All published articles of this journal are available on ScienceDirect.

A Systematic Review of the Risk and Protective Factors of Tobacco Use among South Indian Adults
Authors Info & Affiliations
Abstract
Background:
India is facing a crucial health burden due to the incremental rise in the prevalence of tobacco use and associated diseases. Sociocultural factors largely influence tobacco use behaviour. Hence, documenting the risk and protective factors associated with tobacco use among the South Indian population helps develop context-based interventions and policies to reduce tobacco-related issues.
Objective:
This systematic review aims to synthesise the available literature evidence on the risk factors contributing to tobacco use and the protective factors safeguarding against this health risk behaviour among South Indian adults.
Methods:
The primary author conducted a PRISMA-compliant systematic search using five databases: PubMed, Scopus, Web of Science, Wiley Online Library, and Science Direct from the inception to June 23, 2021. A manual search was also done in Google Scholar to find pertinent publications. 13 articles that met the review's inclusion criteria were selected from the 5063 articles that were initially found after a thorough screening process and suitable quality assessment. According to the socio-ecological model, the risk and protective factors identified were divided into five levels: intrapersonal, interpersonal, organisational, community, and public.
Results:
From the included studies, the major risk factors found were stress, low perceived health effect, low income, peer influence, nature of the occupation, lack of awareness about health effects due to community marginalization, community misconception of positive aspects of tobacco use and ease of availability in the market. The major protective factors identified were awareness, perceived harm to social image, familial support, community-based health education, exposure to tobacco warning labels and government initiatives of tobacco control.
Conclusion:
The multi-level factors identified from the current review findings reveal the need for population and context-specific interventions as well as the tobacco control policies to be developed in the near future. Interventions tailored to address the risk factors and incorporate the protective factors identified would benefit the South Indian community in tackling this health burden.
1. INTRODUCTION
Tobacco use is one of the leading causes of preventable morbidity and mortality across the globe. As per global statistics, around 100 million people died in the 20th century due to tobacco consumption and associated diseases. It is anticipated that this could account for up to 1 billion deaths in consecutive centuries if proper interventions are not provided [1, 2]. The South-East Asia region mainly consists of developing countries, and tobacco use kills nearly 1.2 million people in these regions annually [1, 3, 4]. India is a middle-income developing country and the second-largest tobacco producer and consumer after China [5]. In India, tobacco consumption is very complex since there is a wide variety of smoking (bidi, cigarettes) and smokeless forms (khaini, chewing pan, gutkha or pan masala and mishri) of tobacco available in the market.
According to the Global Adult Tobacco Survey (GATS) conducted in 2016–17, in India, the overall prevalence of smoking tobacco use is 10.38%, and smokeless tobacco use is 21.38%. Irrespective of its form, tobacco use has health consequences [6, 7]. Empirical studies conducted in India have found various demographic, social, economic and cultural factors associated with tobacco use. But most of the studies were confined to a small geographical location representing only one state [8]. As per the key findings from Phase 1 of the National Family Health Survey conducted in 2019–20, which incorporated results of current tobacco use among Indian adults in 22 states and union territories, the prevalence of tobacco use in South Indian states is noteworthy. The tobacco prevalence among men in Karnataka, Andhra Pradesh, Telangana, and Kerala, as per the report, are 27.1%, 22.6%, 22.3% and 16.9%, respectively, whereas, among females, it is 8.5%, 3.8%, 5.6%, 2.2% respectively [8]. Compared to the northeastern states of India, where any type of tobacco consumption is considerably high due to the cultural relevance and social acceptability [9], the major factors behind the increasing tobacco use among the South Indian population have not been comprehensively documented yet.
