All published articles of this journal are available on ScienceDirect.

Analysis of HIV/AIDS Integration into the Academic Curriculum at a Selected University in South Africa
Authors Info & Affiliations
Abstract
Background:
Although there is evidence that education is a social weapon in the fight against HIV/AIDS, there is also evidence that, to date, HIV/AIDS is not fully integrated into all the disciplines in Higher Education Institutions (HEIs). Therefore, most of the university students in South Africa are not well prepared to be HIV/AIDS-competent graduates who can live and work in a society ravaged by AIDS.
Objective:
This study sought to analyse the extent of HIV/AIDS integration into the curricula in various departments at a selected university in the Limpopo Province, South Africa.
Materials and Methods:
The study used quantitative and qualitative approaches to analyse the extent of HIV/AIDS integration into the curricula. The curriculum calendars were retrieved from the university website. An audit tool guided retrieval of HIV/AIDS content and was analysed using SPSS V 25. The qualitative content analysis was used to describe the nature of HIV/AIDS content.
Results:
Out of eight schools, about 68 modules had HIV/AIDS content. The majority of the modules (53; 78%) were offered at the undergraduate level. Furthermore, the majority of the HIV/AIDS content (62; 91%) was integrated into undergraduate compulsory modules. Most (34; 51%) of the HIV/AIDS content were located in health sciences disciplines. HIV/AIDS content was mostly integrated into existing carrier modules. Time allocation for the teaching of HIV/AIDS was not indicated. Most of the modules did have information about teaching and assessment strategies.
Conclusion:
It is recommended that discipline-specific HIV/AIDS content be integrated into all disciplines.
1. INTRODUCTION
South Africa has the highest prevalence of HIV infections among youth and adolescents worldwide, accounting for nearly 18% of global HIV infections among 15 to 24-year-old youth in 2016 [1]. Despite the decrease in HIV infections worldwide, South Africa had 9.9 new infections per 1000 adults in 2016, with approximately 37% of those new infections in young people aged 15–24 years 22% in young women [2]. The high prevalence of sexually transmitted infections (STIs), including HIV among South African youth, is attributed to the fact that young people engage in risky sexual behaviours such as non-condom use, multiple sexual partners, transactional sex and early sexual debut [3]. These young people include university going students who are more vulnerable to HIV infections as compared to the general population [4, 5]. In light of this, there remains a critical need to prevent HIV among the youth if the battle is against the pandemic is to be won [6].
Higher Education Institutions (HEIs) in South Africa decided to integrate HIV/AIDS into the curriculum to produce HIV/AIDS competent graduates [7]. In a bid to ensure that students in the tertiary sector are adequately prepared to live and work in a society ravaged by HIV/AIDS, the higher educator sector was singled out as having a pivotal role to play in responding to the impact of HIVAIDS [8]. For instance, the core business of universities such as teaching, research, and engagement, were seen as the most contributors towards addressing the epidemic [9].
The rationale for including HIV/AIDS in the university curriculum is undeniable in South Africa and beyond. The basic argument for incorporating HIV/AIDS into the curriculum rest on the protective effect of education on health [10]. The assumption is that HIV/AIDS education is pivotal in ensuring that students have the necessary knowledge and skills to adopt protective behaviours against HIV, other sexually transmitted infections and unintended pregnancies [7]. Although authors [11-13] observed that “increased knowledge about HIV/IDS may not necessarily lead to positive behaviour change, yet knowledge about a disease may be an initial step towards behavioral risk change”. Hence, it is acknowledged as the first stage in the behaviour change process [14]. As such higher education occupies a unique position to influence the discussion, to act and to develop policy on HIV/AIDS, and, in the absence of a cure, education is the best social solution to the epidemic [10].
