All published articles of this journal are available on ScienceDirect.

Perceptions of Mothers and Community Members Regarding Breastfeeding in Public Spaces in Alexandra, Gauteng Province, South Africa
Abstract
Background:
Mothers experience significant barriers to breastfeed in public spaces, which could result in a detrimental impact on the World Health Organization’s recommendation of exclusive breastfeeding. Failure to support and accept breastfeeding in public spaces could lead to mixed feeding or even abandonment of breastfeeding.
Objective:
The current study aimed to identify the knowledge of breastfeeding benefits and perceptions about it among mothers and community members in Alexandra, Gauteng Province, South Africa.
Methods:
A quantitative, non-experimental descriptive study was deployed using two structured questionnaires, which were distributed among mothers (n=96) and community members (n=96). All 192 questionnaires were completed and returned, although two questionnaires of mothers could not be used due to incompleteness. An excel spread sheet and Statistical Package for Social Sciences version 25 was used to analyze the data.
Results:
The findings of the current study revealed a positive correlation between the knowledge level about breastfeeding benefits [infants (r=0.45, p≤0.000) and mothers (r=0.29, p≤0.000)] and perceptions in public spaces. Community members and mothers who were knowledgeable regarding breastfeeding benefits exhibited supportive attitudes towards breastfeeding in public spaces.
Conclusion:
Altogether, the majority of mothers (69%) were comfortable to breastfeed in public spaces, and community members (84%) were supportive. Limited knowledge of breastfeeding benefits was associated with unsupportive attitudes towards breastfeeding in public spaces. Health messages that target these factors are essential to encourage support and acceptance of breastfeeding in public spaces. This could be executed through public education via posters in public spaces and during community health outreaches.
1. INTRODUCTION AND BACKGROUND
Exclusive breastfeeding (EBF) for the first six months of life is important for both infants and mothers as well as community members. However, it is difficult to practice if mothers cannot breastfeed whenever and wherever as needed by the infants. Failure to support and accept breastfeeding in public spaces could lead to mixed feeding or even abandonment of breastfeeding. EBF has been defined as breastfeeding of breastmilk for the initial six months of life without giving any supplementary feeds or water, but with oral rehydration solution, drops, and syrup (vitamins, minerals, and medicine) when required [1, 2].
EBF holds health benefits for infants, mothers, and community members. Infant benefits include decreased weight loss, allergies, respiratory tract infections and diarrhea, increased glucose serum levels, and periods of breastfeeding [3, 4]. Maternal health benefits include prevention of pathological breast engorgement, a decreased incidence of sore nipples, and promotion of bonding between the infant and mother [5, 6]. Community benefits include producing healthy communities, reduced child mortality, reduced pollution, and savings on governmental healthcare costs by decreasing hospital admission rates [7, 8].
Globally, only one out of three infants is exclusively breastfed for the first six months [9]. In the United States of America (USA) in 2016, 83.3% of mothers initiated breastfeeding, but only 25.4% breastfed exclusively for three months [10]. The United Kingdom also remains below target, with 23.0% of mothers reporting EBF at six weeks and 1% at six months [11]. In African countries, breastfeeding rates vary widely. The percentage of infants who were exclusively breastfed was 44% in Swaziland in 2010, 34% in the Central African Republic in 2010, 43% in Mozambique in 2011, 37% in the Democratic Republic of the Congo in 2011, and 31% in Zimbabwe in 2011, while Nigeria had the lowest rate of 17% in 2011 [12]. In South Africa, EBF is uncommon for the entire first six months [13, 14]. Although the country has the highest breastfeeding initiation rate of 75-79% compared to the other African countries, EBF is not maintained [15]. The South African statistics indicated that the percentage of infants who were exclusively breastfed decreased with age from 44% for 0-1 month to 24% for 4-5 months, respectively [16].
In order to exclusively breastfeed, mothers should be able to do it anytime and everywhere, however, mothers encounter challenges when breastfeeding in public spaces [17]. Lack of support from the community members was the most cited challenge that mothers experience [18-20]. A study conducted in Scotland showed that mothers do not want to breastfeed in public spaces because they fear adverse reactions from the community members [21]. Studies showed that community members dishonor breastfeeding in public spaces because they view breasts as sexual organs which should not be displayed in public spaces [20, 22]. Culture was among other factors that affect breastfeeding in public spaces. In societies where breastfeeding is culturally accepted, breastfeeding in public spaces is not an issue, hence is being promoted [23]. Some cultures, such as Kenyans, considered breastfeeding in public spaces as a negative practice that predisposes an infant to evil spirits, therefore, it is seen as immoral practice [24].
Socio-cultural context influences and guides the mothers’ decision to breastfeed in public spaces [25, 26]. In South Africa, it is prevalent for mothers to breastfeed in public spaces although public encounter may create a state of negative surprise for bystanders, which mostly result in emotional discomfort for the mothers [14, 27]. Media in South Africa revealed that mothers are often subjected to verbal and physical abuse, which discourages them from breastfeeding in public spaces, thus disadvantaging infants and mothers from obtaining its’ health benefits [28, 29]. However, in South Africa, breastfeeding in public spaces is slowly becoming acceptable. One family restaurant group initiated a new breastfeeding policy that allows mothers to breastfeed freely in their restaurants [30]. During the world breastfeeding week in 2019, a panel of registered dieticians gathered to address the burning question of how mothers can be empowered to breastfeed in public spaces [31].
