All published articles of this journal are available on ScienceDirect.

Professional Nurses Perceptions of Integrated School Health Team Performance in the Eastern Cape Province of South Africa in 2018
Abstract
Background:
Optimal performance of the school health programme requires integration between services and other programmes to make sure that school health services are delivered in the most efficient and effective way.
Aim:
The aim of the current study was to assess nurse’s perception of the integrated school health performance and determine team, service-related factors associated with the optimal functioning of the integrated school health teams.
Methods:
An analytical cross-sectional study was conducted in the Eastern Cape Province, South Africa, amongst all professional nurses who were team leaders for one year or more. In the school health teams in the Eastern Cape in 2018 or a school health member deputised in for a team leader. Primary data was collected from the participants using a structured self-administered questionnaire with closed-ended questions. Descriptive statistics were used to describe the socio-demographic variables. Bivariate analysis and multi-variate logistical regression were used to identify potentially significant associations.
Results:
Of the 172 professional nurses invited to participate, a total of 120 nurses were included in the study. Fifty-two (43%) professional nurses reported their satisfaction with the service delivered (i.e. optimal functioning perception). Females (OR: 1.09 CI: 0.48-2.52) and respondents of age group 60 years and above (OR: 1.09 CI: 0.48-2.52) showed increased probability of a satisfactory perception of optimal functioning, however significance was only seen for female sex (p<0.05). Clear roles and responsibilities were associated with a 5.7 (95% CI 1.26 – 42.38) times more chance of optimal function than when there is no clear roles or responsibilities (p = 0.043). On the other hand, a health team that needed all the other services had a 69 per cent less chance of an optimal function than the team that needed just some of the other services.
Conclusion:
Professional nurses have a positive perception of the performance of school health teams. Clear roles and responsibilities (accountability), support from other DOH and with adequate follow up procedures in place, school health teams have the potential of performing optimally.
1. BACKGROUND
South Africa ranks amongst the highest investors in healthcare in comparison to other countries in Africa utilising 8.7 per cent of its gross domestic product (GDP), healthcare [1]. Despite the high expenditure, health outcomes are sub-optimal when compared to other middle income countries [2].
The poor health outcomes in terms of life expectancy are attributed to the quadruple burden of disease (consisting of violence and injuries, non-communicable diseases, Human Immunodeficiency Virus (HIV) and Acquired Immunodeficiency Syndrome (AIDS) and Tuberculosis) [2] coupled with systemic challenges with regards to the availability of human and financial resources, fragmented service delivery and accessibility of health services [2].
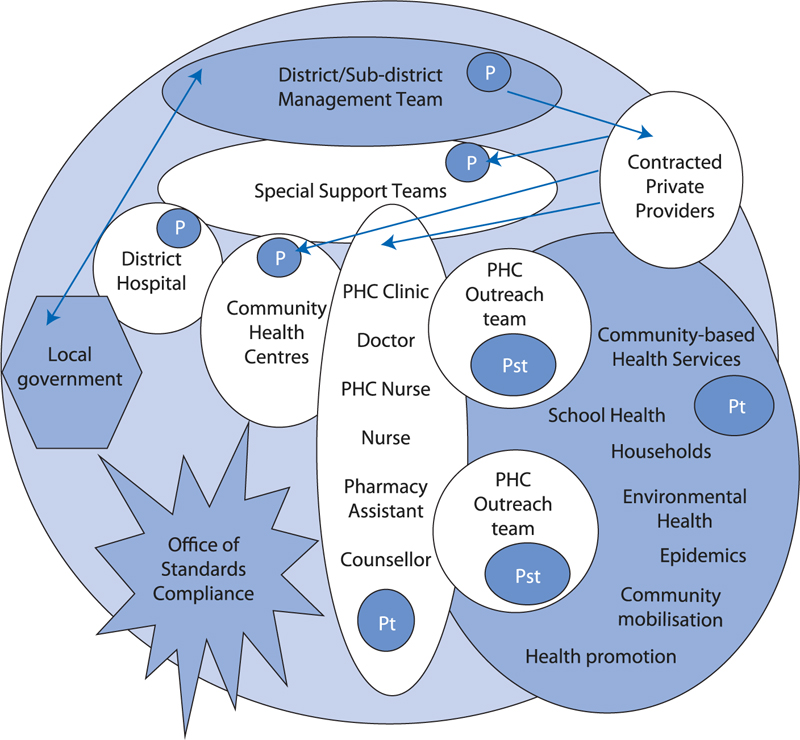
In order to address the challenges from a health system perspective, the South African government adopted the primary healthcare (PHC) re-engineering framework as a modality for health services. The re-engineering of primary health care emphasises promotive and preventive health care as a basis for the overall interventions [3]. The four streams of the PHC framework include the ward based outreach teams, primary healthcare clinic, integrated school health teams and contracted general practitioners (Fig. 1).
