All published articles of this journal are available on ScienceDirect.

Linking Care and Support Systems to Improve Childhood Malnutrition: Early Childhood Development Practitioners’ Perceptions of Integrating Multisectoral Systems in South Africa
Abstract
Introduction:
Child malnutrition is a persistent global challenge. It is the cause of nearly 45% of global child mortalities. To ensure positive child health outcomes, integrated multisectoral approaches among families, communities, and government systems to ensure positive child health outcomes are neccesary.
Objectives:
This study identifies how different care support systems can be linked to ensure optimal childhood nutrition outcomes in South Africa. This is through multisectoral approaches from the early childhood development (ECD) practitioners' perspective.
Materials and Methods:
We integrated the components of the different support systems and multisectoral approaches. The conceptional framework of the causes of malnutrition by The United Nations Children's Fund (UNICEF) recognizes that malnutrition is due to inadequate care services, diet, and care practices influenced by individual, household, community, and structural determinants. While the Nurturing Care Framework, which looks at how policies and services can support families, parents, and other communities in providing nurturing care.
Design:
A sequential mixed methods approach was used. For the quantitative method, we did a cross-sectional descriptive analysis of 2 966 children who were under-five years' old in the 2017 South African National Income Dynamics Study (NIDS) between July and August 2022, we conducted five in-depth interviews with ECD practitioners using this qualitative method, and the data was analyzed using thematic analysis. Data was triangulated to understand the factors influencing children’s nutritional outcomes and to provide the narratives of ECD practitioners. This enabled us to highlight challenges and opportunities in linking children to services they need.
Results:
This study showed that 22.16% of children were stunted, 16.40% were overweight, and 5.04% were underweight. ECD practitioners reported a lack of support received at health facilities and other social services when making referrals, a lack of parental support in nutrition programmes, systemic challenges experienced in getting ECD centers registered, and the ECD's inability to qualify for subsidized nutrition grants.
Conclusion:
It is critical for us to understand the challenges and opportunities for multisector collaboration. This understanding will enable strategies and policies aimed at providing efficient and effective service referral and service delivery to improve childhood malnutrition in South Africa.
1. INTRODUCTION
Globally, 45% of children under five years’ old deaths are attributed to malnutrition. This represents nearly five million children dying in that age group. It goes without saying that this is a public health concern of global importance [1]. South Asia and sub-Saharan Africa account for 80% of these global under-five deaths [2, 3]. International efforts have been implemented to improve and strengthen multi-sectorial systems, including the Renewed Efforts Against Child Hunger in 2008, a UN-led inter-agency partnership with 13 countries taking part. This programme aimed to strengthen the coordination and facilitation of multisectoral nutrition programmes in various countries [4]. Other programmes, such as the Scaling Up Nutrition (SUN) Movement, which was established in 2010, aimed to end malnutrition in all its forms by uniting various government departments, businesses, researchers, civil society, and donors around the world. The SUN movement intended to have countries joining the movement committed to ending malnutrition through having multi-stakeholder partnerships and policymakers coordinating the effort to supports and scale up early childhood nutrition [5]. Up until today, 65 countries and 4 Indian states joined the SUN Movement, to focus on specific actions for nutrition. These include feeding practices, fortification of foods, micronutrient supplementation, and treatment of acute malnutrition. Furthermore, nutrition strategies such as agriculture, clean water and sanitation, education, social protection, health care, and resilience support were emphasized. The effectiveness of the programme was its ability to have political commitment from government states to prioritize nutrition on their national agenda [5, 6].
While the value of various sectors working together to improve nutrition is acknowledged, many countries face multiple challenges in coordination and implementation [7]. Therefore, in many cases, good programmes and policies are formulated at a higher level of government or international organizations [8]. However, practical implementation becomes a challenge due to multiple factors. These include corruption, lack of financial resources, unmotivated staff, lack of engagement with the people who require services the most, and lack of adequate coordination [9-11]. Therefore, the most vulnerable populations, such as children and people experiencing poverty, are the most affected. Coordinated efforts between individuals, households, government departments, Non-Government Organizations, and nonprofit organization are required to address the burden of malnutrition. This is critical because positive nutrition outcomes may have a positive impact on human development, human capital, and individuals' overall wellbeing [12, 13]. Wellbeing impacts individuals’ lives and that of their families, communities and society. The need to have different sectors working to resolve this challenge has been well recognized in the literature [14, 15].
In South Africa, evidence is sparse on how different sectors work together to reduce child malnutrition which dates back to 1994, when South Africa first became a democratic country [14]. In that year, the Integrated Nutrition Programme (INP) was first introduced and was intended to address children's nutritional needs at the population, household, community, and health facilities levels by the South African government [15]. The United Nations sustainable development goal 2 (SDG) target 2.2 aims to end all forms of malnutrition by 2020, including reducing stunting and wasting in children under five years' old. However, malnutrition is still very high in South Africa, with nearly 27% of children under five stunted, 17.1% overweight, 5.9% underweight, and 2.5% wasted [16, 17]. SDG Target 3.2 emphasizes the need to end all preventable deaths of children under-five and reduce under-five mortality to at least 25 per 1000 live births. However, South Africa has an under-five mortality rate of 32.2 per 1000 live births, and 30.9% of childhood mortalities are attributed to severe acute malnutrition [18, 19].