It is argued that higher education institutions have a moral and intellectual duty to produce students who can deal with HIV and AIDS on a personal and professional basis and find creative solutions to this epidemic [15, 16]. This simply implies that students are the future leaders in government and private sectors in terms of any country's development. Therefore, it is imperative to target this age group cohort for HIV and sexuality education [8, 17]. Therefore, universities should be at the forefront of battling the pandemic as most students fall under HIV at-risk population group of under 25, and HIV/AIDS can undermine the function of higher education institutions [17]. Due to the absence of a vaccine or cure for HIV/ AIDS, its prevention relies on the adoption of safe sexual behaviours and therefore, education remains the critical enabler for changing risk behaviours [8, 17]. It is against this backdrop that universities have an essential role to play in the fight against the pandemic.
Despite HIV/AIDS education being singled out as urgent much has not been done to integrate it into the academic curriculum [7, 10]. They are a few examples that highlight how HIV/AIDS content is being introduced into academic curricula in different universities across the globe. Needs assessment surveys and reviews conducted in Africa and around the world to measure the HIV/AIDS curricular response show that the teaching of HIV/AIDS was minimum; it depended on the interest of the faculty [9, 18-23]. In general, HIV/AIDS education in higher education is offered in four main ways: stand-alone module, adding it into existing modules, HIV/AIDS focused qualifications, and HIV/AIDS focused research [9, 21, 23]. The reluctance or inability to teach about HIV/AIDS has been attributed to several factors. Lecturers who are supposed to teach HIV/AIDS have insufficient knowledge about curriculum integration, fear that HIV and AIDS content can dilute discipline content, they are not trained to teach sensitive issues in class, and they see it as a waste of time [24-26]
There is little information available concerning howHEIs in South Africa integrate HIV/AIDS into the curriculum [25, 27-29] (25, 27-29). The bulk of HIV initiatives in higher education are extra-curricular rather than curricular. Little is known about how it is taught. Information provided by previous surveys regarding the teaching of HIV/AIDS is based on academic perceptions [9, 20-22, 30]. Therefore the current study seeks to provide an in-depth analysis of how HIV/AIDS is integrated into curricula.
The university students at the institution engage in unprotected sex, putting themselves at risk of HIV infection as confirmed by different studies conducted at the university [31, 32]. Also, regular student reproductive health statistics at the university suggest there is an increase of STIs(60%), HIV infections(100%), termination of pregnancies(32%) referrals(40%) and unplanned pregnancies(60%)in the last five years [33]. Furthermore, a recent study at the University of Venda suggests that male students have a negative attitude towards contraceptives, such as condoms, and they did not use them [34]. Besides, there is inadequate HIV/AIDS education and limited commitment by the university to support these programmes [35]. Taken together, these facts provide a compelling rationale to focus on HIV/AIDS education in Higher education institutions [36]. The purpose of the study was to analyse the extent of HIV/AIDS integration in the curricula in various schools and departments at the University of Venda.
2. MATERIALS AND METHODS
2.1. Study Setting
The University of Venda (UNIVEN) was founded in 1981 and is in the Vhembe district of the Limpopo Province, South Africa. In 2002, the Department of Higher Education and Training mandated the UNIVEN to become a comprehensive university focusing on professional and career-focused programmes. The university's academic configuration has eight schools and 59 departments offering a range of undergraduate and postgraduate academic programmes in various subjects. The eight schools include Agricultural Sciences, Education, Environmental Sciences, Health Sciences, Human and Social sciences, Law, Management Sciences and Mathematical and Natural Sciences. It has about 15,704 students, inclusive of postgraduates and undergraduates. Furthermore, it has a staff capacity of 800 comprising of teaching staff, administrative, staff and support staff [37].
2.2. Study Design
Content analysis was used to analyse the documentation obtained. Content analysis is a procedure for analysing text and has been used in research exploring newspaper articles and interview transcripts [38]. This study applied quantitative and qualitative content analysis to examine the extent of HIV/AIDS content in the curricula. The rationale for using this approach was to conduct an in-depth analysis of the extent of HIV/AIDS content integration into the various modules at the university. The quantitative content analysis enabled us to quantify the amount of HIV/AIDS content being currently taught in the curriculum across all schools. In addition, the qualitative component allowed us to analyse in detail the modules with HIV/AIDS content. The study was conducted after permission was granted by the University of Venda Research and Ethics Committee (SHS/17/PH/08/1506).