Integrated school health teams are a component of the PHC re-engineering framework. The South African Integrated School Health Policy positions that the school health team consists of a professional nurse who leads the team, an auxiliary nurse or enrolled nurse, an oral hygienist and a health promoter (who will be shared with the PHC ward-based team) [4].
In 2012, the revised policy provided for a comprehensive Integrated School Health Programme (ISHP) for grade 0 to 12 learners, implemented at sub-district level. This implementation strategy incorporates the principle of equity and human rights with specific consideration to the availability of resources required to cover all learners [4].
The aim of the revised policy was to facilitate services to reach each individual learner in all the schools within sub-districts, simultaneously outlining the roles and responsibilities of the respective departments in addressing the health needs of learners. The programme offers a comprehensive and integrated package of services, including sexual and reproductive health services for older learners [4].
As part of the school health programme, health promotion aims to create a healthy school environment by promoting the general health and wellbeing of learners and educators and by addressing key health and social barriers to learning in order to promote effective teaching and learning. This assists in increasing knowledge and awareness of health-promoting behaviour [4].
South Africa’s school health programmes have struggled in the past due to poor management, inequitable distribution of resources and a historical lack of collaboration between the departments of health and basic education. In the 2016/17 four provinces did not achieve the national target, with the Eastern Cape being one of the provinces reporting coverage below the national target [5]. Even though coverage has increased in the other provinces in the last three years, the Eastern Cape was the only province where coverage dropped from 19.0 per cent in 2015/16 to 17.2 per cent in 2016/17. This indicates that there is still a gap with regards to implementing the Integrated School Health Policy in the Eastern Cape Province [5].
Optimal performance of the school health programme requires integration between services and other programmes to make sure that school health services are delivered in the most efficient and effective way [4]. Proper referral and follow-up of learners who are assessed and noted to have health or other problems, including intersectoral collaboration between the Department of Health (DoH), Department of Basic Education (DBE) and the Department of Social Development (DSD) are important considerations for the optimal performance of the school health teams. The aim of this study was to assess professional nurse’s perception and determine team and service-related factors associated with the optimal performance of the integrated school health teams.
2. MATERIALS AND METHODS
2.1. Study Design and Setting
The study was a cross-sectional study with an analytical component. The study was conducted in the Eastern Cape Province that has a population of 6,562,053 and has 79 school health teams working on the Integrated School Health Programme (ISHP).
2.2. Study Population and Sample Size
The study population included all professional nurses who were team leaders for one year or more in the school health teams in the Eastern Cape in 2018 or a school health member standing in for a team leader. Members of the school health team who were not professional nurses (e.g. Oral hygienist, enrolled nurses, and health promoter) were excluded from participating. The total population size was approximately 300. Thus, a sample size of 172 was required to maintain a five per cent precision at the 95 per cent confidence level.
2.3. Data Collection
A structured self-administered questionnaire was used to collect data from participants. Socio-demographic information that was collected of the participants’ ages, gender, how long they have been working, and the logistics around working as part of this team. The participants were requested to complete fifteen questions to analyse the factors that influence the success of school health teams divided into four sub-sections namely, management and leadership, referrals and follow-up, feedback and meetings, and work routines. The self-administered questionnaire was in English, however, participants were given the opportunity to express themselves or respond in the language most comfortable to them. The questionnaire was anonymous and largely self-administered.