Little impact has been observed in programmes intended to reduce childhood malnutrition in South Africa. The country has government nutrition programmes designed to reduce child malnutrition, which have been strengthened since the emergence of democracy in 1994 [15]. They include introducing the INP, the National School Nutrition programme (NSNP), and feeding schemes. The INP was inclusive of three components, which are health, community, and nutrition promotion. However, these sectors were working in silos, and there is a paucity of evidence on whether they have successfully reduced child malnutrition [15]. The INP aimed to provide an intersectoral department collaboration with an approach to redress nutrition challenges. Therefore, multisectoral collaboration would address malnutrition’s determinants [20]. However, various scholars and members of civil society have critiqued the INP asserting that it lacked operation plans to make sure it would work across all sectors, including budgeting for staffing [21, 22]. Although programmes are in place to reduce child malnutrition, bottlenecks still hinder program implementation [23]. Previous studies have argued that nutrition programmes have long been available; however, their main focus was on food provision through the distribution of food parcels [8, 9, 24]. While these efforts directly dealt with the issue of food access, they ignored the role of the underlying factors associated with child malnutrition. These factors included poverty, illness, lack of maternal and child care, access and health service utilization, and access to clean, safe, and healthy environments.
The National Nutrition Security Plan of 2018- 2024 addresses food insecurity through a coordinated approach encompassing government departments such as social development, primary education, health, and agriculture [25]. Furthermore, the country has made provisions such as social grants and cash transfers to improve childhood malnutrition [26]. While the INP aims to facilitate cross-sectoral collaboration, effective planning and budgeting have not been observed in meeting nutrition goals. To improve child health, there is a need to strengthen and coordinate mechanisms such as interagency coordination, policy integration, data sharing and monitoring systems as well as community engagement across all government and non-government departments. The multifaceted nature of undernutrition necessitates multidimensional interventions that transcend sectoral lines. Therefore, eradicating malnutrition among children should remain a priority for government departments, and nutrition-related policies should receive significant attention. First, there is a need to understand the role of other sectors, such as health, social welfare, early childhood development centres (ECDs), and education. Secondly, there is a need for various sectors need to commit to using their resources and capabilities to help reduce child malnutrition. Therefore, this study aims to understand how different sectors can be linked to improving the nutritional outcomes of children under five.
2. CHILD MALNUTRITION AND MULTIFACETED INTERACTIONS OF FACTORS: SOME THEORETICAL PERSPECTIVES
The framework presented in Fig. (1) below is the adaptation of the 1990 United Children’s Fund (UNICEF) conceptual framework of the causes of malnutrition and the Nurturing Care Framework established in 2018. The UNICEF’s conceptual framework explains the multifaceted interaction of distal and proximal factors in understanding child malnutrition [27]. On the other hand, the Nurturing Care Framework provides a direction for childcare using evidence-based research. Furthermore, it explains how services and policies can help support parents, families, and communities in nurturing care [28]. Both these frameworks are relevant as they show that the child's nutritional status is beyond their food access. They also suggest that different systems can work together to improve nutrition and allow children to achieve optimum development. Fig. (1) depicts the complex interactions between the individual household and family, health, environment, and social systems. The dotted lines represent a moderation among these systems. Besides ensuring that children have adequate nutrition, linking various care systems will be essential to ensure good health, offer security and safety, and provide responsive caregiving. The broken arrows that point to optimum nutrition show that national responses to the different childcare structures may influence the children’s nutritional outcomes. The solid lines show direct pathways from the nutrition-enabling environment to the various systems that may influence child malnutrition. Based on the theoretical insights from the two adapted frameworks, this study hypothesized that for a child to grow and meet the optimum development, multiple systems must work together, including families, in providing nurturing and care to improve children’s nutritional outcomes, thus suggesting a need for a multisectoral approach in childcare and nutritional outcomes.
Fig. (2) below is a further illustration of Fig. (1) above. It depicts an expanded explanation of the underlying determinants of child malnutrition at the individual, household, and community levels. These determinants fall within the family, health, environmental and social systems.
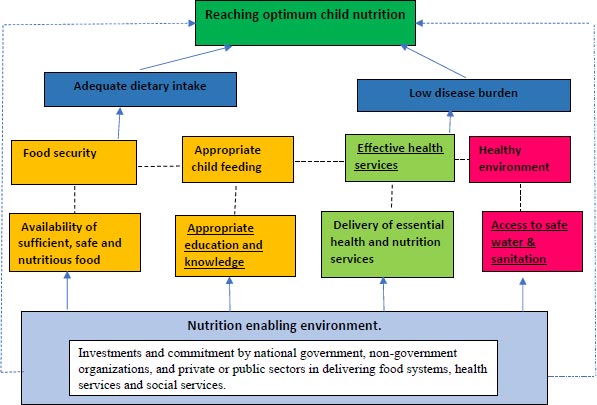
Source: Authors’ adaptation of UNICEF, 2013 and WHO, 2018.
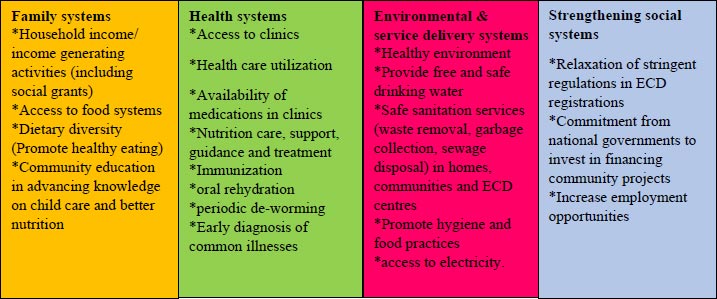
Adapted from USAID Multisectoral nutrition illustrative examples (USAID, 2014).
