All published articles of this journal are available on ScienceDirect.

Modeling of Risk Factors of Childhood Stunting Cases in Malang Regency using Geographically Weighted Regression (GWR)
Abstract
Background:
Stunting is one of the fundamental problems in Indonesia's human development, with complex risk factors such as inadequate environmental sanitation.
Objective:
This study aims to conduct an analysis and mapping of spatially correlated sanitation risks on the prevalence of stunting among toddlers in Malang Regency, Indonesia.
Methods:
The field observations were conducted in 390 villages of urban and rural areas in Malang Regency. The secondary data of weighing toddlers in 2020 were collected from Malang Regency Health Office. The data included the identity of the residents and the history of the toddlers, while data from monthly program reports were collected from the Central Bureau of Statistics of Malang Regency. Furthermore, the study applied one and eight variables of Y and X. The Y variable was the number of stunting case toddlers, while X included the percentage of access to safe drinking water, percentage of access to permanent hygienic latrines, the topography of the region, percentage of Integrated Healthy Centre access, percentage of Exclusive Breastfeeding, Population density, ODF (Open Defecation Free) village and percentage of Integrated Healthy Centre Empowerment. Modeling the case of childhood stunting with the spatial regression method using Geographically Weighted Regression can be considered a sound approach.
Results:
The result showed that the distribution model of risk factors causing toddler stunting showed a spatial autocorrelation tendency with a clustered pattern in the area. The risk factors that were found to be spatially correlated with the incidence of stunting in children under five years of age in Malang district included access to proper drinking water (X1), access to latrines (X2), access to integrated health services (X3), exclusive breastfeeding coverage (X4), regional topography (X5), population density (X6), and empowerment of integrated health services (X8). However, the ODF (X7) did not show any correlation with stunting cases in the area.
Conclusion:
Spatial diversity and geographic variation affect the distribution pattern of risk factors causing stunting in Malang Regency. Therefore, stunting control with specific and sensitive interventions should be based on regional and local characteristics.
1. INTRODUCTION
Stunting is a medical condition characterized by impaired growth of the body and brain in toddlers resulting from prolonged malnutrition [1, 2]. Several health and non-health factors contribute to stunting, with health factors accounting for about 70% and non-health factors accounting for about 30% of the risk factors. Non-health factors include various aspects such as food security, sanitation, poverty, education, social, economic, and environmental factors [3]. WHO data on the prevalence of stunting in toddlers shows that Southeast Asia has the second-highest rate of stunting cases at 31.9%, after Africa at 33.1%. Indonesia is the sixth country in Southeast Asia, after Bhutan, Timor Leste, Maldives, Bangladesh, and India, with a high risk rate of 36.4% stunting cases. Among 18 provinces in Indonesia, East Java has a particularly high prevalence of stunting, with 30-40% of toddlers classified as short or very short.
Malang Regency is one of the 100 priority districts or cities for stunting national intervention [4]. However, despite efforts to address the high rate of stunting in the area, progress has been ineffective due to differences in risk factors between different regions. To address this issue, it is imperative to identify specific risk factors that are unique to each locality. Spatial analysis using Geographically Weighted Regression (GWR) is a powerful method to simplify complex problems by mapping and predicting the variation in risk factors that correlates with regional child stunting [5]. This method allows for the identification of factors related to stunting in toddlers in each region by observing the model. By using geographic factors as an independent variable that can affect the response variable, the GWR modeling provides a spatial method for tailoring interventions and programs to the local risk factors [5].
Using the GWR technique, earlier studies have presented data on cases of stunting associated with area-based risk variables. For example, modeling of malnutrition in toddlers in East Java using GWR has identified influential variables such as the ratio of health workers to the number of toddlers and the average age of first marriage of 16 years [6]. Another study used Geographically Weighted Logistics Regression with Gaussian Adaptive Kernel Weighting Functions to identify factors with a significant effect on cases of malnutrition, including the coverage of infants who received complete immunizations, exclusive breastfeeding, visits to the health center, households with clean and healthy behavior, the percentage of active health centers, and environmental sanitation [7]. Based on these findings, this study creates maps and models the distribution of stunting cases in Malang Regency, focusing on risk factors that are spatially correlated with the incidence of stunting in children under five.
2. MATERIALS AND METHODS
2.1. Data Source
To collect data for the study, field observations were conducted in 390 villages throughout Malang Regency. In addition, secondary data on weighing toddlers in 2020 were obtained from the Malang Regency Health Office. This data included the identity of the residents and the toddlers' histories. Monthly program reports were also collected from the Central Bureau of Statistics of Malang Regency. The study applied both dependent (Y) and independent (X) variables, including the number of toddler stunting cases (Y) and eight independent variables (X). These independent variables consisted of the percentage of access to safe drinking water, percentage of access to permanent hygienic latrines, the topography of the region, percentage of access to Integrated Healthy Centre services, percentage of Exclusive Breastfeeding, population density, ODF (Open Defecation Free) village status, and percentage of Integrated Healthy Centre Empowerment.