2.4. Data Management
Data were extracted from the questionnaires, where it was captured using the Epi Info software tool. The data was cleaned and exported to Stata Version 13.0 (StatCorp.2013. Stata Statistical Software: Release13. College Station, TX: StataCorp LP)., which was used for the analysis. Access to equipment and storage media was limited to the principal investigator. All electronic files were protected with login and passwords. Primary data were cleaned and coded before analysis and log files were backed up and stored using an external hard drive. All completed data sheets were stored in a lockable cupboard for further reference and safekeeping. After the data storage period of five years, all hard copies and electronic data will be destroyed securely.
2.5. Data Analysis
The socio-demographic variables were summarised using proportions for categorical variables and measures of central tendency for numerical variables and displayed in a table. Professional nurses perception of optimal functioning of the school health team was the outcome variable.
All variables with a significance of p<0.2 were included in the multivariable logistic regression model along with ‘optimal functioning’ as it was an important variable of interest in this study. Variables were tested for collinearity and those with a variable inflation factor >5 were excluded. A stepwise backward logistic regression analysis was conducted to identify the specific important confounding factors. Interaction between significant variables was also tested.
2.6. Ethics and Informed Consent
Ethical approval for the study was obtained from the University of KwaZulu Natal Biomedical Ethics Research Committee (Ref no. BE554/18). The Eastern Cape Department of Health (DoH) and the Eastern Cape Department of Education provided authorisation to conduct the study. Gatekeeper’s permission was obtained from the District Managers of the Health Districts. Informed consent was obtained from participants. The informed consent document was translated into isiXhosa and Afrikaans.
3. RESULTS
3.1. Study Population
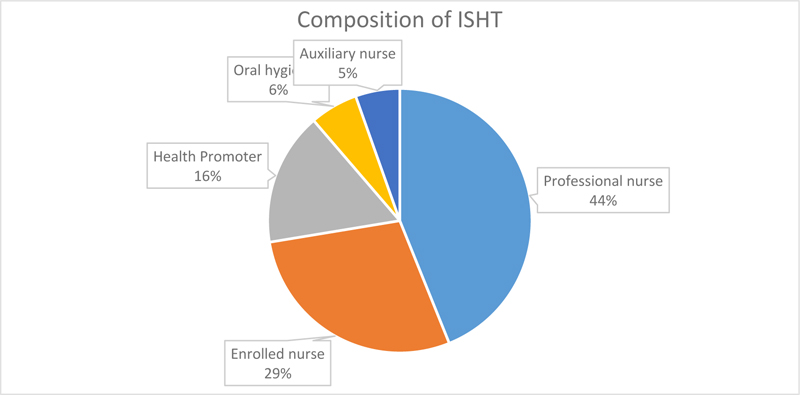
Of the 172 professional nurses invited to participate, 120 nurses were included in the study, 52 nurses were not available to participate as their contracts expired. The yield was thus 70 per cent. The mean (SD) age was 55.1 years (±12 years), with a range between 27 years old and the oldest being 68 years old. The median age was 60 years (IQR: 46– 64 years), indicating a skewed to the left distribution of the study population with the majority of the participants aged between 60 and 65 years old. The ISHT in the Eastern Cape in 2018 consisted mainly of professional nurses and enrolled nurses with a limited number of other cadres such as oral hygienists, health promoters and auxiliary nurses (Fig. 2). The majority (52%) of the members of the ISHT were in the age group 50-<65 years old and comprised a higher proportion (89%) of females. The majority of them served the OR Tambo district (30%), followed by Chris Hani (17%) and 13 per cent for Nelson Mandela Metro.
One hundred (83%) of the school health teams assessed 50 or more school-going children per month and 54% (60) referred more than 20 school-going children per quarter. Fifty-six per cent of the school health teams (63) visited at least 5 schools per month and 110 (92%) of the school health teams did fewer than 21 follow-ups of cases per month in their sub-districts. Forty-seven (39%) of the school health teams had formal monthly meetings to discuss challenges or cases, with 73 (61%) of the meetings being informal (other). One hundred and five (88%) of the health teams participating in the study were clear about their roles and responsibilities.