3. MATERIALS AND METHODS
3.1. Study Design and Setting
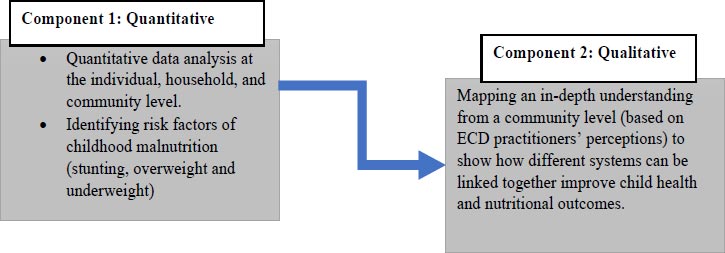
This study adopted a mixed-methods sequential analytical study design and combined the quantitative and qualitative methods. Fig. (3) above illustrates how the mixed-methods sequential study design was implemented. The advantage of this mixed-method approach was that it allowed for combining both qualitative and quantitative research methods. Additionally, a mixed methods approach allows for the completeness of the overall findings [29]. It offers an in-depth understanding of the ECD practitioners’ lived experiences in childcare and captures the complexities experienced when making referrals to other sectors. For the quantitative approach, this study used data from the National Income Dynamics Study (NIDS) Wave 5 conducted in 2017. DataFirst granted permission for the authors to use the NIDS data. The sequential study design allowed first for analyzing the secondary data of the NIDS wave 5-panel dataset. Results from the quantitative analysis informed the types of questions to explore in the in-depth interviews.
South Africa is selected as a country of analysis by the authors. The country has the highest income disparities and inequality globally [30]. The NIDS is a panel study conducted in all nine provinces in South Africa every two years. Five waves of data have been collected between 2008 and 2017. The three main questionnaires utilized in this study were for the household, child, and adult. Data were merged to obtain all variables of interest, including the anthropometric measurements (height and weight) of the children. This study was conducted in the Limpopo and Gauteng provinces for the qualitative component. The rural site was in Capricorn District, North of Limpopo, in a village called ga-Masemola, Sekhukhune. These two sites demonstrated the most need for services based on socioeconomic characteristics. Ga-Masemola is a poor rural community characterized by a lack of adequate infrastructure and experiences service delivery problems such as poor sanitation and water shortages from time to time. The urban site was in Thulani (Snake Park or Doornkop). Thulani falls under Ward 50, region D and compromises of formal RDP houses (which are government subsidized) houses, informal backyard shacks, and small sections of informal settlements, which do not have legal recognition (Patel et al., 2012). The researcher purposefully selected these areas due to their accessibility.
3.2. Quantitative Component
The quantitative component entailed the cross-sectional secondary data analysis of the NIDS wave 5-panel dataset. Furthermore, the component shows the children’s context, individual-level characteristics, home context, and community setting. These background characteristics enable us to see the risk factors driving childhood malnutrition. They are critical as they show how the different care systems can be linked and work together to improve child nutritional outcomes.
3.3. Study Population and Inclusion Criteria
Data were restricted to dyads of 2 966 mothers aged 15-49 years and their children under-five with complete anthropometric figures. Data for children who were alive during the survey and were born five years before the survey were included in the analysis.
3.4. Sample Design
The 2017 NIDS wave five data used the stratified, two-stage cluster sample design to select the dwelling units to be visited. A sample of 400 Primary Sampling Units (PSUs) was drawn in the first phase from Statistics South Africa’s 2003 Master Sample of 3000 PSUs. When the Master Sample was compiled, eight non-overlapping samples of ten or twelve dwelling units were systematically drawn within each PSU. In the first stage, 400 PSUs had to be drawn from the 3000 PSUs in the Master Sample. The explicit strata in the Master Sample are the 53 district councils (DCs). The sample was proportionally allocated to these 53 strata, and PSUs were selected within strata with probability proportional to size (Woolard et al., 2010).
3.5. Survey Questionnaires
This study used three questions from the NIDS study: the household, child, and adult questionnaires. All the questionnaires were merged during data curation to allow for data analysis.
3.6. Dependent Variables
The outcome variable for this research is child malnutrition. It is measured using the World Health Organization (WHO) child growth standards. Malnutrition is measured using the indicators of stunting (defined as low height-for-age), overweight (high weight-for-height), and underweight (low weight for age) [3]. Table 1 below shows the measurement of the malnutrition indicators.
3.7. Independent Variables
Selected independent variables were analyzed at the individual level (age, sex, birth weight, access to medical aid, child support grant recipient, mother’s employment, marital status, level of education, ethnicity, religion), at the household level (household income, number of people living in the house, living arrangements, family support) and community level (residence type, access to services, access to water and electricity, community safety, community cohesion). The analysis was guided by the framework presented in Fig. (1) and depicts the linkages between family, health, environmental and social systems.
3.8. Data Analysis
Through frequency tables and charts, descriptive analysis was produced to show the levels and patterns of childhood malnutrition. The statistical software, STATA version 17 was used as data analysis software. The Chi2 tests statistic of association was also used to determine the significance level between the outcome variables and independent variables.