2.2. Data Analysis Procedure
The data relationships between X and Y variables were analyzed using the GWR model. This method is a development of linear regression, with each parameter calculated at each location point. Therefore, each geographical location point has a different regression parameter value with significant local variables for each observation location. The case of stunted toddlers was modeled using the Global Linear Regression or the Ordinary Least Square (OLS) methods. Classical regression was employed to test the assumptions of data normality, and the value of the Variance Inflation Factor (VIF) was examined to check for multicollinearity assumptions. Additionally, the Shapiro-Wilk Normality test was used to analyze residual normality assumptions. Multiple linear regression modeling techniques were used for the analysis when all the assumptions of the model were satisfied. However, in cases where one of the assumptions was not met, a spatial effect test was conducted on the remaining multiple linear regression model. The Breusch-Pagan test was employed to observe spatial heterogeneity.
To model the case of toddler stunting with the spatial regression method using GWR, several stages were followed: (a) The optimum bandwidth value is determined based on the Cross Validation (CV) criteria, with CV calculations carried out until the minimum value is obtained, (b) Obtaining the weighting matrix using the Gaussian kernel function, and (c) estimating the parameters of the GWR model using the optimum bandwidth. The results of OLS and the GWR regressions were compared by using R2 and SSE criteria. To determine the significant effect of X variables on stunting cases in each area group, a partial test was performed using t-test statistics on each parameter of the observation area. The significance of the GWR model parameters is tested using the following hypothesis:
H0: βk (ui,vi)= 0
H1: βk(ui,vi) ≠βk; i=1,2,...,22, k=1,2,3
Results were visualized in the form of a thematic map of toddler’s stunting case areas using the Geographic Information System with ArcGIS 10.9 application.
3. RESULTS AND DISCUSSION
3.1. Description of Stunting Cases in Malang Regency
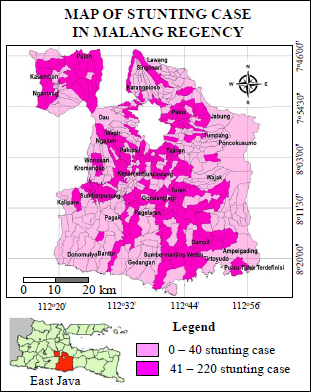
An illustration of the distribution of stunting cases in Malang Regency is presented in Fig. (1). In 390 villages (both in urban and rural areas), toddler stunting cases occurred in 385 villages, while the rest of the 5 villages were free of stunting cases. The number of stunting cases was grouped into two intervals namely, the low range (0 - 40 stunting cases) and the high-range (41 - 220 stunting cases). The low range cases were found in 203 villages, while the high-range cases were found in 182 villages. The case was absent in 5 villages. The highest stunting case was found in Pakis Sub-regency, with a total of 1,660 toddlers and the lowest was found in Pagak Sub-regency with a total of 70 toddlers. The high cases were found in several villages in Pakis, Tajinan, Turen, Gondanglegi, Dampit, Sumbermaning Wetan, Pujon, Kasembon dan Ngantang Sub-regencies. The geographical characteristics of these Sub-regencies have differences. The northern, western and central parts are relatively fertile areas, the southern part is limestone mountains, while the eastern part is mountains and hills.
The distribution pattern of stunting cases tended to cluster in adjacent areas. The diversity of those patterns was influenced by location factors with the same risk factor characteristics. The figure showed that the distribution of childhood stunting was evenly distributed in all topography of the region and it was most frequent in hilly topography (100-500 meters asl) with 11,454 cases (Fig. 1).
3.2. Linear Regression Modelling (Global Regression) childhood stunting cases
Multiple linear regression analysis was carried out to obtain variables that had a significant linear effect on the case of childhood stunting. Examination of the assumptions of the multiple linear regression model was carried out with several formal tests. Examination of the assumption of no multicollinearity data can be viewed from the value of VIF (Variance Inflation Factor). The VIF values of the predictor variables were all smaller than 10, admittedly there was no multicollinearity. The linear regression equation for the response to variables of childhood stunting was obtained by the following model:
 |
Based on the obtained model, access to safe drinking water (X1), access to permanent hygienic latrines (X2), regional topography (X3), and population density (X6) had a positive relationship with childhood stunting. Meanwhile, the variables of Integrated Healthy Centre access (X4), exclusive breastfeeding (X5), ODF villages (X7), and Integrated Healthy Centre empowerment (X8) had a negative relationship to childhood stunting. This means that the lower access to Integrated Healthy Centre was, the more childhood stunting increased. Testing the normality of the linear regression residuals was carried out using the Shapiro-Wilk test method. The results of the normality test produced a P value of more than 0.3712, so it failed to reject H0 at a significance level of α = 0.05, which means that the residuals fulfilled the assumption of a normal distribution.
3.3. Spatial Regression Models of Geographically Weighted Regression (GWR)
GWR is a development of a regression model in which each parameter is calculated at the location point with different values. To prepare the GWR Model, the following stages are followed:
3.4. Heteroscedasticity Test
Heteroscedasticity Test was conducted to determine the homogeneity of variance on the residuals of the study variables. This is important to determine the subsequent step because the GWR model is considered to be good when there is heteroscedasticity. The Breusch-Pagan test was used for the test, with the H0test rejected when the p-value < α. The results of the Breusch-Pagan test showed a value of 26.593 with a p-value of 0.0008309. As the p-value was smaller than the 0.05 level of significance, H0 was rejected. Therefore, the residuals in the multiple linear regression model between the dependent and independent variables had spatial diversity. To overcome the problem of heteroscedasticity in the linear regression model, the GWR method was applied.