Hence, considering the rise in tobacco use prevalence in South Indian states and the socio-cultural determinants which influence this behaviour, the current systematic review tries to synthesise the available literature evidence on the major risk factors contributing to this behaviour and also the protective factors which safeguard individuals from engaging in the risk behaviour. This review tries to evaluate the multi-level factors using the socio-ecological model to comprehensively understand these factors. Grounded in Urie Bronfenbrenner’s (1977) ecological framework, McLeroy et al. (1988) developed a multilevel ecological model specific to health behaviour [10, 11]. According to this model, there are five levels of influence on various health behaviours: individual, interpersonal, organizational, community and public policy [12, 13]. Factors such as attitudes, knowledge and belief influencing behaviour are classified under the individual level, while all other environmental influences on an individual’s behaviour, such as peer influence, organizational structures, community norms and societal policies, come under the other four levels [14]. This model is found to be effective in developing health promotion interventions because it explores beyond the individual level influences on behaviors and examines different levels of environmental factors influencing that behaviour [15]. This review could provide insight into the multi-factorial approach that can be considered while developing further interventions to encourage individuals to quit this addictive habit.
2. METHODS
2.1. Search Strategy
This systematic review was carried out according to the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines published by Page et al., 2021 [16]. A systematic search was conducted on five databases: PubMed, Scopus, Web of Science, Wiley Online Library and Science Direct from inception to June 23, 2021, by the first author. A manual search was also performed on Google Scholar to identify additional relevant studies. The key search terms used were “Factors”, “Tobacco Use,” and “India.” The same keyword search was followed in the five databases, for example, in PubMed ((“factor”[All Fields] OR “factor s”[All Fields] OR “factors”[All Fields]) AND (“tobacco use”[MeSH Terms] OR “tobacco”[All Fields] OR “tobacco use”[All Fields]) AND (“India”[MeSH Terms] OR “India”[All Fields] OR “India s”[All Fields] OR “Indias”[All Fields])). The search term was kept broad to extract all the relevant literature. The manual search was done using specific key terms such as “Smoking,” “Correlates,” and “Predictors” after the database search intended to cross-check if any relevant information was missed out. The extracted dataset from the systematic search was saved, and records are kept with the authors.
2.2. Study Selection Criteria
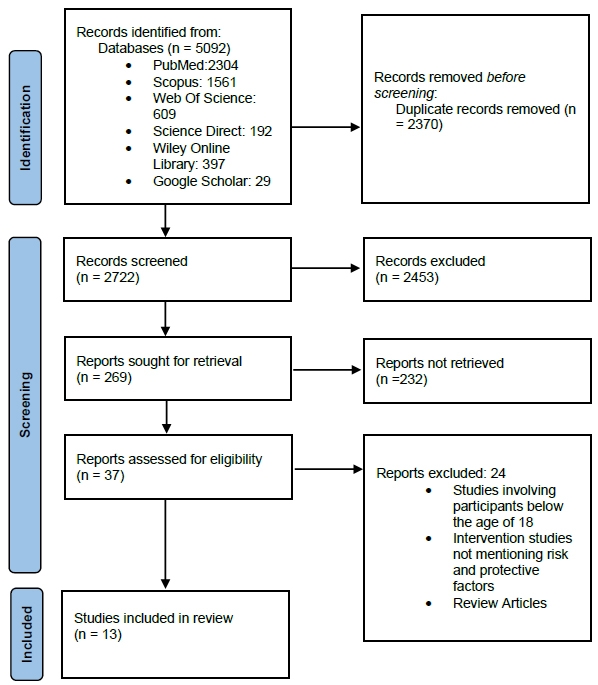
The extracted data from each database (PubMed: 2304, Scopus: 1561, Web of Science: 609, Science Direct: 192, Wiley Online Library: 397, Google Scholar: 29) was imported to Zotero, a bibliographic reference management tool and all duplicates were removed. The de-duplicated citations in Zotero were then exported to data extraction file format for further screening. In the initial stage, a brief title review was done to check the relevant article by the first author. This was followed by a detailed abstract screening and full-text assessment to determine the outcome of interest and other inclusion requirements. The main outcome of interest measured were risk and protective factors influencing tobacco use behaviour among South Indian adults. The study inclusion criteria were:(i) quantitative, qualitative or mixed-method studies (ii) studies conducted in various parts of South India (iii) studies in which participants are above 18 years of age, and (iv) studies published in English language. The exclusion criteria include: (i)studies reporting factors influencing substance use in general and not specifically tobacco use behaviour (ii) study designs such as protocol studies, conference papers and review articles. The step-by-step article screening process and reasons for excluding articles are depicted in the PRISMA flow diagram (Fig. 1).