There is a need to encourage and promote the practice of EBF, especially in public spaces. The authors believe that the interventions to encourage social acceptance and support of breastfeeding in public spaces require an understanding of its’ benefits, knowledge, and perceptions in public places. The rationale of this study was to identify the various views, ideas, thoughts, and understanding of mothers and community members in the Gauteng province in South Africa, regarding breastfeeding in public spaces, in order to encourage support and acceptance of breastfeeding in public spaces hence promoting the wellbeing and health of infants and mothers as well as the communities.
2. MATERIALS AND METHODS
A non-experimental, descriptive survey was conducted in five Alexandra Township clinics, Gauteng Province in South Africa [32, 33]. Alexandra Township was established in 1912 and is located 13km north-east of Johannesburg [34]. It covers over 800 ha, with a population of approximately 350,000 [35].
2.1. Population
The study constituted two populations, mothers and community members who attended healthcare service in participating Alexandra clinics. An estimated total of 8400 patients (approximately 4500 community members and 3900 mothers) attend these primary health clinics per month.
2.2. Inclusion Criteria
The study constituted two samples. Therefore, respondents who met the characteristics as outlined in Table 1 were included in this study [36].
| Inclusion criteria for mothers | Justifications |
| 1. Mothers who BF infants aged 0-6 months. 2. Mothers aged 18 years and older and mothers aged younger than 18 years whose legal guardians were able to give consent. 3. Mothers who brought their children to the wellness clinics. |
1. This group is still expected to EBF their infants even in public spaces. 2. Persons older than 18 years are legally fit to give consent in SA. Mothers younger than 18 years are regarded as minors. As a result, in addition to their consent, their parents/legal guardians also needed to give consent for their participation in the study. 3. To avoid additional stress to participating mothers by not requiring additional travels/clinic attendances. |
| Inclusion criteria for community members | Justifications |
| 1. Individuals aged 18 years and older. 2. Community members who were not critically ill. 3. Community members residing in the same geographical area as the sampled nursing mothers. |
1. This group is legally fit to give consent. 2. To avoid additional stress to them. 3. Shares common public spaces with mothers. |
2.3. Sample, Sample Size, and Sampling Technique
The two samples were mothers breastfeeding infants aged 0-6 months and community members who attended healthcare services at any of the five participating clinics. A statistician was consulted to calculate the sample size required for this study, as follows: Confidence level of 95%, which amounted to a Z-score of 1,645, margin error of 10% (0.1), standard deviation of 0.5: n= Z2.S. (1-5)/e2 n= 1.962.0.5. (1-5)/0.12 n= 96.
Therefore, 96 respondents were the desired sample size for each population in this study [37, 38]. Four participating clinics had 19 mothers and 19 community members each, and the fifth clinic had 20 respondents per population to cover the exact desired sample size. Recruitment from clinic A, B, C, D, and E was done on consecutive weekdays.
Clinics had numerous potential respondents who were willing to participate; therefore, random sampling was used to create an equal and independent opportunity for all respondents to participate [39]. Paper squares with an equal number of YES and NO options on it were folded, placed in a bowl, and mixed well. Each potential respondent got the opportunity to select a paper and when a YES was drawn, he/she was included in the study and was excluded in case of NO. After each respondent drew, the paper square was replaced and mixed well again before the next respondent got an opportunity to draw. This process was repeated until the desired sample per clinic was reached.
2.4. Data Collection Instrument
Two separate questionnaires were used for mothers and community members, and both consisted of three sections: A: Socio-demographic characteristics; B: Knowledge level of breastfeeding benefits; and C: Perceptions of breastfeeding in public spaces. The contents of the questionnaire were the same, except section C that addressed the specific perceptions of breastfeeding in public spaces for each population.
The public perception survey on breastfeeding and public opinion about breastfeeding questionnaires were previously used in similar studies conducted in Hong Kong and the USA, respectively [32, 33]. The original questionnaire was adapted with the consultation of a statistician to check and verify the suitability (content, wording, language level, the order of Likert-items) to the South African context, therefore, enhancing the validity and reliability of the tool.
The original questionnaire was available in English, but was translated into three local languages (Setswana, isiZulu, and Tsonga), frequently used in the study area. The translation was done into the respective native languages by three bilingual native speakers. All questionnaires were checked for correctness by another three different bilingual native speakers of the respective languages.
2.5. Questionnaire Validity and Reliability
Face validity was confirmed by academic peers and the questionnaires appeared to be clear and relevant [40]. Content validity was ensured by adapting questionnaires from existing ones and by using subject experts to check the relevance and adequacy of the questionnaire [41]. Based on the feedback of the experts, the questionnaires were finalized.
Cronbach’s alpha coefficient was calculated to estimate the questionnaires’ reliability. Excellent reliability is indicated by a coefficient value greater than 0.8; however, a value above 0.6 is acceptable [40]. For the instrument from the USA, the Cronbach’s alpha coefficient was 0.89 [42]. For the current study, Cronbach's alpha was applied separately to the Likert scale sections [43]. Section B (knowledge level regarding benefits of breastfeeding for infants α=0.84, and for mothers α=0.74) and Section C (perceptions of the acceptability of breastfeeding in public spaces α=0.65, and perceptions of support α=0.81). Therefore, Cronbach’s alpha coefficients were acceptable, and questionnaires were reliable. Furthermore, reliability was ensured by deploying a pre-test in “Clinic X” representing 10% (n=9) of the main study sample size. The pilot study sample was not included in the main study to minimize the potential bias that may arise due to multiple administrations of the same questionnaire. The questionnaire was administered on day one and re-administered after a seven-day interval to ensure that executed modifications and adjustments were feasible, and respondents were interpreting questionnaires correctly.