3.2. Perception of Integrated School Health Team Performance
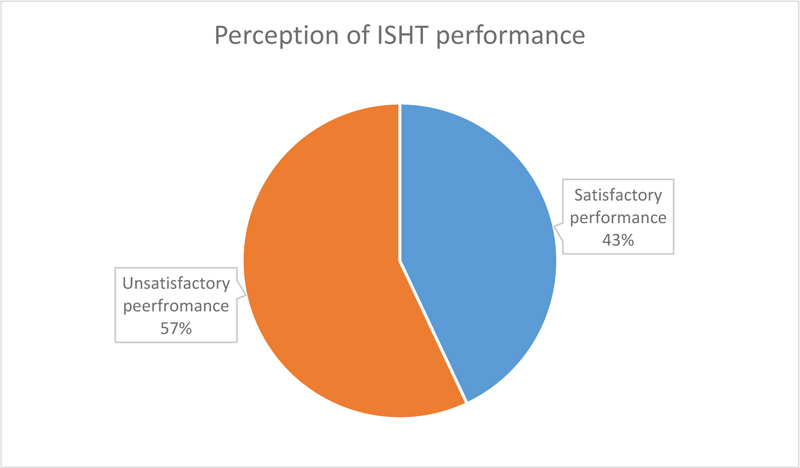
Fifty-two (43%) professional nurses reported a positive perception of the service delivered by the school health teams (Fig. 3).
Amongst the ISHTs whose performance was perceived as satisfactory, 90% (n = 46/52) of the professional nurses were females and 56% (n=29/52) of the professional nurses were above the age of 60. Fifty-eight percent (n= 30/52) of ISHTs visited more than 5 schools per month and 81% (n= 42/52) assessed more than 50 children per month. Of the ISHTs with positive perception 25% (13/52) had the relevant cadres as members of the team. Overall respondents indicated that 88% (105/120) of the ISHTs had clearly defined roles and responsibilities, with 96% (50/52) of the ISHTs that were perceived to have satisfactory performance having clearly defined roles and responsibilities. Monthly meetings were conducted by 39% (n=47) of the ISHTs, with only 42% (n=22/52) of the ISHTs with a positive perception of ISHT performance conducted monthly meetings.
Of the respondents that had a positive perception of ISHT performance, 100% (n = 52) indicated that transport was important, 98% (n = 51) were of the view that the attitude of team members was important, 100% (n=52) indicated that resources were important, and 96% (n = 50) were interested in seeing client satisfaction (Table 1).
| Overall Service |
Unsatisfactory (n=68) |
Satisfactory (n=52) |
p-value |
Overall (n=120) |
|---|---|---|---|---|
| Age Group | 0.758 | |||
| <60yrs | 32 (47%) | 23 (44%) | 55 (46%) | |
| 60+yrs | 36 (53%) | 29 (56%) | 65 (54%) | |
| Gender | 0.828 | |||
| Male | 7 (10%) | 6 (11.5%) | 13 (1%) | |
| Female | 61 (90%) | 46 (90%) | 107 (89%) | |
| Schools Visited | 0.72 | |||
| <5 | 31 (46%) | 22 (42%) | 53 (44%) | |
| 5+ | 37 (54%) | 30 (58%) | 67 (56%) | |
| School Children Assessed | 0.51 | |||
| <50 | 10 (15%) | 10 (19%) | 20 (17%) | |
| 50+ | 58 (85%) | 42 (81%) | 100 (83%) | |
| Relevant Cadres | 0.099 | |||
| No | 59 (87%) | 39 (75%) | 98 (82%) | |
| Yes | 9 (13%) | 13 (25%) | 22 (18%) | |
| Clear Roles/Responsibilities | 0.012 | |||
| No | 13 (19%) | 2 (4%) | 15 (13%) | |
| Yes | 55 (81%) | 50 (96%) | 105 (88%) | |
| Follow-Ups | 0.02 | |||
| <21 | 66 (97%) | 44 (85%) | 110 (92%) | |
| 21+ | 2 (3%) | 8 (15%) | 10 (8%) | |
| Meetings Conducted | 0.538 | |||
| Other | 43 (63%) | 30 (58%) | 73 (61%) | |
| Monthly | 25 (37%) | 22 (42%) | 47 (39%) | |