3.5. Optimum Weight Selection
The GWR model employed weights based on the geographical location of each village in Malang Regency. To determine the weights, the first step was to ascertain the longitude and latitude of each village. The Euclidean distance was then calculated based on the geographical location of the area, and the sequence of other adjacent regions was used to determine an area based on the Euclidean distance. This enabled the closest order of the region to be obtained for the entire observation area. Furthermore, the optimum bandwidth for each village was chosen with the kernel function. To determine the best kernel method, modeling was conducted for each weight, and the Cross Validation (CV) value was obtained. The weight with the smallest CV value was used to build the model. The Adaptive Gaussian weighting emerged as the optimal weighting for the GWR modeling due to its smaller CV value compared to others. After the formation of the weighting matrix, a partial parameter test was conducted to determine the factors influencing the occurrence of childhood stunting in Malang Regency. The GWR model was tested to identify the influence of location factors on childhood stunting. The parameter testing of the GWR model, using Adaptive Gaussian weighting, showed that the F-count statistic was 2.1868, which was greater than the critical value of F (0.05; 53.961; 322.039) = 1.38. Therefore, Ho was accepted, and it was concluded that the weighting of the Adaptive Gaussian Kernel affected the parameter estimation of the GWR model. In conclusion, there was a spatial influence or geographical factors affecting childhood stunting in Malang Regency.
3.6. Model Selection
The regression model was selected by assessing the goodness of fit as viewed from the R2 value. A higher value relative to other models indicates better performance. The goodness of fit measures is obtained from the linear regression and GWR. Based on the criteria of R2 from the Akaike information criterion (AIC) and the SSE values, the GWR outperforms the OLS regression model. The superiority is evidenced by its ability to increase the R2 value and decrease the AIC and SSE. The overall R2 values indicate that the GWR model produces a higher value. Specifically, the OLS and GWR models yielded an R2 value of 7% and 32.13%. This demonstrates that the GWR model is more suitable for modeling cases of childhood stunting in the Malang Regency. The coefficient of determination (R2) value explains 32.13% of the variability of the risk factor variables influencing childhood stunting, while the remaining 67.87% is explained by other external risk factors.
3.7. Model Building
The modeling process using the GWR method requires data on the geographical location of each village, including their latitude and longitude. The weighting matrix used should be formed from the adaptive Gaussian weighting function, which is selected based on the criteria of the largest R2 and smallest AIC. The GWR modeling process generated 385 local models, one for each urban village in Malang Regency, and identified variables that have significant effects on childhood stunting cases (Table 1 and Fig. 2). As shown in Table 1 and Fig. (2), the GWR model for Toyomarto village identified access to safe drinking water (X1) and population density (X6) are the two significant variables.
 |
From the model formed in Toyomarto village, an increase in access to safe drinking water (X1) by one percent resulted in a decrease of 0.489323369 in stunting prevalence, while other variables were considered constant, and the influence of the location around point 1 was considered constant. Similarly, an increase in the variable of access to permanent hygienic latrines (X2) by one percent resulted in a decrease of 0.297 in stunting prevalence, while other variables were constant, and the influence of the location around point 1 was considered fixed. In addition, an increase of one percent in the Integrated Healthy Centre (X4) reduced the stunting prevalence by 0.422, with other variables being constant, and the influence of the location around point 1 was considered constant. Moreover, an increase of one percent in the regional topography variable (X3) resulted in a decrease of 0.017 in stunting prevalence, while other variables were constant, and the influence of the location around the observed point, namely point 1 was considered fixed. Finally, an increase of one percent in Population Density variable (X6) increased the stunting prevalence by 0.003, with other variables being constant, and the influence of the location around point 1 was considered constant.
| S.No. | Significant Variable | Village | Number of Significant Villages |
|---|---|---|---|
| 1 | X1,X3,X5,X6 | Pakisjajar, Bunutwetan, Asrikaton, Saptorenggo, Argosari, Gunung Jati, Sidomulyo, Slamparejo, Taji, Jabung, Kemantren, Sidorejo, Ngadirejo, Sukolilo, Sidoluhur, Watugede, Tamanharjo, Baturetno, Dengkol, Wonorejo. | 20 |
| 2 | X2,X5,X6 | Donomulyo, Purworejo, Sumberoto, Tempursari, Kedungsalam, Mentaraman, Purwodadi, Arjosari, Sumberkerto, Pringgodani, Pandanlandung, Sidorahayu, Parangargo, Sitirejo, Sumbersekar, Kucur, Petungsewu, Selorejo, Tegalweru, Tempursari. | 20 |
