All published articles of this journal are available on ScienceDirect.

Health Services Utilisation before and during an Armed Conflict; Experiences from the Southwest Region of Cameroon
Abstract
Introduction:
Armed conflicts are a threat to the health of populations in affected areas. The threat can have several forms, such as direct injury or disruption of health service delivery and utilisation. There has been an armed conflict (Anglophone crisis) in the English-speaking regions of Cameroon since 2017. We assessed the utilisation of health services before and during the armed conflict s in the Southwest region of Cameroon.
Methods:
A retrospective study of surveillance data was carried out between 2016 and 2018. Regional data for selected routine immunisation, reproductive health, disease surveillance and HIV/AIDS indicators were retrieved. The data were presented as frequencies and described narratively.
Results:
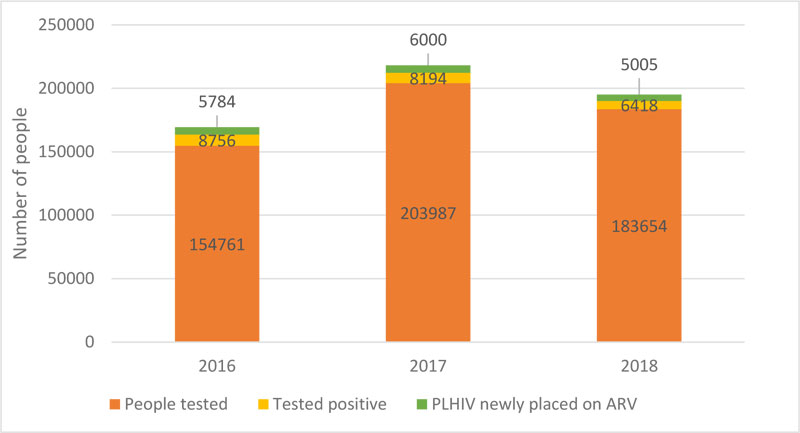
In general, there was a difference in the utilisation of health services before and during the armed conflict. Specifically, there was an improvement in health service utilisation indicators from 2016 to 2017, followed by a decline in 2018. The DPT3 vaccination coverage dropped from 90% in 2017 to 55% in 2018; deliveries attended by qualified personnel dropped from 46% in 2017 to 26% in 2018; the absolute number of people tested for HIV dropped from 20,3987 in 2017 to 18,3654 in 2018.
Conclusion:
The utilisation of health services by the population of the Southwest region declined during the armed conflict. This decline could have a significant impact on the population’s health and potentially affect the set global health targets such as improved vaccination coverage in all districts. Due to the armed conflict, there were challenges with regard to accessing health services. Local, national, regional and global authorities must work together to develop risk mitigating interventions in settings with armed conflicts to preserve the delivery and utilisation of health services.
1. BACKGROUND
Armed conflicts are known to disrupt the provision of health services to the public. In several settings, there are reports of negative effects of armed conflicts on the health services [1]. In any given setting, armed conflicts can directly cause injury to the population living in the affected areas or disrupt health service delivery. Furthermore, the populations affected by armed conflict suffer from diverse traumas which may be physical, psychological or both [2]. Disruptions of health service delivery during conflicts exacerbate the risk of preventable mortality and morbidity on the affected population.
2. INTRODUCTION
Globally, all continents have experienced armed conflicts at some period in the past. For example, in Asia, Syria, Afghanistan and Iraq are experiencing the most violent conflicts in recent times [3-6]. In Africa, the Democratic Republic of Congo, South Sudan and the Central African Republic are facing protracted conflicts; and in the Americas, Mexico is experiencing criminal violence [7]. It has been reported that armed conflicts can negate the efforts made in the fight against causes of mortality and morbidity, including eradication of poliomyelitis [8-10].
In Africa, endemic poverty and weak health systems amplify the negative effects of armed conflicts in the region. In countries experiencing protracted conflicts in the region, there are shortages of health staff, under resourced facilities and interrupted medical supplies [11-13]. Population displacement has the potential to negatively affect the public health system in settings that are not directly experiencing armed conflicts [14].
