All published articles of this journal are available on ScienceDirect.

Participatory Development in Community Health for the Pgazkoenyau Ethnic: A Case Study in an Ethnic Community in Thailand
Authors Info & Affiliations
Abstract
Background:
Most ethnic communities in Thailand were settled in remote areas with poor living conditions. Therefore, the “human-centered” concept was adopted to develop community health using the participation process.
Objective:
This research aimed to develop community health using the participation process at two Pgazkoenyau ethnic (Karen) communities whose environmental contexts were similar, in Tha Song Yang and Mae Ra Mard District, Tak Province.
Methods:
The multi-stage mixed methods design was applied for data collection. 24 participants were purposely recruited in the qualitative approach due to their responsibility as community health development operators. Qualitative data were collected using semi-structured interviews and analyzed using content analysis. In addition, quantitative data were gained through interview forms and laboratory test reports. Then they were analyzed using descriptive statistics, t-test to compare mean behavioral variables, and z-test to compare the proportion of two communicable diseases and blood chemical residues, with 95% confident interval.
Results:
The development process consisted of problem finding, data feedback and community stage, capacity building, operation, creative meeting, networking and social capitalizing. They could manage all activities following the community plan: identify helminthiasis and malaria cases, introduce cholinesterase test kits, improve community environmental health, improve healthy behaviors and build capacity for health promotion skills. Evaluated community activities showed increased scores concerning knowledge, attitudes and practices about disease prevention. The prevalence rate of helminths infection decreased significantly. The environmental context was also improved to enable the population’s healthy living conditions.
Conclusion:
Community development should be based on community resources and all available social and human capital for sustainable development.
1. INTRODUCTION
“Development” is a process from unsatisfying conditions to a more satisfying state, involving a dynamic process [ 1]. Development is directly related to change. It means a process of changes which have been planned. These planned changes hypothesize that the new conditions will be better than the old ones. However, changes sometimes have problems naturally that more or less will depend on each context. Development can be defined based on two aspects, modern perception and religion. Firstly, the modern perception views development as materialized growth in terms of both format and quantity, such as roads and transportation, housing construction and economic indexes. Secondly, according to the Buddhist point of view [2], development means the growth of body and mind. It emphasizes quality of life, correctness and sufficiency and maximizes utility, cohesiveness and beneficence, without destroying nature and the environment.
“Local community” is a human habitat connected to geographic conditions and social relationship systems, supporting human life [3]. Attachment and interaction, among others, create a process for maintaining peaceful lives. It constitutes a primary unit for both self-reliance and dependence, related to social mobilizing processes. The community is a valuable psycho-cultural unit representing its identity concerning ideology, rights and management power [4].
The dynamics of economics and technology have changed policy and country development trends, resulting in health development guidelines in Thailand. Disease control and prevention policy focus on non-communicable diseases, while communicable diseases, an indicator for underdeveloped countries, have been neglected. However, rapid development creates big gaps in health accessibility between urban and rural areas and rich and poor populations. The health of vulnerable groups, such as the poor and minorities, remain specific issues needing attention. To address these problems, tailor-made solutions are crucial. The management process has to integrate, synchronize and remain consistent with local lifestyle, as well as consider community participation processes [5, 6]. Disease control capacity development in a community involves health learning processeswhose tools include communication and community health education to create community participation in disease control. Its goals are harmonized, peaceful and focused on creating a healthy community. Then management mechanisms for community development require a whole community social system consisting of public partners, local governors, private partners and civil society. The dominant working body comprises local governors, whereas the beneficiary will be the civil society. In conclusion, community development involves everyone’s responsibility to participate in every step of the process, including design, plan, implementation and evaluation, to share common benefits.
Community well-being development is a process to improve community well-being conditions in all aspects, including economic, societal, political, and environmental, to address the dynamics of globalization, and advance self-reliance [7]. By this, communities will be able to solve their problems and fulfil their needs by themselves. The target of community development is “people” varied and distributed around the country, in many forms such as villages, urban cities, occupational groups or even some specific activity groups, etc. These groups form the foundation of the country; as a consequence developing these groups leads to developing the country.