| Children Referred | 0.498 | |||
| <20 | 33 (49%) | 22 (42%) | 55 (46%) | |
| 20+ | 35 (52%) | 30 (58%) | 65 (54%) | |
| Transport | 0.505 | |||
| Other | 2 (3%) | 0 (0%) | 2 (2%) | |
| Very Important/ Important | 66 (97%) | 52 (100%) | 118 (98%) | |
| Attitude | 0.232 | |||
| Other | 5 (7%) | 1 (2%) | 6 (5%) | |
| Very Important/ Important | 63 (9%) | 51 (98%) | 114 (95%) | |
| Resources | 0.132 | |||
| Other | 4 (5.9%) | 0 (0%) | 4 (3%) | |
| Very Important/ Important | 64 (94%) | 52 (100%) | 116 (9%) | |
| Satisfaction | 1 | |||
| Other | 2 (3%) | 2 (4%) | 4 (3%) | |
| Very Important/ Important | 66 (97%) | 50 (96%) | 116 (97%) | |
| Professional Team | 1 | |||
| Incomplete | 67 (99%) | 51 (98%) | 118 (98%) | |
| Fully Constituted | 1 (2%) | 1 (2%) | 2 (2%) | |
| Referral Services Available | 0.265 | |||
| Incomplete | 52 (77%) | 35 (67%) | 87 (73%) | |
| Fully Constituted | 16 (24%) | 17 (33%) | 33 (28%) | |
| Other Services Needed | 0.043 | |||
| Some Needed | 36 (53%) | 37 (71%) | 73 (61%) | |
| All Needed | 32 (47%) | 15 (29%) | 47 (39%) |
| VAriable | Bivariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| Unadjusted OR | P-value | 95% CI | Adjusted OR | P-value | 95% CI | |
| AGE (60+) | 1.12 | 0.758 | 0.54-2.33 | 1.09 | 0.832 | 0.48 -2.52 |
| GENDER (Female) | 0.88 | 0.0828 | 0.27 -2.90 | 0.86 | 0.832 | 0.22 -3.44 |
| RELEVANT CADRES (Yes) | 2.19 | 0.104 | 0.86-5.77 – | 1.55 | 0.398 | 0.56 – 4.40 |
| Schools Visited | 1.14 | 0.720 | 0.55-2.38 | 1.42 | 0.428 | 0.60-3.44 |
| Children Assessed | 0.72 | 0.511 | 0.27-1.92 | 0.59 | 0.39 | 0.18-2.01 |
| Clear Roles and Responsibilities | 1.20 | 0.024 | 1.53-38.99 | 5.81 | 0.043 | 1.36-41.31 |
| Follow-ups | 6.00 | 0.028 | 1.42-41.01 | 6.74 | 0.185 | 1.41-53.215 |
| Meetings Conducted | 1.26 | 0.538 | 0.60-2.65 | 2.65 | 0.981 | 0.42-2.40 |
| Children Referred > 20 versus < 20 | 1.29 | 0.498 | 0.62-2.68 | 1.38 | 0.489 | 0.56-3.47 |
| Other Services Needed | 0.46 | 0.045 | 0.21-0.97 | 0.31 | p=0.03 | 0.10-0.86 |
3.3. Team and Service-related Factors Affecting Optimal Functioning of the ISHT
The findings were categorised nominally by either unsatisfactory or satisfactory perception of optimal functioning (Table 2). Among those that had an optimal function perception, 58 per cent (n = 30) had visited at least five schools, 80.8 percent (n = 42) had assessed at least 50 school children, 75 percent (n = 39) did not have relevant cadres of staff (Table 1).