2.6. Data Collection Procedure
Health Research Ethics Committee (HREC) of the North-West University (NWU) granted ethical clearance (Ref: NWU-00116-18-A1) to conduct the study. Provincial consent (Ref: GP 201810 040) was obtained from the Gauteng Department of Health via the National Health Research Database website. The managers from the participating clinics signed goodwill permission for the research to proceed at their facilities. All 192 respondents signed voluntary informed consent (IC). Data collection took place during the last two weeks in February 2019. Clinic A, B, C, D, and E in Alexandra were visited on consecutive weekdays. Respondents completed the questionnaires in a private room where refreshments were offered. The time to complete the questionnaire ranged from 15 to 25 minutes. No respondent’s name was written on the questionnaire to ensure anonymity. The researcher and the research assistants were available to clarify any questions or inquiries that respondents had as they were completing questionnaires. Each respondent sealed the completed questionnaire in an envelope, which was then placed into a collection box. The envelopes had no names or marks that could be used to identify respondents. The researcher collected the boxes of completed questionnaires from participating clinics on a weekly schedule for data analysis.
2.7. Data Analysis
Before the data was analyzed, all questionnaires were reviewed and two incomplete questionnaires (from mothers) were discarded to ensure the accuracy of the data. Data from the questionnaires were transferred to an Excel sheet in code format by the researcher. The statistician assisted in analyzing the data using the Statistical Package for Social Sciences version 25 [44]. Descriptive statistics were applied to summarize data using frequency distributions and percentages. Inferential statistics (Pearson’s correlation efficient, factor analysis, t-tests, and ANOVAs were used to extract the relationship between variables [45].
3. PRESENTATION OF RESULTS
Questionnaires were distributed to the sampled 96 breastfeeding mothers and 96 community members to be completed and returned. The response rate of mothers was 98% (n=94) as two questionnaires were discarded and for community members was 100% (n=96). Results are presented in the same order as in the questionnaire together with the relationship between variables.
3.1. Section A: Socio-Demographic Characteristics
3.1.1. Mothers
As illustrated in Table 2, most of the mothers were single (60.6%) and attained secondary school education. The majority (61.7%) of maternal age ranged between 26-35 years. Unemployed mothers (58.5%) were most common in the study sample. The highest percentage of mothers (72.3%) had one or two children.
3.1.2. Community Members
The largest portion of the community members (67.7%) were single. Sixty-three-point five percent (63.5%) participants obtained a secondary school education, and 49.0% had one or two children. Less than half of the community members (38.5%) were permanently employed. The age of 29.2% of the community members exceeded 45 years (Table 2).
3.2. Section B: Knowledge Level Of Breastfeeding Benefits
3.2.1. Mothers
Most mothers (67.0%) strongly agreed that breast milk provides all the nutrients required by infants, followed by 60.6% who also strongly agreed that breastfeeding protects infants against infections, with 54.3% who strongly agreed that breastfeeding infants are healthier than formula-fed infants. Forty-four-point seven percent (44.7%) of mothers strongly agreed that breastfeeding does not create pollution, while 40.4% also strongly agreed that breastfeeding produces a healthy community and 41.5% agreed that breastfeeding protects mothers against breast and ovarian cancer. The knowledge of some breastfeeding benefits of the mothers was lower, such as that breastfeeding tones the mother’s body (38.3%), helps the government to save healthcare costs by reducing hospital admissions (36.2%), reduces absenteeism from work (29.8%), and assists in child spacing by preventing pregnancies (26.6%) (Table 3).
| - | Mothers (n=94) |
Community members (n=96) |
||
| Variables | Frequency | Percentage | Frequency | Percentage |
| Marital status | ||||
| Single | 57 | 60.6 | 65 | 67.7 |
| Married | 37 | 39.4 | 27 | 28.1 |
| Divorced | 0 | 0 | 1 | 1.0 |
| Widow(er) | 0 | 0 | 3 | 3.1 |
| Educational level | ||||
| None | 4 | 4.3 | 6 | 6.3 |
| Primary | 4 | 4.3 | 7 | 7.3 |
| Secondary | 57 | 60.6 | 61 | 63.5 |
| Tertiary | 29 | 30.9 | 22 | 22.9 |
| Number of children | ||||
| None | 0 | 0 | 12 | 12.5 |
| 1-2 | 68 | 72.3 | 47 | 49.0 |
| 3-4 | 25 | 26.6 | 30 | 31.3 |
| Above 4 | 1 | 1.1 | 7 | 7.3 |
| Age (in years) | ||||
| 18-25 | 26 | 27.7 | 15 | 15.6 |
| 26-35 | 58 | 61.7 | 27 | 28.1 |
| 36-45 | 8 | 8.5 | 26 | 27.1 |
| Above 45 | 2 | 2.1 | 28 | 29.2 |
| Employment status | ||||