2.3. Study Population
The study utilised the online 2018 University of Venda academic calendar. The calendar module information includes the module name, title, contents and codes. The academic calendar of the University of Venda contains detailed information on all the courses offered in each department, including the course codes, the course titles and synopses of course contents.
2.4. Sampling and Sampling Procedure
The sampling method was purposive. Copies of the eight [8] calendars, one from each school were obtained online. Using these school calendars, modules with HIV/AIDS content were examined. Those modules with HIV/AIDS content descriptions were set aside. Those without HIV/AIDS content were excluded from the study, and 68 modules with HIV/AIDS content were identified.
2.5. Data Collection
Using both the 2018 online university and school calendars, all modules with HIV/AIDS content were carefully analysed. The calendars for all schools/faculties were painstakingly gone through from one department to the other. The study assumes that courses that feature HIV/AIDS content have integrated some form of HIV/AIDS content into the curriculum. The data was collected by two different research assistants who were working independently. To evaluate the curricula, a data extraction tool was developed by the research team. The research team used this tool, and then they compared the results so as to reach a consensus regarding the content related to HIV/AIDS content.
2.6. Data Analysis
Data was analysed using content analysis methods suggested by [38]. Content analysis involves coding and analysing qualitative data using deductive and inductive approaches [39]. For example, deduction analysis was used by developing codes based on the study objectives. Frequency analysis for each of the categories across all curricula was used to provide a guide to the extensiveness of HIV/AIDS content present. This was done using the descriptive statistics function of SPSS 24.0 to identify frequencies and percentages. Further, the curricula was analysed inductively using thematic analysis.
3. RESULTS
3.1. Modules with HIV/AIDS Content Across Schools
The findings revealed that a total of 68 modules/courses out of 1979 modules had HIV/AIDS content. The results show that the School of Health Sciences led with 34 modules (50%) with HIV/AIDS content, followed by Human and Social Sciences with ten modules (15%). The School of Education was in the third position with eight modules (12%). The School of Law was in the fourth position with seven modules. School of Agriculture claimed the fifth position with three modules (4%), followed by Schools of Environmental Science and Management Science, which shared the fifth spot with two modules (3%) each. These findings are summarised in Tables 1 and 2.
| School | Departments |
|---|---|
| Agriculture Sciences, | 10 |
| Education, | 5 |
| Environmental Sciences, | 5 |
| Health Sciences, | 5 |
| Human & Social sciences | 8 |
| Law | 6 |
| Management Sciences | 9 |
| Mathematical & Natural Sciences | 9 |
| School/Faculty Name | Modules with HIV/AIDS content | % |
|---|---|---|
| Agriculture Sciences | 3 | 5% |
| Environmental Sciences | 2 | 3% |
| Education | 8 | 12% |
| Health Sciences | 34 | 51% |
| Human and Social Sciences | 10 | 13.% |
| Law | 7 | 10% |
| Maths and Natural Science | 2 | 3% |
| Management | 2 | 3% |
| TOTAL | 68 | 100% |
3.2. Modules with HIV/AIDS Content Across each Department and Schools
In the School of Agriculture, only three departments had courses/modules with HIV/AIDS content. The Department of Plant Production, Consumer Science, and Institute of Rural Development had one module (33.3%) each with HIV/AIDS content. Against all expectations, the Department of Forestry, Horticulture, Soil Science, Animal Science, Food Science and Technology, Agricultural Economics and Agricultural and Rural Engineering did not have any modules with HIV/AIDS content. In the School of Health Sciences, all the departments had modules with HIV/AIDS content. The Department of Public Health was the front runner offering 14 modules (41%) with HIV/AIDS-related content, followed by the Department of Advanced Nursing Science with seven (20.5%) modules. The Department of Nutrition Science came third with seven modules (20.5%) and Department of Psychology five modules (14.7%) and Centre for Biokinetics, Recreation and Sport Science performed poorly with one module (2.9%).