4. QUALITATIVE COMPONENT
The qualitative component of this study was completed next. It involved using a qualitative method. In-depth interviews using structured topic guides were used to explore The perception of ECD practitioners, perceptions about how they thought other care and support systems could be linked to improving childhood malnutrition. The aim of using semi-structured questionnaires was to ensure that the main themes the researcher was interested in were covered in the interviews while allowing for open-ended questions and flexibility in data collection. Table 2 below is an overview of primary data collection.
| S/N | Variable | Definition | Measurement |
|---|---|---|---|
| 1 | Stunting | Stunting was measured using the WHO Child Growth Standards of -2 standard deviation lower than -2 | This is a binary outcome. 0 “Not stunted.” 1 “Stunted” |
| 2 | Underweight | Defined as a weight for age less than -2 standard deviation according to the WHO Child Growth Standards | This is a binary outcome. 0 “Not underweight.” 1 “underweight” |
| 3 | Overweight | Defined as a weight for age of over 2 standard deviations | This is a binary outcome. 0 “Not overweight.” 1 “Overweight” |
| Study Site | Participants | Data Collection Method and Tool | Description of Data |
|---|---|---|---|
|
Urban Thulani Johannesburg- Gauteng Province |
Three ECD practitioners | Face-to-face qualitative in-depth interviews using a semi-structured interview guide | Issues covered: *Childcare practices * Strengthening the family and community to improve malnutrition *Linking different systems to strengthening childcare and health outcomes *Challenges face ECD institutions in providing childcare |
|
Rural Gamasemola -Capricorn District Limpopo Province |
Two ECD practitioners |
4.1. Study Participants and Recruitment
The ECD practitioners were recruited through the community ECD Forum, The researcher was allowed to present the her PhD research project in the community meeting. The presentation highlighted the importance of childcare, health, and the dangers of child malnutrition. Interested practitioners volunteered and completed the screening form and consent form to participate.
4.2. Sampling Strategy
The snowball sampling strategy was used to identify study participants. For this study, ECD practitioners were recruited because they were the primary carers of children under-five outside the home setting. The quantitative results showed that children in ECDs presented with better health outcomes than children cared for at home. In Thulani, the researcher identified the community leader, who referred the researcher to the ECD forum. The ECD forum is a platform where the ECD practitioners in the community come together to share their experiences, share information, and experiences on their lived experiences as childcare workers. This meeting is held bi-monthly. In Gamasemola, the researcher identified one ECD center, and purposive snowballing was used to determine the other two centers.
4.3. Sample Size
This study formed part of a larger PhD project that focused on the social context of childhood malnutrition. For this study, a sub-section that focused on those who care for the child in formal institutions outside the home setting, a total of 10 ECD centers were sampled. Five in-depth interviews with ECD practitioners were conducted. In Thulani, initially, six practitioners from ECD centers volunteered. However, half of the ECD practitioners could not be reached during the data collection phase, leaving only three practitioners to be interviewed. In Gamasemola, three ECD practitioners were recruited. Due to the absence of the third ECD practitioner during the data collection phase, only two interviews were conducted.
ECD practitioners were recruited because they lived in the community, worked in the ECD center, and had at least five years of experience in childcare.
4.4. Qualitative Data Collection
4.4.1. Study Tools
The semi-structured interview guide was used. The advantage of this method is that it guides the conversation and at the same time allows the participants to express themselves because of the method's open-ended nature.
Interviews ranged between 45 minutes to 90 minutes. In Limpopo, the interviews were conducted in seSotho as people in the local area were more familiar with Northern Sotho. However, in the urban site, both isiZulu and Sesotho were used in the interviews. All the interviews were recorded and later transcribed and translated into English. The researcher also wrote field notes and recorded her observations during interviews.
The interviews were one-on-one and held at the ECD centers to make it convenient for the participants.
Privacy was maintained with only the researcher and participant in a quiet space during the interview. Participants were also assured that their names would not be included in the final research report. All the interviews were recorded and later transcribed and translated into English. The researcher also wrote field notes and recorded her observations during interviews. After the interview, the researcher wrote summaries of the discussions and highlighted the key emerging points.
4.5. Qualitative Data Analysis
The researcher used field notes and transcripts to do manual coding. The data coding followed the conceptual framework of this study as a guide to identifying a group of emerging themes related to linking different care and support systems to improve child nutritional outcomes. The major themes were highlighted and copied to an Excel sheet. Data charting was also done simultaneously. The deductive coding was used during data analysis, and the code tree was established. New codes were also established when they did not fit pre-existing code trees. Thematic analysis was used for the analysis of this study. This study explored themes on childcare practices, social systems strengthening, service delivery, and community and family strengthening.
5. RESULTS
Table 3 describes the outcome variables and presents their mean and standard deviations. As presented in Table 3, stunting was the highest amongst children under 5 (22.16%) compared to the indicators of overweight (16.40%) and underweight (5.04%).
Table 3.
