All published articles of this journal are available on ScienceDirect.

Alcohol Consumption, Physical Activity, and CAD Risk Factors in Firefighters
Abstract
Introduction:
Firefighting is a physically and psychologically stressful occupation, where firefighters often resort to alcohol use as a coping strategy. Firefighters are particularly vulnerable to alcohol misuse and alcohol disorders, negatively affecting their health, well-being and, possibly, work performance. Therefore, this study investigated the prevalence of alcohol consumption and its relationship with the participants’ sociodemographic characteristics, weekly physical activity, and coronary artery disease (CAD) risk factors.
Methods:
This study used a quantitative, cross-sectional and descriptive design. A total of 124 full-time firefighters, males and females, were conveniently recruited from the City of Cape Town Fire and Rescue Service, South Africa, between September to November, 2020. Firefighters were then separated according to sex, age, ethnicity, and CAD risk factors. Mann-Whitney U and Kruskal-Wallis H were used to determine the statistical differences between groups, Kendall’s Tau was used to assess the correlation between ordinal and continuous variables, and Chi-square to assess the association between categorical variables. A p-value of less than 0.05 was used to indicate statistical significance.
Results:
In the present study, 72.6% (n = 90) of firefighters reported consuming alcohol, of which 75.5% (n = 74) were male and 61.5% (n = 16) were female. Of this total, 40.0% (n = 44) reported that they consumed a variety of alcoholic beverages, 32.2% (n = 36) consumed beers mainly, 14.4% (n = 16) consumed spirits mainly, and 13.3% (n = 15) consumed wines mainly. In addition, 21.1% (n = 19) were categorised as moderate drinkers and 10% (n = 9) as heavy drinkers. The overall volume of alcohol consumption was significantly different between sexes and ethnicities (p <0.05). In addition, the volume of alcohol consumption was significantly associated with sex, ethnicity, total low-intensity physical activity minutes, diastolic blood pressure, and hypertension (p = 0.005). Sex (p = 0.021) and ethnicity (p = 0.042) were significantly associated with alcohol type. The volume of alcohol consumption was a significant predictor of total low-intensity physical activity, as well as systolic (p = 0.048) and diastolic blood pressures (p = 0.036).
Conclusion:
The majority of firefighters consumed alcohol, preferred a variety of alcoholic beverages and were classified as light drinkers. Younger male firefighters consumed more alcohol than females and were more likely to be categorized as heavy drinkers. Alcohol consumption was significantly associated with sex, ethnicity, physical activity, and hypertension. Educational programs to mitigate alcohol consumption should be implemented as a preventative measure in the fire service, especially among young male firefighters.
1. INTRODUCTION
Firefighting is a physically and psychologically stressful occupation, where firefighters are routinely exposed to hazardous environments, harmful chemicals and fumes. Firefighters are often the first responders to traffic collisions and are required to make life or death decisions and, sometimes, to perform emergency resuscitation [1-4]. Due to the hazards and stress related to the profession, firefighters are particularly vulnerable to alcohol abuse and alcohol-related disorders, which places an additional burden on an already high-risk occupational group [4-7].
Over fifty percent of firefighters reported excessive alcohol use and often indulged in periodic binge drinking [6]. Studies reported that alcohol use was significantly related to post-traumatic stress disorders (PTSDs) in firefighters and was often used as a coping mechanism to deal with occupational stressors [1-6]. However, firefighters also engaged in social drinking as part of an acculturated social system because of the emotional support and social acceptance by their peers [8-10]. Regardless of the reason for indulging in alcohol consumption, the behaviour was often coupled with cigarette smoking that collectively presented an increased health risk for developing obesity, hypertension and cardiometabolic disease [4, 6, 8-12]. Moreover, heavy or binge alcohol consumption was associated with post-episodic hangovers and lethargy that often resulted in physical inactivity [11] and sedentary behaviour [13]. Hazardous drinking is especially harmful and may be a catalyst for poor overall health and well-being [1, 7, 8]. Carey et al. [14] reported that younger firefighters (<40 years), specifically younger female firefighters, were more prone to binge drinking behaviour. However, as firefighters’ years of service increased, their likelihood of indulging in binge drinking episodes decreased [4]. Due to the camaraderie of firefighting, younger firefighters may feel pressured to engage in socially acceptable but risky behaviours, such as social drinking, in order to appease the older firefighters and be accepted as part of the professional group [4, 6, 14]. Studies conducted on firefighters in South Africa reported that firefighters’ were under severe psychological load, which resulted in firefighters routinely opting for unhealthy coping mechanisms [15, 16]. This may inadvertently contribute to the high development of cardiovascular disease in firefighters in the CoCTFRS [17].
In the City of Cape Town Fire and Rescue Service (CoCTFRS), poor exercise and dietary habits [18] were found to be associated with a high prevalence of coronary artery disease (CAD) risk factors [17]. Firefighters engaging in risky alcohol behaviour present an added health burden that generally adds to their overall CAD risk. Although studies have previously been published involving this dataset, the heavy alcohol use among these firefighters remains a major concern. Moreover, no research has been published on alcohol use in firefighters in the CoCTFRS. Previous studies have shown that firefighters in South Africa are rather busy, largely due to the high number of informal settlements and wildland firefighting [19, 20]. Firefighters often choose to destress by engaging in unhealthy lifestyle practices, one of which is the use of alcohol [16]. This study focuses on investigating the heavy alcohol use in this population, which may contribute to the overall deterioration in the firefighters’ cardiovascular health. Therefore, the aim of this study is to investigate the prevalence of alcohol consumption and its relationship with sociodemographic characteristics, weekly physical activity, and coronary artery disease risk factors in firefighters from the CoCTFRS. The authors hypothesised that with increased alcohol consumption, physical inactivity, both on-and-off duty, would increase, particularly in younger firefighters of mixed ethnicity. In addition, the authors hypothesized that alcohol consumption would be significantly related to CAD risk factors.
