All published articles of this journal are available on ScienceDirect.

The Effects of Meditation with a Biofeedback Program on Stress and Depression Levels among People with Mild Depression Diabetes
Authors Info & Affiliations
Abstract
Background:
The increased amount of depression among people with diabetes is a burden on society. Biofeedback and meditation can impact the self-regulation of this group.
Objective:
This study aims to study the effect of combining meditation with a biofeedback training program on the stress and depression among diabetes people with mild depression.
Methods:
This study is based on a randomized controlled trial approach.
One hundred two participants were divided into three groups of 34 participants each, involving meditation, a combination of meditation and Skin Conductance (SC) with Skin Temperature (ST) biofeedback, and a control group. All three groups received routine nursing. Measurements were made using the Symptoms of Stress Inventory (SOSI) and the Beck Depression Inventory (BDI). Data were analyzed using frequency, percentage, mean, standard deviation, and MANOVA and MANCOVA. The duration of the study was from June 2018 to October 2019.
Results:
There were statistically significant differences in stress and depression among the three groups. Those receiving both meditation and biofeedback had the greatest reduction in the linear combination of stress and depression. Accordingly, the biofeedback program is a program that is capable of helping people learn how to relax, as biofeedback instruments feed information back to people through on-screen visual signals, thus enabling them to learn about their progress and success.
Conclusion:
In summary, a combination of meditation and SC and ST biofeedback can reduce stress and depression in people with mild depression diabetes.
1. INTRODUCTION
The number of people with diabetes is continually increasing, globally. The World Health Organization [1] has reported that type 2 diabetes is considered a severe challenge for the healthcare system of countries and it includes approximately 90% of diabetic people [1]. Diabetes is a kind of chronic disease that causes adverse economic and social effects since it requires long-term treatment. In every phase of treatment, people are likely to have risks of acute and chronic complications, which may lead to disability or death [2]. When some people have complications, they are unable to work as usual and become dependent on their family members in terms of expenses and care [3]. Since it is a severe chronic disease and requires long-term treatment, it causes high expenditures for treatment, resulting in changes in the overall economy of the nation [3].
According to the literature review, it was found that major psychological impacts can occur after having been sick with diabetes. Among the psychological impacts of diabetes are the effects it has on one’s self-esteem and self-image [4]. These individuals are less aware of their values because they cannot work hard and feel fatigued because of their high blood glucose levels. Some people have to quit their jobs because of their need for self-care [5]. Illness-related stress is a common reaction to DM [6, 7]. There are many reasons for stress in people with diabetes, including, for example, conditions of the chronic disease, treatment received, lifestyle changes, economic situations, and changes in social roles. Significant negative impacts can also occur after DM. These major negative impacts cause tension arising from the nature of those diseases, such as suffering for months, years or even a lifetime while receiving treatment in a hospital regularly, as well as feeling depressed or having subsequent complications [8, 9]. Studies have shown that the most frequent problems of people with diabetes include such connecting factors as psychological stress and depression [10-21]. Researchers have asserted that comorbid DM and depression appear to have an additive effect on mortality rates [18, 22].
Most current treatments for diabetes mellitus are geared toward palliative physical treatments and the prevention of exacerbations and complications. People with diabetes may have to take medication for the rest of their lives. However, pharmacological treatment alone remains inadequate. Although emotional care is also important in reducing the exacerbation of the disease, there is less attention to its importance [23, 24]. Consequently, several self-regulation techniques are available for emotional care. According to the literature review, meditation plays a key role in positive physiological and psychological states in people with diabetes [25-30]. Most importantly, meditation can help reduce the stress and depression of these individuals [31-33].
While there are multiple approaches to meditation, transcendental meditation (TM) involves the use of chanting or mantras as focal points for concentration or attention [32, 34]. With TM, the person's body achieves a deep rest state as mental activities decline. As a result, symptoms of stress are relieved, and the nervous system is re-energized [35-37]. When people practice TM, their bodies achieve a condition marked by deep relaxation, which is contrary to the fight or flight response [38]. Practiced regularly, TM offers greater coherence in brain function, in which the person’s mind becomes more perceptive, focused, creative, and intelligent [38-40]. The person that practices TM can learn about advanced practices in order to enhance his/her cognitive and active abilities as a result of the slightest yet more powerful state of awareness [32, 37, 39]. Regular practice of TM effectively rehabilitates people by relieving their psychological stress [30, 34, 36-38, 41], anxiety [32, 34, 38], the organization of their brain function [34, 38, 42], the enhancement of harmony [43], and the development of optimistic social interactions [32]. Furthermore, TM is associated with a physiological means for combating depression [41]. Studies have shown that TM has been found to bring about positive psychological effects in people with diabetes [30, 32, 44-46].
