All published articles of this journal are available on ScienceDirect.

Exploration of the Prevalence and Profile of Suicide Cases in the Population of Northern Morocco (2017-2022)
Authors Info & Affiliations
Abstract
Background:
Suicide, a complex phenomenon that constitutes a major public health issue, has been increasingly prevalent in the Moroccan context. Against this backdrop, this study examines the prevalence and profile characteristics of suicide cases in the northern region of Morocco.
Methods:
Employing a retrospective research design, we analyzed data from the forensic unit service in three provinces over six years, yielding a sample of 480 suicide cases. Data were subjected to statistical analysis using the SPSS software version 23, involving the bilateral Pearson Chi-square and independent t-tests.
Results:
Our findings reveal that suicide predominantly affects men (75%), who are typically unmarried (56%), residing in rural areas (75%), and having low levels of formal education (84%), with a majority being unemployed (57%). Hanging was the predominant method used to commit suicide (93%). Additionally, while psychiatric disorders had been diagnosed in 42% of cases, only 29% were receiving psychiatric care. Notably, suicide rates displayed an unexpected seasonal variation, peaking during the spring season and reaching their maximum in June.
Conclusion:
In conclusion, our study underscores the relevance of young and adult males from rural areas who are single, lacking education, unemployed, and not receiving medical care as the most vulnerable population segment regarding suicide. Further multidimensional research encompassing psychological, social, cultural, and economic factors could advance the formulation and implementation of effective suicide prevention policies.
1. INTRODUCTION
Suicide is the leading cause of violent death [1], as defined by the World Health Organization (WHO). It is considered a public health priority due to the alarming increase in suicide cases and suicide attempts, which have risen by 60% over the past 45 years [2]. Suicide accounts for 1.4% of all deaths worldwide, representing more than 700,000 deaths yearly (equivalent to one suicide every four seconds), surpassing the annual number of deaths resulting from wars and homicides combined, and ranking as the fifteenth leading cause of mortality globally. It is among the top three leading causes of death among individuals aged 15 to 44 years and the second leading cause among young people aged 10 to 24 years in some countries. The WHO estimates that deaths by suicide could reach 1,007,000 per year by 2030 [3]. The idea that the suicide rate is higher in high-income countries than in low- and middle-income countries (LMICs) has been refuted, especially given that LMICs account for 75% of suicide cases [3]. The standardized suicide rate projected by the WHO for 2019 was 11.2 per 100,000 in African regions, 10.5 per 100,000 in Europe, and 10.2 per 100,000 in Southeast Asia, all of which exceed the global average of 9.0 per 100,000 [4]. However, the rate was recorded at 6.4 per 100,000 in the Eastern Mediterranean region. These alarming figures demonstrate the urgent need to address this escalating behavior according to the recommendations of the WHO and UN via the Global Mental Health Action Plan and the third Sustainable Development Goal [5].
The situation in Morocco is similarly grave, with a rate of 7.2 per 100,000 inhabitants recorded in 2019, exceeding that of other Maghreb countries, including Algeria, Tunisia, Egypt, Mauritania, and Libya, with rates ranging between 2.5 and 4.5 per 100,000 inhabitants [4]. The northern Moroccan region of Tangier Tetouan Al Hoceima is among the most affected by this phenomenon. In fact, Morocco does not possess a centralized national register of suicide [6] apart from the archives of the regional Medico-legal Units. Attempts and cases of suicide are declared through different media outlets. Therefore, the minister in charge of health and social protection refers in this matter to the figures published by the WHO [6]. Studies shedding light on suicide attempt trends are abundant [7-12]compared to those dedicated to completed suicide cases. The study by Mahir et al. showed that 1130 cases of suicide by self-poisoning were reported between 1981 and 2007 [13], which tragically and enduringly affects the economic, emotional, and social well-being of the bereaved population [14], regardless of their age, religion, ethnicity, gender, income levels, and regions. Despite the complexity of suicide, studies suggest it may be preventable [15, 16]. Thus, this study aims to determine the prevalence of suicide cases in Northern Morocco and investigate the demographic profile, encompassing age, gender, and socioeconomic status of individuals who die by suicide, in an attempt to enhance academic comprehension of suicide epidemiology in the region, and raise awareness of the problem's magnitude.