The Pgazkoenyau ethnic group (Karen) comprises border seam line inhabitants between western Thailand and Burma, in Tak Province. Their communities are located in remote rural areas and face many difficulties in terms of transportation and amenities. They cannot access equitable educational, economic and health opportunities [8]. This impacts their quality of life and well-being conditions. Her Royal Highness Princess Maha Chakri Sirindhorn has expressed an understanding concerning the quality of life of children, youth and populations in remote rural areas [9]. Therefore, most of her works emphasized developing remote rural areas. These programs and activities focus on developing community potential, at the same time avoiding changes in culture and local way of life [10]. She has included these ethnic communities in her royally initiated projects. These projects emphasize developing human capital according to the National Economic and Social Development Plan, starting from the 8th plan until now. Especially the 9th to11th National Economic and Social Development Plans promoted social immunity in Thai society by promoting literacy. The importance of developing human capital and sustainable society is prominent in the 12th National Economic and Social Development Plan, incorporating the sufficiency economy philosophy and Sustainable Development Goals using a people-centered approach [11]. Because the focus remains on the community, every related stakeholder should seriously cooperate in the development process. To achieve country and society targets, each individual and community has to be developed. This means the targets of every royally initiated project are not only to improve people’s quality of life in remote rural areas but also to maximize human resource capacity. Thus, community harmony constitutes the key to fulfilling people’s and community members’ happiness. This study aimed to (1) explore the well-being development processes in the community and (2) investigate the results of well-being development processes in the community under the royally initiated projects of Her Royal Highness Princess Maha Chakri Sirindhorn. This constituted a case study from Tak Province.
2. MATERIALS AND METHODS
Research and development built a multi-stage community health development project. Its foundation was based on Deming’s Cycle concept [12]. The data were collected using mixed methods technique, as shown in Table 1.
2.1. Study Site
Communities included the Mae Fah Luang Mountain Thai Community Learning Center (NESDB) Baan Tee Sa Nhor, Mae WaLaung Subdistrict, Tha Song Yang District, and Baan Huai Hang, KaNaeJuae Subdistrict, Mae Ra Maad District, Tak Province. These isolated villages are in the national park along the Thai-Myanmar border and far from urban civilization, amenities and health services. Both are Pgazkoenyau ethnic (Karen) communities that constitute a monoculture with their language for daily life communication. Because their villages are located in remote areas, they live in a primitive way using seasonal farming and hunting for a living. Very few people migrate to work outside the villages. Most importantly, these two targeted villages have similar environmental contexts.
2.2. Data Collection Qualitative Study
Descriptive phenomenal qualitative data were collected from 24 local team members from two networks who implemented this community health development project: 16 participants were implementing leaders, while 8 participants were academic supporters and learning process conductors. The data were collected using participatory observation, and field notes were used to record techniques and processes of the whole community development. In this study, the researchers served as an important tool. We fully participated in every activity of the development team in both targeted areas. The participants, both at the initial and during the later surveys, comprised the same group. Other related key informants were contacted to complete the data to achieve the study objectives. Snowballing was applied to purposively select these key informants. Telephone calls were used in cases where additional data were required. The researchers collected data until reaching the saturation point to ensure data richness. The research team regularly conducted creative meetings to share findings, reflect on the study situation and improve the quality of data collection throughout the data collection process. Validity of the data was tested using triangulation with a documentary search and informal interviews with other related health staff who were not local team members [13].
| Step According to Deming’s Cycle | Activity/Process | Data Collection |
|---|---|---|
| Plan | Workshops analyzing social capital of the community and its networks to construct integrated community development plans | Qualitative data were collected by participatory observation and documentary search. |
| Do | Each organization implements planned activities according to its mission, such as leaders’ capacity building and learning process construction for screening tests of: helminths, malarial fever, blood chemical residues and community environmental improvement. | Qualitative data were collected by participatory observation |
| Check | Evaluate activities/processes implemented by each organization | Data were collected using informal interviews and questionnaires concerning health behaviors, and laboratory tests. |
| Act | Analyze collected data, then tri-angulate and benchmark against the milestones to develop the improvement plan |
In participatory observation, the researchers joined these two networks as team members to observe the first-hand perspectives of the group and their activities. Instead of observing as outsiders, we played two roles at once, objective observer and subjective participants [14, 15]. To join each group, we received support from the public health officer, a gatekeeper of the group. This person introduced us to the group and helped us to gain their acceptance [16]. We built a trustworthy rapport among the group members to make them feel comfortable with our presence, and we improved our relationship to be sufficiently reliable to share sensitive information. We were completely open with the group members yet remained discreet [17]. When we participated, we took brief notes whenever we could, then elaborated on them after the activity was over [18].