Another intervention with potential value for controlling or reducing stress and depression for people with diabetes is biofeedback. Skin conductance (SC) and skin temperature (ST) biofeedback are used to assess the physiological reactions to stress changes inside the body. SC biofeedback is a vehicle that can enable people to control their perspiration gland function under mental control through relaxation. ST biofeedback is the process of using equipment to practice body temperature control through relaxation. SC and ST biofeedback closes the gap between autonomic functions and awareness. Through SC and ST biofeedback, people can learn to control physiological processes that are usually controlled by the autonomic nervous system. By applying biofeedback, people can learn how to gain cognitive control over this autonomic system. As a result, these people will be able to increase their attention [47-49], balance within the elderly population [50], and cognitive effects [51]. Furthermore, biofeedback can decrease negative symptoms such as headache [52, 53], stress [54-58], combined stress and anxiety [59], anxiety [57, 60], chronic back pain [61], depression and anxiety [62, 63], stress, combined anxiety and depression [64-66] and depression [67].
As previously stated, biofeedback alone can yield positive outcomes. Nevertheless, combining biofeedback with other programs has proven to obtain even better outcomes [54]. According to previous studies, the combination of meditation and biofeedback programs can be useful for people that have DM [64, 68, 69]. As a supplement to meditation, biofeedback is useful for improving the psychological condition of people that are diabetic by reducing stress and depression [32, 56, 64, 70, 71]. Additionally, there are now only a few research designs aimed at testing the effect of combining meditation with biofeedback as a means of lowering stress and depressive symptoms among people with diabetes in Thailand.
This study aims to study the effect of combining meditation with a biofeedback training program on the stress and depression levels among DM people with mild depression.
2. MATERIALS AND METHODS
The present study consists of a Randomized Controlled Trial (RCT) approach involving meditation, a combination of meditation and SC with ST biofeedback, and a control group receiving routine care only. Experimental group 1 received meditation training, experimental group 2 received meditation training in combination with the SC and ST biofeedback training programs, and the control group did not participate in the training program. All three groups received routine care. One hundred two participants were matched in pairs in three groups of 34 subjects per group based on sex, age, and disease. Measurements were made using the SOSI, SC, and ST biofeedback instrument and BDI. The differences in stress and depression among the diabetic people were compared among the people who had meditated, the people who had both meditated and practiced the biofeedback program, and the people who did not participate in the experimental program. A questionnaire was used to collect information on the socio-demographic characteristics of the study samples, including sex, age, education level, marital status, monthly household income, income sufficiency, occupation, and access to medical care and symptom diagnosis. The SOSI comprised 107 questions, as created by Leckie and Thompson in 1979 (adjusted from the Cornell Medical Index) and was compiled into the Thai language by Muecke in 1994. The BDI comprises 20 questions. It was arranged in a multi-choice answer format created by Beck in 1982 [72] and was compiled into the Thai language by Ruchiwit [73].
The mentioned types of interventions offer a framework for the achievement of essential self-regulation skills to cope with stress and depression disorders in people with diabetes, as shown in Fig. (1).
2.1. Sample/Participants
The sample group was composed of adult and older people who were diagnosed with type 2 DM with or without comorbidities and were treated at the General Practice Outpatient Department at Thammasat University Hospital (TUH) in Thailand. A previous research study conducted by Thongkhum, Ruchiwit, and Somprasert (2015) that investigated the effect of meditation and the biofeedback training program on the stress levels of people with diabetes found an applicable Cohen’s effect size (f=0.33), which was a median level [74]. With this effect size, the researcher calculated the sample size by using G*Power 3.1.5 in order to obtain a sample size of 92 subjects. Since three sample groups were required, 31 subjects were placed in each group. Additionally, the researcher increased the size of the sample group by ten percent in order to compensate for sample attrition during the study. Hence, the total sample size was 102 subjects divided into three groups of 34 subjects each. For this study, it was found that the effect size of stress was 0.517 and that the effect size of depression was 0.353.
2.2. Hypothesis
The mean scores on stress and depression are significantly lower in a group combining meditation with the biofeedback group those in a meditation-only group at six weeks after completion of the intervention.