The results also reflected that only two departments in the School of Management Sciences offer modules with HIV/AIDS content. The Department of Business Management and Tourism and Hospitality Management had each one module (50%) with HIV/AIDS content, respectively. In the School of Law, the Department of Criminal justice offered three modules (43%) with HIV/AIDS content, followed by the Department of Public Law with two modules (28.5%). The Department of Criminal and Procedure Law and Mercantile Law have one module (14.2%) each, respectively. In the School of Education, all departments had modules with HIV/AIDS content. The Department of Foundations of Education offered four modules (50%) with HIV/AIDS, followed by Curriculum Studies, Early Childhood, Education Management and Professional Studies, with each offering one module (12.5%), respectively.
In the school of Mathematics and Natural Sciences, only the department of Microbiology had two modules with HIV/AIDS content. Surprisingly, the Department of Biochemistry, Chemistry, Computer Science, Botany, Physics, Statistics, Zoology and Mathematics, and Applied Mathematics had no modules (0.0%) with HIV/AIDS content. In the School of Human and Social Sciences, the Centre for African Studies has the highest number of modules 3(30%) with HIV/AIDS content, followed by the department of social work with two modules (20%), Department of Development Studies 1 (10%) and Communication and Applied languages 2 (20%). The Mathivha Centre for African Languages, Arts, and Culture did not have any (0.0%) modules with HIV/AIDS content. In the school of Environmental Sciences, the Department of Geography and Geoinformation Sciences and Hydrology and Water Resources each had one module (50%) with HIV/AIDS content. However, the Department of Ecology and Resource Management, Mining and Environment Geology and Urban and Regional Planning did not have (0.0%) modules with HIV/AIDS content. This is summarised in Table 3.
| Department Name | Modules with HIV/AIDS content | % |
|---|---|---|
| Agricultural Economics & Agribusiness | 0 | 0.0% |
| Agriculture and rural engineering | 0 | 0.0% |
| Animal Science | 0 | 0.0% |
| Consumer Science | 1 | 33.3% |
| Forestry | 0 | 0.0% |
| Food Science & Technology | 0 | 0.0% |
| Institute of Rural development | 1 | 33.3% |
| Horticulture sciences | 0 | 0.0% |
| Plant production | 1 | 33.3% |
| Soil Science | 0 | 0.0% |
| Advance Nursing science | 7 | 20.5% |
| Centre for Biokinetics, recreation sports science | 1 | 2.9% |
| Public Health | 14 | 41% |