| Unemployed | 55 | 58.5 | 33 | 34.4 |
| Part-time employed | 4 | 4.3 | 20 | 20.8 |
| Self-employed | 4 | 4.3 | 6 | 6.3 |
| Full-time employed | 31 | 33.0 | 37 | 38.5 |
| Benefits of BF for infants, mothers and community | Mothers | Community members | ||||||
| SD | D | A | SA | SD | D | A | SA | |
| BF provides required nutrients to the infants. | 4 (4.3) |
0 (0) |
27 (28.7) |
63 (67) |
5 (5.2) |
2 (2.1) |
33 (34.4) |
56 (58.3) |
| BF protects infants against infections. | 5 (5.3) |
2 (2.1) |
30 (30.9) |
57 (60.6) |
6 (6.3) |
7 (7.3) |
38 (39.3) |
45 (46.9) |
| BF babies are healthier than formula-fed babies. | 4 (4.3) |
3 (3.2) |
36 (38.3) |
51 (54.3) |
3 (3.1) |
2 (2.1) |
33 (34.4) |
58 (60.4) |
| BF protects mothers against breast and ovarian cancer. | 9 (9.3) |
18 (19.1) |
39 (41.5) |
28 (29.8) |
7 (7.3) |
32 (33.3) |
30 (31.3) |
27 (28.1) |
| BF helps to tone the body of the mother. | 12 (12.8) |
31 (33) |
36 (38.3) |
15 (16) |
10 (10.4) |
33 (34.4) |
29 (30.2) |
24 (25) |
| BF prevents pregnancy and assists in child spacing. | 19 (20.2) |
32 (34) |
25 (26.6) |
18 (19.1) |
23 (24) |
29 (30.2) |
24 (25) |
20 (20.8) |
| BF helps government to save healthcare cost by reducing hospital admissions. | 14 (14.9) |
19 (20.2) |
34 (36.2) |
27 (28.7) |
10 (10.4) |
10 (10.4) |
34 (35.4) |
42 (43.8) |
| BF does not create pollution- there are no plastics, rubber nipples, and formula containers on the landfills. | 9 (9.6) |
13 (13.8) |
30 (31.9) |
42 (44.7) |
5 (5.2) |
9 (9.4) |
31 (32.3) |
51 (53.1) |
| BF produces healthy community- fewer sick babies and reduced mortality rate of children. | 7 (7.4) |
16 (17) |
33 (35.1) |
38 (40.4) |
8 (8.3) |
13 (13.5) |
33 (34.4) |
42 (43.8) |
| BF reduces absenteeism at work. Parents do not have to stay at home to look after their sick child. | 15 (16) |
30 (31.9) |
28 (29.8) |
21 (22.3) |
12 (12.5) |
24 (25) |
28 (29.2) |
32 (33.3) |
3.2.2. Community Members
As indicated in Table 3, 58.3% of the community members strongly agreed that breast milk provides all the nutrients required by the infants, 53.1% strongly agreed that breastfeeding does not create pollution, 60.4% strongly agreed that breastfeeding infants are healthier than formula-fed infants, and 46.9% strongly agreed that breastfeeding protects infants against infections. Of all the community members, 25% agreed that breastfeeding assists with child spacing by preventing pregnancy, 31.3% agreed that breastfeeding protects mothers against breast and ovarian cancer, 30.2% strongly agreed that breastfeeding helps to tone the mother’s body, and 33.3% strongly agreed that breastfeeding reduces absenteeism at work. Less than half of community members (43.8%) strongly agreed that breastfeeding helps the government to save healthcare costs by reducing hospital admissions and the same percentage (43.8%) also strongly agreed that breastfeeding produces healthy communities. There is no specific trend to favor the knowledge levels of either the mothers or the community members.
3.3. Section C: Perceptions Of Breastfeeding In Public Spaces
3.3.1. Mothers
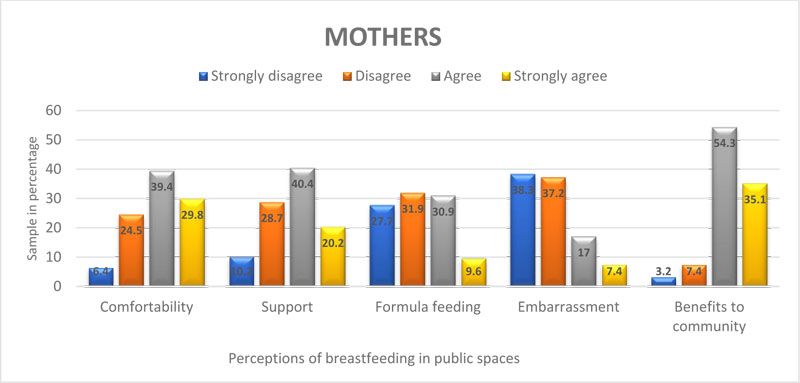
Fig. (1) shows that 69.2% of mothers felt comfortable (agreed and strongly agreed) when breastfeeding their infants in the presence of community members in public places (Comfortability), while 38.3% strongly disagreed that breastfeeding in public spaces is embarrassing (Embarrassment). Some mothers (31.9%) preferred formula feeding over breastfeeding in public spaces (Formula feeding). Less than half of the mothers (40.4%) agreed that community members supported them when they were breastfeeding their infants in public spaces (Support). Fifty-four-point three percent (54.3%) of mothers agreed that breastfeeding is beneficial to the community (Benefits to the community).
| - | Knowledge level | Perceptions | |
| Kaiser-Meyer-Olkin Measure of Sampling Adequacy. | 0.859 | 0.556 | |
| Bartlett’s Test of Sphericity | Approx. Chi-square | 721.222 | 221.239 |
| df | 45 | 10 | |
| Sig | 0.000 | 0.000 | |
3.3.2. Community Members
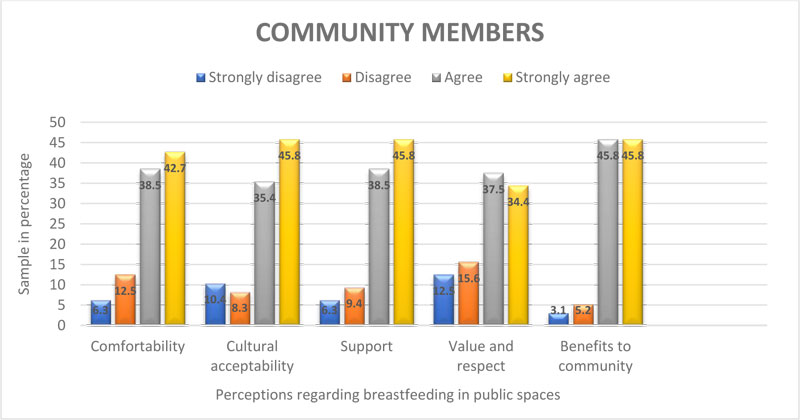
As illustrated in Fig. (2), 81.2% of community members were comfortable (agreed and strongly agreed) when mothers were breastfeeding their infants near them in public places (Comfortability) and 35.4% agreed that it was culturally acceptable for mothers to expose the breast and breastfeed infants in public spaces (Cultural acceptability). The majority of community members (84.1%) supported (agree and strongly agreed) mothers who were breastfeeding in public places (Support), and 34.4% strongly agreed that they respected and valued mothers who were breastfeeding public spaces (Value and respect). The highest percentage (91.6%) of the community members were aware (agreed and strongly agreed) that breastfeeding in public spaces is beneficial to the community (Benefits to the community).