2.3. Quantitative Study
Quantitative data were collected using questionnaires identifying villagers’ behaviors. The questionnaires, developed by the researchers, comprised three components, including knowledge relating to helminths and malaria, attitudes toward disease prevention and disease prevention behaviors. The content in the questionnaire was validated by three infield experts: family medicine, behavioral science and community public health using item-objective congruence (IOC). The IOC of each item was calculated by dividing the total scores by three. The remaining items consisted of every item whose average score was more than 0.5. Then the language clarity was checked by a community teacher with the same Karen ethnic. After that, it was pilot tested with 30 Karen hilltribe members residing in another community having the same characteristics as the study subjects [19]. Its reliability was confirmed using Cronbach’s alpha with a score of 0.7.
Concerning details of the questionnaire, the knowledge component comprised a checklist test of ten items with two choices: yes and no. The questions asked about communicable diseases; hosts, agents, environment and modes of transmission. Regarding the attitude part, a Likert scale [20, 21] was applied to measure attitudes, beliefs and values concerning helminthiasis and malaria and their related risk behaviors. The participants were asked to choose one of three rating scales, i.e., agree, undecided and disagree according to their opinion. These 12 attitude items included 6 positive and 6 negative statements. Lastly, the behavior section comprised three frequency rating scale checklists: never, sometime and always. Eight items explored the healthy behaviors for helminths and malaria prevention and control.
The population of this quantitative survey comprised community members aged more than ten years residing in the two targeted villages. The unit of analysis constituted one household. Totally, 192 subjects from the two villages were randomly selected. The random sampling process involved (1) all members initially, and then each member was marked with a specific number for each household and (2) from this population, researchers randomly chose subjects using random number tables. The number of subjects was selected considering sex and age ratio of the population. The details of the sample size by age group are shown in Table (2).
| Years | Village | Total Household | Sample Size by Age Group* | ||||
|---|---|---|---|---|---|---|---|
| <18 Years | 19-24 Years | 25-59 Years | >60 Years | Total | |||
| 2016 | I | 82 | 19 | 20 | 20 | 19 | 78 |
| II | 121 | 26 | 30 | 32 | 26 | 114 | |
| 2018 | I | 82 | 18 | 20 | 20 | 19 | 77 |
| II | 121 | 25 | 29 | 32 | 26 | 112 | |
Regarding collecting data among illiterates, high school students were trained by the researchers and their teachers to assist the participants. In addition, structured interviews were conducted in their own dialect, Karen. However, literate subjects could complete the questionnaire themselves. Data were collected using the same questionnaires in the same populations at the beginning of program development in October 2016 and the evaluation period in November 2018.
For testing, the medical science technicians with field parasite examination expertise in the investigating unit of Regional Disease Control II performed laboratory analysis using Kato’s thick smear technique [22, 23] to identify helminths infection in the populations or the two targeted sites. After that, these specimens were sent to the laboratory for confirmation tests using the Formalin Ether Concentration Technique [24, 25].
In addition, the staff from the Vector Borne Disease Control Center conducted malarial screening tests using malarial screening test kits. In case of positive detection, those specimens were sent to the advanced laboratory of the Regional Disease Control II to confirm by morphology diagnosis under a microscope and using real-time PCR.
Moreover, blood chemical residues were checked using cholinesterase test kits (serum test) detected and interpreted by medical science technicians from Regional Disease Control II.
Concerning the stool examination, malarial screening tests and blood chemical checks involved routine examination executed once annually among all community members residing in the remote areas under the royal project.