2. MATERIALS AND METHODS
This study used a quantitative, cross-sectional and descriptive design. A total of 124 full-time firefighters, males and females, were conveniently recruited from the CoCTFRS, South Africa, between September to November, 2020. At the time of data collection, there were roughly 950 firefighters permanently employed in the CoCTFRS, and using Slovin’s formula, a sample size of 274 firefighters was required. However, the sample number was limited by the CoCTRS due to concerns about work schedule interruption. For this study, full-time firefighters between the ages of 18 to 65 years from the CoCTFRS were recruited to participate in the study. Firefighters that were volunteers, part-time or on sick leave, were excluded from participating in the current study. The administrative staff was also excluded from participating.
Firefighters were approached directly at each individual fire station, where information about the study was provided to all participants, and thereafter, they gave written informed consent to participate in the study. The study protocol was approved by the Biomedical Research Ethics Committee (BMREC) at the University of the Western Cape (Ethics reference number: BM19/4/3). The study was also sanctioned by the chief fire officer of the City of Cape Town Fire and Rescue Service, as well as the director of Policy and Strategy of the City of Cape Town.
2.1. Research Procedures
A researcher-generated questionnaire was used to collect data on the demographic characteristics and lifestyle behaviours of firefighters, such as date of birth, sex, family history of CAD, cigarette smoking behaviour, and alcohol use. Ethnicity was self-reported by each participant, based upon the historical South African racial classification system, i.e., Black, mixed ethnicity, White, Indian, and other. The International Physical Activity Questionnaire (IPAQ) was used to measure occupational and weekly physical activity behaviour. The questionnaire is divided into multiple sections, namely, exercise in leisure time, transportation-related physical activity, domestic work-related physical activity, and occupation-related physical activity. The total physical activity, in minutes, was added up to determine the weekly physical activity of firefighters. The IPAQ has been shown to be a reliable questionnaire to determine the physical activity habits of individuals according to repeatability (r = 0.8) and content validity (r = 0.30). The questionnaire was self-administered; however, the researcher went through each question with all firefighters that volunteered to participate in order to reduce self-reporting errors from the firefighters.
Body mass was measured using a precision electronic scale, with the participant wearing minimal indoor clothing, and measured to the nearest 50 grams. Stature was measured using a portable stadiometer while standing barefoot, with the heels together, on a level plastic base. The heels, buttocks and upper back were aligned to the stadiometer rod, and the participant’s head was placed in the Frankfort plane [21]. Waist and hip circumferences were taken using a standard steel tape measure. The cross-hand technique was used for all measurements [21]. Waist circumference was measured at the point of the umbilicus [21], between the lower costal border and the top of the iliac crest, perpendicular to the long axis of the trunk. Hip circumference was taken at the level of the greatest posterior protuberance of the buttocks [21]. Waist and hip circumferences were measured to the nearest 0.1 cm at the end of normal expiration [21]. Blood pressure was measured using a standard blood pressure sphygmomanometer and stethoscope, with an adult-size blood pressure cuff and, where necessary, a larger cuff size was used for firefighters with larger upper arms. The standard auscultatory method of blood pressure measurement was used [21]. Total cholesterol and non-fasting blood glucose were measured using the standard prescribed finger-prick method and analysed with an AcuTrend® Plus GC meter. The research instruments used for data collection were calibrated prior to testing. A minimum test-retest reliability coefficient of 0.8 was required prior to the commencement of the study, and only one tester was used for data collection in the study [21].
2.2. Classification of Coronary Artery Disease Risk Factors
Age is defined as a risk factor for men aged 45 years or older and women aged 55 years or older [21]. Family history of heart disease is defined as myocardial infarction, coronary revascularization or SCD before the age of 55 years in the father or other male first-degree relative or before the age of 65 years in the mother or other female first-degree relative [21]. Hypertension is defined as resting systolic blood pressure (SBP) equal to or more than 140 mm Hg and/or resting diastolic blood pressure (DBP) equal to or more than 90 mm [21]. Obesity is defined as a body mass index (BMI) of 30 kg•m-2 or more. Cigarette smoking is defined as being a current cigarette smoker or having quit smoking within the last 6 months [21]. Central obesity is defined as a waist circumference (WC) of more than 102 cm for men and 88 cm for women [21]. Diabetes is defined as a non-fasting blood glucose concentration of 11.1 mmol•L-1 or above [21] or diagnosed by a medical doctor. Dyslipidemia is defined as a total serum cholesterol concentration equal to or above 5.18 mmol•L-1 [21]. Physical inactivity is defined as firefighters not participating in thirty minutes of moderate-intensity physical activity on three days of the week for at least three months consecutively [21].
2.3. Classification of Alcohol Consumption and Type and Physical Activity
Firefighters who consumed at least one alcoholic beverage per month were classified as alcohol consumers. When classifying alcohol consumption according to volume, firefighters who consumed 1 to 7 units of alcohol per week were rated as light drinkers, those with 8 to 14 units of alcohol per week as moderate drinkers, and those over 14 units of alcohol per week as heavy drinkers [22]. Alcoholic beverages were classified into beers or ciders mainly, wines, spirits only or mixed alcoholic beverages that encompassed a combination of two or more types of alcohol. One unit of beer or cider was classified as a regular 330 ml can/bottle, a unit of wine was classified as a standard glass of 150 ml, a unit of hard liquor (spirits) was classified as a standard shot of 44 ml, and mixed drinks encompassed all the aforementioned alcoholic units. Physical activity was measured based on the American College of Sports Medicine (ACSM) guidelines [21] and IPAQ [23]. Low-intensity physical activity was classified as firefighters not producing a sweat, moderate-intensity physical activity as light sweating and being able to hold a conversation while exercising, and vigorous-intensity physical activity as producing heavy sweating and the inability to converse. Total weekly physical activity encompassed all daily domestic activity, including occupational, recreational, and travel-related activity.