Cameroon has been experiencing armed conflicts in her Northern and Western regions. The Boko Haram insurgency in Nigeria began in 2010 and later spread to the Northern regions of Cameroon in 2013 [15]. Some studies have documented the implications of the insurgency on the public health sector in Nigeria [16, 17]; however, to the best of our knowledge, only one study has reported the impact on the health sector in Cameroon [14]. The Boko Haram insurgency reduced the availability and accessibility of health services in the affected areas [14]. At least eight out of the thirty health districts in the Far North region of Cameroon were severely affected [14]. Many health facilities closed as health workers and the communities fled for safety. The disruption of normal life and health services due to the insurgency created an enabling environment for the spread of communicable diseases. The influx of refugees from Nigeria into Cameroon also put a strain on the weakened health services in the area, rendering containment of any outbreak a difficult task [14, 18-20].
In 2016, Cameroon faced another crisis in the English-speaking Northwest (NW) and Southwest (SW) regions. What began as a peaceful protest of lawyers and teachers over perceived marginalization termed the ‘Anglophone Crisis’ turned into an armed conflict by the end of 2017 [21]. The armed conflict is characterised by burning of villages, destruction of property, kidnappings, extra-judiciary killings and population displacements according to eye witness reports. The armed conflict has since contributed to at least 246 000 internally displaced persons, with an additional 26 000 people registered as refugees in neighbouring Nigeria [22]. The armed conflict has had an impact on the economic development of these two regions. Small businesses have been forced to shut down due to the reduced number of business days caused by ghost towns imposed by the activists. Moreover, demand for services has been reduced as the population has fled the area. Major businesses in the agricultural sector such as the Cameroon Development Corporation and Pamol Plantation have also witnessed a drop in revenue due to low production resulting from attacks on their workers, among other reasons. The political scene has not been left unscathed. An increase in the intensity of fighting has been witnessed during national holidays and election season. Political figures have been targeted and their properties are destroyed.
The SW region is the most affected by the armed conflict with 15 of its 18 health districts being severely affected [23]. Since the beginning of the armed conflict in late 2017, health personnel and health facilities in the SW have been purposefully targeted by the warring parties. In times of war, health workers have the duty to provide health services to the population regardless of their political affiliations. However, in the SW, health workers in high-risk zones are caught between the military and non-military groups who exert pressure on them not to treat the opposing party. Failure to comply to the demands of either party has led to the harassment of health workers. A similar situation was reported by Nepalese health workers during the People’s War [11]. The respect of medical neutrality remains a challenge during armed conflicts [12]. By 2018, there were over 70 attacks on health personnel and infrastructure according to the SW Regional Delegation of Health (RDPH). Similarly, the supply of medicines and commodities from the regional warehouse to the districts is hampered by theft and destruction linked to armed groups. Supervisors are not willing to go into conflict zones for fear of being attacked by either warring party or being caught in crossfire. Thus, the quality of health services provided in the few facilities still operating cannot be ascertained. All these factors have contributed to the demotivation of many health workers in the region.
In many African countries, data on the effects of violence on the public health system is limited. A PubMed search for articles reporting the effect on conflicts on the health system in African countries produced 721 articles (Appendix A). The PubMed search utilized the following keywords: war, conflict, insurgency, health sector, health system. A majority of the articles focused on individual health programmes primarily mental health followed by child and maternal health. Only 2% of the search output focused on the effect of armed conflicts on the health system with the main theme being post-conflict health system strengthening.
Given the paucity of data on the topic, we, therefore, documented the effects of an armed conflict on the utilisation of health services in the SW region of Cameroon. Specifically, we aimed to compare community uptake of health services before and during the armed conflicts. We also aimed to describe the challenges faced with the delivery of health services in a region that is experiencing armed conflicts. We selected some indicators for use in the comparison of the uptake of health services. The indicators selected represent two key primary health care programmes: immunisation and reproductive health. Immunisation and reproductive health services are critical to achieve the targets of the Sustainable Development Goal 3 (SDG3). The SDG3 is to “Ensure healthy lives and promote wellbeing for all at all ages”. In addition, disease surveillance indicators for malaria and HIV were also included. Malaria and HIV are two infectious diseases of high public health priority in the African region.
We used a retrospective study design to address our objectives. Our findings raise awareness on the risk of armed conflicts on the delivery and utilisation of health services in affected communities, and provide more evidence for the development of policies that can mitigate this risk pre and post-conflict in similar African settings.