Inclusion criteria
1. Volunteer subjects, aged more than ten years and were residing in the village throughout the program intervention
2. Volunteer subjects, completing the surveys both in 2016 and 2018: questionnaires surveys, stool examination results, malarial screening test findings and blood test report.
2.4. Data Analysis
Quantitative data were analyzed using descriptive statistics such as percentage, average and standard deviation. The score of knowledge, attitudes, behaviours and latrine coverage before and after the invention was compared using t-test statistics to evaluate the success of the health program intervention operated in the community. The comparison of helminthiasis and blood chemical residual using z – test statistics with a p-value of 0.05 [26] was used to confirm the impact of the program intervention and any affected sustainable healthy behaviors.
Qualitative data analysis was performed following the principles of the method of thematic analysis [27]. The transcripts and notes were read and reread to identify initial semantic categories and registrars were coded using word occurrences. Categories were then proposed and revised as further data were collected and analyzed [28]. Content analysis was the core method used to ascertain meaning. Firstly, each researcher independently performed ones’ own content analysis. Then a panel discussion was held at the last stage to execute the final results of the study. To further increase the credibility and validity of the results, the researcher employed triangulation using evidence from different types of data sources, including documentary search and informal interviews with other related health staff who were not local team members. The triangulation process [13, 29, 30] combined multiple methods to gather data when conducting the primary research at different times and places.11 Lastly, triangulation theory used more than one theoretical approach or more than one construct model based on grounded theory techniques to interpret and support data [29].
3. RESULTS
3.1. Key Success Factors of the Community Well-Being Development Process
The community development focused on improving people’s and community members’ capacity, so they could manage their own resources/community social assets to help themselves [31]. The concept of this development process involved a people-centred approach. This meant the development process was initiated by people recognizing their own problems and understanding them using their own perceptions. Then they worked cooperatively to solve these identified problems. The external development team would stimulate and support community members and their leaders to maximize their own capacity. Consequent development activities are described below.
3.1.1. Identifying Community Problems
Identifying community health problems could be categorized into two components. The first part involved reflecting on health problems using numerical data, statistics and health databases. These data were provided by health service systems, especially primary care services within the community. We could collect these secondary data from reports and conduct surveys to obtain primary data. The second section involved health problems reflected by the population and community members. These data comprised people’s perceptions. These included physical illnesses and health conditions perceived through their experiences. The development team members were not concerned with only biomedical conditions, but the developers understood the meaning and definition of health and illness in the sense of holistic community practices.
3.1.2. Conducting Data Reflection and Public Hearing Forums
The most important activity in community development was conducting public hearing forums. This constituted the most significant social tool to drive development processes based on community participation concepts [32]. Public hearing processes involves reflecting borderless opinions, feelings and thoughts. It freely allows discussion and information sharing of specific public concerns. No fixed formal patterns of public hearing approaches were employed. Based on deliberative democracy and health literacy concepts, public hearing processes needed adapting and applying according to each target, to permit community members to maximize their learning capacity. Deliberative democracy could not be emphasized in health condition development among ethnic communities not possessing sufficient confidence to comment or share their perceived feelings and thoughts. As a result, the development process could integrate learnings of health, democracy, community development and the sharing process could stimulate the moderators and organizers of the meetings.
3.1.3. Building Capacity
“People-centered” development and sustainable development constitute capacity building processes for community members, especially empowering community leaders [33]. Consequently, they could use their highest competencies, with support from government organizations and staff in terms of processes, opinions, guidelines and empowerment strategies. In this study, capacity building is meant to inspire and educate key individuals in community development processes, so they could design and implement their own community development activities. Particularly, this capacity building process was crucial for ethnic communities because of being context specific in terms of language, culture and traditions. The key success factor was the participation of “local people” [34] as leaders on the development team, especially communication for behavioral health changes.
3.1.4. Implementing
Public hearing processes were employed to allow community members to design their own community development activities according to their perceived needs and also congruent with local health facility plans to solve health and environmental problems. All related stakeholders should cooperate in implementing the aforementioned community development plans following Deming’s Cycle [12]. Their steps comprised planning, implementing, evaluating and identifying improvement plans (PDCA Cycle). Importantly, these development activities should not affect the community’s lifestyle, yet they constituted only changes in practices according to community contexts and culture.