Bivariate analysis of socio-demographic factors showed that the respondents in the age group 60 years and above (OR: 1.12 CI: 0.54-2.33) have an increased probability of having a satisfactory perception of optimal functioning, with the female gender being the only variable that was statistically significant (p<0.05) (Table 2).
After multivariate analysis, females (OR: 1.09 CI: 0.48-2.52) and respondents age group 60 years and above (OR: 1.09 CI: 0.48-2.52) showed an increased probability of a satisfactory perception of optimal functioning, however, significance was only seen for female sex (p<0.05). Being female was significantly associated with a satisfactory perception of optimal functioning (p<0.05). Age > 60 years (OR: 1.09 CI: 0.48-2.52) was associated with the perception of optimal functioning (Table 2).
Ninety-six per cent (n = 50) of optimal functioning ISHT’s had clear role responsibilities, 85 per cent (n = 44) conducted less than 21 follow up visits, 58 per cent (n = 30) had conducted meetings at a different frequency rate which was not monthly, and 58 per cent (n = 30) had referred at least 20 children. Eighty-one per cent (n= 42) of those that are functioning optimally assessed more than 50 school children per month. There was a significant difference in the perception of optimal functioning between school health teams with clear roles and responsibilities than those without. Furthermore, among the team that showed an optimal function perception, 98 per cent (n = 51) had an incomplete professional team. Moreover, among all that indicated an optimal function perception, 100 percent (n = 52) indicated that transport was important, 98 percent (n = 51) were of the view that attitude was important, 100 percent (n=52) indicated that resources were important, as well as 96 per cent (n = 50) were interested in seeing satisfaction.
After bivariate analysis, clear roles and responsibilities [1.20 (95%CI 1.5- 38.99, p = 0.024)] and follow up visits were significantly associated with optimal functioning [6.00 (95% CI 1.42-41.01, p= 0.028)]. On the other hand, there was an increase in the probability of optimal function for those teams which followed up more than 21 times, where the odds went up to 41.01 (95%CI 0.60– 30.61, p = 0.185) times more than those who had less than 21 follow-ups. Clear roles and responsibilities was the only factors that remained statistically significantly associated with optimal function after multivariate analysis (Table 2).
After controlling for confounders and co-linearity, clear roles and responsibilities and the need for other services were the only significant contributing factors. Adjusting for all the studied factors, clear roles and responsibilities was associated with a 5.7 (95% CI 1.26 – 42.38) times more chance of optimal function than when there is no clear roles or responsibilities (p = 0.043). On the other hand, a health team that needed all the other services had a 69 per cent less chance of an optimal function than the team that just needed some of the other services.
4. DISCUSSION
The importance of health and the overall wellbeing in schools and communities has been shown to improve the learning outcomes of learners. Strengthening school health programme services at a district health level has been the focus of the ISHP programme, however there is little evidence in the local context of the current state of ISHT performance or the factors with which it is associated.
Staff composition and allocation may differ between provinces; however, teams are allocated according to the required norm of one team to 2,000 learners who require a health assessment. As per the South African Integrated School Health Policy, the school health team consists of a professional nurse who leads the team, an auxiliary nurse or enrolled nurse, an oral hygienist and a health promoter (will be shared with the PHC ward-based team). The results indicate that majority of the staff in the school health teams comprised of professional nurses, with more enrolled nurses (63%) than auxiliary nurses (12%), and that there were only a few health promoters (36%) and oral hygienists (13%) per team.
Professional nurses appear to be the ‘backbone’ of school health services as 97 per cent of the school health teams consist of a professional nurse, which is in line with the findings of other research [6, 7]. Unavailability of professional nurses in three per cent of the teams was caused by management-related issues whereby whenever sub-districts experienced a shortage of personnel in the primary health care facilities, and managers withdrew school health nurses to replace the missing staff members. This is consistent with other similar studies, as professional nurses are often unclear about their roles and responsibilities, which cripples the continuity and the quality of services offered to the school children [7].