2.4. Analysis
All data were double-entered into a Microsoft Office Excel spreadsheet and then cleaned of errors. Thereafter, data were exported to the Statistical Package for the Social Sciences (SPSS) version 27 for descriptive and inferential data analysis. The normality of the data was assessed using the Shapiro-Wilks test, which indicated that the data were not normally distributed. Firefighters were classified based on sex, age, ethnicity and major CAD risk factors for data analysis. Mann-Whitney U and Kruskal-Wallis H were used to determine statistical differences between groups. When significant differences were found between groups, a Bonferroni correction was applied. Kendall’s Tau was used to assess the correlation between ordinal variables. The Chi-square test was used to assess the association between categorical variables. To ensure the normality of the data, the data was first case ranked and, secondly, transformed using the inverse DF (idf. normal) function in SPSS to ensure normality of the data. For variables that had a significant correlation, a linear regression was generated to predict physical activity and blood pressure in firefighters. For linear regression, the assumptions met are: (1) the data was continuous, (2) the data had a linear relationship, (3) there were no significant outliers, (3) observations were independent, (4) there was homoscedasticity, and (5) the residuals of the regression line were approximately normally distributed. Collinearity and autocorrelation were tested using the variance inflation factor (VIF) and the Durbin-Watson statistic, respectively. For VIF, values under 5.0 and a Durbin-Watson statistic between 1.5-2.5 were considered acceptable, indicating no collinearity and that the data was not autocorrelated. A P-P plot and scatter plot were used to visually assess the normality of the residuals and whether homoscedasticity was present. A p-value of less than 0.05 was used to indicate statistical significance.
3. RESULTS
The mean (X̅±SD) age of all the firefighters was 37.53±9.05 years, and mean body mass and stature were 87.4±17.9 kg and 172.6±7.3 cm, respectively. The majority of firefighters were male (79.1%), with mean age, body mass, and stature of 37.8±9.8 years, 87.8±18.5 kg, and 174.7±6.5 cm, respectively, whereas for females, mean age, body mass, and stature were 36.4±5.4 years, 85.9±16.2 kg, and 164.8±4.5 cm, respectively. When all participants were classified into age-group categories, the age-group 20-29 years represented 19.4% of the participants in the study, the age-group 30-39 years had the highest number of participants with 44.4%, the age-group 40-49 years had 24.2%, and the age group 50-65 years had the lowest number with 12.1%.
In the present study, 72.6% (n = 90) of firefighters reported that they consumed alcohol, the majority (40.0%, n =36) of firefighters reported that they consumed mixed alcoholic beverages, followed by 32.2% (n = 29) who consumed beers or ciders, 14.4% (n = 13) who consumed spirits, and 13.4% (n = 12) who consumed wines (Table 1). According to sex, 75.5% (n = 74) of male firefighters reported that they consumed alcohol, whereas 61.5% (n = 16) of female firefighters reported consuming alcohol, with most males consuming mixed drinks (45.9% vs. 18.9%). According to age group, in the age group 20-29 years, a total of 83.3% reported consuming alcohol; in the age group 30-39 years, 65.5% (n = 13) reported that they consumed alcohol and lastly, in the age group 50-65 years, 86.7% (n = 11) reported drinking alcohol. According to ethnicity, white firefighters had the highest prevalence of alcohol consumption, with 95.2% (n = 19), with 60% (n = 12) preferring to have mixed drinks. Firefighters of mixed ethnicity followed by 70.0% (n = 34) of firefighters consuming alcoholic beverages.
Based on firefighters presenting with multiple CAD risk factors, 82.8% (n = 20) of aged (≥45 years) firefighters consumed alcohol, 77.8% (n = 27) of obese firefighters consumed alcohol, 75.5% (n = 28) of cigarette smokers consumed alcohol, 80.5% (n = 26) of hypertensive firefighters consumed alcohol, 76.5% (n = 10) of physically inactive firefighters consumed alcohol, 72.0% (n = 26) of dyslipidemic firefighters consumed alcohol, 81.8% (n = 7) of diabetic firefighters consumed alcohol, with mixed drinks being preferred by all firefighters that had CAD risk factors present.
| - | Alcohol Use | Type of Alcohol | Volume of Alcohol Consumption | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variable | n | % | Beers/Ciders (%) | Wines (%) | Spirits (%) | Mixed (%) | Median | Interquartile range |
Units of Drink+ X̅±SD |
p |
| Total firefighters | 90 | 72.6 | 32.2 | 13.3 | 14.4 | 40.0 | 2.0 | 6.8 | 5.5±10.9 | |
| Sex | ||||||||||
| Male | 74 | 75.5 | 32.4 | 8.1 | 13.5 | 45.9 | 2.23 | 7.5 | 6.2±11.6 | 0.005** |