| Psychology | 5 | 14.7% |
| Nutrition science | 7 | 20.5% |
| Accountancy | 0 | 0.0 |
| Business information system | 0 | 0.0 |
| Business Management | 1 | 50% |
| Economics | 0 | 0.0 |
| Human resource management & Labour relations | 0 | 0.0 |
| Public and Development Administration | 0 | 0.0 |
| Tourism and Hospitality Management | 1 | 50% |
| OR Tambo Institute of governance | - | - |
| Criminal justice | 4 | 57% |
| Criminal and Procedure Law | 1 | 14.2% |
| Jurisprudence | 0 | 0.0% |
| Mercantile Law | 1 | 14.2% |
| Private Law | 0 | 0.0% |
| Public Law | 1 | 14.2% |
| Curriculum studies | 1 | 12.5% |
| Early childhood education | 1 | 12.5% |
| Education Management | 1 | 12.5% |
| Foundations of Education | 4 | 50% |
| Professional studies | 1 | 12.5% |
| Biochemistry | 0 | 0.0% |
| Botany | 0 | 0.0% |
| Chemistry | 0 | 0.0% |
| Computer Science | 0 | 0.0% |
| Physics | 0 | 0.0% |
| Statistics | 0 | 0.0% |
| Mathematics and Applied Mathematics department | 0 | 0.0% |
| Microbiology | 2 | 100 |
| Centre for African studies | 3 | 30 |
| Communication and Applied languages | 2 | 20 |
| Development Studies | 1 | 10 |
| English | 1 | 10 |
| Institute for Gender and Youth studies | 1 | 10 |
| MER Mathivha Centre for African languages, Arts and Culture | 0 | 0.0 |
| Social Work | 2 | 20 |
| Media studies | 1 | 10 |
| Ecology and resource management | 0 | 0.0% |
| Geography and Geoinformation sciences | 1 | 50% |
| Hydrology and water resources | 1 | 50% |
| Mining and Environmental Geology | 0 | 0.0% |
| Urban and regional planning | 0 | 0.0% |
| TOTAL | 2 |
3.3. Distribution of Modules with HIV/AIDS Content
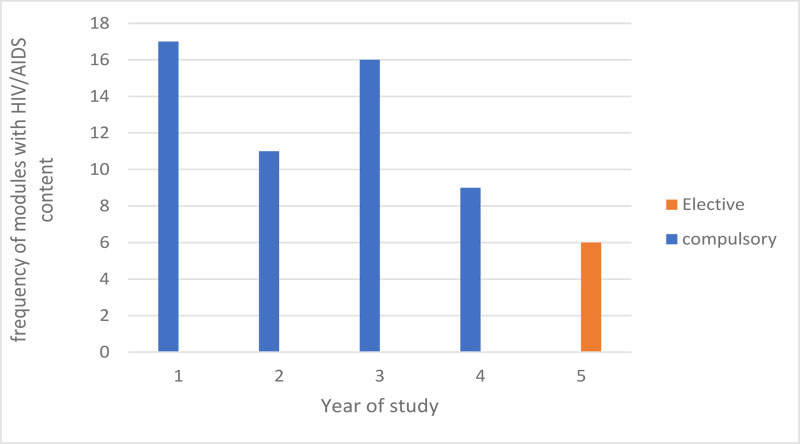
The majority of the modules with HIV/AIDS content, 62(91%) were compulsory, whereas 6(9%) were electives and were postgraduate modules only (Fig. 1). HIV/AIDS content was unevenly distributed across years of study, with more content covered in the first year than any other year. Majority of modules with HIV/AIDS content were found at first-year level 17(27%), followed by the second-year group, which had 11(16%). Regarding the third year, it had 16(24%) followed by fourth 9(13%) and postgraduate levels 15 (22%) (Fig. 1).
3.4. Thematic Analysis of Modules with HIV/AIDS Content
This section provides an overview of modules with HIV/AIDS content. The thematic analyses of the curricula yielded four themes: mode of delivery, teaching/learning tools, assessment strategies, topics/content covered. The gaps, opportunities and strengths in the curricula were also considered (Table 4).