3.1.5. Conducting Creative Meetings
This kind of meeting focused on borderless and informal sharing among community members. To identify acceptable solutions based on democratic concepts, everyone could participate freely; every thought and opinion was valued, and all members were respected and treated as equals. Thus, creative meetings contributed to inventive and feasible development activities, which all members designed together. The members agreed to implement the designed development activities to achieve the same targets without reducing any human value.
3.1.6. Fundraising and Networking
To develop an ethnic community, fundraising proved a crucial activity to be culturally rich, but monetarily poor. In this study, “funds” covered all resources: man, money and material (3Ms) for community development processes. This comprised one key success factor of community development [31]. The existing community’s capital and network co-operation also drove the community development processes toward their expected direction. The aforementioned fundraising not only gathered financial resources and materials, but also human resources, important for building community capacity. Human resources were not only supporters but also contributors to learning processes between the external staff and internal population when executing planned activities. Within the three years of this study, community health development processes could be summarized as shown in Table 2.
| 1st Year | 2nd Year | 3rd Year |
|---|---|---|
| Network meeting | Network meeting | Network meeting |
| Study community context | Design development activities | Design development activities |
| Construct knowledge | Construct knowledge | Implement plan |
| Analyze problems and needs | Implementation plan | Advocate policy |
| Design development activities | Advocate policy | Evaluate |
| Network | Conclude/assess and summarize learnings from activities. | |
| Implement plan | ||
| Conclude and summarize learnings from activities |
3.2. Key Performance Index of Development Results
The target of ethnic community development was the well-being of the people in the community. This study concerned quantitative indicators and impacts of community development according to children and youth regarding remote rural area development plans. Regarding the Disease Control Department’s responsibility, the two main variables included prevalence rate of malaria and helminths infection. Then they were adopted to be community development indicators. The intervention was to improve health behaviors by developing health communication and managing the community environment. The environmental development could be observed through changes in community contexts and the existing community development activity/project plans and implementation (Table 3).
3.2.1. Health Behavior Improvement According to Self-Prevention and Control in Communicable Diseases
Table 4 provides the subjects’ health behavioral data collected, analyzed and compared between 2016 and 2018. The result showed significantly improved communicable -disease-related knowledge and attitudes toward disease prevention and disease preventing behaviors. Communicable disease-related knowledge scores increased by 3.45 points on average (t 3.25, p-value 0.001). Attitudes toward disease prevention scores increased by 6.45 points on average (t 2.94, p-value 0.001). Moreover, disease preventing behavior scores increased 2.72 points on average (t 1.87, p-value 0.05).
| Variable | Year | n* | Mean score/S.D. | t-test | P-value |
|---|---|---|---|---|---|
| Knowledge | 2016 | 192 | 4.68/3.51 | t=3.25 | P=0.001 |
| 2018 | 189 | 8.13/2.67 | |||
| Attitude | 2016 | 192 | 18.67/7.34 | t=2.94 | P=0.001 |
| 2018 | 189 | 25.12/3.08 | |||
| Practice | 2016 | 192 | 3.15/2.93 | t=1.87 | P=0.05 |
| 2018 | 189 | 5.87/0.81 |
3.2.2. Health impact of program development by the prevalence of communicable diseases, blood chemical residues and sanitation improvement
(1) Regarding intestinal helminths infection (≥1 species) among students and people in targeted areas in 2016 and 2018, prevalence totalled 25.6 and 12.7%, respectively. Comparing the infection rate using Z test statistics indicated a significant reduction (z3.86, p-value 0.015).
(2) Chemical residues in the subjects’ blood detected using cholinesterase test kits (serum test) showed slight differences between 2016 and 2018 (z 0.94, p-value 0.057).
(3) Toilet coverage among households in the targeted areas significantly increased between before and after implementing the community development project (t 4.61, p-value 0.001) (Table 5).
3.2.3. Environment Improvement
When comparing before and after implementing the community development project, improved community environmental management practices could be observed in the activities listed below.