2. METHODS
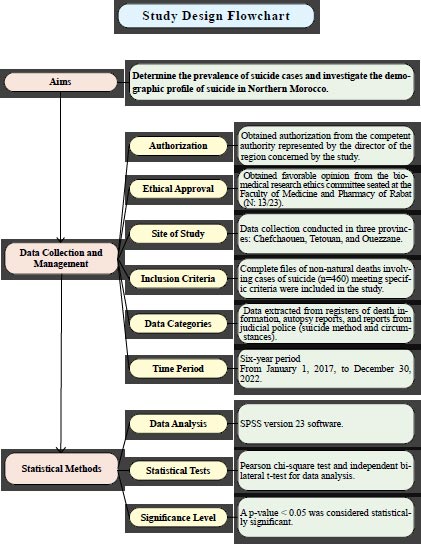
2.1. Aims
This study aims to determine the prevalence of suicide cases and investigate the demographic profile, including age, gender, and socioeconomic status, of individuals who die by suicide. By achieving these objectives, the study intends to contribute to the academic understanding of suicide epidemiology in Northern Morocco. The study also seeks to shed light on the magnitude of the issue and generate knowledge that can inform targeted interventions and strategies to effectively address the growing concern of suicide in the region.
2.2. Data Collection and Management
Data collection was conducted in three provinces: Chefchaouen, Tetouan, and Ouezzane, after obtaining authorization from the competent authority represented by the director of the region concerned by the study and the favorable opinion of the biomedical research ethics committee seated at the Faculty of Medicine and Pharmacy of Rabat (N: 13/23). At the level of the forensic medical units, all files of non-natural deaths that specifically involved cases of suicide were exhaustively consulted (n=480, with 10 files referred to Tangier; 6 referred to Rabat and 4 incomplete files), of which 460 were complete and met the inclusion criteria of the current study: a) a file concerning a completed suicide; b) the suicide occurred in the region of Tangier-Tetouan-El Hoceima; c) the file contained all necessary and useful data for the study.
The extracted data were divided into three categories according to the consulted documentation: registers of information related to deaths (name, age, address, gender, and date of suicide), autopsy reports written by a forensic physician (suicide method), and reports edited by the judicial police (circumstances of suicide). Data collection covered the period from January 1, 2017, until December 30, 2022, approximately six years (Fig. 1).
2.3. Statistical Methods
Data collection was performed using a pre-established, tested, and validated grid encompassing all variables studied in this paper. Data analysis was performed through SPSS version 23 software, using the Pearson chi-square statistical test and the independent bilateral t-test, and a p-value < 0.05 was considered significant.
3. RESULTS
Table 1 demonstrates that individuals under 20 years of age account for 15%, while those aged between 21 and 30 and between 41 and 60 account for a quarter of the sample each. Suicide affects men more than women, with three-quarters (3/4) in our sample being male. and half of the suicide cases were single (56%). The cases that resided in rural areas were the most affected by suicide. Accounting for three quarters (75%). The distribution of suicide cases does not differ significantly across the three provinces where the data was collected. Most people who committed suicide in these provinces had never received any formal education, with a percentage of 84%. Joblessness significantly contributes to the increase in the suicide rate. With over half of the cases (57%) being unemployed. The preferred method of suicide is hanging. Accounting for 93% of the cases (Table 1).
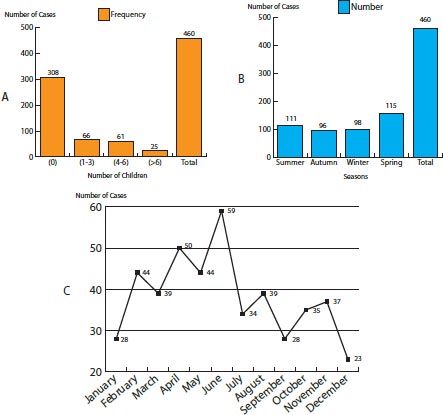
Moreover, with regard to the mental health status of the individuals who committed suicide, only one-third (29%) were receiving psychiatric care at the time of their death. Those with confirmed diagnoses of psychiatric disorders accounted for 42% of the population (Table 1). Fig. (2) explains the distribution of the number of suicide cases according to:
The data is depicted in Fig. (2A) indicates an inverse relationship between the number of suicide cases and the number of children. In other words, the incidence of suicide tends to decrease as the number of children in a family increases. Fig. (2B) shows that the suicide rate is higher during the spring season compared to other seasons. The curve displayed in Fig. (2C) reflects that the cumulative number of suicide cases reached its peak in June.