| Theme | Sub themes |
|---|---|
| 1.Mode of delivery | 1.1 Stand- alone modules |
| 1.2 Integrated into existing modules | |
| 1.3 Infusion | |
| 2.Teaching & learning tools | 2.1 Lectures |
| 2.2 Group discussions | |
| 2.3 Presentations | |
| 2.4 Case study/scenarios | |
| 2.5 Class discussion | |
| 2.6 Problem based learning | |
| 2.7 Research projects | |
| 2.8 Work based learning | |
| 2.9 Guest lecture/workshops | |
| 2.10 Role play | |
| 3.Assessment strategies | |
| 3.1 Test | |
| 3.2 Written examinations | |
| 3.2 Assignments | |
| 3.3 Oral Presentations | |
| 4.Topic/Content covered | 4.1 Knowledge |
| 4.2 Attitude | |
| 4.3 Skills |
3.4.1. HIV/AIDS Topic/Content Covered
Although the modules with HIV/AIDS content were from different disciplines, three themes emerged. Knowledge, attitude and skills. Majority of the HIV/AIDS content was knowledge-based. Most of the modules reflected on HIV/AIDS epidemiology issues such as basic facts, for example, definitions, types HIV strain, HIV/AIDS statistics, the impact of HIV/AIDS on a different population, HIV transmission routes, stages of infection, clinical symptoms/ of HIV/AIDS, myths about HIV/AIDS. Another prominent knowledge area was the treatment of HIV/AIDS as a disease. Treatment issues such as anti-retroviral therapy, HIV vaccines, adherence to medication, medication side effects and defaulting. Prevention was another issue, which emerged after analysis. HIV and voluntary testing, abstinence, safer sex practices, HIV/AIDS education, community-based HIV/AIDS education, needle exchange, prevention of mother to child transmission, prophylaxis, legislations and male circumcision were some of the issues. To a lesser extent, the HIV/AIDS content objectives addressed the affective domain in the form of psychosocial issues such as HIV/AIDS stigma, workplace discrimination, coping with HIV/AIDS, mental health issues, voluntary counselling and testing, ethical issues and confidentiality. This was realised mainly in psychology and nursing modules. The skills component was not visible and rarely addressed (Table 4).
It was realised that the breadth and depth of the HIV/AIDS content in these modules have some gaps. The HIV/AIDS content focused mainly on knowledge and neglected effective and skill components aspects. Hence, this kind of information is not balanced enough to equip the students with knowledge and skills to engage with the epidemic effectively. Students are unable to see the connection between the disease and how they can contribute to fighting against it from the perspective of their disciplines. Further, it is challenging to ascertain what time is allocated to the topic or content. It was also realised that when HIV/AIDS content was offered, it was once off.
3.4.2. Mode of Delivery
The modules selected in this sample reflect a wide variety of approaches adopted towards HIV/AIDS. HIV/AIDS content was integrated into different modules using a variety of curriculum models. Majority of HIV/AIDS content was integrated into an existing carrier module such as psychology, social work, gender studies, nursing, public health, nutrition, sociology, microbiology and media studies. The thematic analysis further shows that infusion is another approach used to integrate HIV/AIDS content into disciplines such as Law, English, Environmental sciences, hydrology, tourism, economics and Agriculture. HIV/AIDS stand-alone modules were also used mostly in the school of education. Stand-alone modules focus primarily or exclusively on necessary information about HIV/AIDS and ways to prevent HIV infection. In this case, all the five stand-alone modules were in the school of education, and they targeted all pre-service teachers in different departments (Table 4).
3.4.3. Teaching & Learning Tools
The thematic analysis shows that HIV/AIDS was taught using a range of teaching and learning methods. Most of the HIV/AIDS content in health, social sciences law and education disciplines was delivered by in classroom methods such as lectures, group discussions, presentations, case study/scenarios, class discussion, research projects, guest lectures by experts. Student-centered problem-based learning method was limited to the school of health sciences. Out of class experiential learning techniques were limited, but there were few examples such as work-based practical and role-plays, which were also used to teach about HIV/AIDS content most in health sciences disciplines (Table 4). The content analysis suggests that there is a huge reliance on traditional didactic classroom-based teaching methods such as lectures, which are not effective in teaching HIV/AIDS education because they lead to information fatigue among students. Opportunities for experiential learning are very few; hence students are unlikely to develop skills or behaviours that facilitate behaviour change. Further, some modules with HIV/AIDS content in environmental sciences, agriculture, mathematical and Natural sciences and management disciplines did not specify the teaching strategies to deliver HIV/AIDS content.
3.4.4. Assessment Strategies
Content analysis shows that modules in education and health sciences written examination, tests and assignments were the most common assessment methods used to assess students HIV/AIDS content. However, it should be noted that other modules with HIV/AIDS content from other schools especially did not specify the assessment strategies. This analysis points out that traditional assessment strategies were still used to assess HIV/AIDS content.