3.4. Relationship Between Variables
The extraction of the relationship between the quantitative variables was carried out by employing Pearson’s correlation coefficient (r). Pearson’s correlation coefficient is a measure of the strength of the association between two variables [46]. Before the implementation of Pearson’s correlation coefficient, factor analysis (FA) was executed to reduce the number of Likert-item statements into a set of components to ease the explanation and interpretation of findings [47].
The FA was done following three steps. The first step of FA is to determine Kaiser-Meyer-Olkin. Kaiser-Meyer-Olkin was used to check if the Likert-scale data is suitable for FA [42]. High values, close to 1.0, indicate that FA could be applied to structure the data. If the value is less than 0.50, the results of the FA would probably be inapplicable. The Kaiser-Meyer-Olkin for the knowledge level of breastfeeding benefits measured 0.86, and 0.56 for perceptions. Therefore, FA was applicable, as the Kaiser-Meyer-Olkin was above 0.05 (Table 4).
The second step is to select the FA method. Principal component analysis was utilized as a method to execute FA. Principal component analysis was suitable as it aimed at reducing Likert-item statements to a small set that still contains most of the information in the large set [46]. As illustrated in Table 5, the statements related to knowledge level of breastfeeding benefits were reduced to two components (component 1: knowledge level of breastfeeding benefits for infants, and component 2: knowledge level of breastfeeding benefits for mothers). Furthermore, based on Table 5, the perceptions of mothers and community members regarding breastfeeding in public spaces were also reduced to two components (component 1: perceptions of the acceptability of breastfeeding in public spaces, and component 2: perceptions of support for breastfeeding in public spaces) [48].
| Pattern Matrix | |||
| Components | |||
| 1 | 2 | ||
| B. Knowledge level: Breastfeeding benefits | |||
| 1: Provides adequate nutrients | 8.908 | ||
| 2: Lessens infections to the infants | 0.833 | ||
| 3: Infants are healthier | 0.761 | ||
| 8: Less pollution | 0.643 | ||
| 9: Reduces child mortality rate | 0.589 | ||
| 4: Protects mothers against cancer (breasts & ovaries) | 0.358 | ||
| 6: Prevents pregnancy | 0.786 | ||
| 5: Tones mothers’ body | 0.731 | ||
| 10: Reduces absenteeism at work | 0.696 | ||
| 7: Minimizes health cost | 0.602 | ||
| C: Perceptions regarding BF in public spaces | |||
| Mothers | Community members | ||
| 1: Comfortable | 1: Comfortable | 0.834 | |
| 2: Culturally acceptable | 2: Support | 0.810 | |
| 5: Benefits to community | 5: Benefits to community | 0.636 | |
| 3: Support | 3. Prefers formula feeding in public spaces | -0.923 | |
| 4: Respect &value | 4 Embarrassing | -0.914 | |
| - | Components | Initial Eigen values | Extraction of sum squared loadings | Rotation sums of squared Loadingsa | ||||
| Total |
% of variance |
Cumulative % |
Total |
% of variance |
Cumulative % |
Total | ||
| Perceptions | 1 | 2.065 | 41.307 | 41.307 | 2.065 | 41.307 | 41.307 | 1.832 |
| 2 | 1.397 | 27.937 | 69.244 | 1.397 | 27.937 | 69.244 | 1.769 | |
| Knowledge level | 1 | 4.397 | 43.965 | 43.965 | 4.397 | 43.965 | 43.965 | 3.777 |
| 2 | 1.433 | 14.325 | 58.291 | 1.433 | 58.291 | 58.291 | 3.106 | |
The final step determined the Total Variance (TV) by calculating the percentage of the variables that is explained by the components. The aim of the TV is to indicate the strength of association among variables in the components [47]. Higher percentages of TV indicate strong levels of association, implying that better predictions could be made [47]. Looking at the TV in Table 6, the first two components of perceptions regarding breastfeeding in public spaces and of the knowledge level of breastfeeding benefits had 69.2 and 58.3 cumulative percentages, respectively. Both cumulative percentages exceeded 50%, indicating good strength of association of variables and consequently, good predictions.
After completion of the above three steps, Pearson’s correlation coefficient was deemed suitable to be implemented.
3.4.1. Relationship Between Variables: Mothers
The T-test, Pearson correlation coefficient, and one-way ANOVA test were used to determine the relationships between the mothers’ socio-demographic characteristics and their knowledge levels of breastfeeding benefits as well as their perceptions of breastfeeding in public spaces.