| Childhood Malnutrition | |||
|---|---|---|---|
| Stunting | |||
| Not Stunted | Stunted | Total | |
| Frequency | 2,309 | 657 | 2,966 |
| Percent | 77.8 | 22.16 | 100.00 |
| Length/Height-for-age | - | - | - |
| Mean | -0.39 | -3.09 | -1.02 |
| Standard deviation | 1.84 | 1.50 | 2.11 |
| Overweight | |||
| - | Not overweight | Overweight | Total |
| Frequency | 2 479 | 487 | 2 966 |
| Percentage | 83.60 | 16.40 | 100.00 |
| BMI- for age | - | - | - |
| Mean | 0.24 | 3.68 | 0.80 |
| Standard deviation | 1.23 | 4.49 | 2.48 |
| Underweight | |||
| - | Not Underweight | Underweight | Total |
| Frequency | 2 816 | 150 | 2 966 |
| Percent | 94.96 | 5.04 | 100.00 |
| Weight-for-age | - | - | - |
| Mean | 0.04 | -2.73 | -0.11 |
| Standard deviation | 1.85 | 0.93 | 1.91 |
| Variable | Categories | Frequency | Percentage |
|---|---|---|---|
| Maternal age (in years) | 15-24 25-29 30-34 35-39 40- 49 |
497 604 602 417 847 |
16.74 20.36 20.28 14.06 28.55 |
| Marital status | Married/Living with a partner Single/divorced |
775 2 191 |
26.13 73.87 |
| Mother's biological children | one child two children three children four children five children and above |
1 093 845 564 239 225 |
36.86 28.48 19.02 8.07 7.58 |
| Medical aid | Yes No |
297 2 669 |
10.02 89.98 |
| Level of education | No schooling Primary schooling Secondary schooling Tertiary schooling |
81 337 1 850 698 |
2.74 11.35 62.37 23.54 |
| Employment status | Yes No |
1 252 1 714 |
42.22 57.78 |
| Current activity | Student/other volunteer Ill/homemaker Unemployed-active Unemployed - discouraged. Employed |
207 374 682 452 1 252 |
6.97 12.61 22.98 15.23 42.22 |
| Water sources | Water carrier/other Public tap Piped water at home |
186 389 2 389 |
6.27 13.12 80.61 |
| Toilet type | None/bucket Chemical/ pit-latrine Flush toilet |
102 851 2011 |
3.44 28.72 67.84 |
| Household electricity | Yes No |
2 682 282 |
90.48 9.52 |
| Variable | Categories | Frequency | Percentage |
|---|---|---|---|
| Child's Age in months | 0-11 months 12-23 months 24-35 months 36-47 months 48-59 months |
306 584 613 698 765 |
10.31 19.67 20.68 23.53 25.80 |
| Race | African Mixed race White/Indian/Asian |
2 275 406 285 |
76.69 13.69 9.62 |
| Illness episode | No Yes |
2 609 357 |
87.98 12.02 |
| Sought health care | Yes No |
233 103 |
69.21 30.79 |
| Reason for not seeking care | No time/resources Already on treatment Child is not sick enough |
18 20 63 |
17.67 20.18 62.15 |
| Child day-care | In school Creche/day mom At home |
243 730 1 994 |
8.19 24.60 67.22 |
| Child support grant | No Yes |
576 2 390 |
19.41 80.59 |
| Medical aid | Yes No |
205 2 759 |
6.91 93.09 |
| Characteristics | Child Malnutrition | ||
|---|---|---|---|
| Child Stunting | Child Overweight | Underweight | |
| Child's age in months 0-11 months 12-23 months 24-35 months 36-47 months 48-59 months Χ2 p-value |
16.05 33.43 25.08 19.25 16.31 0.001*** |
22.26 32.69 20.29 8.63 5.62 0.001*** |
6.14 3.40 4.17 4.66 6.90 0.326 |
| Disease episode No Yes Χ2p-value |
21.83 24.62 0.496 |
16.6 15.01 0.651 |
5.05 4.98 0.964 |
| Child support grant No Yes Χ2 p-value |
17.26 23.34 0.029* |
16.29 16.43 0.951 |
4.07 5.28 0.448 |
| Medical aid No Yes Χ2 p-value |
11.36 22.99 0.002** |
16.89 16.39 0.879 |
2.7 5.22 0.144 |
| Care during the day In school (Gr R/1) Creche/day mom At home Χ2 p-value |
14.29 17.08 24.98 0.005** |
5.79 12.88 18.99 0.002** |
11.24 2.98 5.04 0.012* |
The summary statistics giving descriptive background information on the caregiver and the household are presented in Table 4 above. A total of 2 966 women aged 15-49 were surveyed. The majority were single or divorced (73.87%), had no medical aid (89.98%), had up to the secondary level of education (62.37%), were unemployed (57.78%), and just above a quarter (28.72%) lived in households that use pit-latrines as toilets.
Table 5 above, shows that most The majority of children were cared for at home during the day (67.22%), received the child support grant (80.59%), and had no medical aid (93.09%). Nearly a quarter of children were cared for at creches during the day (24.60%). Of the children who were ill, 30,79% caregivers did not seek health care. The highest cited reason for no care was that the child was not sick enough (62.15%).
Table 6 presents the bivariate analysis of selected caregiver and child level characteristics and the nutritional outcomes of stunting and child overweight. We find that the age of the child and where the child is cared for during the day is significantly associated with child stunting and overweight. However, variables such as the child support grant and medical aid were the only variables associated with child stunting.
5.1. Qualitative Component of this research
Five in-depth interviews with key informants who were ECD practitioners were conducted. The key informants were between the ages of 35 and 50 years. Their experience running the ECD centers ranged between eight and twelve years. One of the five ECD centers was not registered with the Department of Social Development. The number of children in ECD centers varied between 20 to 76 children. Rural areas have the highest number of learners enrolled in the ECD centers, ranging from 60 to 76. On average, the ratio of ECD practitioners to children was 2 -30 or 4-60+.
In our mixed methods research approach, four broad themes were drawn from the qualitative interviews with the ECD practitioners. (1) Strengthening family systems: parental involvement in the care of their children, (2) Linking health systems to improve child malnutrition, (3) Environmental health systems: Service delivery, (4) Strengthening social systems: addressing barriers to ECD registration. The themes and sub-themes are described in detail below:
5.2. Family Care Systems: Parental Involvement in the Care of their Children
The child’s home setting was an important influencing factor in a child meeting their optimal nutrition. Children live in diverse home settings with complex family dynamics. These dynamics ranged from multidimensional households, single-parent-led homes with absent fathers, skipped generations due to orphanhood, parental absenteeism due to labor or educational migration, multiple nuclear families in one yard, and the emergence of teenage motherhood. In the urban areas, absent fathers were more prevalent. However, in the rural areas, the father was not present due to labor migration. The household socioeconomic status (income), size, and knowledge of child feeding practices majorly influence the quality of children’s care, health, and nutrition. While it was evident that the children lived in homes with multiple family members, it was clear that the grandmother was the next most available person to take care of the child in the absence of a biological mother.