| 3 | X2,X6 | Banjarejo, Tulungrejo, Bantur, Wonorejo, Srigonco, Sumberbening, Rejosari, Tambakasri, Kedungbanteng, Tambakrejo, Sidoasri, Ringin kembar, Tegalrejo, Baturetno, Srimulyo, Sukodono, Tirtoyudo, Gadungsari, Wonoagung, Tamansatriyan, Ampelgading, Sukorejo, Tlogosari, Jogomulyan, Kepatihan, Sumbertangkil, Pujiharjo, Purwodadi, Sonowangi, Sidorenggo, Simojayan, Taman Asri, Taman Sari, Argoyuwono, Tirtomarto, Tawangagung, Lebakharjo, Tirtomoyo, Purwoharjo, Mulyoasri, Dawuhan, Wringinanom, Talok, Sempal wadak, Dalisodo, Tambak Asri, Jambearjo, Malangsuko, Tirtomoyo, Srigading, Tunjungtirto, Langlang, Ampeldento, Kepuharjo, Ngenep, Girimoyo, Bocek, Donowarih, Tawangargo, Ngijo, Mulyoagung, Landungsari, Kalisongo, Gadingkulon, Jombok. | 65 |
| 4 | X3,X6 | Klepu, Dampit, Amadanom, Bumirejo, Pamotan, Sumber suko, Majang tengah, Rembun, Pojok, Jambangan, Ngadireso, Sumberejo, Wonorejo, Wonomulyo, Poncokusumo, Pandansari, Sukolilo, Blayu, Codo, Dadapan, Bringin, Sumberputih, Sumberputih, Wonoayu, Bambang, Patokpicis, Turen, Pagedangan, Sedayu, Tawang rejeni, Gedog Wetan, Gedog Kulon, Undaan, Sawahan, Kedok, Talangsuko, Tumpukrenteng, Sananrejo, Sanankerto, Tumpang, Jeru, Pandanajeng, Kambingan, Tulusbesar, Benjor, Duwet, Sekarpuro, Pandansari, Madiredo, Wiyurejo. | 49 |
| 5 | X3,X5,X6 | Sukomulyo, Bendosari, Ngabab, Pujon Lor, Tawangsari, Pujon Kidul Ngroto, Pandesari, Tulungrejo, Waturejo, Kaumrejo, Sumberagung, Mulyorejo, Purworejo, Banjarejo, Pagersari, Sidodadi, Ngantru, Banturejo, Pandansari, Sukosari, Kasembon, Wonoagung, Pait, Bayem, Pondok Agung. | 26 |
| 6 | X4,X5,X6 | Gampingan, Sumberejo, Rejoyoso, Sumberejo, Sukonolo, Panggungrejo, Sukosari, Sumberjaya, Bulupitu, Ganjaran, Karangsuko, Brongkal, Kanigoro, Balearjo, Kademangan, Banjarejo, Kepanjen, Sukoraharjo, Sambigede, Senggreng, Ternyang. | 21 |
| 7 | X5,X6 | Wonokerto, Karangsari, Bululawang, Wandanpuro, Lumbangsari, Penarukan, Ardirejo, Dilem, Talangagung, Mojosari, Curungrejo, Tegalsari, Kedungpedaringan, Panggungrejo, Mangunrejo, Kemiri, Jenggolo, Sengguruh, Cepokomulyo, Ngadilangkung, Sumberpucung, Jatiguwi, Ngebruk, Karangkates, Kromengan, Jatikerto, Slorok, Ngadirejo, Karangrejo, Palaan, Ngasem, Plandi, Kluwut, Genengan, Glanggang, Karang Pandan, Kebon Agung, Pakisaji, Sutojayan, Wadung, Wonokerso, Kendalpayak, Karang Duren, Permanu, Jatisari, Jatirejoyoso, Peniwen. | 47 |
| 8 | X6 | Sumbermanjing Wetan, Harjokuncaran, Ringinsari, Argotirto, Druju, Sekarbanyu, Tamankuncaran, Ngebruk, Pajaran, Jambesari, Karanganyar, Karangnongko, Ngadas, Wajak, Ngembal, Sukoanyar, Kidangbang, Kemulan, Sukorejo, Tajinan, Ngawonggo, Tangkilsari, Pandanmulyo, Purwosekar, Gunung Ronggo, Gunung Sari, Jatisari, Sumbersuko, Randugading, Kidal, Ngingit. | 31 |
| 9 | X1,X3,X6 | Wringinsongo, Bokor, Slamet, Ampeldento, Sumberkradenan, Kedungrejo, Banjarejo, Pucangsongo, Sukoanyar, Sumberpasir, Pakis kembar, Mangliawan, Kenongo, Pagentan, Banjararum. | 15 |
| 10 | X1,X5,X6 | Sukopuro, Lawang, Sumber Ngepoh, Bedali, Sidodadi, Candirenggo, Ardimulyo, Randuagung, Losari. | 9 |
| 11 | X1,X6 | Kalirejo, Wonorejo, Sumber Porong, Mulyoarjo, Toyomarto. | 5 |
| 12 | X2 | Bandungrejo, Gedangan, Gajahrejo, Sidodadi, Sindurejo, Tumpakrejo, Girimulyo, Sitiarjo, Sumberagung, Sidorejo, Gunungrejo, Tegalgondo. | 12 |
| 13 | X2,X4,X5,X6 | Kalipare, Putukrejo, Tumpakrejo, Arjowilangun, Sukowilangun. | 5 |
| 14 | X2,X5 | Kaliasri, Sumbermanjing Kulon, Pandanrejo, Sempol, Jedong, Mendalanwangi, Karangwidoro, Tlogosari. | 8 |
| 15 | X3,X7 | Pulungdowo. | 1 |
| 16 | X4,X5 | Tlogorejo, Gading, Putuk Rejo, Suwaru, Pagelaran. | 5 |
| 17 | X4,X6 | Krebet, Kuwolu, Bakalan, Sudimoro, Kasri, Pringu, Gdl Kulon, Gd Wetan, Putat Kidul, Sepanjang, Putat Lor, Urek Urek, Ketawang, Clumprit. | 14 |
| 18 | X5,X6,X8 | Jambuwer, Ngajum, Banjarsari, Kranggan, Kesamben, Balesari, Wonosari, Kebobang, Sumbertempur, Sumberdem, Bangelan, Plaosan. | 12 |
| 19 | X1,X3,X6 | Wringinsongo, Bokor, Slamet, Ampeldento, Sumberkradenan, Kedungrejo, Banjarejo, Pucangsongo, Sukoanyar, Sumberpasir, Pakis kembar, Mangliawan, Kenongo, Pagentan, Banjararum. | 15 |
In the variables of Exclusive Breastfeeding (X5), ODF Villages (X7), and Integrated Healthy Centre Empowerment (X8) the coefficient was negative. Therefore, it can be interpreted as follows, an increase in the Exclusive Breastfeeding variable (X5) by one percent reduced the stunting prevalence by 0.252 on the condition that the other variables were constant and the influence of the location around point 1 was considered constant. Stunting prevalence decreased by 0.280 with an increase in the ODF Villages variable (X7) by one percent. Meanwhile, other variables were constant and the influence of location around point 1 was considered constant. An increase of one percent in Integrated Healthy Centre Empowerment (X8) reduced the stunting prevalence by 0.0339. Other variables were constant and the influence of the location around point 1 was also considered constant.