2.3. Quality Assessment of the Included Studies
Two authors independently assessed the methodological quality of all the included studies using the appropriate appraisal tools based on study designs. Mixed Methods Appraisal Tool (MMAT) version 2018 was used for the quality assessment of qualitative, quantitative and mixed-method studies included in the review [17]. As per MMAT, it is discouraged to calculate an overall score from the ratings of each criterion. Rather it is advised to provide a more detailed presentation of the ratings of each criterion as “Yes,” “No,” or “Can’t Tell” to better inform the quality of the included studies. This would thus lead to performing a sensitivity analysis. Any disagreements in the inclusion of studies during the quality assessment were addressed and resolved through discussion among the authors, thus ensuring inter-rater agreement regarding included study quality (Supplementary File: Quality Assessment of Included Studies).
2.4. Data Extraction and Analysis
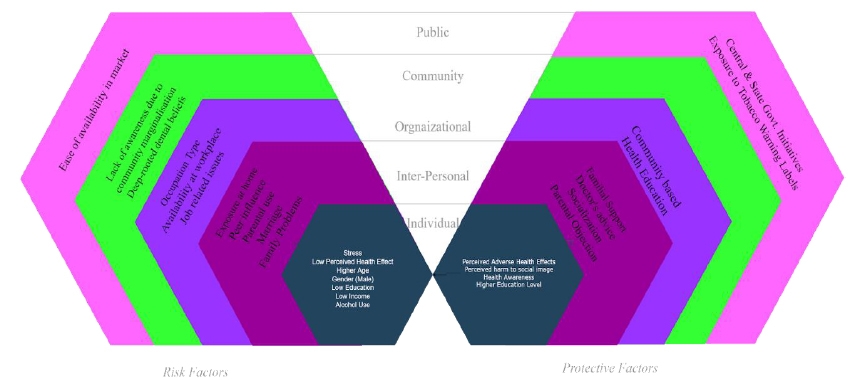
The data extracted from the eligible studies were: the first author's surname, year of publication, research location, study design, sample size, major risk factors identified, major protective factors identified, and the levels per the socio-ecological framework. Table 1 shows the study characteristics of eligible studies, and the extracted data are shown in Tables 2 and 3. Table 2 shows the major risk factors of tobacco use and Table 3 shows the major protective factors of tobacco use. The narrative synthesis of the identified risk factors and protective factors was done according to the socio-ecological framework, and the identified factors have been illustrated in Fig. (2). Risk and protective factors of tobacco use among South Indian adults from a socio-ecological Framework.
| S.No. | Author & Year | Location | Sample Size | Study Design |
|---|---|---|---|---|
| 1 | Veeraiah et al.,2020 | Tamil Nadu | Quantitative=555 Qualitative interview= 26 |
Sequential explanatory mixed-methods design |
| 2 | Karuveettil et al.,2020 | Kerala | Interview=15 FGD=2 groups |
Ethnography (Qualitative) |
| 3 | Bhaumik et al.,2019 | Kerala | 21 | Qualitative study |
| 4 | Shetty et al.,2017 | Karnataka | 450 | Cross-sectional study |
| 5 | Patel et al.,2016 | Karnataka | 372 | Cross-sectional study |
| 6 | Corsi et al.,2014 | Andhra Pradesh | 4534 | Survey |
| 7 | Kumar et al.,2011 | Karnataka | 333 | Cross-Sectional study |
| 8 | Jodalli & Panchmal, 2019 | Karnataka | 802 | Cross-Sectional study |
| 9 | Menon et al.,2020 | Kerala | 5784 | Survey |
| 10 | Prabhu et al.,2014 | Karnataka | 200 | Cross-sectional study |
| 11 | Francis,2017 | Tamil Nadu | 400 | Cross-sectional study |
| 12 | Francis,2018 | Tamil Nadu | 259 | Cross-sectional study |
| 13 | Mallikarjun et al.,2014 | Karnataka | 263 | Cross-Sectional study |
| S.No | Author & Year | Location | Study Design | Major Risk Factors Identified | Level as per Socio-ecological Framework |
|---|---|---|---|---|---|
| 1 | Veeraiah et al.,2020 | Tamil Nadu | Sequential explanatory mixed-methods design | Stress, low perceived health effects, Exposure to smoke at home Peer/Social influence, ease of availability |
Individual, interpersonal, public |
| 2 | Karuveettil et al.,2020 | Kerala | Ethnography (Qualitative) | Parental influence, peer pressure, marriage, availability of tobacco at the workplace, lack of awareness due to community marginalization, Perceived health benefits |
Individual, Interpersonal, community, organizational |
| 3 | Bhaumik et al.,2019 | Kerala | Qualitative study | Stress, nature of occupation, availability at workplace, peer influence | Individual, interpersonal, organizational |
| 4 | Shetty et al.,2017 | Karnataka | Cross-sectional study | Stress, Nature of occupation, tobacco use by family members, age (higher) | Individual, interpersonal, organizational |