“You see, it is very rare for you to see a child being dropped off or being picked up by a father. In the morning, most of the children are dropped off at the crèche by their mothers. In the afternoon, you will see the children being picked up by their older siblings on their way back from school. Even just for fetching them, they can send anyone to fetch the child, and we fight the parents every time. And you’ll see with the time they fetch the child that there’s no one at home. This child is 10 or 8 and has the key. Imagine that if someone is watching, who wants to do something to these kids, what would happen?”
ECD practitioner. MZ1,502, Thulani3.
In addition to the family care system and the household shortage of income, lack of parental involvement and knowledge about nutritious foods was perceived as the cause of undernutrition among children. In the rural setting, caregiver involvement was more problematic than in the urban setting. Lack of parental/caregiver attendance at ECD meetings means they missed important information, including the child’s progress and nutrition status, especially when the nurses came to schools to do assessments.
“Sometimes I call the parent to come to the crèche so that I can report a problem that I have picked up with the child. But some parents choose not to come. But sometimes they do not want to come because they owe fees, so they send the siblings of the child. There is not much I can speak with the sibling, um, I mean, they are a child. There is nothing further that I can do about it. So, I just leave it as it is”.
ECD practitioner MK,45, Gamasemola
5.3. Linking Health Systems to Improve Child Malnutrition
There was a great demand and an unmet need for health services in urban and rural settings. While ECD practitioners acknowledged that health practitioners occasionally came to the ECD centers for growth monitoring, nutrition assessment, and vaccine rollout, these procedures were only done once a year. In their opinion, there was a need to have constant monitoring and follow-up of the children with nutritional deficiencies was necessary. This is because the follow-up may lead to referrals and combat child underweight or child overweight. ECD practitioners also mentioned that while the health practitioners visiting the crèches did referrals when a child's health challenge was identified the choices or decisions for healthcare utilization were based on the prior service that the caregivers had received from the clinic. The caregivers in Thulani reported that the staff’s bad attitudes, long queues, medication shortages, and maltreatment were by the barriers to health-service utilization, particularly in urban areas.
“We do not wait for the nurses to come to the crèche to do assessments. When we see that something is not right with the child, we advise the mother to take them to the clinic. Sometimes when the child’s parents get to the clinic, they do not get help for their children, or they are just given panado. The problem is the same even for us as practitioners; when
1 Pseudonym initials Identifier.
2 Age of the participants.
3 Name of place of interviewee.
ECD practitioner LT,39, Thulani
5.4. Environmental Systems: Addressing Lack of Service Delivery
ECD practitioners also illustrated that keeping the environment clean and having access to clean drinking water can help improve children’s health outcomes. While ECD practitioners in the rural setting reported the problem of water shortages, the ECD practitioners in the urban setting reported challenges with the water, electricity, and waste management in their area. There were challenges with garbage removal which was not always done timeously on the set days, frequent water interruptions would happening without prior notice, and the water taker sent to the community was not always accessible to everyone. Routine water cuts resulted in the ECD practitioners being forced to close the crèches because of hygiene issues on the days when there was no water.
“Here in Thulani, we do not have electricity. In fact, we have not had electricity since one year ago. People do not want to pay for electricity, so Eskom [electricity provider] cut us off. It is very difficult for us to manage to preserve our food. This also affects the quantity of the food that we buy. It’s boring to always go to people’s houses to put your meat or food in other people’s fridges. It is a lot of work to be going up and down fetching the food, so ECD practitioner we make sure that we finish the food that we have cooked.”
ECD practitioner NC, 51, Thulani
ECD practitioners in rural Limpopo expressed their views of how water shortages affect food preparation, and sanitation in rural Limpopo. Their lack of access to water has impacted their food preparation. and hygiene as the caregivers need to wash their hands in clean water before carrying children, after changing nappies and before preparing food.
“The shortage of water is a problem. At first, the municipality used to open the communal taps once a week, every Sunday. Since the beginning of this year, the taps no longer have water. We are relying on Jojo tanks to get rainwater which are now running dry because it is winter and there is no rain.”
ECD practitioner MK,45, Gamasemola
5.5. Strengthening Social Systems: Addressing Barriers to ECD centre Registration
ECD practitioners found the ECD centre registration process strenuous, This impacts on the young children’s optimum development. The ECD practitioner whose crèche was not registered expressed how she was denied the nutrition grant for her ECD because of structural challenges and space. The yard space plays a critical space in the application process, as Thulani was previously an informal settlement that later developed into government-subsidized structures. Therefore, the issue of the yard space in urban areas was more problematic than it was in rural areas.
“This crèche does not have a permit to operate yet. Although it is registered as a nonprofit organization, there are still compliance issues that the Department of Social Development (DSD) has, which make it difficult for us to follow. This crèche does not receive the nutrition grant. Therefore, I have to rely on the child school fees of R400 a child per month. Sometimes I don’t even know whether that money will come or not. As you can see, the crèche is a safe space for children to be cared for. Children who are not in crèches roam around the streets- what is worse is that we do not even have safe areas to play here in this community. Empty spaces have become rubbish dumping sites”. Our local government does not care about the ECD center. You can see even during Covid-19, all schools and employment sectors were told they could return to work, just not ECD” sector.