3. METHODS
3.1. Study Setting
The SW region is one of the ten regions of Cameroon with a total population of 1,817,667 inhabitants according to estimates provided by the Ministry of Health (MOH) in 2018. The region is one of the two English-speaking regions of the country. Before the armed conflict, most inhabitants were involved in farming and fishing as the major source of income.
The SW region is made up of 18 health districts (HD) with 116 health areas. Health services in the region are delivered by a total of 308 health facilities (2 regional hospitals, 12 district hospitals, 17 sub-divisional hospitals, 167 integrated health centres and 110 private health facilities). Integrated health centres are the lowest category of health facilities in Cameroon. Health activities in the region are coordinated by the RDPH.
3.2. Study Design and Data Source
A retrospective analysis of routine surveillance data was carried out from 2016 to 2018. Data was sourced from regional health records for 2016, 2017 and 2018. In health facilities, data collectors extract weekly and monthly data from both in and out patient consultation registers for disease surveillance indicators, EPI registers for routine immunisation indicators, Antenatal care (ANC) and maternity registers for reproductive health indicators and the Day Hospital registers for HIV/AIDS indictors. The extracted data is then submitted as weekly and monthly paper-based reports to their respective district health services where the data is compiled before submission to the RDPH office. Parallel to this mode of data transmission, reports are also transmitted via the digital health information system (DHIS2) from health facilities to the regional office. At the RDPH this data is analysed, transmitted to the central level and stored in the regional database. For this study, data for key health outcomes from January to December 2018 were retrieved from the regional database and compared to those of a similar period in 2016 and 2017.
3.3. Health Service Indicators
The health service delivery indicators were purposively selected from the disease prevention and case management components of the health sector as outlined in the Cameroonian Health Sector Strategic Plan (HSSP) [24]. Two out of the five components that constitute the health sector portray direct use of health services by the community i.e. disease prevention and case management.
Disease prevention indicators included indicators from routine immunisation and reproductive health (RH) while case management indicators included indicators from disease surveillance and HIV/AIDS being a priority disease.
Routine immunisation indicators were: BGG coverage; DTP3 coverage; and, DTP specific dropout rate (children who didn’t complete 3 doses of DTP). The RH indicators were: pregnant women seen at ANC1; pregnant women who received IPT3; HIV infected pregnant women on ART; and, deliveries attended by qualified staff. These health indicators were selected as they represent tracers used to evaluate the attainment of objective 3 of the HSSP disease prevention component. Objective 3 aims at “at least an 80% increase in the coverage of high impact preventive interventions for mothers, newborns and children in at least 80% of health districts by 2027”. These preventive interventions include ANC services, assisted deliveries, immunisation, counselling and testing for HIV and hepatitis for all pregnant women, among others.
Disease surveillance indicators: total consultations; suspected cases of malaria and typhoid which are the top reasons for consultation. For HIV/AIDS: the number of people tested; people tested positive; and, people newly placed on ART were selected as indicators to evaluate the attainment of specific objective 1 of the HSSP case management component aimed at providing care by 2027 for all communicable and non-communicable diseases as well as their complications according to standards in at least 80% of health facilities.
3.4. Data Synthesis and Analysis
Data were analysed using Stata 14.0. Service delivery indicators for routine immunisation and RH were presented as frequencies calculated using the estimated yearly regional target population count provided by the MOH as the denominator and the number of acts carried out as the numerator. Indicators for disease surveillance and HIV/AIDS were calculated based on the number of consultations for the year. Challenges faced were narratively reported.
4. RESULTS
4.1. Trends in Health Service Indicators
Our objective was to evaluate the uptake of health services before and during the armed conflicts. Indicators used for this objective were derived from the Cameroonian Health Sector Strategic Plan. The plan has components that assess service delivery (disease prevention and case management components). So, indicators from these components (immunisation, reproductive health, malaria, and HIV) recognised nationally were used.