3.4.1.1. Marital Status
The t-test revealed a significant theoretical difference in the perceptions of the acceptability of breastfeeding in public spaces between single and married mothers [t (92) =2.70, p≤ 0.008, CI.95 0.095-0.620]. Thus, the average value of the perceptions of the acceptability of breastfeeding in public spaces of single mothers (M=3.08, SD=0.63) exceeded that of married mothers (M2.72, SD=0.61). The effect size value (d=0.57) also suggested a moderate significant practical difference. The findings indicate that single mothers support and accept breastfeeding in public spaces more than married mothers.
3.4.1.2. Ordered Variables (Educational Level, Parity, and Age)
The current study revealed a significant relationship between parity and knowledge level of breastfeeding benefits for infants (r=0.27, p≤0.007), indicating that as the maternal parity increases, the mothers’ knowledge levels of breastfeeding benefits for infants also increase.
No relationship was found between the educational level, parity, age, and perceptions concerning breastfeeding in public spaces. These findings suggested that increased maternal age, educational level, and parity did not affect the acceptance and support of breastfeeding in public spaces (all p-values ≥0.05) (Table 7).
3.4.1.3. Employment Status
As demonstrated by the one-way ANOVA test, there were no significant correlations between the employment status of mothers and knowledge levels of breastfeeding benefits nor with perceptions regarding breastfeeding in public spaces (all p-values ≥0.05).
3.4.1.4. Knowledge Level of Breastfeeding Versus Perceptions of Breastfeeding in Public Spaces
This study also revealed a significant positive relationship between the knowledge level of breastfeeding benefits for infants and the perceptions of breastfeeding in public spaces [perceptions of support (r=0.46, p≤0.000) and perceptions of acceptability (r=0.21, p≤0.042)]. This indicates that an increased knowledge level about breastfeeding benefits for infants was associated with mothers’ increased acceptance of breastfeeding in public spaces (Table 7).
3.4.2. Relationship Between Variables: Community Members
The Pearson correlation coefficient and t-test were used to extract relationships between community members socio-demographic characteristics and knowledge level of breastfeeding benefits as well as perceptions of breastfeeding in public spaces as follow:
3.4.2.1. Ordered Variables (Educational Level, Parity, and Age)
A significant relationship was found between age and knowledge level of breastfeeding benefits for infants (r=0.29, p≤0.003) and mothers (r=0.32, p≤0.001). This finding suggested that as community members age progressed, their knowledge levels of breastfeeding benefits also increased.
Another significant association was discovered between age and perceptions [support (r=0.29, p≤0.003) and acceptability (r=0.24, p≤0.016)] regarding breastfeeding in public spaces. This implies that as community members’ ages increase, the more they support and accept breastfeeding in public spaces.
No association was found between educational level, parity, and knowledge level of breastfeeding benefits nor perceptions of breastfeeding in public spaces (all p-values ≥0.05) (Table 7).
3.4.2.2. Employment Status
The one-way ANOVA test indicated that there were no significant correlations between the employment status of community members and their knowledge levels of breastfeeding benefits nor with their perceptions regarding breastfeeding in public spaces (all p-values ≥0.05).
| - | Educational level | Parity | Age |
Knowledge level of BF benefits for infants |
Knowledge level of BF benefits for mothers |
Acceptability of BIP |
Support of BIP |
||
| Mothers | Knowledge level of BF benefits for infants | CC | 0,148 | .275** | -,019 | 1,000 | .532** | -.210* | .464** |
| Sig. (2-tailed) | 0,156 | 0,007 | 0,853 | 0,000 | 0,042 | 0,000 | |||
| N | 94 | 94 | 94 | 94 | 94 | 94 | 94 | ||
| Community members | Knowledge level of BF benefits for infants | CC | 0,140 | 0,139 | .299** | 1,000 | .528** | .421** | .462** |
| Sig. (2-tailed) | 0,173 | 0,178 | 0,003 | 0,000 | 0,000 | 0,000 | |||
| N | 96 | 96 | 96 | 96 | 96 | 96 | 96 | ||
| Knowledge level of BF benefits for mothers | CC | -0,062 | 0,076 | .324** | .528** | 1,000 | 0,141 | .217* | |
| Sig. (2-tailed) | 0,552 | 0.460 | 0,001 | 0,000 | 0,170 | 0,034 | |||
| N | 96 | 96 | 96 | 96 | 96 | 96 | 96 | ||
| Acceptability of BIP | CC | -0,123 | 0,114 | .244* | .421** | 0,141 | 1,000 | .755** | |
| Sig. (2-tailed) | 0,234 | 0,268 | 0,016 | 0,000 | 0,170 | 0,000 | |||
| N | 96 | 96 | 96 | 96 | 96 | 96 | 96 | ||
| Support for BIP | CC | -0,156 | 0,091 | .297** | .462** | .217* | .755** | 1,000 | |
| Sig. (2-tailed) | 0,130 | 0,376 | 0,003 | 0,000 | 0,034 | 0,000 | |||
| N | 96 | 96 | 96 | 96 | 96 | 96 | 96 | ||
| - |
Educational level |
Parity | Age | Knowledge level of BF benefits or infants | Knowledge level of BF benefits for mothers | Acceptability of BIP | Support of BIP | |
| Knowledge level of BF benefits for infants | CC | .144* | .190** | .152* | 1,000 | .533** | 0,102 | .457** |
| Sig. (2-tailed) |
0,047 | 0,009 | 0,036 | 0,000 | 0,163 | 0,000 | ||
| N | 190 | 190 | 190 | 190 | 190 | 190 | 190 | |
| Knowledge level of BF benefits for mothers | CC | -0,085 | 0,090 | .208** | .533** | 1,000 | 0,140 | .297** |
| Sig. (2-tailed) |
0,242 | 0,217 | 0,004 | 0,000 | 0,053 | 0,000 | ||
| N | 190 | 190 | 190 | 190 | 190 | 190 | 190 | |
| Acceptability of BIP | CC | -0,102 | 0,031 | .299** | 0,102 | 0,140 | 1,000 | .219** |
| Sig. (2-tailed) |
0,162 | 0,676 | 0,000 | 0,163 | 0,053 | 0,002 | ||
| N | 190 | 190 | 190 | 190 | 190 | 190 | 190 | |
| Support of BIP | CC | -0,127 | 0,123 | .243** | .457** | .297** | .219** | 1,000 |
| Sig. (2-tailed) |
0,082 | 0,091 | 0,001 | 0,000 | 0,000 | 0,002 | ||
| N | 190 | 190 | 190 | 190 | 190 | 190 | 190 | |
3.4.2.3. Knowledge Level of Breastfeeding Versus Perceptions of Breastfeeding in Public Spaces
The researchers found a significant positive relationship between knowledge level of breastfeeding benefits [for infants (r=0.46, p≤0.000) and mothers (r=021, p≤0.034)] and perceptions of support of breastfeeding in public spaces. This finding implies that as the knowledge level of breastfeeding benefits increased, community members' support and acceptance for breastfeeding in public spaces more.