The southern regions of Sumbermanjing Wetan, Dampit, Gondanglegi, Bululawang, and Pagelaran Sub-regencies have been identified as areas with an estimated stunting risk, where the number of cases exceeds 21, as shown in Fig. (2). The primary risk factors predicted include population density, access to permanent hygienic latrines, regional topography, and exclusive breastfeeding coverage. Poor sanitation due to the discharge of wastewater from households and septic tanks may lead to a decline in groundwater quality, which can be associated with the population density and location of the area. The presence of e-coli bacteria in groundwater is an indication of this pollution, and consumption of water contaminated with e-coli bacteria may lead to diarrhea. In highland or mountainous topography areas, limited access to clean water is an issue due to the location of deep underground springs, which may lead to stunting in toddlers. Furthermore, toddlers from families with poor access to clean water and sanitation often experience diarrhea more frequently than those with good water and sanitation conditions. The completeness of exclusive breastfeeding is another factor affecting the risk of toddlers experiencing the condition.


This condition results in groundwater quality decline or environmental pollution due to poor sanitation such as seepage of wastewater from households. It includes seepage from septic tanks and the pollution is marked by the presence of coli bacteria in groundwater. In theory, the high content is due to the proximity of the septic tanks and drainage channels to the wells, located in densely populated areas, in which on-site sanitation is still used. Meanwhile, the use of water containing coli bacteria for consumption may cause diarrheic. Stunting tends to occur in areas with the characteristics of medium-high lands and mountains. Highland areas or mountains in some places lack clean water because of the location of the springs which are deep underground. Families with a lack of access to clean water and sanitation are more likely to experience diarrheic. The completeness of exclusive breastfeeding affects the risk of toddlers suffering from stunting.
3.8. Regional Topography (X3) and Population Density (X6) Correlate with Access to Safe Drinking Water (X1) and Access to Permanent Hygienic Latrines (X2)
One of the risk factor variables related to sanitation and the geographical environment which include the coverage of access to safe drinking water (X1), access to permanent hygienic latrines (X2), regional topography (X3), and population density (X6) significantly affect the stunting prevalence. This condition indicates that the increase in population density affects sanitation problems. Groundwater pollution or a decline in quality is closely related to the level of population density and the location of the area. This is because the population is directly related to the waste discharged into the environment. The decline in groundwater quality or pollution is due to poor sanitation such as seepage of wastewater from households. This includes seepage from septic tanks and the contamination is marked by the presence of coli bacteria [7-9].
Theoretically, the high content of the bacteria is due to the proximity of the septic tanks and drainage channels to the wells, which are located in densely populated areas. The use of water containing coli for consumption can cause diarrheic. A study investigation, using data from 137 developing nations, analyzed environmental factors, specifically insufficient sanitation and water supply. The study's statistical analyses showed that inadequate sanitation had an odds ratio (OR) of 1.37 (95% CI, 1.33-1.41), while unsafe water had an OR of 1.09 (95% CI, 1.06-1.12) [3]. Therefore, insufficient sanitation and unsafe water had a risk factor for childhood stunting of 1.37 and 1.09 times, respectively. Other results obtained household sanitation data on households of untreated water for drinking. The results of logistic regression statistical tests showed that people who drink untreated water had an Odds Ratio of 3.47 (95% CI 1.73-7.28). Therefore, these households had a risk of childhood stunting by 3.47 times, with a P value = <0.001 [10]. The results are consistent with study in Yogyakarta where the high risk of unclean water facilities caused acute diarrhea in toddlers by 2.44 times compared to clean water facilities [11].
A previous study shows that toddlers living in households with 0% access to sanitation have a 1.04 times risk of experiencing stunting. Furthermore, a p-value = 0.001 indicates that households with 0% access to sanitation influence childhood stunting [12]. Toddlers in households without access to latrines are more at risk of suffering from stunting (Fig. 3).
