All published articles of this journal are available on ScienceDirect.

Lessons Learned to Control COVID-19 to Prevent a Crisis: The Case of Iran
Editorial
Following the detection of the first case of infection due to COVID-19 in Iran central province (named Markazi) on 18 Feb 2020, a serious alert was announced at Arak University of Medical Sciences (the main medical university in Markazi province) to prevent a disaster. The performed measures played a unique role in improving patient care and prevention and control of the disease. Previously, it was expected that Markazi province, due to being situated on the junction of the national highways and placing in the center of Iran, was faced with huge health and social crisis. However, fortunately, the disease morbidity and mortality have been placed in a stabilized status after 7 weeks of the epidemic.
1. INTRODUCTION
Following detection of the first case of infection due to COVID-19 in the Iran central province, named Markazi, on 18 Feb 2020, a serious alert was announced at Arak University of Medical Sciences, the main medical university in Markazi province. Holding coordination sessions in the province authorities, forming Rapid Response Teams (RRTs), and screening COVID-19 among the total population by Primary Health Care (PHC) teams were among the main performed measures. These measures finally indicated a positive impact on the prevention and control of COVID-19 in the province.
2. MEASURES
To expose the situation, the first session of passive biodefence on COVID-19 was held on 19 Feb 2020, and the proposals on prevention and control were enacted and issued. The aim of passive biodefence sessions is to prevent human morbidity and mortality and also to reduce the vulnerability of the infrastructures [1]. A workgroup to increase coordination and cooperation between the governmental and non-governmental organizations was set up two weeks prior to the diagnosis of the first case of COVID-19 in the province. Consequently, promoting coordination among different sectors, holding educational sessions for the healthcare representatives of organizations and industries, preparation and distribution of learning aids among the population and extensive campaign using radio, television and newspaper facilities were put on the table for action.
The number of RRTs, which were consisted of experts in environmental and public health as well as general physicians, was doubled at the provincial and city level. Additionally, reserve teams were predicted for emergency situations. Different scenarios were defined for RRTs and they were trained to face a probable crisis. When positive cases of COVID-19 were reported, RRTs were dispatched immediately to the location to find cases and to provide general and personal training on COVID-19 prevention and also for proper use of disinfectants. Likewise, World Health Organization (WHO) RRTs were deployed in Italy in March 2020 to study disease development, identify and test suspected cases, support the national response, assess patient treatment at hospitals and finally to provide recommendations on quarantine [2].
In addition to RRTs, other PHC teams, including health experts in family, teenagers, young, school, occupational and non-communicable diseases, provided the required educations for pregnant women, middle-aged and elderlies, students, industry employees and people with underlying diseases. Mental health experts provided psychological support for the patient and their family members. It is worth noting that before the province-level warning announcement to be issued, the first arrangements, including the formation of core educational teams, and supply and equipment of healthcare and laboratory centers, were performed.
Among other important measures that improved COVID-19 surveillance system indices was preparing diagnostic COVID-19 kits. Preparation of diagnostic kits and promoting the laboratory biosafety were performed by virologists and the university leadership. Assessment of the first samples suspected to COVID-19 and approving or rejecting them were performed using this laboratory. These and other measures performed by the virology laboratory of Arak University of Medical Sciences caused it to be introduced as the second COVID-19 laboratory in Iran after the reference national laboratory, namely Pasteur Institute of Iran.
The announcement of the positive cases was made so that the laboratory results were reported to the health deputy through SMS in 24 hours and then were announced to the authorities of the related city healthcare centers to start the patient and their relatives’ follow-ups. Then, RRTs followed the patient and its network contact. The patient relatives were also tested for COVID-19 at the province-level moreover than the city level.
On the basis of predicting an increase in the prevalence of COVID-19 and the emergence of more severe situations, it was decided by the university and national authorities to perform screening of the suspected people using rural and urban PHC centers. Standard disease surveillance system divides screening measures to passive screening (self-declaration) in which people themselves refer to the PHC centers, and active screening, which is performed for the contact network of the patient over a 14-days period and also for high-risk groups including elderlies, pregnant women, people with high blood pressure, diabetic and cardiovascular patients and lastly for other population [3]. Arak University of Medical Sciences performed both active and passive screening to identify the suspected cases of COVID-19. After this, on the basis of the national protocol for the diagnosis and treatment of COVID-19, the cases were divided into outpatient and inpatient groups [4].
CONCLUSION
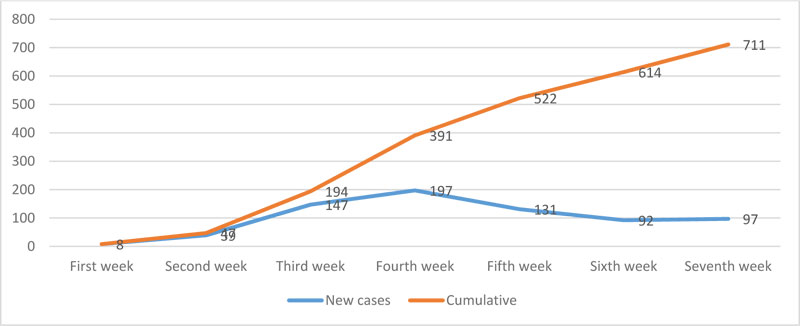
The performed measures have played a unique role in improving patient care and prevention and control of COVID-19. Previously it was expected that Markazi province, due to being situated on the junction of the national highways and also proximity to Qom province as the epicenter hub of COVID-19, was faced with huge health and social crisis. However, fortunately, the disease morbidity and mortality have been placed in a stabilized status after 7 weeks of the epidemic. In this regard, new cases and cumulative frequency of COVID-19 in Markazi province are shown in Fig. (1), which is an indication of a decreasing trend in the diagnosis of new cases and the positive effect of the performed measurements.
ACKNOWLEDGEMENTS
The authors would like to gratefully acknowledge the deputy for research and technology of Arak University of Medical Sciences to provide the background to perform this study.