The findings of this study showed that 87 per cent of the school health teams did not have an oral hygienist and 64 per cent of the school health teams did not have a health promoter. The World Health Organisation highlights the need for oral health promotion in schools as oral health is fundamental to general health and wellbeing [8]. The school health team works with the primary health care team to provide oral health education, treatment, regular monitoring and, for more complicated conditions, referral to other dental or medical specialists and secondary care [8]. In the South African context, oral health problems are the most commonly reported health problems in school-aged children; the prevalence of dental caries is as high as 87 per cent in some provinces [6, 9]. On the other hand, in 2017 a mixed-methods study conducted at 23 health-promoting schools in KwaZulu-Natal to evaluate an implemented tooth brushing programme; showed that the school setting has the potential to deliver integrated preventive and promotive programmes provided they are supported by adequate funding and resources [10]. Not having an oral hygienist on site has been a notable challenge in delivering school health services, as the professional nurses reported that this delays the response rate (waiting period) to learners’ cases as they need to be referred to primary health care facilities with limited basic equipment.
4.1. Age, Gender, and Relevant Cadres
Majority of the professional nurses were female and above the age of 60 years. It was noted that the majority of the professional nurses on the Integrated School Health Programme are retired nurses who are employed on a contract basis. There are no studies in the local South African context that report on age groups of school health team staff. Other studies have focussed on the socio-demographic and health profile of South African school-aged children rather than on the staff delivering the school health programme [6].
Of the professional nurses who participated in this study, 89 percent were female and only 10 percent were male; however, there is limited research in the South African context that reports on the gender of the school health team staff.
This study shows that 56 per cent of the school health teams visited more than five schools per month. Previous research has demonstrated the challenge of attaining 100 per cent coverage of schools in sub-district areas [6, 7, 11]. The challenges of attaining 100 per cent coverage highlighted in this study include demarcation and distance of schools, shortage of staff and unavailability of transport. These challenges are similar to other studies conducted in the South African context on factors which affect service delivery including school visits (48, 50). Nurse to school ratios varied from as high as 1:8 in one sub-district to as low as 1:3 in another sub-district. These ratios mean that schools would be visited approximately once every five years at best. The average nurse to school ratio was 1:20 - 1:30 [11].
4.2. Availability of Transport and Resources
In this study, transport and resource availability, attitude and satisfaction of services rendered were found to be important (>95%), though not showing a significant association with the optimal functioning. Even though there was not enough evidence to suggest that their availability or need influences optimal functioning, the availability of transport and resources are an integral part of the implementation of the school health programme. On the contrary, a qualitative, explorative study conducted in Mpumalanga and the Gauteng province in 2010 noted that professional nurses reported that rather than the unavailability of transport, certain rural communities had poor roads and this made it difficult for outreach programmes [7].
In this study, the unavailability of transport was magnified as professional nurses also mentioned having to use their own cars to travel to schools which caused a strain in service delivery. Work vehicles were not designated exclusively for the Integrated School Programme but were shared with other programmes in the sub-district.
4.3. Clear Roles and Responsibilities
The study’s findings confirm that having clear roles and responsibilities is strongly associated with optimal functioning (OR= 5.7, 95% CI=1.26-42.38). Having clear roles and responsibilities assists the various departments and partners in understanding what is expected of them, and thus facilitates the improved implementation of the programme. In the South African context, poor relationships between key stakeholders, in particular, the Departments of Health and Education, has been noted as a factor that contributes to poor policy performance of the Integrated School Health Programme [6].
4.4. Follow-ups of Screened School-Going Children
Bivariate analysis indicated that follow-ups conducted monthly (OR=6.00, 95% CI=1.42-41.01) of school-going children receiving school health services had a strong relationship with a positive perception of ISHT performance. The school-going children were screened and those who needed other DoH services would be referred accordingly; thus, the need to conduct follow-ups to ensure adequate intervention. When followed up, many children were reportedly unable to access referral services such as optometry and dentists due to their unavailability, location distance, and prohibitive transport costs. Therefore, nurses could also not follow-up and do home visits with children who were identified with problems. Lack of transport for nurses to schools compounded the situation. These results are consistent with previous research showing that follow-ups can be a measure of the quality services offered by the Integrated School Health Programme [6].