One multi-country study showed that sanitation contributed to a reduction in the prevalence of nutritional intake deficits in urban and rural toddlers by 22–53% and 4–37%. Different studies have shown that poor sanitation increases the risk of toddlers experiencing stunting. Hygiene interventions including hand washing, water quality care, sanitation, and health education contributed to a 2–3% reduction [13]. In another study, toddlers from families with poor water and sanitation conditions experienced diarrhea more often [14]. This is because subclinical infections from exposure to polluted environments and nutrition can reduce the ability of the intestines to prevent disease-causing organisms from entering the body [15]. Another infectious disease due to an unfavorable environment was a worm infection or STH (Soil-Transmitted Helminth). STH worms are transmitted through the soil and include Ascaris lumbricoides, Trichuris trichiura, Ancylostama duodenale, Necator americanus, and Strongylaides steicoralis [16].
In several studies, altitude or regional topography is associated with stunting [17-19]. The highest prevalence was in Bangli Regency, Bali province in the medium-high and high lands topography [17]. Furthermore, stunting was more common in the northern part of Ethiopia where the area has characteristics of medium-high and high lands [18]. Another study conducted in Manggarai, Indonesia found Moran's stunting value of 0.45 with a p-value of 0.0001 in the region altitude from sea level. Therefore, stunting cases are significantly higher in mountainous areas in Manggarai Regency [19].
There were differences in the risk factors for stunting in each regional zone. Based on multivariate analysis, the determinant of the condition in the lowland ecosystem zone was energy intake. In addition, the determinants in the medium-high land zone were the practice of compassion and environmental sanitation; and in the mountainous ecosystem, it was environmental sanitation [20].
Population growth has an impact on the increase of population density which affects poverty. Rapid population growth intensifies the strain on land, negatively impacting food production, leading to unemployment, and potentially triggering poverty [21]. Food access has several indicators affecting the level of poverty indicators [22] with population growth [23].
To measure poverty, the Central Bureau of Statistics uses the concept of the ability to fulfill basic needs, and this concept refers to the Handbook on Poverty and Inequality published by the World Bank. By using the approach, poverty is viewed as an economic inability to fulfill the basic food and non-food needs as measured from the expenditure side. A population is categorized as poor when it has an average monthly per capita expenditure below the poverty line. Based on several studies, the income of parents determines the status of malnutrition or childhood stunting. This is in line with the results in Pujon Sub-district, Malang Regency, 96% of childhood stunting was found in parents with incomes below the minimum standard wage [24]. Meanwhile, low family income affects the family's ability to fulfill food needs. A sufficient family income would enable the purchase of high-quality and nutritious food ingredients. Insufficient nutritional consumption in toddlers causes childhood stunting, and this is supported by the stunted toddlers’ families, which were 47% of the poverty line.
3.9. Coverage of Access to Integrated Healthy Centre (X4) and Integrated Healthy Centre Empowerment (X8) has a Positive Effect on Exclusive Breastfeeding Coverage (X2)
The exclusive breastfeeding coverage (X2), Integrated Healthy Centre access (X4), and Integrated Healthy Centre Empowerment (X8) significantly affected childhood stunting in several urban villages in Malang Regency. This condition shows that these risk factors were related to each other. Therefore, an increase in exclusive breastfeeding coverage must be influenced by Integrated Healthy Centre access and empowerment. The risk factors for Integrated Healthy Centre access and empowerment affected the adjacent sub-districts in Malang Regency, such as Ngajum and Wonosari with 16 adjacent villages. Based on the results, mothers who had toddlers with poor nutrition were less active to come to the Integrated Health Centre. This is because they felt less confident concerning the condition of the toddler. Some did not need to come to health services when their toddler was sick with a cough and cold because the condition can be easily treated by purchasing drugs from stores [24]. The ability of a household to access health services including the Integrated Healthy Centre is related to the availability of health service facilities and the economic capacity to pay service costs [25]. The results are also supported by a study conducted on the relationship between families’ access to Integrated Healthy Centre with the nutritional status of toddlers in Rancaekek Kulon Village, Rancaekek District [26]. Furthermore, there is a relationship between the level of mothers’ participation with the nutritional status of toddlers and the behavioral utilization of the Integrated Health Centre. The relationship between nutritional status and morbidity of toddlers is very significant. The mothers’ active visits to Integrated Healthy Centre also affected the nutritional status of the toddler (p-value 0.02). Empowerment of the cadres for toddlers can be studied with an approach consisting of Alignment, Capability, Trust, and Participation [27]. The results of other studies state that there was a relationship between the role of the village government and the activity of the Integrated Healthy Centre cadre. This finding is consistent with the results of another study on mothers of stunted toddlers in Pujon Sub-District, Malang Regency, where 60% of them possessed good nutritional knowledge. However, it should be noted that the presence of stunted toddlers in some Integrated Healthy Centre areas remains low [23].