ECD practitioner MT,51, Thulani
In addition to wanting the relaxation of the stringent ECD registration laws, ECD practitioners expressed the unmet need for income-generating opportunities in the communities that they lived in. They also felt that the government needed to be more involved in creating employment opportunities for the people who reside in both rural and urban communities. Both research sites were characterized by high poverty levels, unemployment, and dependence on social grants as a source of household income. In many cases, the social grant income is insufficient to accommodate the children's or the family's needs. They said that the high poverty levels also perpetuate high crime rates.
6. DISCUSSION
This study provided a mixed methods analysis of the linkages of different care systems and the ECD practitioners’ perceptions of how these systems can be linked together. We found that childhood malnutrition was staggeringly high, characterized by high stunting, overweight and underweight of children under five years’ old. Stunting and overweight results remain unchanged compared with the South African National Health and Nutrition Examination Survey conducted a decade ago [31]. Our qualitative assessment helped us to identify four critical childcare systems: the family, health, environmental and social systems. However, our study has found growing disintegration of childcare and support systems services. This disintegration is not only present in South Africa but also in many sub-Saharan countries. For example, a study conducted in Mozambique by Michaud-Létourneau and Pelletier supports our findings. It also found a lack of understanding of the meaning of “coordination” and the lack of understanding of roles and responsibilities in “coordinated” care among different sectors responsible for childcare service provision. The same study found this lack of integration in care services has resulted in children facing multiple adversities, including poverty, poor nutrition, and poor health outcomes (Michaud-Létourneau & Pelletier, 2017).
Regarding the health care systems, our findings show that some caregivers sought care when their children were ill. From the quantitative component, a small proportion of those who did not seek care cited “the child was not sick enough” as their main reason for lack of health care utilization (HCU) for their children. We also found that just over 90% of children had no medical aid access. Prior studies have indicated that children under-five morbidities and mortalities were due to preventable causes and the lack of timely HCU, which can contribute to these adverse health outcomes [19, 32, 33]. Similar to what has been found by other studies, the ECD practitioners also explained that sometimes they pick up health challenges with the child and refer the parents/caregivers for health care. However, they faced poor staff attitudes, lack of medication, long queues, and parents being turned away at local clinics [34,35]. The literature also supports our findings on the lack of HCU which, suggesting an overstretch in the health system, especially in South Africa, where over 80% of the population relies on the public healthcare provision [34]. According to Wendimagegn and Bezuidenhout, government healthcare services should provide promotive, preventative, curative, and rehabilitative services [36]. A global study conducted on low middle-income countries (LMICs) found that the quality of care for vulnerable populations such as the poor, less educated, and those with stigmatized conditions was worst compared to non-vulnerable populations. Mothers and children during preventative or curative clinic or hospital visits were given less than half of the recommended clinical interventions [37]. Therefore, service gaps at healthcare facilities due to under-resourcing and overcrowding highlight an urgent need to coordinate policies targeting service delivery issues in the health sector [38].
We also found a significant relationship between children being overweight and being cared for at home during the day. Children at ECD centers presented with better health outcomes than children cared for at home. In South Africa, registered ECD centres are regulated to ensure that children at least receive a healthy breakfast and lunch. Additionally, centres in-low income settings where children receive a CSG, can benefit from a nutrition government grant of R17 a day per child [40]. ECD centers can protect against childhood malnutrition, cognitive deficits, and academic underachievement resulting from poor nutrition [39]. However, the ECD practitioners expressed frustration with the bureaucracy of registering the ECD centers. For example, to qualify for the ECD permit and registration, centers must have enough area per child space indoors and outdoors, the class-to-teacher ratio should be 1:6 children, and a separate area for cooking and meal preparation. Unregistered centers do not qualify for the ECD nutrition grant of R17 per child per day. This means centers rely on the school fees they receive. Due to caregiver unemployment, the payment does not come on time or does not come at all. In South Africa, the Department of Education ECD census in 2021 found that only 42% of the ECD centers were registered, and only a third received the nutrition grant subsidy [40]. The restrictive laws and regulations in registering ECD centers make it challenging to deliver effective and quality childcare services They also serve as a barrier to the integration of the care system, thus making it difficult to improve children’s nutritional outcomes.
Although our data show that children in ECDs have better health outcomes, the family system is critical to improving child nutrition. The ECD practitioners reported challenges with parental involvement and partnerships, where the caregivers would not attend meetings when requested and would have older siblings collect their children. ECD practitioners perceived this as a lack of care for the child’s safety. According to the Epstein model of parental partnerships, parental involvement includes communication, school involvement, shared decision-making within the school, and community partnerships. This study found that children whose parents were involved in their care and education had better developmental outcomes, such as demonstrating social competence, communication, and extended development beyond education [41]. This study has proven that parental involvement is critical because it makes referrals easier, particularly when an ECD practitioner notes a child's problem with a child that needs attention. A study conducted in Ethiopia found that the mother’s low number of children ever born, high socioeconomic status, and level of education were associated with responsive caregiving [42]. In South Africa, a study conducted on the livelihood activities of informal traders found that mothers felt they had no choice but to look for more cost-effective ways to ensure their children are cared for. This includes the older sibling caring for the younger children. This is because caregivers are expected to make additional payments at the ECD centers after a particular number of hours, which can be expensive. Therefore, the next available childcare arrangement in the mother's absence is care by the older sibling [43, 45].