| 5 | Patel et al.,2016 | Karnataka | Cross-sectional study | Stress, Gender(male) Peer influence, Parental tobacco use | Individual and Interpersonal |
| 6 | Corsi et al.,2014 | Andhra Pradesh | Survey | Low education, low income, occupation type (unskilled manual occupation) | Individual and organizational |
| 7 | Kumar et al.,2011 | Karnataka | Cross-Sectional study | Lack of knowledge about health effects of tobacco use, Peer pressure, Parental tobacco use |
Individual and interpersonal |
| 8 | Jodalli & Panchmal, 2019 | Karnataka | Survey | Lower economic status | Individual |
| 9 | Menon et al.,2020 | Kerala | Survey | Gender(male), alcohol use, course level characteristics | Individual and organizational |
| 10 | Prabhu et al.,2014 | Karnataka | Cross-sectional study | Peer pressure, family problems, financial drawbacks, stress and job related issues | Individual, interpersonal and organizational |
| 11 | Francis,2017 | Tamil Nadu | Cross-sectional study | Stress reduction, nature of occupation | Individual and organizational |
| 12 | Francis,2018 | Tamil Nadu | Cross-sectional study | lack of awareness about oral health, deep rooted dental beliefs in the community |
Individual and community |
| S. No | Author& Year | Location | Study Design | Major Protective Factors | Level as per Socio-ecological Framework |
|---|---|---|---|---|---|
| 1 | Veeraiah et al.,2020 | Tamil Nadu | Sequential explanatory mixed-methods design | Perceived adverse health effects, Perceived harm to social image, Support from family, health advice from doctor |
Individual, interpersonal |
| 2 | Karuveettil et al.,2020 | Kerala | Ethnography (Qualitative) | Socialization, health awareness | Individual and interpersonal |
| 3 | Bhaumik et al.,2019 | Kerala | Qualitative study | Perceived shame about behaviour, Central and state government awareness initiatives | Individual and public |
| 5 | Patel et al.,2016 | Karnataka | Cross- sectional study | Health education, parental objection(influence) | Interpersonal and Community |
| 6 | Mallikarjun et al.,2014 | Karnataka | Cross-Sectional study | Higher education level, exposure to tobacco warning labels | Individual and public |
3. RESULTS
3.1. Characteristics of the Eligible Studies
13 articles are included in this systematic review with a sample size of participants ranging from 15-5784. Of these, six were conducted in Karnataka, three in Tamil Nadu, three in Kerala and one in Andhra Pradesh. No studies matching the inclusion criteria of the current review were found from the remaining southern state of Telangana. Table 1. shows the details of included study characteristics. (Table 1 study charac-teristics of eligible studies).
The review findings organized the risk and protective factors of tobacco use as per the socio-ecological framework into five major domains: individual, interpersonal, organizational, community and public. A summary of risk and protective factors identified as per the framework has been depicted in Fig. (2). Risk and protective factors of tobacco use among South Indian adults from a socio-ecological Framework.
3.2. Individual Level
Six studies identified stress as the major risk factor influencing tobacco use behaviour [18-23]. Lack of knowledge about the health effects of tobacco use is also a major risk factor identified in this review [18, 24-26]. Lower education levels and low economic status are other individual-level risk factors identified in the current review [5, 22, 27]. Two studies reported gender as a significant individual-level risk factor influencing tobacco use and reported that males are more involved in tobacco use [21, 28]. One of the studies reported that alcohol use is also a major risk factor influencing tobacco use [28]. Another study identified that higher age also acts as a risk factor influencing individuals’ tobacco use [20].