2.3. Data Collection
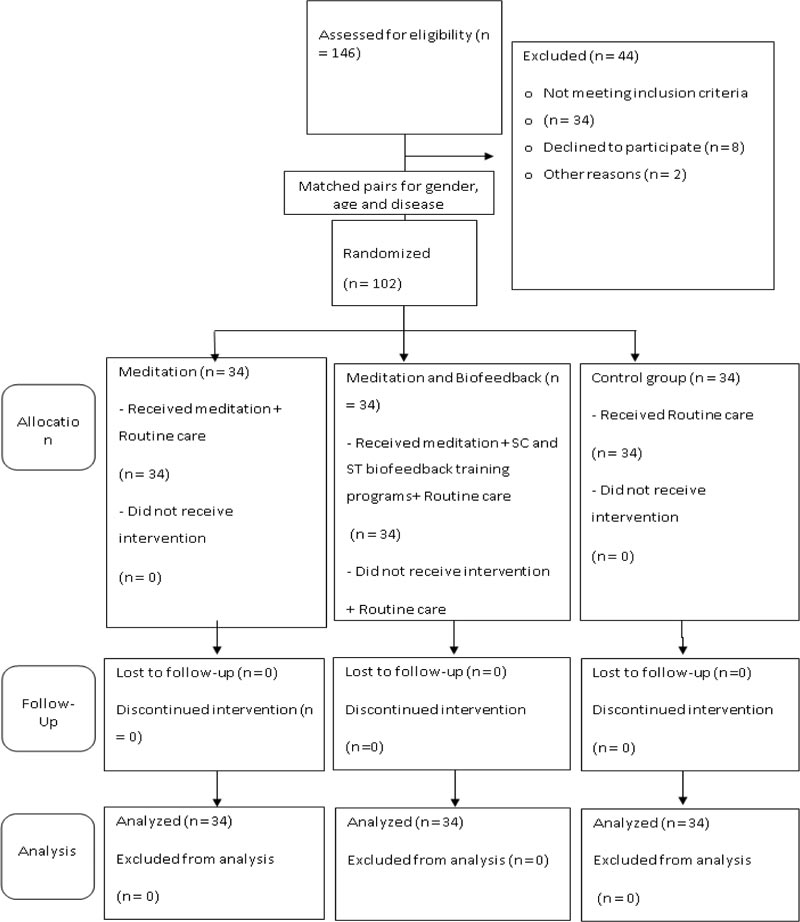
The CONSORT flow diagram describes the progression of the randomized experiment tracking the experimental and control groups. It was conducted in the following three stages.

2.3.1. Enrollment
The sample group was recruited from the target population at the General Practice Outpatient Department, TUH, by using simple random sampling, which consisted of drawing lots to obtain subjects for participation. The researcher selected subjects based on a set of characteristics and inclusion criteria with the purpose of obtaining 102 subjects for participation in the research project in line with the calculated sample size. Additionally, the subjects were also selected according to their levels of depression (with the mild level, as measured by BDI, taken to be within a scoring range of 10-15 points). The subjects were then matched in pairs in three sample groups of 34 subjects per group, as based on similar characteristics of sex, age, and disease.
2.3.2. Random Assignment
The participants were randomly assigned to a three-arm randomized controlled trial by using simple random sampling by the lottery method (random assignment) as follows: 1) meditation and routine nursing care (n = 34); 2) combined meditation with biofeedback and routine nursing care (n = 34); and 3) a control group receiving routine care only (n = 34). By employing a randomized block design, the research was able to ensure a directed random assignment to the treatment groups (two intervention groups and one control group) in equal numbers. This research was identified as a blind experiment since the participants received no information describing the experiment.
2.3.3. Follow-up
All three sample groups were subjected to the experiment together every week for six weeks. The CONSORT flow diagram regarding the effect of combining meditation with the biofeedback training programs on the stress and depression of people with diabetes is shown in Fig. (2).
2.4. Data Analysis
Data were analyzed using frequency, percentage, mean, standard deviation, MANOVA, and MANCOVA.
2.5. Measurements
The protection of rights of the study subjects was established as follows. Consideration of the Research Ethics Committee: The researcher presented the research proposal for consideration by the Ethical Review Sub-Committee Board for Human Research Involving Sciences, Thammasat University, No. 3 (project code number: 094/2561) and the Human Research Ethics Committee of Thammasat University Hospital, Thammasat University. This study was approved on January 7, 2019.