4. DISCUSSION
The study found out that HIV/AIDS content was integrated into only 68 modules. These findings corroborate the surveys conducted by [9, 21, 30], which also concluded that minimal HIV/AIDS content is included in the curricula. Furthermore, this corroborates a recent systematic review conducted by [7], which also indicated that worldwide that HIV/AIDS content is not fully integrated into curricula. These findings show that little progress has been made regarding the integration of HIV/AIDS content into curricula since previous studies in 2005 and 2010, which indicated that integration of HIV/AIDS content was neglected by most higher education institutions in South Africa [7]. This can be explained by the fact that lecturers who are supposed to teach HIV/AIDS have insufficient knowledge about curriculum integration, fear that HIV and AIDS content can dilute discipline content, they are not trained to teach sensitive issues in class, and they see it as a waste of time [15].
Similar to other studies, our study reported that HIV/AIDS content was integrated mainly into health sciences disciplines [9, 10, 21, 40]. This is not surprising since this is the trend nationally and internationally, whereby HIV/AIDS issues are regarded as health issues rather than as social issues [9, 23]. More so, health, medical and allied health disciplines are expected by their respective degree councils to equip students with HIV/AIDS competencies [7]. This can also be explained by the fact that the majority of the lecturer in universities do not understand what integration entails [15, 28]. It may be that curricular content reflects the views and interests of academics teaching these modules. HIV/AIDS content can be integrated into a variety of modules in any discipline [15, 25, 41].
The study findings also showed that HIV/AIDS content was integrated more into undergraduate compulsory first-year level modules. This is in line with studies conducted in different countries to assess the integration of HIV/AIDS into the academic curriculum in higher learning institutions [7, 30, 42]. HEAIDS (2010) recommends that HIV/AIDS content should be taught at all levels of learning, beginning at the entry-level of education so that students grow with filters as they progress. Authors [7, 29] argue that “that while students must learn about the specific aspects of the pandemic that will impact on their professional practice, the inclusion of HIV in only one module may limit the student's understanding of the complex nature of the pandemic”. This means that lack of cross-curriculum integration may mean that students forget what they have learned since it is not reinforced in other modules. Besides, it is argued that HIV/AIDS content should be embedded in all modules that are compulsory at all levels because HIV/AIDS affects everyone [15, 25, 26, 30, 43]. All graduates are expected to be exposed to HIV/AIDS content from entry-level to exit level [7]. From a holistic perspective, HIV/AIDS education can be integrated into every discipline, but this needs to be done at the programme level when curricula are designed to avoid repetition and omission of knowledge and skills [44].
The narrow HIV/AIDS content found in the curricula, mainly focuses on biomedical aspects such as epidemiology, prevention, psychosocial factors and treatment. Similar findings were reported in previous studies [15, 30, 41]. According to behaviour change theories, knowledge, attitudes, and skills are the keys to the decision to adopt or change HIV risk behaviours [45, 46]. Therefore, if HIV/AIDS education is to be effective, three components must be holistically addressed by the curriculum; they should emphasize knowledge, attitude skills to achieve the change of behaviour [45, 47]. HIV/AIDS content or competencies should have a reflection of both cognitive and affective domains that may influence behaviour change among the youth [5, 9, 23]. Young people in South Africa and beyond possess a high level of knowledge about HIV/AIDS [21, 48]. However, there is a gap between knowledge and behaviour change among youth [3]. Authors [7, 8, 49] suggest HIV/AIDS education is best approached from a critical paradigm that recognises the need to challenge and change social norms, human behaviour, laws, policies and practices in societies impacted by the pandemic. They pinpointed issues such as social justice issues, gender inequalities, poverty, legal implications, developmental implications, management and workplace issues, social and psychological issues, ethical issues, human rights issues, health issues as some of the issues to be included in the curriculum [7]. Others suggest that content should be relevant to both the discipline and the context in which the students live and work [15, 28]. This implies that professionals interacting with the public must be able to deal with constraints imposed by socio-cultural norms around HIV/ AIDS and related topics [9].