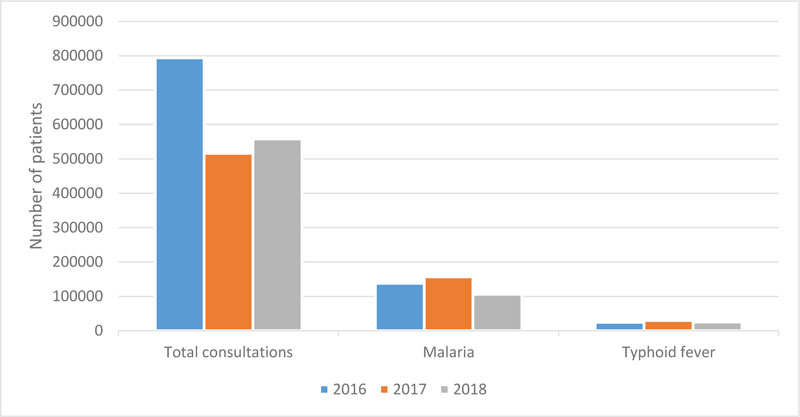
Table 1 represents key disease prevention indicators for January to December 2016, 2017 and 2018. Generally, there was an improvement in routine immunisation and RH indicators from 2016 to 2017 which corresponds to a period when there was no armed conflict. In 2018 when the armed conflict had started, a drop was observed in the indicators when compared to 2017. Similarly, there was an increase in the number of patients tested and treated for HIV in 2017 compared to 2016, but a drop was observed when compared to 2018 (Fig. 1). However, for disease surveillance there was a drop in the number of total consultations between 2016 and the proceeding years while malaria consultations increased between 2016 and 2017 but dropped thereafter (Fig. 2). Considering the annual population growth estimates, all indicators for 2018 in the region were expected to be similar if not better than those for 2017.
| Indicator | Pre conflict | Per conflict | ||
|---|---|---|---|---|
| 2016 | 2017 | 2018 | ||
| Routine Immunisation | BCG coverage (%) | 67 | 87 | 54 |
| DTP3 coverage (%) | 89 | 90 | 55 | |
| DTP specific dropout rate (%) | 5 | 7 | 6 | |
| Reproductive Health | Pregnant women seen at ANC 1 (%) | 57.5 | 56.3 | 38.9 |
| HIV infected pregnant women on ART (%) | 84.6 | 79.2 | 69.2 | |
| Pregnant women who received IPT3 (%) | 38.1 | 39.9 | 45.6 | |
| Deliveries attended by qualified personnel (%) | 52.9 | 46.4 | 26.4 | |
4.2. Challenges Faced
The provision and uptake of health services during the armed conflict faced several challenges including a) reduced accessibility of the community to health facilities due to population displacement; b) inability of drugs and supplies to get to health facilities as a result of attacks on the highway, blocked roads or active fighting; c) abandoned health facilities due to attacks on health personnel or infrastructure; d) breakdown in communication networks hampering remote supervision and data collection in facilities operating in high risk zones; and e) theft or expiration of drugs due to low consumption resulting in huge financial loss.
5. DISCUSSION
The armed conflict negatively impacted on the uptake of health services in the SW region as evidenced by the downward trends of some key health service indicators in 2018 compared to 2017. Vaccination coverage for DTP3 dropped from 90% in 2017 to 55% in 2018; assisted deliveries dropped from 46.4% in 2017 to 26.4% in 2018; the number of people living with HIV/AIDS (PLHIV) lost to follow up increased from 1613 in 2017 to 2282 in 2018. Access to healthcare was hampered by the massive displacement of the population and the inability of medical supplies to penetrate the high-risk zones. Countries faced with armed conflict have reported the re-emergence of infectious diseases, exacerbation of health conditions, unhealthy coping mechanisms, increased mortality and weakening of the health system [25-28].
Limited access to health services, especially preventive and curative interventions, poor water and sanitation conditions as well as constant movements of the population make areas experiencing armed conflicts to be susceptible to re-emergence of infectious diseases [29, 30]. The observed decline in the number of consultations for malaria and typhoid fever attests to a reduction in the uptake of health services by the community members during the armed conflict period.
The reduced uptake of health services during armed conflicts will likely result in disease outbreaks. In 2018, a Monkeypox outbreak was declared in the Akwaya HD of the SW region. Investigations revealed that at the time of detection, the outbreak was dying out. Early outbreak detection was hampered by limited access to health services as a result of insecurity prevailing in that district.
Other public health challenges reported in the region include poor sanitation, inadequate collection and disposal of household waste in urban towns. Consequently, heaps of dirt are common on most streets and this puts the community at risk of hygiene related communicable diseases. Facing the breakdown of surveillance and public health systems during the armed conflict, there is an urgent need for health promotion strengthening in the region.