4.5. Other Services Needed
A network of referral facilities (optometrists, dental services, audiology services, mental health services, social workers) and functions is needed to varying degrees. For some of these services, such as optometry, contracting of private sector providers through public-private partnerships is required due to public sector incapacity [6]. In a study conducted in South Africa, correspondingly, many children were reportedly unable to access referral services such as optometry and dentists due to their unavailability, location distance, and prohibitive transport costs [11].
These findings concur with this study, as health teams that needed all the other services were associated with a lower probability of 0.3(95% CI 0.10 – 0.86) in the Eastern Cape Province for optimal functioning. Previous research has also discovered that part of the two sets of factors that contribute to poor policy performance of the Integrated School Health Programme is the immaturity of the district health system, general nursing staff shortages, and a relative lack of referral services [6].
4.6. Study Limitations
The responses of the participants in the study were beyond the researcher’s control. It is possible that the study participants were not completely honest with their responses to questions regarding adherence, or needing support, as they may have felt that their responses may affect their work status. Such questions depend on the honesty of the study participants and cannot be verified.
Surveys measuring health care effectiveness are prone to social desirability bias and gratitude bias, whereby participants may possibly over-report positive experiences perceiving the research process as being a sign of sensitivity. This may have resulted in an over-estimation of satisfactory perceptions of optimal functioning. This is also likely to introduce non-differential misclassification of outcomes, which would bias the associations towards a null. However, efforts to reduce this misclassification of outcomes included using self-completed anonymous questionnaires, and that Departmental all Programmes Managers and immediate supervisors were excluded from the data collection process. Participants were also provided with participant information sheets that included the reassurance that their responses would remain confidential and would not influence the treatment received or working relations in their departments. During the period of data collection, there were supervisors and management present in the facilities. Although participants were assured that confidentiality would be maintained and their participation in the study would not influence their working relations with their supervisors, some participants were however still reluctant to participate.
This study was an analytical cross-sectional study; therefore, the cause and effect relationship does not necessarily mean that only one factor directly causes a satisfactory perception of optimal functioning. The small sample size resulted in the study being underpowered to detect associations of socio-demographic variables with the outcomes. These associations, however, vary considerably in the literature. Also, as a result of the cross-sectional study design, causality could not be determined.
The generalisability of the study findings is limited owing to the small sample size, however the random sampling of sub-districts and professional nurses contributes to the representativeness of the study sample. The study was conducted on only those professional nurses who had the experience of the Integrated School Health Programme who were in the Eastern Cape sub-districts, and the sample, therefore, does not represent the whole population of South Africa’s ISHP. Furthermore, due to time, budget, and resource constraints, a larger overall sample size was not feasible either.
CONCLUSION AND RECOMMENDATIONS
Our findings provide compelling evidence that there should be clear roles and responsibilities (accountability), and adequate follow up procedures in place so that school health teams have the potential of satisfactory performance.
ISHP needs to be of importance to managers so that the school health nurses receive the necessary support to ensure that policy guidelines are followed so as to combat challenges in their Sub-districts. Having support from management also promotes the coordination of the available resources for optimal implementation of ISHP.
LIST OF ABBREVIATIONS
| DOH | = Department of Health |
| ISHP | = Integrated School Health Programme |
| ISHT | = Integrated School Health Teams |
| PHC | = Primary Healthcare Care |
AUTHORS' CONTRIBUTIONS
SN: conducted research, drafted initial manuscript. OHM: data analysis, finalisation of manuscript.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical approval for the study obtained from the UKZN BREC, Ref no. BE554/18. Approval was also obtained from the Eastern Cape Department of Health (DoH) and the Eastern Cape Department of Education. Gatekeeper’s permission was obtained from the District Managers of the Health Districts.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Informed consent was obtained from all participants.
STANDARDS OF REPORTING
STROBE guidelines and methodologies were followed in this study.
AVAILABILITY OF DATA AND MATERIALS
The data supporting findings of this study is available from the corresponding author [S.M.N], upon reasonable request.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