3.3. Interpersonal Level
Peer pressure is the commonly identified risk factor among the interpersonal level risk factors influencing tobacco use [18, 19, 21, 22, 25]. Tobacco use by family members and exposure to second-hand smoke at home are also important interpersonal-level risk factors identified [18, 20, 21, 24, 25]. One study reported that family problems are another risk factor influencing individuals’ engagement in tobacco use [22]. A community-based study conducted in Kerala found that after marriage male partners influence tobacco use initiation among females [24].
3.4. Organizational Level
The major organizational-level risk factors of tobacco use found from this review are ease of availability of tobacco at the workplace [18, 19, 24], nature of occupation [19, 20, 23, 27] and job-related issues [22]. A study conducted among college students by Menon et al.,2020 found that course-level characteristics influence tobacco use [28].
3.5. Community Level
Two studies, both of which were community-based, included in the present review identified two community-level risk factors influencing tobacco use. Lack of awareness due to community marginalization is a major risk factor influencing tobacco use, and deep-rooted beliefs among specific communities regarding the positive effect of tobacco use on oral health act as a major risk factor for tobacco use [24, 26].
3.6. Public Level
One study identified the ease of availability of tobacco products as a potential public level risk factor influencing tobacco use [18].
Five studies that met the current study's inclusion criteria identified the major protective factors influencing tobacco use among South Indian adults [18, 19, 21, 24, 29]. Organizational-level protective factors were not identified in any of the included studies.
3.7. Individual Level
The major individual-level protective factors include individuals’ perceived awareness about the adverse health effects of tobacco use [18, 24] and perceived harm to social image [18].
3.8. Interpersonal Level
Two studies reported parental objection towards tobacco use and family support as the major interpersonal level protective factors [18, 21]. Socialization and health advice from doctors also act as protective factors helping individuals refrain from tobacco use [18].
3.9. Community Level
Health education in the community, especially among marginalized communities, is a major community-level protective factor influencing tobacco use [21].
3.10. Public Level
Tobacco warning labels and exposure to it are among the public level protective factors found in this review [29]. Further, the central and state government awareness initiatives were also identified as a potential public level protective factor in helping individuals refrain from tobacco use [19].
4. DISCUSSION
To the best of our knowledge, the current review is the first systematic study conducted to identify the risk and protective factors influencing tobacco use among South Indian adults. The findings are in light of the increasing prevalence of tobacco use in the Southern regions of India and the urgent need to explore the risk and protective factors of tobacco use among the sub-groups of the population with higher prevalence [30]. According to the socio-ecological model, the major domains under which the risk and protective factors were explored were: individual, interpersonal, organizational, community and public. Stress, lack of knowledge about the health effects of tobacco, lower education level and economic status, male gender, higher age and alcohol use were identified as major risk factors within the intrapersonal domain, whereas the protective factors found were individual’s perceived awareness of the adverse health effects of tobacco use and perceived harm to social image [5, 18-28]. These findings highlight the necessity for tobacco control measures targeting people from different social backgrounds who are more prone to tobacco use behaviour and for awareness campaigns that are accessible to people from all social strata.
Peer pressure is the most compelling risk factor influencing tobacco use within the interpersonal domain, along with exposure to second-hand smoke at home due to other family members’ tobacco consumption and other family problems [18-22, 24]. Findings from a community-based study in the Wayanad district of Kerala state found that marriage accounts for the initiation of tobacco use behaviour among females because of their partners’ influence [24]. This results from the sociocultural acceptability of tobacco use and the significant interpersonal influence of partners who use tobacco. Therefore, through family-level health awareness promotion, it is necessary to limit these degrees of influence and exposure to second-hand smoke at home.
Within the interpersonal domain, the major protective factors safeguarding individuals from engaging in tobacco use were socialization, parental objection and family support [18, 21, 24]. Additionally, a study found that health advice from doctors and medical professionals is also a potential interpersonal-level protective factor [18]. The findings suggest the key role of interpersonal support as a major protective factor in helping individuals abstain from this health-risk behaviour. An incorporation between interpersonal factors like parental support and organizational factors like counselling services provided by schools and the workplace needs to be encouraged to help people avoid engaging in this health risk behaviour.