3. RESULTS
3.1. Primary Data
The samples included three groups of respondents, 34 persons each, consisting of experimental group 1, experimental group 2, and the control group. The subjects were selected in pairs based on identical profiles in terms of age, age, and disease. The mean age of all three groups was 59.5 (SD = 9.7). In all three groups of diabetic people, over half were female (61.8%), with most participants (41.9%) falling into the 56-65 year age group with equal percentages of the sample having diabetes (47.6%) and diabetes with hypertension (47.6%). About 76.5% of the people had been sick for five years or less, while 71.6% had been sick for longer than ten years. When using the chi-squared test, the findings showed that sex, age, level of education, marital status, monthly household income, income sufficiency, occupation, and medical rights and symptom diagnoses did not have a statistically significant level of 0.05. This finding demonstrates that the characteristics of the primary data of the meditation group, the meditation and biofeedback group, and the control group were equal and suitable for testing in the next statistical test, as shown in Table 1.
| Personal Data | Meditation |
Meditation with Biofeedback |
Control | Total | Chi-Square | ||||||||
| Value | df | p | |||||||||||
| n | % | n | % | N | % | n | % | ||||||
| Gender | Male | 13 | 38.24 | 13 | 38.24 | 13 | 38.24 | 39 | 38.24 | 3.99 | 2 | 0.13 | |
| Female | 21 | 61.76 | 21 | 61.76 | 21 | 61.76 | 63 | 61.76 | |||||
| Total | 34 | 100 | 34 | 100 | 34 | 100 | 102 | 100 | |||||
| Age (years) | Under 45 | 5 | 14.71 | 5 | 14.71 | 5 | 14.71 | 15 | 14.71 | 8.34 | 8 | 0.40 | |
| 46 – 55 | 5 | 14.71 | 5 | 14.71 | 5 | 14.71 | 15 | 14.71 | |||||
| 56 – 65 | 14 | 41.18 | 14 | 41.18 | 14 | 41.18 | 42 | 41.18 | |||||
| 66 – 75 | 10 | 29.41 | 10 | 29.41 | 10 | 29.41 | 30 | 29.41 | |||||
| Mean (SD) | 59.27 (10.51) | 58.18 (10.25) | 61.03 (8.30) | 59.49 (9.69) | |||||||||
| Total | 34 | 100 | 34 | 100 | 34 | 100 | 102 | 100 | |||||
| Educational level | No formal education | 3 | 8.82 | 2 | 5.88 | 0 | 0.00 | 5 | 4.90 | 13.09 | 10 | 0.22 | |
| Primary school | 12 | 35.29 | 10 | 29.41 | 19 | 55.88 | 41 | 40.20 | |||||
| Secondary school | 3 | 8.82 | 5 | 14.71 | 1 | 2.94 | 9 | 8.82 | |||||
| High school, Vocational certificate | 4 | 11.76 | 8 | 23.53 | 4 | 11.76 | 16 | 15.69 | |||||
| High vocational certificate, Diploma | 4 | 11.76 | 3 | 8.82 | 1 | 2.94 | 8 | 7.84 | |||||
| Bachelor’s degree, Master’s Degree | 8 | 23.53 | 6 | 17.65 | 9 | 26.47 | 23 | 22.55 | |||||
| Total | 34 | 100 | 34 | 100 | 34 | 100 | 102 | 100 | |||||
| Marital Status | Single | 3 | 8.82 | 4 | 11.76 | 3 | 8.82 | 10 | 9.80 | 2.89 | 8 | 0.94 | |
| Married | 26 | 76.47 | 25 | 73.53 | 26 | 76.47 | 77 | 75.49 | |||||
| Widowed | 2 | 5.88 | 4 | 11.76 | 3 | 8.82 | 9 | 8.82 | |||||
| Divorced | 1 | 2.94 | 1 | 2.94 | 1 | 2.94 | 3 | 2.94 | |||||
| Separated | 2 | 5.88 | 0 | 0.00 | 1 | 2.94 | 3 | 2.94 | |||||
| Total | 34 | 100 | 34 | 100 | 34 | 100 | 102 | 100 | |||||
| Household Monthly Income (Baht) |
Under 10,000 | 16 | 47.06 | 13 | 38.24 | 12 | 35.29 | 41 | 40.20 | 1.06 | 2 | 0.59 | |
| Over 10,000 | 18 | 52.94 | 21 | 61.76 | 22 | 64.71 | 61 | 59.80 | |||||
| Total | 34 | 100 | 34 | 100 | 34 | 100 | 102 | 100 | |||||
| Income Sufficiency | Sufficient | 16 | 47.06 | 13 | 38.24 | 12 | 35.29 | 41 | 40.20 | 1.06 | 2 | 0.59 | |
| Insufficient | 18 | 52.94 | 21 | 61.76 | 22 | 64.71 | 61 | 59.80 | |||||
| Total | 34 | 100 | 34 | 100 | 34 | 100 | 102 | 100 | |||||