There was also a significant relationship between the knowledge level of breastfeeding benefits for infants and the perceptions of the acceptability of breastfeeding in public spaces (r=0.42, p≤0.000). This finding suggested that as the knowledge level of breastfeeding benefits for infants increases, the more the community members exhibit acceptance attitudes towards mothers breastfeeding in public spaces (Table 7).
3.4.3. Relationship Between Variables: Combined (Mothers and Community Members)
The Pearson correlation coefficient and t-test were used to extract relationships between combined populations’ socio-demographic characteristics and knowledge level of breastfeeding benefits as well as perceptions of breastfeeding in public spaces as follow:
3.4.3.1. Ordered Variables (Educational Level, Parity and Age)
There was a significant positive correlation between the educational level (r=0.14, p≤0.047), parity (r=0.19, p≤0.009), age (r=0.15, p≤0.036), and knowledge level of breastfeeding benefits for infants. This finding indicates that when educational level, parity, and age increase, the knowledge levels of mothers and community members regarding breastfeeding benefits for infants also increase.
There was also a significant positive correlation between the age and knowledge level of breastfeeding benefits for mothers (r=0.20, p≤0.004). This finding suggested that as age increases, the knowledge levels of respondents regarding breastfeeding benefits for mothers also increases.
A positive association was discovered between the age and the perceived acceptability of breastfeeding in public spaces (r=0.29, p≤0.000), indicating that respondents accepted breastfeeding in public spaces more as their age progressed.
Another positive association was found between the age and perceptions of support for breastfeeding in public spaces (r=0.24, p≤0.001). This implies that respondents supported breastfeeding in public spaces to a greater extent as their ages progressed (Table 8).
3.4.3.2. Knowledge Level of Breastfeeding Versus Perceptions of Breastfeeding in Public Spaces
Finally, the researchers found a positive correlation between the knowledge level of breastfeeding benefits for infants and its’ support in public spaces (r=0.45, p≤0.000) and another significant correlation between the knowledge level of breastfeeding benefits for mothers and perceptions of support for breastfeeding in public spaces (r=0.29, p≤0.000). This suggested that as the respondents become more knowledgeable regarding breastfeeding benefits, the more they exhibit supportive attitudes towards it (Table 8).
4. DISCUSSION OF FINDINGS
The findings will be discussed according to the format of the questionnaire as combined populations (mothers and community members).
4.1. Socio-Demographic Characteristics
In this study, 60.6% of mothers and 67.7% of community members were single. This finding contrasted those of a study done in Nigeria, which reported that the majority of their respondents were married [49].
Most respondents had secondary school education (mothers= 60.6% and community members=63.5%), which could be due to that respondents did not pursue their tertiary education after high school education. This finding supported those of a previous study done in Italy, where, out of 523 respondents, 247 obtained high school certificates. However, the findings of the studies differ in that 21% had no formal education, and those who had tertiary education were more than in the current study [49, 50].
The study revealed that there were more unemployed mothers (58.5%) as compared to 38.5% of community members who were permanently employed. This finding correlates with those of a study done in Europe, with more than half of their participants (53.6%) who were unemployed [50].
The majority of mothers’ age ranged between 26-35 years (61.7%). In contrast, a study done in Mauritius regarding breastfeeding practice and infant feeding patterns reported fewer (38.4%) mothers who were aged 25-35 years old [51].
The highest percentage of mothers (72.3%) and community members (49.0%) had one or two children. The rationale behind this might be due to family planning utilization, which is available and accessible in local clinics for free. Consistent with the current findings, a study that was done in Ethiopia also reported that the majority of respondents’ parity ranged from 1-3 children [52].
4.2. Socio-Demographic Characteristics Versus Knowledge Level of Breastfeeding Benefits
Educational level has been associated with breastfeeding knowledge level, while lower employment showed a negative relationship with breastfeeding knowledge level [49, 50, 53]. A study conducted in Italy showed that improved education has a high positive impact on the knowledge level of breastfeeding [54]. Employed mothers are associated with decreased breastfeeding practice and knowledge of breastfeeding [55].
The current study findings regarding the association between the age and breastfeeding knowledge level concurred with those of investigators in Europe [50]. However, the findings contrasted with the study done in Nigeria, which reported a positive relationship between age and breastfeeding knowledge [49]. In a literature review, no data was found to rationalize this finding.
