.14, 336.0)
| Variables | Frequency (n) | M±SD | Percentage (%) |
|---|---|---|---|
| Gender | |||
| Male | 1 | 2.5 | |
| Female | 39 | 97.5 | |
| Age in yr. | 44.8±9.05 | ||
| Age | |||
| 30-45 | 22 | 55.0 | |
| 46-60 | 18 | 45.0 | |
| Grade level | |||
| Primary | 3 | 7.5 | |
| Secondary | 37 | 92.5 | |
| Year of employment | |||
| 1-15 | 39 | 97.5 | |
| 16-30 | 1 | 2.5 | |
| Received training on NCDs | |||
| Yes | 24 | 60.0 | |
| No | 16 | 40.0 | |
| Attend refresher courses | |||
| Yes | 6 | 15.0 | |
| No | 34 | 85.0 | |
| Do client counselling | |||
| Yes | 30 | 75.0 | |
| No | 10 | 25.0 | |
| Always feel need to tell their client what to do | |||
| Yes | 35 | 87.5 | |
| No | 5 | 12.5 | |
| Chronic health condition | |||
| None | 19 | 47.5 | |
| One | 17 | 42.5 | |
| More than one | 4 | 10.0 |
| Variables | Baseline (pre) | End (post) | Chi-square | df | p-value |
|---|---|---|---|---|---|
| Knowledge of diabetes risk | |||||
| Poor | 23 (57.5) | 16 (48.5) | |||
| Average | 17 (42.5) | 15 (45.5) | 2.735 | 2 | 0.25 |
| Good | 0 (0.0) | 2 (6.1) | |||
| Knowledge of hypertension risk | |||||
| Poor | 23 (57.5) | 21 (63.6) | |||
| Average | 13 (32.5) | 11 (33.3) | 1.399 | 2 | 0.49 |
| Good | 4 (10.0) | 1 (3.0) | |||
| Knowledge of diabetes complications | |||||
| Poor | 16 (40.0) | 14 (42.4) | |||
| Average | 19 (47.5) | 15 (45.5) | 0.044 | 2 | 0.97 |
| Good | 5 (12.5) | 4 (12.1) | |||
| Knowledge of hypertension complications | |||||
| Poor | 22 (55.0) | 24 (72.7) | |||
| Average | 16 (40.0) | 9 (27.3) | 3.407 | 2 | 0.18 |
| Good | 2 (5.0) | 0 (0.0) | |||
| Knowledge of advice for diabetic patient | |||||
| Poor | 14 (35.0) | 14 (42.4) | |||
| Average | 23 (57.5) | 17 (51.5) | 0.433 | 2 | 0.80 |
| Good | 3 (7.5) | 2 (6.1) | |||
| Knowledge of advice for hypertension | |||||
| Poor | 15 (37.5) | 19 (57.6) | |||
| Average | 21 (52.5) | 12 (36.4) | 2.948 | 2 | 0.22 |
| Good | 4 (10.0) | 2 (6.0) | |||
| Knowledge of Nutrition advise for NCDs | |||||
| Poor | 13 (32.5) | 6 (18.2) | |||
| Average | 18 (45.0) | 22 (66.7) | 3.483 | 2 | 0.17 |
| Good | 9 (22.5) | 5 (15.2) |
| Variables | 95% CI for Exp. (B) | |||||||
|---|---|---|---|---|---|---|---|---|
| B | S.E | Wald | df | p-value | Exp(B) | Lower | Upper | |
| Knowledge of diabetes risks | 0.74 | 0.51 | 2.12 | 1 | 0.14 | 2.10 | 0.77 | 5.73 |
| Knowledge of hypertension risks | 0.33 | 0.38 | 0.74 | 1 | 0.38 | 1.39 | 0.65 | 2.97 |
| Knowledge of diabetes complications | -0.99 | 0.75 | 1.74 | 1 | 0.18 | 0.37 | 0.08 | 1.62 |
| Knowledge of hypertension complications | 2.97 | 1.45 | 4.21 | 1 | 0.04 | 19.6 | 1.14 | 336.0 |
| Knowledge of advice for diabetes | -0.20 | 0.60 | 0.11 | 1 | 0.73 | 0.81 | 0.24 | 2.68 |
| Knowledge of advice for hypertension | 0.39 | 0.50 | 0.60 | 1 | 0.43 | 1.48 | 0.54 | 4.02 |
| Constant | 0.27 | 1.94 | 0.02 | 1 | 0.88 | 1.31 | ||
4. DISCUSSION
The primary objective of this study was to assess CHWs’ knowledge of NCDs risk. From the initial assessment, it became clear that CHWs were lacking knowledge of diabetes and hypertension and needed another training to be able to support their clients/patients adequately and effectively.
The overall poor knowledge found in this study corroborates the finding of Tsolekile et al. [15], who also found the CHWs score to be poor for diabetes and hypertension. Consequently, CHWs' poor knowledge could lead to providing ill-advised information to patients [16]. Furthermore, the majority of the CHWs seem to apply a general understanding of health conditions when advising the patient assigned to them. Tsolekile et al. [15] and O'Brien et al. [17] observed that CHWs work as a general health worker who seems to cover a wide variety of health services. On the other hand, many of the CHWs sees NCDs management as just a part of the services to be offered [15]. Having no specific full knowledge of managing a particular risk factor could result in a conflict when a new way of managing NCDs is introduced.