| Occupation | Unemployed | 10 | 29.41 | 5 | 14.71 | 5 | 14.71 | 20 | 19.61 | 11.29 | 8 | 0.19 | |
| Government/state enterprise employee | 14 | 41.18 | 14 | 41.18 | 13 | 38.24 | 41 | 40.20 | |||||
| Self-employed/private company employee | 2 | 5.88 | 6 | 17.65 | 7 | 20.59 | 15 | 14.71 | |||||
| Merchant/business owner | 7 | 20.59 | 8 | 23.53 | 4 | 11.76 | 19 | 18.63 | |||||
| Agriculturist | 1 | 2.94 | 1 | 2.94 | 5 | 14.71 | 7 | 6.86 | |||||
| Total | 34 | 100 | 34 | 100 | 34 | 100 | 102 | 100 | |||||
| Rights to medical care | At their own expense | 5 | 14.71 | 5 | 14.71 | 3 | 8.82 | 13 | 11.76 | 4.46 | 6 | 0.61 | >|
| Claimable medical fee | 21 | 61.76 | 19 | 55.88 | 26 | 76.47 | 66 | 64.71 | |||||
| Universal coverage ID card | 3 | 8.82 | 2 | 5.88 | 2 | 5.88 | 7 | 6.86 | |||||
| Social Security | 5 | 14.71 | 8 | 23.53 | 3 | 8.82 | 16 | 15.69 | |||||
| Total | 34 | 100 | 34 | 100 | 34 | 100 | 102 | 100 | |||||
| Comorbidity | Diabetes | 16 | 47.06 | 16 | 47.06 | 16 | 47.06 | 48 | 47.06 | 6.03 | 6 | 0.41 | |
| Diabetes and ischemic heart disease | 1 | 2.94 | 1 | 2.94 | 1 | 2.94 | 3 | 2.94 | |||||
| Diabetes and hypertension | 16 | 47.06 | 16 | 47.06 | 16 | 47.06 | 48 | 47.06 | |||||
| Diabetes, ischemic heart disease and hypertension | 1 | 2.94 | 1 | 2.94 | 1 | 2.94 | 3 | 2.94 | |||||
| Total | 34 | 100 | 34 | 100 | 34 | 100 | 102 | 100 | |||||
3.2. The Findings Supported the Research Hypothesis
In this section, the methods for testing the hypothesis are described.
| Testing Group | n | Stress | Depression | ||
| M | SD | M | SD | ||
| Control | 34 | 2.52 | 0.13 | 0.64 | 0.08 |
| Meditation | 34 | 2.16 | 0.25 | 0.58 | 0.07 |
| Meditation and biofeedback | 34 | 2.04 | 0.20 | 0.53 | 0.04 |
Bartlett's test: approx. chi-square = 28.14, df =1, p = 0.00
Levene's test: Stress F = 1.41, df1 = 2, df2 = 99, p = 0.25; Depression F = 1.60, df1 = 2, df2 = 99, p = 0.21
3.2.1. Comparison between Post-test Stress and Depression by Group
Multivariate analysis of covariance was applied in order to compare the mean differences of the post-test stress and depression in the different groups. It was found that the mean scores for each pre-test group were different with a statistical significance. Thus, the test enabled the control of the covariate, and it was found that the variance-covariance matrix of variables of each group was different with a statistical significance at a level of 0.05 (Box's M = 35.81, F = 5.79, df1 = 6, df2 = 244271, p = 0.00). When considering the correlation of dependent variables, it was found that both post-test variables had a statistically significant correlation at the level of 0.05 (approx. chi-squared = 28.14, df = 1, p = 0.00). The results thus showed that both variables were suitable for the MANCOVA, as shown in Table 2.
Based on the results of the MANCOVA, carried out by using the pre-test score as a covariate, it was found that the mean vectors of the post-test stress and depression of the post-test groups were different with a statistical significance at a level of 0.05. When analyzing variance by variables and comparison of paired means, it was found that stress and depression were different between the groups with statistical significance at a level of 0.05 (Pillai's trace = 0.31, p = 0.00). When considering the control group, the mean of stress and depression was higher than in the other groups. For the meditation group, the mean of stress and depression was higher than in the meditation and biofeedback group, with statistical significance at a level of 0.05. The findings are presented in Table 3.