| Female | 16 | 61.5 | 31.3 | 37.5 | 12.5 | 18.9 | 1.0 | 4.3 | 2.6±6.9 | |
| Age-groups | ||||||||||
| 20-29 years | 20 | 83.3 | 40.0 | 20.0 | 10.0 | 30.0 | 1.3 | 7.1 | 9.9±20.8 | 0.920 |
| 30-39 years | 36 | 65.5 | 36.1 | 11.1 | 11.1 | 41.7 | 2.0 | 6.0 | 4.3±6.6 | |
| 40-49 years | 21 | 70.0 | 28.6 | 14.3 | 19.0 | 38.1 | 1.2 | 6.0 | 4.4±6.7 | |
| 50-65 years | 13 | 86.7 | 23.1 | 7.7 | 15.4 | 53.8 | 7.5 | 19.0 | 4.9±4.8 | |
| Ethnicity | ||||||||||
| Mixed ethnicity | 49 | 70.0 | 30.6 | 14.3 | 14.3 | 40.8 | 2.8 | 7.1 | 4.3±6.4 | 0.011* |
| Black | 21 | 65.6 | 52.4 | 19.0 | 4.8 | 23.8 | 0.8 | 4.5 | 3.6±5.9 | |
| White | 20 | 95.2 | 15.0 | 5.0 | 20.0 | 60.0 | 3.0 | 8.13 | 12.3±21.6 | |
| Total weekly physical activity | ||||||||||
| Low-intensity | 83 | 74.8 | 32.5 | 14.5 | 14.5 | 38.6 | 2.0 | 6.0 | 4.8±7.0 | |
| Moderate-intensity | 46 | 73.0 | 28.3 | 17.4 | 13.0 | 41.3 | 2.5 | 8.0 | 4.5±5.6 | |
| vigorous-intensity | 83 | 73.5 | 32.5 | 13.5 | 12.0 | 42.1 | 2.0 | 6.5 | 5.3±10.9 | |
| Occupational physical activity | ||||||||||
| Low-intensity | 78 | 75.7 | 33.3 | 14.1 | 11.5 | 41.0 | 2.0 | 6.0 | 4.7±6.6 | |
| Moderate-intensity | 3 | 50.0 | 0.0 | 0.0 | 33.3 | 33.3 | 0.5 | 12.6 | 5.3±8.6 | |
| Vigorous-intensity | 81 | 73.0 | 33.3 | 12.3 | 13.6 | 40.7 | 2.0 | 7.5 | 5.3±8.6 | |
| CAD risk factors# | ||||||||||
| Age | 24 | 82.8 | 25.0 | 8.3 | 20.8 | 45.8 | 4.0 | 9.0 | 5.3±7.1 | 0.859 |
| Obesity | 35 | 77.8 | 34.3 | 17.1 | 14.3 | 34.3 | 2.0 | 7.3 | 4.6±6.1 | |
| Central obesity | 36 | 78.3 | 30.5 | 16.7 | 16.7 | 36.1 | 2.0 | 7.1 | 4.4±5.9 | |
| Cigarette smoking | 37 | 75.5 | 32.4 | 5.4 | 21.6 | 40.5 | 3.0 | 8.5 | 7.2±15.1 | |
| Hypertension | 33 | 80.5 | 42.4 | 9.1 | 12.1 | 36.4 | 4.0 | 7.0 | 6.4±8.7 | |
| Physical inactivity | 13 | 76.5 | 23.1 | 23.1 | 30.8 | 23.1 | 1.5 | 6.3 | 4.4±8.5 | |
| Dyslipidemia | 36 | 72.0 | 41.7 | 11.1 | 11.1 | 36.1 | 2.0 | 6.0 | 5.3±14.2 | |
| Diabetes | 9 | 81.8 | 22.2 | 0.0 | 22.2 | 55.6 | 4.0 | 11.5 | 6.4±9.1 | |
+ One unit of beer or cider was classified as a regular 330 ml can/bottle, a unit of wine was classified as a standard glass of 150 ml wine, and a unit of hard liquor (spirits) was classified as a standard shot of 44 ml.
#indicates alcohol consumption according to the presence of various CAD risk factors.
3.1. Volume of Alcohol Consumption in Firefighters
The mean (X̅±SD) alcohol consumption per week was 5.5±10.9 units in all firefighters. In male firefighters, the mean volume of alcohol consumption was 6.2±11.6 units compared to 2.6±6.9 units for female firefighters, which was statistically significant (p = 0.005). The mean volume of alcohol consumption was similar in firefighters of mixed ethnicity at 4.3±6.4 units and 3.6±5.9 units in Black firefighters but much higher at 12.3±21.6 units in White firefighters, which was statistically significant (p = 0.011).
The mean (X̅±SD) volume of alcohol consumption for aged, obese, centrally obese, cigarette smokers, hypertensive, physically inactive, dyslipidemic and diabetic firefighters were 5.3±7.1, 4.6±6.1, 4.4±5.9, 7.2±15.1, 6.4±8.7, 4.4±8.5, 5.3±14.2, and 6.4±9.1 units, respectively. There were no significant differences in the volume of alcohol consumption by firefighters based on the number of CAD risk factors. After applying a Bonferroni correction, there was a significant difference in alcohol consumption between Black and White firefighters (p = 0.004) and between firefighters of mixed ethnicity and White firefighters (p = 0.006).
3.2. Pattern of Alcohol Consumption in Firefighters
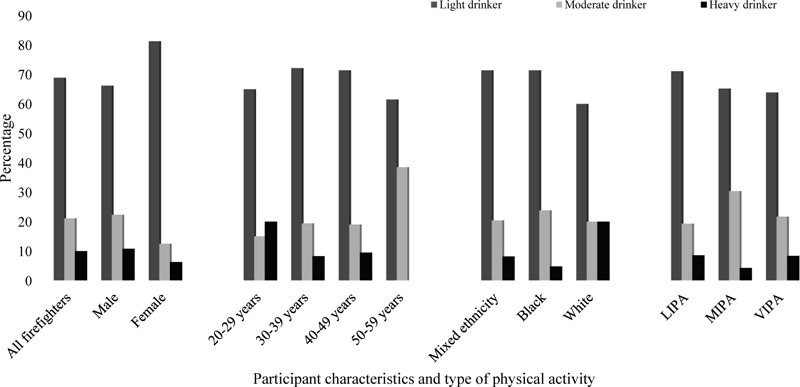
Fig. (1), the majority of firefighters (68.9%, n = 62) were classified as light drinkers, 21.1% (n = 19) as moderate drinkers, and 10.0% (n = 9) as heavy drinkers. According to gender, 66.2% (n = 49) of males and 81.3% (n = 13) of females were classified as light drinkers, 22.3% (n = 4) of males and 12.5% (n = 2) of females as moderate drinkers, and 10.8% (n = 8) of males and 6.3% (n = 1) of females as heavy drinkers. According to age, the age-group 20-29 years had the highest prevalence of being heavy drinkers with 20.0% (n = 4), followed by the age-group 40-49 years with 9.5% (n = 3) as heavy drinkers. According to ethnicity, White firefighters were most likely to be heavy drinkers with 20.0% (n = 4), followed by mixed ethnicity firefighters with 8.2% (n = 4) and Black firefighters with 4.8% (n = 1), the lowest. Considering the type of weekly physical activity, among firefighters who engaged in low-intensity physical activity and vigorous-intensity activity, alcohol consumption was highest at 8.6% (n = 7) and 8.4% (n = 7), respectively. However, in firefighters that engaged in moderate-intensity activity, the highest prevalence of moderate drinkers was present, with 30.4% (n = 14).