(1) Changes in garbage separation and disposal processes at the household level, including biowaste use, income from garbage recycling and constructing context-specific community garbage separation points
(2) Community environmental development activities, such as periodic community cleaning campaigns on special occasions, and students volunteering to collect garbage in public areas with support and supervision from teachers and local agencies
3.2.4. Community Action Plan for Sustainable Development
The evidence from local health facilities’ annual action plans and the four-year community development plan of local governments indicated that local government organizations, primary health care facilities and other related organizations had implemented continuous community development projects [35, 36] especially the 2nd strategy of the four-year community development plan concerning improving the population’s quality of life, which could be concluded as described below.
(1) Environmental development involved two prominent projects. The first constituted a public toilet construction project, a health education project concerning toilet use and a toilet cleaning campaign, under the concept of “Good toilet toward community lifestyle” in the 2019 action plan. The second involved implementing the good garbage management community, a four-year project aimed at community development by transforming organic garbage to soil fertilizer through fermentation [37, 38].
(2) Health behavior improvement could be accomplished through health education programs regarding promoting health and preventing diseases, and community health volunteers’ capacity building program, according to the four-year community development plan 2018-21 [35-38]. Moreover, short term projects were sponsored by the Department of Provincial Administration, around 667 USD/540 EUR per village, to develop community health in the areas under royally initiated programs. The main activity in these projects was health education, such as health education programs concerning helminths infection and diagnosis, malaria control programs, household iodine test programs, child health and nutrition improvement programs, breast cancer screening programs and drug abuse solving programs.
(3) Community diseases prevention involved projects concerning both communicable and non-communicable disease prevention in the community, in addition to dengue fever and malarial prevention and control campaigns [35-39] (Fig. 1).
| Variable | Year | Amount* | Prevalence | Statistics | Significance |
|---|---|---|---|---|---|
| Helminthes | 2016 | 192 | 25.6% | Z=3.86 | P=0.015 |
| 2018 | 189 | 12.7% | |||
| Malaria | 2016 | 192 | 0% | - | - |
| 2018 | 189 | 0% | |||
| Blood chemical residues | 2016 | 192 | 85% | Z=0.94 | P=0.057 |
| 2018 | 189 | 80% | |||
| Latrine coverage** | 2016 | 194 | 65% | t=4.61 | P=0.001 |
| 2018 | 194 | 90% |
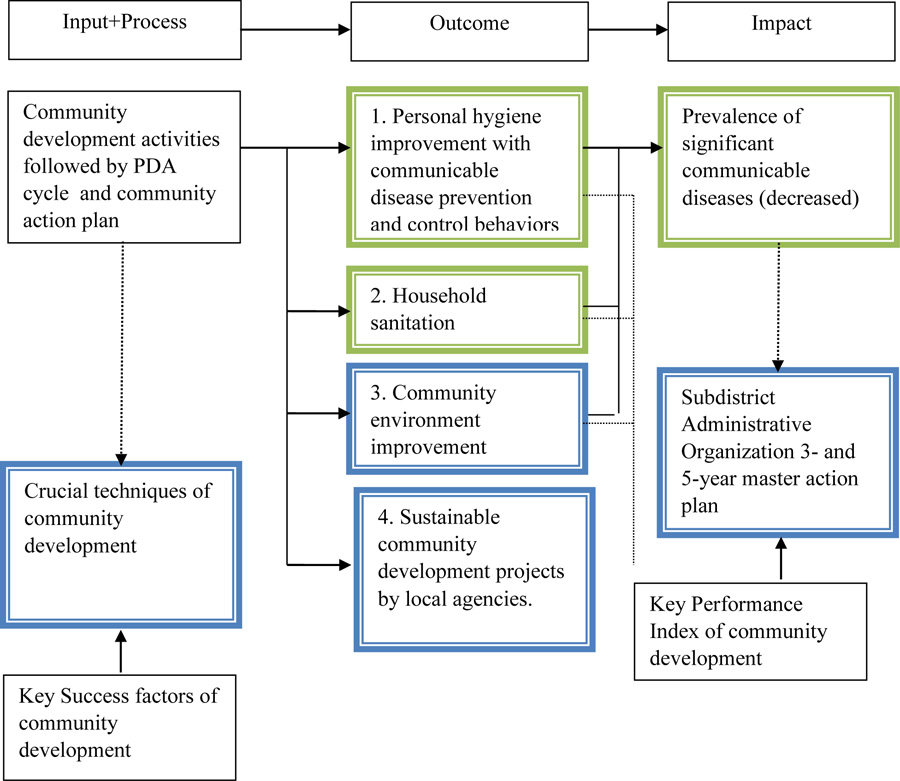
*Green box using Quantitative study, Blue box using Qualitative study
4. DISCUSSION
The target of ethnic community development in the areas under royally initiated projects was to improve people’s quality of life under their original community lifestyle and specific contexts. Therefore, all community health development activities covered three significant dimensions, including physical illness, environmental management and population learning processes to improve health behaviors. The details are provided below.