Majority of the modules had HIV/AIDS content integrated into the carrier module, followed by HIV-infused modules and then stand-alone modules. This corresponds to an HIV/AIDS curriculum audit conducted at other institutions [9, 21, 22, 30, 43], which found the same pattern that HIV/AIDS was integrated into the main carrier. Integration into a 'carrier' courses is where HIV/AIDS is relevant in certain courses in the health and social sciences, education, or that deal with ethics or human rights [7]. This is because it is technically and administratively simpler and more feasible to accomplish [7, 10]. In addition, it is clear where and when to include it and who is responsible for it, needs fewer specialised teachers and assessment is facilitated [10]. However, despite being simple, the integration of HIV/AIDS into carrier modules means that certain aspects of HIV/ AIDS can be included in the module, and other equally important elements will be neglected [18]. Authors [7, 28, 29] suggests that there is a need to adopt a holistic view of HIV/AIDS in the curriculum; therefore, a stand-alone module, if used, needs to be supplemented by some form of curricular infusion at the programme level to ensure adequate coverage and avoidance of duplication.
The content analysis further indicates teaching methods were didactic in nature, and the majority of modules omitted the teaching strategies. This study is consistent with research conducted in other higher education institutions, which concluded that traditional classroom-based teaching strategies were the most commonly used methods for delivering HIV/AIDS education [9, 20-23]. Different pedagogy scholars argue that traditional classroom-based teaching does not promote deep learning despite being praised for maintaining academic rigour [50, 51]. Authors [10, 51] suggest that interactive and participatory methods that encourage participation and discussion among teachers and students are central to the teaching and learning of HIV/AIDS among young people. Therefore, active participation and experiential learning approaches, interactive learning methods and internet-based online are recommended [8, 17, 44]. In other words, when teaching HIV/AIDS education, there should be a mix of didactic and experiential approaches.
The study also shows that most modules did not specify assessment strategies. However, modules in the school of health and education, indicate that traditional assessment methods such as examination, tests and assignment methods were used to evaluate HIV/AIDS content. In the context of tertiary education in South Africa, traditional evaluation methods are the norm, as reflected in the use of written examinations, testing and assignments [52]. Traditional examination-based evaluation, while praised for setting standards across a student group, is criticised for not being effective in measuring individual learning. Innovative methods of assessment that encourage reflection on learning experience are required [52].
CONCLUSION
The study concludes that HIV/AIDS content is taught in all schools at UNIVEN. Out of 68 modules that teach HIV/AIDS content, it is mainly taught at the undergraduate level and mostly in health sciences disciplines. Although there is evidence that HIV/AIDS content is found across all schools curricula, several departments in the School of Mathematical & Natural sciences, Agriculture Sciences, Management Sciences and Environmental Sciences did not have modules with HIV/AIDS content. This suggests that most departments at Univen are not integrating HIV/AIDS content. It is recommended that HIV/AIDS content should be integrated into all postgraduate and undergraduate disciplines. Furthermore, considering that HIV/AIDS is a fast-paced field, regular curricular reviews should be conducted to update and strengthen those modules with existing HIV/AIDS content.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was reviewed, and full ethical clearance was granted by the Research and Ethics Committee of University of Venda, South Africa (SHS/17/PH/08/1506).
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
Not applicable.
AVAILABILITY OF DATA AND MATERIALS
Not applicable.
FUNDING
The research was funded by University of Venda Research and Publications Committee (SHS/17/PH/16) and Higher Education South Africa (HESA) E376. The funders only provided financial resources to support the implementation of the study. The researchers wrote six-monthly reports to appraise the funders of progress regarding the study.
CONFLICT OF INTERESTS
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