| Variables | Classes | ||||
|---|---|---|---|---|---|
| Gender | Female | Male | |||
| 130 (28%) | 330 (71.7%) | ||||
| Age (years) | 0 – 20 | 21 – 30 | 31 – 40 | 41 – 60 | > 60 |
| 69 (15%) | 130 (28.2%) | 69 (17.6%) | 124 (27%) | 56 (12.2%) | |
| Family situation | Single | Divorce | Married | Without | |
| 258 (56.1%) | 17 (3.7%) | 172 (37.4%) | 13 (2.8%) | ||
| Environment | Rural | Urban | |||
| 347 (75.4%) | 113 (24.6%) | ||||
| Study level | Illiterate | Primary | Secondary | University | |
| 388 (84.3%) | 24 (5.2%) | 39 (8.5%) | 9 (2%) | ||
| Profession | Farmer | Student | Daily | Without | Other |
| 54 (12%) | 44 (9.6%) | 59 (12.8%) | 262 (57%) | 41 (8.9%) | |
| Province | Chefchaouen | Ouezzane | Tetouan | ||
| 172 (37.4%) | 118 (25.7%) | 170 (37%) | |||
| Method of suicide | Intoxication | Hanging | Other | ||
| 26 (5.7%) | 429 (93.3%) | 5 (1%) | |||
| Psychiatric disorder | No | Yes | |||
| 269 (58.5%) | 191 (41.5%) | ||||
| Follow up | No | Yes | |||
| 327 (71.1%) | 133 (28.9%) | ||||
| - | Environment | Total | p-value | ||
|---|---|---|---|---|---|
| Rural | Urban | ||||
| N(%) | N(%) | ||||
| Marital status | Single | 186 (53.6%) | 72 (63.7%) | 258 | 0.212 |
| Divorced | 12 (3.5%) | 5 (4.4%) | 17 | ||
| Married | 138 (39.8%) | 34 (30.1%) | 172 | ||
| Widowed | 11 (3.2%) | 2 (1.8%) | 13 | ||
| Gender | Feminine | 107 (30.8%) | 22 (19.5%) | 129 | 0.019 |
| Masculine | 240 (69.2%) | 91 (8.5%) | 331 | ||
| Follow-up | No | 258 (74.4%) | 69 (61.1%) | 327 | 0.007 |
| Yes | 89 (25.6%) | 44 (38.9%) | 133 | ||
| Psychiatric disorder | No | 216 (62.2%) | 53 (46.9%) | 269 | 0.004 |
| Yes | 131 (37.8%) | 60 (53.1%) | 191 | ||
| Provinces | Chefchaouen | 166 (47.8%) | 6 (5.3%) | 172 | 0 |
| Ouezzane | 105 (30.3%) | 13 (11.5%) | 118 | ||
| Tetouan | 76 (21.9%) | 94 (83.2%) | 170 | ||
| Number of children | 1 (0) | 225 (65.0%) | 82 (72.6%) | 307 | 0.132 |
| 2 (1-3) | 48 (13.9%) | 18 (15.9%) | 66 | ||
| 3 (4-6) | 53 (15.3%) | 8 (7.1%) | 61 | ||
| 4 (>=7) | 20 (5.8%) | 5 (4.4%) | 25 | ||
| Age (years) | 0-20 | 62 (17.9%) | 7 (6.2%) | 69 | 0.043 |
| 21-30 | 95 (27.4%) | 35 (31.0%) | 130 | ||
| 31-40 | 57 (16.4%) | 24 (21.2%) | 81 | ||
| 41-60 | 90 (25.9%) | 34 (30.1%) | 124 | ||
| >60 | 43 (12.4%) | 13 (11.5%) | 56 | ||
| Occupation | Farmer | 54 (15.6%) | 0 (0%) | 54 | 0 |
| Without | 193 (55.6%) | 69 (61.1%) | 262 | ||
| Student | 41 (11.8%) | 3 (2.7%) | 44 | ||
| Other | 18 (5.2%) | 23 (20.4%) | 41 | ||
| Method of suicide | Hanging | 324 (93.4%) | 105 (92.9%) | 429 | 0.98 |
| Intoxication | 17 (4.9%) | 6 (5.3%) | 23 | ||
| Other | 6 (1.7%) | 2 (1.8%) | 8 | ||
| - | Gender | Total | p-value | ||
|---|---|---|---|---|---|
|
Feminine N (%) |
Masculine N (%) |
||||
| Marital status | Single | 64 (49.6%) | 194 (58.6%) | 258 | 0.00003 |
| Divorced | 3 (2.3%) | 14 (4.2%) | 17 | ||
| Married | 51 (39.5%) | 121 (36.6%) | 172 | ||
| Widowed | 11 (8.5%) | 2 (0.6%) | 13 | ||
| Study level | Illiterate | 105 (81.4%) | 283 (85.5%) | 388 | 0.442 |
| Primary | 6 (4.7%) | 18 (5.4%) | 24 | ||
| Secondary | 14 (10.9%) | 25 (7.6%) | 39 | ||
| University | 4 (3.1%) | 5 (1.5%) | 9 | ||
| Environment | Rural | 107 (82.9%) | 240 (72.5%) | 347 | 0.0194 |
| Urban | 22 (17.1%) | 91 (27.5%) | 113 | ||
| Psychiatric disorder detected | No | 88 (68.2%) | 181 (54.7%) | 269 | 0.0081 |
| Yes | 41 (31.8%) | 150 (45.3%) | 191 | ||