During armed conflicts, children are the most vulnerable group in the society and bear the brunt of poor health outcomes and malnutrition [31]. Affected children become susceptible to infectious diseases and this is further aggravated by the absence of preventive health interventions like vaccination. The Expanded Programme on Immunisation (EPI) activities in the SW region were hampered by the difficulty to transport vaccines from the regional warehouse to the districts, theft of solar panels and gas bottles powering fridges, poor data reporting and the fleeing of health personnel from some health areas as a result of insecurity. Consequently, the region may witness a setback in the advances made in polio eradication and measles elimination as a result of low vaccination coverage and breakdown of surveillance systems. Polio endemicity in Pakistan, Afghanistan and Nigeria is partly attributed to the protracted armed conflict in these countries [32, 33].
Armed conflicts reduce women’s accessibility to family planning services as well as maternal and neonatal care while exposing them to Gender Based Violence (GBV) and risky sexual behaviours [34]. Reproductive health is considered as a human right for women [35]. Global bodies have recognised this right, as evidenced in its inclusion to the Sustainable Development Goal 3 which targets the reduction of maternal and infant mortality and the universal access to sexual and reproductive health care services by 2030 [36]. The drop in RH indicators in the SW region indicates that many displaced pregnant women give birth under precarious conditions which increases the risk of maternal and neonatal deaths as well as neonatal tetanus, a Vaccine Preventable Disease (VPD) that is nearing elimination in Africa. High maternal and infant mortality rates have been reported in the Democratic Republic of Congo and Syria [37, 38], both countries are experiencing armed conflicts. Countries with armed conflicts have also reported an increase in GBV especially rape [39-41]. We can only speculate that the SW region faces a similar situation. The absence of functional health facilities with adequate technical staff and equipment to manage complications arising from GBV creates a fragile situation. In such situations, strategies to identify GBV survivors who generally shy away from health services due to shame need to be adopted. Also, adequate healthcare and emotional support need to be provided to the GBV survivors. We observed an increase in the proportion of women who received IPT3 in 2018 compared to the previous years. This is unusual considering the fact that there was a drop in the proportion of women attending their first ANC which corresponds to a pregnant woman’s first contact with the health system and deliveries assisted by qualified personnel which marks the end of her follow-up for pregnancy. We speculate that this increase was due to poor data collection.
During conflicts, deaths due to chronic diseases account for a large proportion of mortality rates. Limited access to health facilities for routine check-ups, shortage of medications and the inability to maintain a healthy lifestyle all contribute to the rapid progression of the disease [42]. Moreover, limited access to health facilities and the absence of specialised care in facilities still functioning render the management of complications resulting from interruption of medication difficult. Interruption or non-management of chronic infectious diseases like HIV/AIDS in the region not only puts patients at risk but their entourage as well [43]. Furthermore, the adoption of risky sexual behaviours as a coping mechanism by some people in times of crisis promotes the spread of HIV/AIDS [43]. A breakdown in the provision of services makes the achievement of the 90-90-90 goal for HIV by 2020 difficult [44]. During a crisis, the focus is usually placed on providing basic health care which is usually short-term leaving patients needing chronic care at a loss. Though often neglected, mental health disorders due to exposure to traumatic events and displacements during conflicts have been reported in several settings [45-47]. Health facilities in the region already report patients presenting with stress disorders. Unfortunately, access to mental healthcare is low in the country due to the absence of qualified staff and we were unable to evaluate this health indicator in the study. Priority should be placed on extending mental healthcare to communities in armed conflict settings as recommended by global bodies [48].
Attacks of health personnel and infrastructure in the SW region by both warring parties has created some level of mistrust between the three parties. The population views the health staff and facilities still operating as spies for the government and traps for wounded combatants. On the other hand, the health staff cannot rely on the military to ensure their protection for fear of being assaulted by the said military for treating the opposing party. This mistrust reduces the health seeking behaviour of the population. Moreover, it creates a negative environment for activities such as routine mass campaigns which require collaboration between the communities and the health sector. The health sector would have to engage in frank dialogue with community leaders; deploy health workers to serve in communities they originate from; ensure the protection combatants who seek care; and remain neutral at all times in order to regain the trust of the population. In the present context where the government is making no concessions, these trust building efforts remain a challenge.