Both Soweto and Gamasemola areas were characterized by high poverty and unemployment rates. This study found unemployment among caregivers to be heightened by nearly 60%. Families and caregivers cannot meet their children’s basic needs because of the lack of income. All ECD practitioners spoke of the importance of increasing opportunities for employment and argued that this also would decrease the rising crime rates observed in their communities. Furthermore, environmental systems, such as access to water and electricity, affect hygienic food preparation and nutritional diet. A study conducted in South Africa found that lack of electricity affected how food was stored. Studies have found that inadequate food storage may result in infections, such as diarrhea, a low immune system, and child malnutrition [44,45]. The significant concerns reported in the rural ECD centers were the issue of water and sanitation. In Limpopo, the primary concern was the lack of water. At the time of this research, the ECD practitioners reported that they had no water provision, the communal taps were dry, and they received no announcement from the municipality about providing water, which is part of our Bill of rights. Water was only accessible from the river, which was also running dry due to the shortage of rain. Lack of water affects Children and staff's sanitation and hygienic food preparation, because the water needs to be reused to ensure that it lasts longer. Soweto occasionally gets water shortages, but the challenge is not as severe because the municipality provides water tanks, even though they do not always come as scheduled. Some ECD practitioners reported that they are forced to close the ECD centre for hygiene protocol on the days when there is no water. This may put the children at risk of being at home and not receiving the care they need.
7. STRENGTHS AND LIMITATIONS
Our study’s primary strength was the mixed-methods approach and design, which thoroughly evaluated the factors contributing to child malnutrition and the caregivers views on how different care systems can work together. The rural-urban communities’ inclusion gave insight into the different contexts in which children are brought up and the services they need. These two settings are geographically diverse regarding their availability and access to services, such as (health, education, environmental, and social development services). The limitation of the study is that the qualitative component was only conducted in the Gauteng and Limpopo province. Although the NIDS data was intended to be nationally representative, it was not designed to be provincially representative. Therefore, the results cannot be generalized. Another observed limitation of using qualitative methods was the discussion of delicate subjects such as childcare practices, nutrition, and ECD financing.
To some extent, the researcher’s presence contributed to participant bias, influenced by the respondent’s knowledge of the “right” answer. This bias resulted in ECD practitioners over reporting on the nutrition given to children in ECD centres. A limitation observed from the quantitative analysis was the absence of information on birth spacing and mother’s health information. This information would have been useful to understand these factors’ influence on children’s nutritional outcomes.
CONCLUSIONS AND RECOMMENDATIONS
The coordination of different sectors of care for children is urgently needed. Understanding the challenges and opportunities for collaboration in different sectors from ECD practitioners’ perspectives is critical because they provide secondary care to children without primary caregivers. This understanding will enable efficient and effective service referral and service delivery to improve childhood malnutrition in South Africa. This study highlights the need for continuity and coordination of food, family, and health, systems. While there is a need for systems strengthening, there is also a need for triangulation using the available data to understand the various functions of childcare systems. The evidence-based nurturing care framework builds on the knowledge of how child development unfolds and the int erventions and policies that can improve child malnutrition [28]. When these systems work together, they have the potential to meet the physical, emotional, social, and educational needs of children. Multiple shifts in government departments, such as as providing administrative support to ECD centres to get registered should be implemented to ensure ECD centres are accessible to all children, in the same way that education is prioritized. This is more important given that ECD centers are protectors of adverse child health outcomes, as this study has shown. Some strategic pathways for priority investments and me development to improve child malnutrition include: 1) Improving access to healthy foods - in rural areas and encouraging food gardens in urban areas; 2) developing nutrition education programmes and training health workers to deliver adequate nutrition services to address nutritional needs in both urban and rural areas; 3) investing in water and sanitation infrastructure, particularly in rural areas, to ensure access to clean water and sanitation facilities; and 4) encourage cooperation between government, non-governmental, civil society, and the corporate sectors to make use of resources, and available information for the successful implementation of nutrition programme, as well as engaging communities in the planning, implementation, and monitoring of interventions to ensure their sustainability.
NOTES
1 Pseudonym initials Identifier.
2 Age of the participants.
3 Name of place of interviewee.
LIST OF ABBREVIATIONS
| ECD | = Early Childhood Development |
| NIDS | = National Income Dynamics Study |
| SUN | = Scaling Up Nutrition |
| INP | = Integrated Nutrition Programme |
AUTHOR CONTRIBUTIONS
Conceptualization, MS, SA, and C; methodology, MSS, SA, COO; software, MS; validation; formal analysis, MS; investigation, MS, SA, and CO; resources, MS; data curation, M; writing—original draft preparation, M; writing—review and editing, MS SA, CO; visualization, MS; supervision, SA and CO; project administration, M; funding acquisition, MS All authors have read and agreed to the published version of the manuscript.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The ethical approval was obtained from the University of Witwatersrand Human Research Ethics Committee (Non-medical H21/04/34). Informed written consent was also obtained from ECD practitioners.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committees and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Informed written consent was obtained from ECD practitioners and caregivers, and assent for minor caregivers was given.
AVAILABILITY OF DATA AND MATERIALS
The identified data that were used for generating the results in this manuscript can be obtained from the National Income Dynamics website (http://www.nids.uct.ac.za/ nids-data/data-access)
FUNDING
This research was funded by the National Institute for the Humanities and Social Sciences, The National Research Foundation, and the Carnegie Corporation of New York.
ACKNOWLEDGEMENTS
Declared none.