Another major concern about the poor knowledge of CHWs in this study could be because most of them have never received or participated in any refresher training program after many years of practice. This could have also led to a lack of knowledge updates, which put many of the CHWs in the dark on how they can effectively manage NCDs. Notably, the lack of required refresher training may, therefore, compromise the efficacy of individual CHWs and add to unpredictable effects [17]. Even if all the CHWs have continuously attended a refresher training, the inability to retain the knowledge gained in such training could still result in ineffectiveness. Studies have shown that for knowledge to be retained, follow-up is necessary in order not to lose the knowledge gained and the ability to perform a specific task [15, 18].
Besides, in some countries, evaluations of CHWs curriculums revealed that CHWs frequently lack the knowledge necessary to carefully and efficiently implement their duties [19]. For example, a study conducted in Nigeria among community health extension workers (CHEWs) on the evaluation of the task to provide family planning education, revealed that the greatest number of these health workers lacked understanding about the expected tasks [19, 20]. This could be due to many outdated courses that continue to provide training that is deficient and without good qualities. Therefore, consistent review of curriculums with specialty and the implementation of a regular quality additional training and follow-up could improve the CHWs competency levels to effectively carry out their responsibilities.
The post-assessment results of the MI training showed that overall, the CHWs performed poorly in the knowledge of NCDs and their associated risk factors, i.e., knowledge of diabetes, hypertension risks, hypertension complications, and advice for hypertension, except for the knowledge of diabetes complication, advice for diabetes patients, and nutrition advice for NCDs where most of the participant had average knowledge. CHWs’ poor performance on NCDs risk factors could be due to their inability to retain the knowledge gained after the training. However, a short time frame between the training and the assessment could also influence CHWs poor performance. Kok et al. [21] reported that good knowledge performance could be related to how an intervention was structured. A well-structured intervention involving a combination of motivations, recurrent guidance or close supervision, constant retraining, and better communication between CHWs and health experts, could lead to better improvement in CHWs knowledge.
The findings from regression analysis showed that every unit increase in the grade level significantly improves the knowledge of hypertension. In another term, the higher the grade levels, the higher the hypertension knowledge. However, there could be other factors militating against the CHWs knowledge. This could be a lack of refresher training needed for knowledge upgrades. Our findings also show that forty percent of the participants did not receive training on NCDs, while the majority (85%) never attend refresher training. O'Brien et al. [17] reiterated that the function of CHWs regularly needs intellectual skills which require an upgrade of educational levels or recognized level of education. Furthermore, in another study which investigated the performance of CHWs in Northern Uganda also found that a reasonably high-grade education level is a necessity to perform well [22]. This reasonably high-grade education level could facilitate a better understanding of basic concepts and stabilise the ability to provide useful explanations and advice to patients [17]. Consequently, without a good qualification and quality training of CHWs, the responsibilities expected to be carried out may be unsuccessful [17].
This study has some limitations. Despite the important information provided in this study, the findings should be interpreted with caution, and due to small sample size should not be generalised. The study was conducted in two provinces (peri-urban in the Langa community in Western Cape and Mount Frere, a rural community in Eastern Cape) of which the data from these provinces were merged. The study participants were also recruited from two different organisations (NGOs and department of health) that involved with NCDs, specifically diabetes and hypertension. Furthermore, the peri-urban site in Cape Town where the study was conducted is well resourced than the Mount Frere community in the Eastern Cape, and could reflect the ability to access training opportunities.
CONCLUSION
The findings of this study revealed a poor performance in the knowledge of risk factors for NCDs among CHWs. Moreover, there was an association between the knowledge of risk factors for NCDs and education grade levels among the participants. The department of health needs to organise regular quality refresher training programs for CHWs to upscale their knowledge about NCDs, coupled with a more frequent review of CHWs program and curriculum. Furthermore, CHWs should not be seen as generalists and should be motivated to effect changes in their various communities.
LIST OF ABBREVIATIONS
| NCDs | = Noncommunicable Diseases |
| CHWs | = Community Health Workers |
| SDGs | = Sustainable Development Goals |
| PHC | = Primary Health Care |
| CVD | = Cardiovascular Disease |
| NGO | = Non-Governmental Organisation |
| PURE | = Prospective Urban Rural Epidemiological |
| PI | = Principal Investigator |
| CHEWs | = Community Health Extension Workers |
| OR | = Odds Ratios |
| CI | = Class Interval |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The research was approved by the University of Western Cape Research Ethics Committee (Ethics number: 15/7/99) and International Steering Committee (ISC) of the PURE study and the local Principal Investigators (PI).
HUMAN AND ANIMAL RIGHTS
No Animals were used in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
All the participants who participated were informed verbally about the study and those who gave written informed consent were enrolled.
AVAILABILITY OF DATA AND MATERIALS
The authors confirm that the data supporting the findings of this study are available within the article.
FUNDING
Financial support to implement the study was partly provided by the South African National Research Foundation (NRF) and the Department of Science and Technology (DST) Centre of Excellence on Food Security. The authors also thank the National Research Foundation (NRF) of South Africa for providing S&F - DST/NRF Freestanding Postdoctoral Fellowships Grant (Grant reference/Number SFP180413320381/116715) support to Dr. SO Onagbiye. Opinions, findings, conclusions, and recommendations expressed in this paper are those of the authors, and the funders accept no liability whatsoever in this regard.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The authors would like to thank all the participants in this study. The authors would also like to thank all the experts from the UWC School of public health who contributed to the development of the module. Non-Government Organisation, which employs CHWs who are working in Langa and Department of health in Mount Frere, was also appreciated.