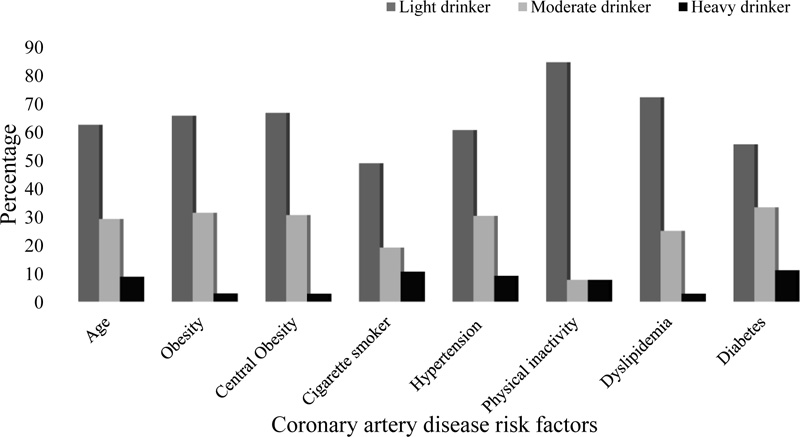
According to CAD risk factors, 8.8% of aged firefighters were rated as heavy drinkers, 2.9% of obese firefighters were rated as heavy drinkers, 2.8% of centrally central obesity firefighters were rated as heavy drinkers, 10.6% of firefighters who were cigarette smokers were rated as heavy drinkers, and 9.1% of hypertensive firefighters were rated as heavy drinkers. There were zero heavy drinkers in firefighters that were physically inactive. Of dyslipidemic firefighters, 2.8% were rated as heavy drinkers, and 11.1% of diabetic firefighters were rated as heavy drinkers (Fig. 2).
There was a significant strong positive correlation between alcohol consumption and the type of alcoholic beverage consumed by firefighters (rτ = 0.721, p <0.001), and a significant strong positive correlation between the amount of low-intensity occupational, physical activity and the total amount of weekly low-intensity physical activity (rτ = 0.834, p <0.001), and a significant moderate positive correlation between alcohol consumption and the volume of alcohol consumption (rτ = 0.669, p <0.001) were reported (Table 2). There was a significant weak positive correlation between alcohol consumption and the total amount of low-intensity physical activity (rτ = 0.168, p = 0.017). There was a significant moderate positive correlation between the type of alcoholic beverage and the volume of alcohol consumption (rτ = 0.491, p <0.001) and between the type of alcoholic beverage and the pattern of alcohol consumption (rτ = 0.564, p <0.001). There was a significant weak positive correlation between the volume of alcohol consumption and sex (rτ = 0.218, p = 0.002), between the volume of alcohol consumption and the total amount of low-intensity physical activity (rτ = 0.168, p = 0.007), between the volume of alcohol consumption and systolic blood pressure (rτ = 0.118, p = 0.034), between the volume of alcohol consumption and diastolic blood pressure (rτ = 0.143, p = 0.015), and between the volume of alcohol consumption and hypertension (rτ = 0.127, p = 0.049). There was a significant weak positive correlation between the pattern of alcohol consumption and sex (rτ = 0.150, p = 0.038), between the pattern of alcohol consumption and the total amount of low-intensity physical activity (rτ = 0.231, p = 0.001), and between the pattern of alcohol consumption and hypertension (rτ = 0.150, p = 0.038). There was a significant weak positive correlation between sex and systolic blood pressure (rτ = 0.138, p = 0.034), and between sex and diastolic blood pressure (rτ = 0.148, p = 0.028). There was a significant weak positive correlation between the total amount of vigorous-intensity physical activity and systolic blood pressure (rτ = 0.116, p = 0.039) and between the total amount of vigorous-intensity physical activity and diastolic blood pressure (rτ = 0.113, p = 0.046). There was a significant weak positive correlation between the amount of low-intensity occupational, physical activity and pattern of alcohol consumption (rτ = 0.147, p = 0.030) and between the amount of low-intensity occupational, physical activity and the total amount of weekly vigorous-intensity physical activity (rτ = 0.207, p = 0.002).
| - | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Alcohol consumption | - | - | - | - | - | - | - | - | - | - | - |
| Type of alcoholic beverage | 0.721** | - | - | - | - | - | - | - | - | - | - |
| Volume of alcohol consumption | 0.669** | 0.491** | - | - | - | - | - | - | - | - | - |
| Pattern of alcohol consumption | 0.785** | 0.564** | 0.837** | - | - | - | - | - | - | - | - |
| Sex | 0.127 | 0.157* | 0.218** | 0.150* | - | - | - | - | - | - | - |
| Total low-intensity physical activity | 0.168* | 0.104 | 168** | 0.231** | -0.007 | - | - | - | - | - | - |
| Total moderate-intensity physical activity | -0.031 | -0.014 | 0.027 | 0.059 | -0.038 | -0.051 | - | - | - | - | - |
| Total vigorous-intensity physical activity | -0.027 | 0.011 | 0.027 | 0.033 | 0.052 | 0.055 | 0.049 | - | - | - | - |
| Low-intensity occupational, physical activity | 0.093 | 0.056 | 0.109 | 0.147* | 0.006 | 0.834** | -0.048 | 0.207** | - | - | - |
| Systolic blood pressure | 0.075 | 0.048 | 0.118* | 0.095 | 0.138* | -0.039 | 0.087 | 0.116* | -0.052 | - | - |
| Diastolic blood pressure | 0.117 | 0.072 | 0.143* | 0.119 | 0.148* | -0.005 | 0.030 | 0.113* | -0.010 | 0.579** | - |
| Hypertension | 0.125 | 0.035 | 0.127* | 0.150* | 0.067 | -0.002 | 0.078 | 0.008 | -0.054 | 0.528** | 0.548** |
1 – alcohol consumption, 2 – type of alcoholic beverage, 3 – volume of alcohol consumption, 4 – pattern of alcohol consumption, 5 – sex, 6 – total low-intensity physical activity, 7 – total moderate-intensity physical activity, 8 – total vigorous-intensity physical activity, 9 – low-intensity occupational physical activity, 10 – systolic blood pressure, 11 – diastolic blood pressure.