The activeness of mothers in accessing the Integrated Healthy Centre and the role of empowerment carried out by village health workers and cadres made a significant contribution in increasing maternal awareness and understanding of providing complete exclusive breastfeeding. Meanwhile, several studies show a relationship between exclusive breastfeeding and stunting prevalence. Breastfeeding is associated with the growth of the toddler's body length. The duration of breastfeeding exhibited a positive correlation with growth length. The prolonged period had a significant impact on the accelerated growth of toddlers during the second and third years of their lives. Furthermore, the results show that toddlers who are not exclusively breastfed may experience stunted growth. In line with 2013 Riskesdas’s study in the Cirebon area in 2011, it was stated that exclusive breastfeeding was the most dominant factor in the persistence of stunting status in toddlers. A study in Aceh proves that toddlers who were given complementary foods at an early age have a risk of becoming stunted 6.54 times compared to those given at the right age [28]. The results are different from a study in the Purworejo area, Central Java, where exclusive breastfeeding was not associated with stunting in toddlers aged 2 years. Furthermore, the coverage below the standard category at 67% affected childhood stunting in the villages of Madiredo, Jambearjo, and Rejosari [23]. The risk of becoming stunted was 3.7 times higher in toddlers who were not exclusively breastfed (breastfeeding < 6 months) compared to those who received exclusive breastfeeding (≥ 6 months) [29]. Toddlers who did not receive colostrum were at a higher risk of stunting [30]. This is because it exerts a protective effect on newborns and prolonged duration of breastfeeding is also a risk factor. Other studies have also stated that giving colostrum to infants is associated with the condition [31].
To address malnutrition, an effective approach involves implementing a stunting program via the Integrated Healthy Centre empowerment model. This requires cross-sectoral coordination and engagement with diverse local government, community, and private institutions. The government exerts efforts through specific interventions conducted by the Ministry of Health, Provincial, and Regency/City Offices. This includes related interventions for environmental health, poverty alleviation, and women's empowerment [32]. The Indonesian government minimizes the percentage of stunting to 5% by 2024. Internationally, the SUN (Scaling Up Nutrition Movement) program which reduces cases of malnutrition has been adopted by Indonesia to provide nutritious and healthy food [33].
Understanding or insight related to malnutrition in toddlers in several areas was obtained from Integrated Healthy Centre activities. The parent’s understanding of the symptoms and consequences, including the prevention of stunting, played a crucial role in shaping their attitude towards maintaining good health [34]. A good insight leads to parents’ awareness of the urgency to prevent stunting. This awareness leads to health behavior, specifically stunting prevention through the fulfillment of nutrition for pregnant women and toddlers, and maintaining sanitation in the home environment [35]. Inadequate parenting of toddlers at risk of stunting can manifest in several ways, including allowing them to refuse food, lacking precision in providing appropriate complementary feeding, failing to prioritize nutrition-conscious family behaviors, and neglecting the nutritional requirements.
3.10. Villages with ODF (Open Defecation Free) Status have a Low Correlation to the Stunting Reduction in the Village Area
Stunting prevention initiatives can be carried out by targeted and considerate dietary treatments. It supports 70% of the interventions for stunting. Sensitive nutrition treatments should ideally be implemented through a variety of non-health development initiatives. The Community-Based Total Sanitation (CBTS) initiative, which strives to enhance the cleanliness and standard of living of Indonesians, is one of the policies put into place there. A strategy called CBTS uses self-triggering to empower the community and change people's attitudes toward healthy living [36]. For instance, this program uses a behavior change ladder to try to change the villagers' practice of open defecation. The behavior change ladder is a progression of changes in behavior from those who initially engaged in open defecation to individuals who are 100% free from open defecation (ODF) [37]. Communities that achieve ODF are anticipated to undergo additional behavioral adjustments related to clean living in the subsequent stage, including hand washing with soap, controlling drinking water and home waste, securing domestic garbage, and more. The final achievement of the behavior change ladder leads the community to implement a complete sanitization. Stunting rates in an area should decline as a result of this achievement.
The series of behavioural changes from open defecation to total sanitation requires continuous monitoring, verification and evaluation [38]. Verification process may ensure changes in village community behaviour for implementing CBTS. Villages stated to be ODF verified when everyone defecates in hygienic latrines, there are community-created general monitoring mechanisms, and there are regulatory punishments or other initiatives to prohibit open defecation [38].
Data from the CBTS monitoring and evaluation show that from the initial triggering in 2012, 32.05% of the villages in Malang Regency have become ODF, totaling 125 villages. According to the GWR study, one out of 385 villages strongly demonstrated a correlation between ODF villages and stunting. Several factor may influence the construction of ODF villages. Demand, supply, and the enabling environment are some of these factors [37]. The demand component is an increase in the community's need for proper sanitation. Demand activities are carried out by triggering, monitoring and using behaviour change media with the aim of the community ability to change their behaviour after triggering [37]. The supply component is the activity of providing access and sanitation services. This component aims to increase the provision of affordable and varied sanitation facilities to the wider community. Activities to encourage the supply component are done through increasing the capacity of sanitation entrepreneurs, choosing the right technology for various hygienic latrines and connecting sanitation entrepreneurs with microfinance institutions [37]. The enabling environment component is to create a conducive environment through cross-sectoral synergies; thus, people are willing and able to make behavioural changes.
The enabling environment component aims to produce policies and regulations which support the CBTS program, increase the capacity of CBTS actors and create a monitoring system for the program performance at the village level. A person's behaviour is determined by three factors, namely predisposing factors, enabling factors and reinforcing factors. Predisposing factors facilitate the formation of behaviour in a person or group of people, which includes knowledge and public attitudes related to ODF [39]. Enabling factors include facilities that support the community to stop open defecation and support the existence of ODF. The reinforcing factor is the support received by the community from community leaders who are of the CBTS actors at the village level.