| Pillai’s trace | F | Hypothesis df | Error df | p | ||
| Pre-test stress | 0.89 | 402.00 | 2 | 96 | 0.00 | |
| Post-test depression | 0.17 | 10.03 | 2 | 96 | 0.00 | |
| Testing group | 0.31 | 8.88 | 4 | 194 | 0.00 | |
| Analysis of between-subjects’ effects | ||||||
| Source | Dependent Variable | Type III SS | df | MS | F | p |
| Pre-test stress |
Post-test stress | 3.42 | 1 | 3.42 | 803.71 | 0.00 |
| Post-test depression | 0.00 | 1 | 0.00 | 0.31 | 0.58 | |
| Between-subjects effects Analysis | ||||||
| Source | Dependent Variable | Type III SS | df | MS | F | p |
| Pre-test depression | Post-test stress | 0.00 | 1 | 0.00 | 0.10 | 0.76 |
| Post-test depression | 0.06 | 1 | 0.06 | 19.53 | 0.00 | |
| Testing group | Post-test stress | 0.10 | 2 | 0.05 | 12.04 | 0.00 |
| Post-test depression | 0.08 | 2 | 0.04 | 12.05 | 0.00 | |
| Tests of between-subjects effects | ||||||
| Source | Dependent Variable | Type III SS | df | MS | F | p |
| Error | Post-test stress | 0.41 | 97 | 0.00 | - | |
| Post-test depression | 0.32 | 97 | 0.00 | |||
| Corrected total | Post-test stress | 8.11 | 101 | - | ||
| Post-test depression | 0.60 | 101 | ||||
3.3. Validity and Reliability
The research methodologies were validated by five qualified experts who examined the content validity of the questionnaire in order to gather demographic information, the home meditation form and the meditation training, together with the SC and ST biofeedback training programs. The known-group technique was used to measure the concurrent validity of the SC and ST biofeedback machines by applying the method with five diabetic people. Their profiles were identical to the target sample. The SOSI and BDI were used to measure reliability by applying the method with 30 diabetic people whose profiles were similar to the target samples. The results were then calculated in order to measure the validity of the research tools by using Cronbach’s alpha coefficient method. The reliability of the SOSI was 0.944, and the reliability of the BDI was 0.732. The pre-use calibration of the SC and ST biofeedback instruments using GSR connected to the signaling apparatus with needles was done by adjusting the needle to zero for each calibration.
3.4. Research Limitations
The study aimed to study the effects of combined meditation with a biofeedback training program on stress and depression among people with diabetes. The findings showed that these programs could significantly alleviate stress and depression. Concerning the limitations regarding combined meditation with biofeedback, the researcher did not control the treatment of the people at home. Those people had to be treated appropriately by using SC and ST biofeedback for six weeks in order to ensure that they could control their stress without using the tools. This treatment allows people to apply stress alleviation techniques from meditation in order to minimize the stress in their daily lives effectively.
4. DISCUSSION
4.1. Discussion of the Findings from the Hypothesis Testing
In this study, meditation training, together with the SC and ST biofeedback training programs, was conducted following the research hypothesis. The people with diabetes in the combined meditation-with-biofeedback group were found to have significantly lower mean scores on stress and depression than the people in the meditation group at six weeks after completion of the intervention. The findings supported the research hypothesis.
The people who received meditation training participated in the meditation program for six weeks with the researcher weekly for 90 minutes, with daily practice at home for at least 20 minutes. This training caused the people to relax, thereby resulting in psycho-physiological changes. The people who trained themselves to control their stress by using biofeedback together with meditation perceived physical changes in their relaxation levels during meditation every week. The biofeedback instruments showed measurements as number scales on the GSR display. In biofeedback, people can observe these displayed values in order to familiarize themselves with the sensations correlated with physical functions. Thus, biofeedback, together with meditation, helped the people to control certain physical functions with the aim of achieving deep relaxation [38, 54, 69, 71, 75].
It can be explained that the complications and effects from DM are factors that potentially cause DM people to experience stress and depression [76-80]. Typically, depression is triggered by the perceptions of people that encounter stressful situations, and depression is triggered when a person persists in negative thinking, with perceptions and feelings about himself or herself and his or her environment over a long period of time, thereby causing distorted ideas of reality. The unfortunate results are negative thoughts and perceptions about themselves, the future, and their surrounding environment [81]. Being negative and having a lack of mindfulness are the most common types of thought patterns found in people with depression. They imagine that their environment is causing them to suffer, and this perception on their part leads to stress. Daily TM practice for six weeks can improve the psychological effects of people with diabetes. As the practitioners concentrate during TM, their awareness becomes acute in a state of restful alertness, referred to as transcendental consciousness [32, 36, 38, 82].