| Variable | Sex | Ethnicity | ||||
|---|---|---|---|---|---|---|
| χ2 | df | p | χ2 | df | p | |
| Alcohol consumption | 2.0 | 1 | 0.156 | 9.0 | 3 | 0.028* |
| Pattern of alcohol consumption | 3.2 | 3 | 0.356 | 12.8 | 9 | 0.170 |
| Alcohol type | 11.5 | 4 | 0.021* | 21.6 | 12 | 0.042* |
| Volume of Alcohol Consumption | ||||
|---|---|---|---|---|
| Model: | β | R2 | F | p |
| Low-intensity physical activity | 22.77 | 0.06 | 7.6 | 0.007** |
| Moderate-intensity physical activity | 0.00 | -0.01 | 0.247 | 0.621 |
| High-intensity physical activity | 0.00 | -0.01 | 0.3 | 0.572 |
| Age | -0.04 | 0.03 | 0.4 | 0.530 |
| Body mass index | -0.40 | 0.01 | 0.1 | 0.71 |
| Waist circumference | 0.01 | 0.00 | 0.1 | 0.808 |
| Systolic blood pressure | 0.40 | 0.03 | 3.9 | 0.048* |
| Diastolic blood pressure | 0.33 | 0.04 | 4.5 | 0.036* |
| Total cholesterol | -0.81 | 0.01 | 1.5 | 0.217 |
| Non-fasting blood glucose | -0.08 | -0.01 | 0.1 | 0.780 |
There was a significant association between alcohol consumption and ethnicity (p = 0.028), where more White firefighters consumed alcohol than Black and mixed-ethnic firefighters. There was a significant association between alcohol type and gender (p = 0.021) and between alcohol type and ethnicity (p = 0.042). Males preferred drinking mixed drinks, especially White firefighters (Table 3).
In Table 4, the volume of alcohol consumption was a significant predictor of the total amount of low-intensity physical activity (R2 = 0.06, p = 0.007). The volume of alcohol consumption explained 6% of the variance in the total amount of low-intensity physical activity of firefighters. In addition, for every one-unit increase in alcohol consumed, the firefighters were more likely to engage in low-intensity physical activity.
The volume of alcohol consumption was a significant predictor of systolic blood pressure (R2 = 0.03, p = 0.048). The volume of alcohol consumed explained 3% of the variance in systolic blood pressure. For every one-unit increase in alcohol consumed, systolic blood pressure increased by 0.4 mm Hg. The volume of alcohol consumption was also a significant predictor of diastolic blood pressure (R2 = 0.04, p = 0.036). The volume of alcohol consumed explained 4% of the variance in diastolic blood pressure. For every one-unit increase in alcohol consumed, diastolic blood pressure increased by 0.3 mm Hg.
4. DISCUSSION
Alcohol consumption, particularly hazardous alcohol consumption, is a concern in firefighters that many researchers have investigated due to the physically and psychologically demanding nature of the occupation [1, 8, 9]. Studies have shown that many firefighters consume alcohol socially as a mood enhancer and as a coping strategy for work-related stress [3, 6, 14]. More importantly, many male firefighters have a significantly higher prevalence of hazardous drinking behaviour than other male workers [24]. Previous research indicated that many firefighters consume excessive amounts of alcohol as a coping mechanism for their mental stress, such as post-traumatic stress disorders (PTSDs) [2, 3, 5, 14]. The hazardous alcohol consumption may contribute to additional health concerns in firefighters, who are already burdened by a high prevalence of premature morbidity and mortality due to the presence of multiple CAD risk factors precipitated by lifestyle and work-related challenges [2, 5, 14, 25, 26].
In the present study, 72.6% of firefighters reported consuming alcohol, of which 75.5% were male, and 61.5% were female. Jitnarin et al. [12] reported a high proportion (82.9%) of firefighters who consumed alcohol, while Piazza-Gardener et al. [4] and Eastlake et al. [27] reported even higher proportions of firefighters who consumed alcohol, at 89% and 98.7%, respectively. Likewise, Li et al. [28] reported that the high prevalence of alcohol consumption was similar between male and female firefighters, with females having a marginally higher prevalence (91% vs. 89%). In strong contrast, Vinnikov et al. [29] reported that 40% of men and 42% of women firefighters were drinkers. Possible explanations for the differences in alcohol consumption may be related to the different workloads placed on firefighters across various fire departments depending on their locations or differences in the mean ages of firefighters between the various cohorts [1-4].
The results indicated that 68.9% of firefighters were classified as light drinkers, 21.1% as moderate drinkers, and 10% as heavy drinkers. Another study also reported that 10.9% of firefighters were heavy alcohol consumers [30]. Similarly, Angleman et al. [31] reported that 71.3% of firefighters were classified as light drinkers, 18.4% as moderate drinkers, and much fewer (4.6%) as heavy drinkers. However, Donovan et al. [22] reported that a higher proportion (81%) of firefighters were light drinkers, with fewer (10%) as moderate drinkers and even fewer (1%) as heavy drinkers. Compared to the study by Donovan et al., the present study had a similar proportion of light drinkers but much higher proportions of moderate and heavy drinkers. In strong contrast, Choi et al. [25] reported that 86.7% of their cohort of firefighters were classified as either moderate or heavy alcohol consumers. The higher proportion of moderate and heavy drinkers in the current study may be due to the high psychological load that firefighters face in South Africa and the unhealthy coping mechanism they often opt for [15, 16].