There may be a number of factors influencing the ODF Villages' limited success in reducing stunting instances in Malang Regency. These conditions included the lack support of CBTS actors at the village level in triggering behavioural changes from people who previously practiced open defecation to defecate in hygienic latrines. Unimplemented regulations, laws, decrees from the central, regional and village governments were also reinforcing factors of community behaviour and were enabling environmental components. The achievement of the enabling environment component in CBTS program is not in line with the reinforcing factors in Lawrence Green's theory. The enabling environment component in which there was support from community leaders to facilitate behaviour change through regulations made or agreed with a joint commitment by local community leaders to support the implementation of the CBTS program according to local government programs and maintain the status of the village verified by ODF.
Another factor influencing the inability of ODF villages to reduce stunting cases in terms of access to sanitation is the motivation to obtain funding for sanitation infrastructure from the government or the private sector for proper latrines. In addition, the weak support from the village head, community leaders, religious leaders, sanitarians and cadres has played a role in slowing down policies at the village level that support STBM. Social support from the village government, community leaders and health workers provides awareness to the public regarding the importance of stopping open defecation [40]. Family and local community support has a high or low relationship with open defecation behaviour [41]. The inconsistency of social support enabling environment and demand components carried out by CBTS actors in villages with ODF status affected the sustainability of the total sanitation program in the area, this was probably one of the factors which led to the childhood stunting cases in villages/ urban villages with ODF status.
3.11. The Analysis of the OLS and GWR Model of Toddler’s Stunting Cases
The assumptions of residuals in linear regression test bring a result that the residuals were normally distributed and independent, but did not fulfill the identical assumptions. The identical assumptions test in linear regression was not fulfilled, thus, it illustrated that the residual variance was different and the cases of childhood stunting were spread spatially. Therefore, the analysis was carried out using the GWR method.
Based on the value of the determination coefficient (R2), the OLS model produces an R2 of 7%, which means that the regression model can explain the variability of childhood stunting cases of 7% while the remaining of 93% is explained by other variables outside the model. Modelling using the GWR method is better compared to the regression model on OLS. This can be viewed from the value of the determination coefficient (R2) in the GWR model which tends to be higher, which was 32.13%, it means that the model formed can explain the variability of childhood stunting which occurs at 32.13%. As viewed from the AIC value, the AIC generated in the GWR model was also smaller than the AIC in the OLS model, which was -64.4284.
Reviewing from the estimated model formed, there was only one model produced in linear regression, while in the GWR model, a model which was produced for each village was able to describe the condition of childhood stunting cases that occurred, thus, this model could show the significant variables obtained from each village.
Based on the analysis results from GWR modelling, it shows that the childhood stunting case is influenced by access to safe drinking water access (X1), access to permanent hygienic latrines (X2), Topography to the region (X3), access to Integrated Healthy Centre (X4), Exclusive Breastfeeding coverage (X5), Population density (X6), ODF village (X7), Integrated Healthy Centre Empowerment (X8).
CONCLUSION
The analysis of toddler stunting distribution in Malang Regency shows the influence of spatial heterogeneity with a clustered pattern in the sub-district administration area. Geographically Weighted Regression (GWR) produced a predictive model, indicating that stunting cases were locally concentrated at the village level, with adjacent areas exhibiting similar risk factors. Furthermore, the GWR modeling used several predictors, including access to safe drinking water, access to permanent hygiene latrines, altitude, Integrated Healthy Centre access, exclusive breastfeeding coverage, population density, ODF villages, and Integrated Healthy Centre empowerment. The model demonstrated an average accuracy rate of 32.13% in predicting the prevalence of stunting in both urban and rural village areas. Furthermore, the study highlights that risk factors such as safe drinking water access, permanent hygiene latrines access, altitude, Integrated Healthy Centre access, exclusive breastfeeding coverage, population density, and Integrated Healthy Centre empowerment could serve as potential predictors for stunting, while ODF risk factors had a low correlation.
LIST OF ABBREVIATIONS
| SDGs | = Sustainable Development Goals |
| GWR | = Geographically Weighted Regression |
| OLS | = Ordinary Least Square |
| ODF | = Open Defecation Free |
| VIF | = Variance Inflation Factor |
| CV | = Cross Validation |
| CBTS | = Community-based Total Sanitation |
| STH | = Soil-transmitted Helminth |
| SUN | = Scaling Up Nutrition Movement |
| SSE | = Sum of Squares due to Error |
| AIC | = Akaike information criterion |
SUGGESTIONS
The stunting prevalence is locally specific, hence the control program adapts to the local risk factors in each village. The influence of safe drinking water access, permanent hygiene latrines access, altitude, Integrated Healthy Centre access, exclusive breastfeeding coverage, population density, and Integrated Healthy Centre empowerment are general risk factors with a significant effect at a village level developed as the main predictors in Malang Regency. Further study is needed on other risk factors outside the variables, including local government policy issues, and social and economic problems on stunting. The Government needs to perform efforts of action plans for stunting control programs according to the local risk factors of each village area.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
Not applicable.
AVAILABILITY OF DATA AND MATERIALS
All data and materials has been incorporated in the manuscript. The raw data is available upon the author request [M.A].
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