TM allows people to be aware of the present moment, and to recognize, understand, accept, and let go of the distress that has occurred within themselves rather than trying to change and challenge what has happened [32, 36, 38, 82]. TM can train the practitioner to control his or her mind for heightened awareness and accepting without judgment stressful events or conditions. TM enables people to separate their thoughts and reality and to recognize the changes that happen when having their thoughts until such thoughts are gone. After practice, the people will become more peaceful and manage their negative thoughts better. Their mind will become peaceful and become self-aware until the stress is decreased [32, 36, 38, 82]. Further, awareness allows for good emotional health and mitigates anger, antisocial behaviors, and stress and depression as well [26, 32, 36, 41, 83].
TM not only allows people to have less stress and depression, but it also enables them to control their lives and develop their flexibility when they have to face any crisis in the future. Further, TM allows people to face and resolve their problems systematically and effectively. According to Maharishi, the TM process involves an extension of consciousness while tapping both creative energy and intelligence. Put simply; meditation can train the practitioner to control his/her mind in order to minimize his/her anxiety with a coping mechanism producing a calm and non-destructive reaction to stressful events. In this way, TM can employ meditative skills to facilitate detachment from anxiety, which is commonly found together with major depressive disorders. Consequently, people will receive good results and have less stress and depression [25, 32, 36, 41, 70, 76, 84-86].
Additionally, TM enables people to consider cause-and-effect relationships better. The reasoning involves a mental mechanism that allows people to accept the reality that they have encountered so that they will try to eliminate their grief and create peace in their minds through meditation. Individuals with depressive-disorder tend to lack the ability to think thoroughly and systematically, resulting in difficulties with problem-solving, even when dealing with just small issues. Some people feel desperate in their efforts to find ways to solve problems. In a study conducted among DM people, their findings revealed that most DM people with depression tended to be those who had problems in life and were unable to solve their problems [32]. On the other hand, TM develops self-confidence, the power of tolerance, clear thinking, and greater power of thought. Additionally, people can apply TM to learn how to react appropriately to the situations they are facing. Learning to become free from distress is considered a form of mental development in its own right.
Furthermore, a lack of social skills and interpersonal skills is associated with depression. It has been reported that people with DM with depression feel disappointed with themselves and do not feel enjoyment or satisfaction with their personal situations or surrounding environment, such as family, friends, work, and activities [32, 76, 82]. Meditation, on the other hand, makes the mind alert and comprehensive, as both the cognitive and physical activities of a person are then able to improve that person’s self and others that come in contact with that person. Furthermore, meditation increases creativity and intelligence, self-confidence, self-esteem, and self-assertiveness and internal control. Thus, meditation boosts the social skills of people such that their depression will inevitably decrease or dissipate altogether [32, 36, 38, 41]. The findings of this research concur with the work performed by Armani Kian and colleagues, in which they took up a study of people with type 2 diabetes. In that study, the experiment was conducted over eight sessions of meditation; and it turned out that meditation effectively lowered the depression scores with a statistical significance (p < 0.05) after the administration of the program [87].
When people practice TM, their bodies achieve a condition marked by deep relaxation, in which fatigue and stress are eliminated, and brain function is orderly. Meditation practice thus allows the body to experience deep and full rest, resulting in physical stress relief. Meditation helps the parasympathetic nervous system to achieve balance so that ultimately the patient's mind will calm down and will be free from stress [26, 32, 38]. Consequently, their bodies tend to secrete adrenaline more and noradrenaline less, making their minds feel comfortable [32, 73, 88]. As a person meditates, breathing becomes shallower, the heart rate slows, and the cardiovascular system achieves a state of intense rest. Levels of various chemical indicators of stress, such as blood lactate and cortisol, become significantly reduced [26, 37, 38]. Moreover, meditation decreases other emotional responses, such as fear, anger, sadness, and a whole host of other negative states of mind.
Additionally, meditation affects brain functioning. It has been found that there are changes in the limbic system, which is the emotional control center of the body. Meditation causes changes in one's feelings, and such changes will be recorded in the emotional control system later, and then be forwarded to the hypothalamus. Additionally, meditation practice results in better functioning of the left hemisphere and more positive emotional development. Moreover, meditation generates and sends alpha waves to the brain, resulting in increased secretion of endorphins, a substance that lets the body and mind stay relaxed. These changes all lead to lowered levels of stress and depression [32, 73, 88]. These changes concur with the work of Sasikumar and Fathima (2017), who found that people with type 2 diabetes who participated in a meditation program were satisfied with this method of relieving stress. They also found that meditation effectively lowered stress and depression scores with statistical significance (p<0.05) after the intervention (p<0.000). Thus, their study showed that meditation is a program capable of reducing depression symptoms [89]. Their findings are in agreement with a study conducted by Whitebird and colleagues, who investigated diabetes distress in people with diabetes mellitus after receiving a meditation program. This study indicated a significant improvement in the stress and depression levels of diabetes patients who had undergone meditation [90].