Efforts made by the government and humanitarian agencies in the SW region to mitigate the effects of the conflict on the health sector have been fruitful to an extent. Within the region, communities are receptive to the new role CHW play as frontline caregivers and collaborate with them to receive basic health services. The collection of vaccines from the regional store by health facilities as opposed to the district has enabled the vaccination of internally displaced children at agreed locations. Unfortunately, these efforts are only concentrated in a few districts as the level of insecurity remains high in most districts in the region. Out of the region, patients on chronic medication especially ARVs have been able to collect their ARVs at other dispensing facilities due to the newly implemented continuous care identity card. Despite these achievements, more humanitarian aid and healthcare system strengthening is required to address the needs of communities in the region. International health organisations should rethink their policy of putting travel embargos or withdrawing consultants from conflict affected areas. This restriction creates a sense of abandonment among supported health staff. In addition, it creates a gap in health system strengthening at a period when it is most needed. On the other hand, the national government should grant more access to humanitarian organisations which are willing to provide assistance in high risk zones.
This study had several limitations. Firstly, the data presented represent only activities that were successfully documented and reported to the regional office. Health services rendered and documented at facilities but not reported due to the armed conflicts were not accounted for. Secondly, the estimated target population for 2018 provided by the MOH did not take into account population displacement. Thirdly, the quality of the reported data could not be ascertained. Fourth, we were limited to conduct statistical analysis due to the nature of the data available to us. Fifth, apart from before and during the armed conflicts comparisons, we did not have any other group to compare with.
CONCLUSION
During the armed conflict in the SW region, utilisation of health services declined in comparison to before the conflict. Some operational changes by authorities partly mitigated the decline in utilisation of health services during the armed conflict. Notwithstanding, a lot still has to be done; challenges such as attacks on health workers and infrastructure, financial loss due to the expiration and theft of drugs from facilities among others must be addressed by all stakeholders. National, regional and global authorities should work together to develop risk mitigating interventions in settings with armed conflicts to preserve delivery of health services. Failure to do so could result in the derailment of global efforts to eliminate VPDs as well as reduce maternal and neonatal mortality.
LIST OF ABBREVIATIONS
| ANC | = Antenatal Care |
| ART | = Antiretroviral Therapy |
| BCG | = Bacille Calmet Guerin |
| CHW | = Community Health Workers |
| DTP | = Diphtheria-Tetanus-Pertussis |
| EPI | = Expanded Programme on Immunisation |
| GBV | = Gender Based Violence |
| HD | = Health District |
| HIV/AIDS | = Human Immunodeficiency Virus/ Acquired Immunodeficiency Syndrome |
| IDP | = Internally Displaced Population |
| IPT | = Intermittent Preventive Treatment |
| NW | = Northwest |
| PLHIV | = People Living with HIV |
| RDPH | = Regional Delegation of Public Health |
| RH | = Reproductive Health |
| SW | = Southwest |
AUTHOR’S CONTRIBUTIONS
HE conceived and designed the study. HE and CJ acquired data and wrote the first draft with supervision from BK. All authors reviewed the various drafts and approved the final manuscript.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study utilized data that is routinely collected by the health authorities for programme strengthening. Therefore, ethics approval was not required for this study. However, approval to access the data was obtained from the Regional Delegation of Public Health.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
Not applicable.
AVAILABILITY OF DATA AND MATERIALS
The datasets used and/or analysed during the current study are available from the corresponding author [H.C.E] on reasonable request.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Dr. Mbome Njie V. Southwest Regional Delegation of Health, Cameroon
Ms. Leoga Mathilda K. Southwest Regional Technical Group-Expanded Programme on Immunisation, Cameroon
Mr. Sielenou Franklin. Southwest Regional Technical Group-Malaria, Southwest Regional Delegation of Health, Cameroon
Mrs. Nankia D. Sandrine. Southwest Regional Technical Group-HIV, Cameroon
Mrs. Suka Caroline. Reproductive Health unit, Southwest Regional Delegation of Health, Cameroon
Mr. Keka Frederic. Reproductive health unit, Southwest Regional Delegation of Health, Cameroon
Mr. Ntsimi Brice. Health information unit, Southwest Regional Delegation of Health, Cameroon