Workplaces where there is the ease of availability of tobacco act as a significant risk factor for employees to engage in tobacco use [18, 19, 24]. It is also observed that cab drivers and unskilled manual workers engage more in tobacco use because of their perceived notion that tobacco use could help them stay up late for work and enhance their performance [19, 20, 23, 27]. Education about the negative health effects of prolonged tobacco use should be provided to help these groups of workers overcome this belief. According to the findings, people's tobacco usage may also be influenced by issues at work [22]. A better approach to overcome this risk factor would be to identify the primary causes of work-related concerns, manage those issues, and promote workplace tobacco reduction measures. Another interesting finding from the review is the result of a study conducted among college students in Kerala, which identified that engagement in tobacco use differs according to the course characteristics or discipline—art stream students showing more involvement in initiating than science stream students [28]. This difference could be explained by factors like the distinct subculture of disciplines, distinctive work-life interchange, lax oversight, opportunities for tobacco exposure, and differences in academic and recreational pursuits. Health risk awareness should be mandatory at the institutional level, irrespective of the discipline, with the help of faculties as behavioural change models for students.
Studies suggesting organizational-level protective factors were not found from the review. The overall evaluation of the risk factors found at this level suggests the implementation of tobacco control techniques at work and raising awareness among those in the professions more susceptible to this risky behaviour.
Two community-based studies included in the review found evidence for the community-level risk factors influencing tobacco use behaviour. Marginalized communities are often deprived of awareness regarding the health hazards of tobacco use, and certain communities have a deep-rooted belief that tobacco use can relieve toothache [24, 26]. Providing health education at the community level is a significant protective factor that reflects the need to tailor community-specific interventions incorporating health education to help communities lacking proper health knowledge regarding tobacco use hazards [21]. Policymakers and healthcare providers should focus on increasing the health literacy of marginalized groups and communities with deep-rooted dental health beliefs.
The general public's accessibility to tobacco products remains a significant risk factor, despite the implementation of tobacco control policies at the public level [18]. The factors identified as protecting people from tobacco use behaviour at a public level include tobacco warning labels on tobacco goods and central and state government awareness programs [19, 29]. Thus, this result indicates the necessity of implementing strict tobacco control policies at the public level and monitoring the existing policies and initiatives to tackle the nationwide health burden of tobacco and thereby improve the health status of the public.
LIMITATIONS
The inclusion of articles was restricted to journal articles, and other findings from national survey reports, commentaries, articles in any regional languages and dissertations were not considered. This might have led to missing out on some information relevant to the topic under study. The heterogeneity of the included articles in terms of research designs can also be viewed as a limitation of this systematic review.
CONCLUSION AND FUTURE DIRECTIONS
The review identified significant findings with respect to a few community-level practices and beliefs existing in South India with respect to tobacco use. The findings imply the need for large-scale tobacco control measures at multiple levels of influence. Future studies can explore how protective factors at each level of the socio-ecological framework could effectively manage the identified major risk factors. Further studies could also focus on age-specific and community-specific exploration of risk factors while developing intervention techniques. Improving health literacy among South Indian adults with respect to health risk behaviours should also be targeted. Policymakers could consider the results from the current study while implementing tobacco control strategies specific to the South Indian context in the future.
AUTHORS’ CONTRIBUTIONS
MD has contributed to the study design, extraction, screening. analysis of the articles and writing the manuscript. ER supervised the review, contributed to the finalization of articles, quality assessment of articles and editing of the manuscript. AJG has contributed to the research methods, revision of manuscript content and organization. RJ has contributed to the supervision, finalization of articles and manuscript content.
CONSENT FOR PUBLICATION
Not applicable.
STANDARDS OF REPORTING
PRISMA guidelines and methodology were followed.
FUNDING
None.
CONFLICT OF INTERESTS
The authors declare that they have no conflict of interest to disclose.
ACKNOWLEDGEMENTS
Declared none.
SUPPLEMENTARY MATERIAL
PRISMA checklist is available as supplementary material on the publisher’s website along with the published article.