Keith et al. [2] reported that the average consumption of alcohol was 36.2 alcoholic beverages per month, compared to a monthly average of 22 alcoholic beverages in the present study. However, Cape Town firefighters preferred consuming mixed drinks, which may underestimate their overall alcoholic consumption due to different methods of recording alcohol consumption, as suggested by Keith et al. [2]. The study by Keith et al. also reported that over 85% of firefighters consumed alcohol, 44.7% drank to excess, and 32% engaged in episodic binge drinking [2]. Moreover, beers were most frequently consumed, followed by spirits and wine. Smith et al. [3] reported that 31.0% of firefighters drank 2 to 4 times a month, 28.2% drank 2 to 3 times a week, and 13.1% drank 4 or more times a week, with 23.3% classified as hazardous drinkers. Kim et al. [32] noted that 45.8% of firefighters were classified as problem drinkers. Consumption of beer and spirits has been shown to increase the risk of cardiovascular disease [33], which is particularly worrying in this population, given the physical nature of their work and high cardiovascular-related mortality [34, 35]. Although firefighting is a physically strenuous occupation, studies suggest that many firefighters indulge in unhealthy lifestyle practices as a coping mechanism, which may account for the high prevalence of alcohol consumption and heavy or hazardous drinking among firefighters [1-4].
According to gender, more male than female firefighters were found to be drinkers (75.5% vs. 61.5%), with more males likely to be moderate and heavy drinkers. Males preferred consuming mixed drinks (45.9%), and females preferred wines (37.5%). In addition, there was a relationship between sex and volume of alcohol consumption, sex and pattern of alcohol consumption, and sex and alcohol type. Carey et al. [14] reported that binge drinking was more prevalent in female than male firefighters (80% vs. 57%); however, male firefighters indulged in more hazardous drinking (0% vs. 15%). In contrast, Muegge et al. [36] found that there was a significant difference in binge drinking habits, where males were more likely to binge drink compared to females (40.2% vs. 25.8%). However, Gallyer et al. [10] reported that problematic drinking was similar between men (63.0%) and women (64.2%), with both being higher when compared to the general population.
When investigating the age group, the youngest (83.3%) and oldest (86.7%) groups of firefighters reported the highest prevalence of alcohol consumption, whereas the age-group 30-39 years had the lowest prevalence of alcohol consumption (65.5%). Likewise, Goh et al. [37] reported a significant difference in risky alcohol use based on age and seniority level in firefighters, with the younger ranked firefighters more likely to participate in risky alcohol use compared to the older firefighters. Younger firefighters had a lower prevalence of heavy drinking than older firefighters. Younger firefighters preferred drinking beers or ciders, whereas other age groups preferred consuming mixed drinks. Younger firefighters tended to engage in more unhealthy and reckless behaviours, such as hazardous drinking, drunk driving and cigarette smoking, compared to older firefighters [12, 38-42]. Older firefighters may be more aware of their health status and the negative consequences of unhealthy behaviour, thereby accounting for the decrease in their alcohol consumption with age [27].
According to ethnicity, White firefighters had the highest prevalence of alcohol consumption (95.2%), along with firefighters of mixed ethnicity (70.0%), both of whom preferred to consume mixed alcoholic beverages, while Black firefighters had the lowest prevalence of alcohol consumption (65.6%), and preferred beers or ciders. Paulus et al. [9] and Smith et al. [8] reported that ethnicity was significantly related to the quantity of alcohol consumed by firefighters. Moreover, the current results showed that White firefighters had a significantly higher volume of alcohol consumption and were more likely to be heavy drinkers. Piazza-Gardner et al. [4] reported that firefighters’ race was a significant predictor of binge drinking, where White firefighters were 4.5 times more likely to engage in binge drinking. There was a significant association between alcohol consumption and ethnicity and between alcohol preference and ethnicity, where White firefighters were significantly more likely to consume alcohol and preferred to consume mixed alcoholic beverages. The study conducted by Carey et al. [14] reported a similar result, where White firefighters were significantly more likely to engage in binge drinking. Likewise, Poston et al. reported that ethnicity was a significant predictor of alcohol use and binge drinking [43].
When investigating the relationship between CAD risk factors and alcohol consumption, aged (≥45 years) firefighters were most likely to consume alcohol and preferred to consume mixed alcoholic beverages that predisposed them to develop hypertension and diabetes. In addition, firefighters who were cigarette smokers, hypertensive, and diabetic also reported a higher prevalence of heavy drinking. Piazza-Gardner et al. [4] reported that the prevalence of binge drinking decreased as firefighters aged or their years of service increased. Similarly, Keith et al. [2] also reported that binge drinking prevalence decreased as firefighters’ years of experience increased. Both Keith et al. and Smith et al. [8] reported a significant negative relationship between age and alcohol use in firefighters. Punakallio et al. reported that as firefighters aged, alcohol consumption decreased [44]. However, among firefighters in the CoCTFRS, alcohol consumption increased with age. This may be due to firefighters’ attitudes toward health becoming progressively more negative as they aged and their experience increased, as noted by Ras et al. [18]. This may result from discontent to setbacks in career progression [1-4]. Previous studies reported that cigarette smoking and alcohol consumption were significantly related, where cigarette smokers tended to consume more alcohol and have more alcohol-related problems [4-6, 9, 12, 45, 46]. In the current study, cigarette smoking was not significantly related to alcohol consumption; however, smokers had the highest average volume of alcohol consumption.
The current results indicated a significant relationship between the volume of alcohol consumed, systolic blood pressure, diastolic blood pressure and hypertension, and between the pattern of alcohol consumption, particularly related to heavy drinking and hypertension in firefighters. In contrast to the present study, Choi et al. [26] reported that alcohol consumption was not significantly related to hypertension in firefighters. Another study by Choi et al. [25] reported that alcohol consumption was significantly related to obesity in firefighters. However, in the present study, hypertension was the only CAD risk factor related to alcohol consumption. Similarly, Soteriades et al. [47] also noted that alcohol consumption was significantly related to high cholesterol but not blood pressure in firefighters. Lee and Kim [24] reported that a higher prevalence of high-risk drinking was related to metabolic syndrome in firefighters, of which one of the key parameters was abnormal blood pressure [27]. A review conducted by Fernández-Solà [7] noted that alcohol consumption, especially excessive use, contributed to increased vascular dysfunction, increased central adrenergic activity and vascular smooth-muscle tone, activation of the renin-angiotensin-aldosterone system, decreased release of nitric oxide, depressed cardiac output, reduced myocardial contractility, and dilatation of all the chambers of the heart. These cardiac effects could account for the relationship between alcohol consumption and hypertension [7]. This may explain why weekly alcohol consumption significantly predicted systolic and diastolic blood pressures in firefighters.