The findings of the current study indicated that mothers with more than one child (multiple parities) are associated with breastfeeding knowledge level. There are several possible rationales for the current finding: for example, previous exposure to breastfeeding and repeated breastfeeding education and information. This finding supported those of a study done in Malawi, which revealed that multiple parities have a positive impact on breastfeeding knowledge level [56].
The findings of the current study, which reported no relationship between marital status and knowledge level of breastfeeding, contrast with those of a study done in Italy, which indicated a positive relationship between marital status and breastfeeding knowledge [49]. The difference could be due to the study setting. In South Africa, husbands often do not involve themselves in infant feeding practices, which is culturally seen as mothers’ responsibility.
4.3. Socio-Demographic Characteristics Perceptions of Breastfeeding in Public Space Acceptability
The age of respondents was proportionally associated with perceptions of support and acceptance of breastfeeding in public spaces. The duration of exposure to previous breastfeeding and experience accumulated, as respondents get older, could account for the current findings. This finding supports those of the previous study done in the USA, which reported that the age progression had a directly proportional relationship with perceptions of support of breastfeeding in public environments [57]. However, the findings of the current study are not consistent with a previous study done in New York City, which found that older adults (65 years and older) are uncomfortable and unsupportive of breastfeeding in public spaces compared to those who are younger (18-44 years old). The difference could have resulted from the evolution of cultural acceptability of breastfeeding in public spaces [58]. Therefore, to enhance social acceptability and support breastfeeding in public and normalize it, cultural barriers need to be identified and solutions should be local context orientated.
4.4. Knowledge Level of Breastfeeding Benefits Versus Perceptions of Breastfeeding in Public Space
Our study revealed that the more knowledgeable people are of breastfeeding benefits, the more they have positive perceptions of support for breastfeeding in public spaces. Generally, people support an action that they are well informed about. A study conducted in the USA revealed that people who were well informed about breastfeeding exhibited more favorable views towards breastfeeding in public [59]. In contrast, several studies indicated that although communities are knowledgeable regarding breastfeeding, they are generally not positive about it in public spaces [60, 61]. Several explanations for these contrasting findings might be due to sexualization of breasts, cultural condemnation of breastfeeding in public and media, which portray formula feeding as more convenient over breastfeeding in public spaces [19, 20, 24].
5. LIMITATION OF THE STUDY
Data were collected by means of self-completion questionnaires. More in-depth information might have been obtained by conducting individual in-depth interviews with mothers and community members. No observations were conducted of women actually BF in public spaces. More information about specific challenges concerning BF in public spaces might have been obtained if interviews had been conducted with mothers of infants who were formula-fed.
CONCLUSION AND RECOMMENDATIONS
Altogether, 69% of mothers were comfortable to breastfeed in public spaces, and community members (84%) were supportive. The majority of respondents were knowledgeable regarding the breastfeeding benefits. However, there was no specific trend to favor the knowledge levels of either mothers or community members. The age, parity, and educational level were found to have a positive relationship with breastfeeding knowledge level. The knowledge that respondents possess concerning breastfeeding benefits has an impact on their perceptions regarding breastfeeding in public spaces. Limited knowledge of breastfeeding benefits was associated with unsupportive attitudes towards breastfeeding in public spaces. Health messages that target these factors are essential to encourage social support and acceptance of breastfeeding in public spaces. This could be executed through public education via posters in public spaces and during community health outreaches.
LIST OF ABBREVIATIONS
| BF | = Breastfeeding |
| EBF | = Exclusive Breastfeeding/breastfed |
| FA | = Factor Analysis |
| HREC | = Health Research Ethics Committee |
| IC | = Informed Consent |
| NWU | = North-West University |
| TV | = Total Variance |
| USA | = United States of America |
ETHICS APPROVAL & CONSENT TO PARTICIPATE
The ethical clearance to execute this study was granted by NWU HREC (Ref: NWU-00116-18-A1). Provincial consent (Ref: GP 201810 040) was obtained from the Gauteng Department of Health via the National Health Research Database website.
HUMAN AND ANIMAL RIGHTS
Animals were not part of this research. All human research procedures and protocols were followed in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975.
CONSENT FOR PUBLICATION
The respondents were informed about the study, including the aims, objectives, data collection process, interpretation and dissemination. The participation was voluntary, and respondents had the right and permission to withdraw from the study at any time without been penalised. All respondents signed IC. To ensure confidentiality, no names or any form of identification was written on the questionnaires. Hard copies of questionnaires and IC forms were scanned separately and then shredded. Electronic copies of scanned questionnaires, IC forms, excel sheets, and Statistical Package for Social Sciences files were kept on a password-protected external hard drive in NWU, Potchefstroom Campus, Quality in Nursing and Midwifery Research Focus Area office. Electronic copies will be deleted from the device and recycle bin in five years from the completion date of the study.
AVAILABILITY OF DATA AND MATERIALS
The data material used and analyzed during the current study are available from the corresponding author [M.N.] on request.
FUNDING
The study was partially funded (bursary for master’s degree students) by the Faculty of Health Sciences, NWU, Potchefstroom Campus. The partial funder (bursary department) was not involved in writing, editing, approval and/or decision to publish this study.
CONFLICT OF INTEREST
The authors declare that no conflict of interest, financial or otherwise, impacted on the current study.
ACKNOWLEDGEMENTS
The authors extend their gratitude to the NWU, Potchefstroom Campus and Gauteng Province Department of Health for granting permission to conduct this study. To the statistician from NWU, thank you for assisting with data analysis. The respondents are thanked for completing questionnaires and thereby supplying data for the current study.