1. Regarding physical examination in the ethnic community, people prioritized economic issues rather than health. Then communicable diseases remained a major health problem, particularly, helminths infection among students [40]. Although they were infected, no symptoms or any severity were observed. Then screening tests to identify infection became important [40-41]. Moreover, communicating treatment guidelines and infection data were crucial for secondary prevention (re-infection) because the majority of the population comprised mono-crop farmers. Chemical substances and pesticides were always used on their farms to increase product yield. Some farmer practices were appropriate, while the others were harmful when considering chemical using guidelines. Blood chemical residue testing among farmers and consumers created awareness and activated strategic plans toward preventing chemical contact and reducing agricultural chemical use [42].
2. Concerning environmental management described in the Ottawa’s Charter, environmental health promotion comprised one significant issue accounting for a population’s well-being [43, 44]. Health hazards were encountered when people resided in polluted or contaminated environments. Environmental management could protect humans from both direct and indirect biological, chemical and physical health impacts [45, 46]. Then ethnic community development had to assess environmental health risks using community participation processes. These activities concerned reflecting on health professionals’ opinions based on community contexts. Then these environmental health risks illnesses links should be depicted to understand the community and related networks, an important learning processes. The environmental health risks in the ethnic community are detailed below:
- Toilet use was an important and urgent issue in community development. Toilet use reduced helminths epidemics because less helminths contamination occurred in the local environment [47]. Then public toilets were built in the ethnic community. To promote toilet use, some toilet standards should be adapted to fit the ethnic community contexts. Government officers’ participation was a key success factor for public toilet construction, especially in the ethnic communities located in forest reservation areas and national parks, due to economic difficulties of the ethnic people. The evidence showed that providing only material support for them to build public toilets by themselves was unsuccessful.
- Regarding household wastewater management, ethnic people, preferred to build their houses on sloping land, so wastewater from houses built on higher land would flow toward houses built on lower land. This initiated the hookworm epidemic cycle in wet areas [48]. Household wastewater management for use in farming was the solution to this situation. Moreover, it could reduce water consumption and household wastewater discharged in natural water sources.
- For garbage, the majority produced in the ethnic community comprised plastics and waste materials. Originally garbage disposal practices in the ethnic community involved burning and littering. Littering in nature caused risks in chemical contact, especially agricultural chemical substances. These could also contaminate community water reservoirs constituting a problematic issue [49]. Two recommendations were offered to manage garbage from the Department of Health. Firstly, garbage sorting was employed for reusing, recycling or transforming to agricultural products and economic resources. Secondly, waste (the garbage which could not be reused or recycled) should be burnt [50]. Community garbage management could reduce disease vectors as well as vector sources [51].
- Regarding livestock management, an ethnic community’s traditional livestock was raised in nature, such as space under their houses because it constituted an economic and convenient practice. Moreover, these animals were easy to guard from their predators [52]. However, confining animals under houses caused annoying results and health deteriorating factors for residences. Raising livestock on a ranch separated from the house was suggested as a livestock management guideline. It became necessary to educate people about the risks of under the house livestock, and usefulness of a ranch separated from the house. Moreover, raising pigs on a ranch could reduce Ascariasis by preventing Ascaris lumbricoides eggs contamination on the ground [53].