There was a significant relationship between the volume of alcohol consumed and the total amount of low-intensity physical activity and the amount of low-intensity occupational activity. There was also a significant relationship between the pattern of alcohol consumed and the total low-intensity physical activity, as well as the amount of low-intensity occupational activity in firefighters. A study conducted by Gilchrist et al. [13] found a similar result, where alcohol consumption was positively associated with the time spent in light-intensity physical activity. As with the present study, Gilchrist et al. reported that moderate-intensity physical activity was not associated with the volume of alcohol consumed. Similarly, Agrawal et al. [11] reported that sedentary behaviour was significantly related to alcohol consumption. This was further supported in two studies, which reported that alcohol consumption was a significant predictor of low-intensity physical activity [48] and a significant predictor of daily physical activity habits [49]. This was similar to the present results, where weekly alcohol consumption was a significant predictor of the total amount of low-intensity physical activity in firefighters. In contrast, Päivärinne et al. [50] reported no significant relationship between alcohol consumption and weekly physical activity. Increased alcohol consumption is reported to negatively affect sleep and increase feelings of fatigue and lethargy after an episode of heavy or binge drinking [1-4, 14, 51, 52]. This may inadvertently lead to firefighters engaging in lower-intensity physical activities in order to cope with the hangover effects of heavy or binge drinking. This can be seen in the present study, where heavy drinking correlated with low-intensity occupational, physical activity. Firefighters may engage in more low-intensity physical activity while on duty or intentionally choose to engage in lower-intensity duties rather than more vigorous-intensity duties. This can be seen in the non-significant negative correlation between alcohol consumption and the total amount of vigorous-intensity physical activity firefighters engaged in. A review article indicated that alcohol use negatively affected glucose metabolism, reduced oxygen consumption, altered temperature regulation, and increased the perception of physical activity intensity [53]. In the present study, total vigorous-intensity physical activity was significantly related to systolic and diastolic blood pressures. This may be due to younger firefighters participating more in vigorous-intensity physical activity but also having the highest prevalence of alcohol consumption and most being heavy drinkers.
4.1. Strengths and Limitations
This study provides valuable research data in a scarcely studied area on alcohol use in firefighters that is related to their demographic characteristics, total weekly physical activity patterns and CAD risk factors, especially in South Africa. The study is limited by convenient sampling and a relatively small sample size prescribed by the municipal authority of the City of Cape Town, which reduces the generalizability of the current results to the entire CoCTFRS. The study was also under-represented by female participants. In addition, the study did not classify firefighters as binge drinkers.
4.2. Recommendations
In future research, a randomised study with a suitably powered sample size is recommended to ensure generalizability to the entire CoCTFRS. Although the current results are promising, a more representative sample of the CoCTFRS is needed to strengthen the inferences made in the current study. A higher representation of female firefighters is recommended, as the current study was underrepresented by female firefighters, limiting the generalizability of the results to the broader female firefighting population. Future studies should also investigate the cause of the high alcohol drinking prevalence in firefighters, particularly related to occupational stress, coping strategies and post-traumatic stress disorders. Although the current study measured weekly alcohol consumption, future studies should use a validated tool that can classify firefighters as heavy, hazardous and binge drinkers.
CONCLUSION
In the present study, 72.6% of firefighters reported consuming alcohol, of which 75.5% were male, and 61.5% were female. The majority of firefighters (69.9%) were categorised as light drinkers, while 21.1% as moderate drinkers, and 10% as heavy drinkers. Young male firefighters consumed more alcohol than females and were more likely to be heavy drinkers. White firefighters were the highest drinkers and preferred mixed alcoholic beverages. The volume of alcohol consumed and patterns of alcohol consumed were significantly related to hypertension, the amount of low-intensity occupational, physical activity and the total amount of low-intensity physical activity. In addition, the volume of alcohol consumed was a significant predictor of systolic and diastolic blood pressures and the total amount of low-intensity physical activity in firefighters. Although these results are modest, the results provide valuable information for this specific population in Cape Town, South Africa. Educational programs should be implemented to reduce the prevalence of excessive and hazardous alcohol use, especially among young male firefighters. Firefighters who are classified as heavy drinkers should be referred to professional counselling for proper intervention to reduce hazardous drinking in firefighters.
LIST OF ABBREVIATIONS
| CoCTFRS | = City of Cape Town Fire and Rescue Service |
| CAD | = Coronary Artery Disease |
| IPAQ | = International Physical Activity Questionnaire |
AUTHORS’ CONTRIBUTIONS
Jaron Ras and Lloyd Leach contributed to conceptualization, methodology, validation, writing, review and editing, and resource collection; Jaron Ras participated in software utilization, formal analysis, investigation, data curation, writing, visualization, and project administration. Supervision was done by Lloyd Leach. All authors have read and agreed to the published version of the manuscript.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study protocol was approved by the Biomedical Research Ethics Committee (BMREC) at the University of the Western Cape (Ethics reference number: BM19/4/3).
HUMAN AND ANIMAL RIGHTS
No animals were used in the studies that are the basis of this research. All the humans were used in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013 (http://ethics.iit.edu/ecodes/node/3931).
CONSENT FOR PUBLICATION
Informed consent was obtained from all participants of this study.
STANDARDS OF REPORTING
STROBE guidelines were followed.
AVAILABILITY OF DATA AND MATERIALS
The data that support the findings of this study are available within the article.
FUNDING
This research was funded by the National Research Foundation (NRF) (Grant Numbers: 117718).
CONFLICTS OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The authors would like to thank the City of Cape Town Fire and Rescue Service for granting permission to conduct the study, each district head and station commander for supporting the study, and every firefighter for voluntarily participating in the study.