When people are trained to control their stress by using biofeedback with meditation by completing the 6-week program, they are then able to perceive the level of their stress and know how to control or mitigate it. The score appearing on the GSR screen is an indicator of the patient's physical reaction to stress while participating in this program. The people will become proficient in fine-tuning their stress and be able to control the stress of their daily lives on their own continually and with no further use of biofeedback. When people find that they have to deal with an uncomfortable situation, they will automatically realize the nature of their stress and be able to apply the stress-relief techniques from the practice in order to manage their stress properly and learn how to resolve the collective stress in their bodies and minds appropriately [58, 73, 91].
The meditation and biofeedback program uses the biofeedback device for weekly monitoring of sweat glands and ST for a period of six weeks, together with practice at home for at least 20 minutes per day. The program, therefore, drives people to learn from their training to the point that they eventually become familiar with the practice. They receive positive reinforcement from their positive behavior, generated by coherent emotions and thoughts, such that they reinforce each other. This practice allows people to learn and adapt their thoughts, perceptions, and feelings, and to behave properly. The result is a state of peacefulness, relaxation, and freedom from stress and depression [32, 38, 82]. These findings agree with the results of a study by Thongkhum, Ruchiwit, and Somprasert (2015), who found that meditation with biofeedback was capable of relieving stress in people more effectively than by meditation alone. The positive feeling that people derived from effective relaxation training, as indicated from the displays of their physical changes via the biofeedback instrument, gave these people the strength they needed to practice relaxation. Consequently, they were fully able to continue to reduce their stress loads [56, 64, 91]. In addition, the meditation and biofeedback program provided alternatives that allowed people to handle their stress and depression by creating their inner peace and self-control.
CONCLUSION
The research findings demonstrate the effectiveness of combined meditation with a biofeedback program in reducing stress and depression after the program was administered. In this study, the researcher advised and encouraged people in their practice from the first to the last week. Most of the people reported feeling relaxed, comforted, having eliminated their negative emotions, and rested from sleep, causing them to have enthusiasm in attending group activities every time. This finding concurred with the observation from the researche which found that the people who participated in the project were satisfied with this method of relieving stress. Combined meditation with biofeedback for the weekly monitoring of sweat glands and skin temperature for six weeks, together with practicing meditation at home for at least 20 minutes a day, made people learn from their practice until they became familiar with the practice. Moreover, they received positive reinforcement from their positive behavior caused by coherent emotions and thoughts. This practice allowed the individuals to learn and adapt their thoughts, perceptions, feelings, and behave properly, resulting in peacefulness, relaxation, and freedom from stress and depression [32, 38, 82].
The research findings should be applied in order to promote good health for the public and to improve the sustainability of solutions for mentally ill patients in Thailand’s mental health system: 1) lower the incidence of mental disorders, including stress and depression; 2) develop quality mental health services; 3) promote healthy lifestyles in order to increase self-regulation skills to cope with stress and depression disorders; 4) increase the ability to identify cognitive distortions and sensibly appraise stressors; 5) educate people about methods for reducing stress and depression at the individual, family, and community levels; and 6) provide health providers with mental health knowledge with the aim of improving mental health care provision at the individual and family levels, while steering clear of preventable hospital admissions for mentally ill individuals.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The data collection in this study was conducted following the approval of the IRB of Thammasat University, Thailand (the Ethical Review Sub-Committee Board for Human Research Involving Sciences, Thammasat University, No. 3) on June 10, 2019 (Approval Number 094/2561) regarding the research settings.
HUMAN AND ANIMAL RIGHTS
No Animals were used in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Informed consent was obtained from all the participants.
AVAILABILITY OF DATA AND MATERIALS
The data that support the findings of this study will be made available from the corresponding author [O.P] on request.
FUNDING
Research refunding was provided by Thammasat University Hospital (project code number: 1128/2561).
CONFLICT OF INTEREST
There was no conflict of interest in carrying out the present study.
ACKNOWLEDGEMENTS
The authors gratefully acknowledge the research fund provided by TUH.