3. Health behavior improvement was a causal factor of both non-communicable and communicable disease management [54]. However, implementing only health behavioral change programs or health education programs could not effectively change human behaviors. The aforementioned programs could only trigger people’s learning processes [55]. Continuous health literacy development processes with regular stimulation were believed to activate people’s pre-contemplation to contemplation, leading to decision making for behavioral change processes [56-58]. These involved time consuming processes need consistency and continuity based on behavioral sciences. Achieving behavioral change in ethnic populations was more difficult than usual because of community-specific concepts, ideology, culture and tradition. The most important factor was differences in language for communication. This was the reason health behavioral change among ethnic people needed “ethnic health communicators”. They served as key individuals acting as interpreters, communicators, process designers and actors on the health team. They provided the main mechanism of the ethnic health behavioral change system [59]. This showed the significance of additional capacity building processes for ethnic health communicators concerning content understanding and persuasive skills. To achieve this, ethnic health communicator recruitment was also one of the key success factors, because we needed to implement it correctly at the beginning. The role of academic and health staff as process facilitators supported the ethnic health communicators along the planned community development process.
The target of health behavioral improvement could change health behaviors, or reduce health risks. Specific health behavior changes need time. Evaluating any health behavioral change also requires closely observing backstage behaviors. The first step of behavioral change was to adjust people’s mindsets. This could be assessed through willingness to change or contemplate where people became open to suggestion and adaptation or ready to change. Then it led to preparation for change, change or action, and maintenance. The impact of health behavioral improvement was reflected by the illness situation caused by those specific risks targeted in behavioral change programs. In short, reduced illnesses could serve as a success indicator of health behavioral programs.
CONCLUSION
The foundation of this community development involved confidence and faith among community members. The processes were valuable, meaningful and competent to community members who maintained their own dignity. Consequently, any practice undermining human dignity should be seriously avoided [60]. Hence, the concepts of this community development are described below.
(1) The principle of human dignity and belief in people’s potential: The action plan focused on community members’ empowerment to maximize their own potential and social capital. The local people possessed the ability to learn and improve themselves when they were provided the opportunity. Thus, they could design, plan, implement and evaluate their own community development projects.
(2) Self-reliance principle: The action plan promoted self-reliance using community empowerment processes. The government organization only supported and facilitated these development processes, particularly issues beyond the community’s authority.
(3) Community participation: Local people were the owners of their community development processes. They would participate in every step of the process from the beginning to the end including problem recognition, situation analysis, design, plan, implementation and evaluation. Government staff created a sense of belonging in the community development project among the local people.
(4) Democracy concept: The community development process was started using dialogue, discussion, creative meetings and consultation to promote community participation. These involved coordinating decision making, implementation and responsibility for the consequences, according to a democratic pattern.
The successes of this three-year development project included better prevention of illness and reduced health risks. Local people attained their expected health behaviors. In addition, the sustainability of this project was illustrated through action plans of every related organization and was consistent and synergized toward the targets of this community development project. Another benefit of this project was coordination, according to democratic concepts, between community leaders and their networks. Most importantly, the ultimate achievement of this project was the community’s learning process to design and plan their next development project based on their specific conditions, contexts and social capital in their community, which we could claim as sustainable development.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by the Committee for Research Ethics of Sirindhorn College of Public Health Chonburi, Praboromarajchanok Institute For Health Workforce Development, Thailand (approval number No T31/2018).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures were followed in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Written informed consent was obtained from each participant before participating in the study.
STANDARDS OF REPORTING
COREQ guidelines and methodologies were followed in this study.
AVAILABILITY OF DATA AND MATERIALS
The data will not be shared because the subjects in this study comprise a vulnerable group. Data supporting the findings of this study are available on request from the corresponding author [W.N], upon reasonable request.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The researchers would like to thank all members of the research participants at Pgazkoenyau Community, Tak Province, Thailand that assisted with the recruitment of participants; Dr. KringKeao Sa-adrat and all stakeholders who shared their time and experiences for this research.