| Age | 0-20 | 32 (24.8%) | 37 (11.2%) | 69 | 0.0069 |
| 21-30 | 30 (23.3%) | 100 (30.2%) | 130 | ||
| 31-40 | 19 (14.7%) | 62 (18.7%) | 81 | ||
| 41-60 | 33 (25.6%) | 91 (27.5%) | 124 | ||
| >60 | 15 (11.6%) | 41 (12.4%) | 56 | ||
| Province | Chefchaouen | 57 (44.2%) | 115 (34.7%) | 172 | 0.023 |
| Ouezzane | 37 (28.7%) | 81 (24.5%) | 118 | ||
| Tetouan | 35 (27.1%) | 135 (40.8%) | 170 | ||
| Number of children | 1 (0) | 78 (60.5%) | 229 (69.4%) | 307 | 0.047 |
| 2 (1-3) | 25 (19.4%) | 41 (12.4%) | 66 | ||
| 3 (4-6) | 22 (17.1%) | 39 (11.8%) | 61 | ||
| 4 (>7) | 4 (3.1%) | 21 (6.4%) | 25 | ||
| Follow-up | No | 98 (76.0%) | 229 (69.2%) | 327 | 0.149 |
| Yes | 31 (24.0%) | 102 (30.8%) | 133 | ||
| Number of yearly cases | 2017 | 24 (18.6%) | 54 (16.3%) | 78 | 0.503 |
| 2018 | 25 (19.4%) | 49 (14.8%) | 74 | ||
| 2019 | 24 (18.6%) | 50 (15.1%) | 74 | ||
| 2020 | 18 (14.0%) | 65 (19.6%) | 83 | ||
| 2021 | 23 (17.8%) | 60 (18.1%) | 83 | ||
| 2022 | 15 (11.6%) | 52 (15.7%) | 67 | ||
In this study, we investigated the effect of the residential environment of individuals who died by suicide on other studied variables. Significant associations were found between the residential environment and gender (p=0.01), age (p=0.04), province (p=0.00), presence of psychiatric disorder (p=0.004), psychiatric follow-up (p=0.007), and employment status (p=0.00). However, marital status, number of children, and method of suicide were not found to relate to the residential environment of those who died by suicide (Table 2).
Based on the results presented in Table 3, it appears that gender may be significantly associated with the marital status of individuals who have committed suicide (p=0.00), as well as their place of residence and province (p<0.05), age (p=0.006), and the presence of diagnosed psychiatric disorders (p=0.008). However, no significant associations were found between gender, level of education, and psychiatric follow-up (p>0.05).
In this study, we examined the impact of the presence of psychiatric disorders among individuals who died by suicide on the studied variables. Significant associations were found between age (p=0.00), gender (p=0.009), province (p=0.00), level of education (p=0.001), rural environment (p=0.004), and occupation (p=0.00). However, no significant relationships were found between the presence of psychiatric disorders and marital status, number of children or method of suicide (Table 4).
| - | - | Psychiatric Disorder | |||
|---|---|---|---|---|---|
| - | Variables | Yes | No | Total | p-value |
| Gender | Feminine | 41 (8.9%) | 88 (19.1%) | 129 (28.0%) | 0.09 |
| masculine | 150 (32.6%) | 181 (39.3%) | 331 (72.0%) | ||
| Marital status | Single | 109 (23.7%) | 149 (32.4%) | 258 (56.1%) | 0.445 |
| Divorced | 10 (2.2%) | 7 (1.5%) | 17 (3.7%) | ||
| Married | 67 (14.6%) | 105 (22.8%) | 172 (37.4%) | ||
| Widowed | 5 (1.1%) | 8 (1.7%) | 13 (2.8%) | ||
| Province | Chefchaouen | 47 (10.2%) | 125 (27.2%) | 172 (37.4%) | 0 |
| Ouezzane | 67 (14.6%) | 51 (11.1%) | 118 (25.7%) | ||
| Tetouan | 77 (16.7%) | 93 (20.2%) | 170 (37.0%) | ||
| Number of children | 0 | 133 (29.0%) | 174 (37.9%) | 307 (66.9%) | 0.511 |
| 1-3 | 24 (5.2%) | 42 (9.2%) | 66 (14.4%) | ||
| 4-6 | 22 (4.8%) | 39 (8.5%) | 61 (13.3%) | ||
| ≥7 | 12 (2.6%) | 13 (2.8%) | 25 (5.4%) | ||
| Age (years) | 0-20 | 9 (2.0%) | 60 (13.0%) | 69 (15.0%) | 0 |
| 21-30 | 65 (14.1%) | 65 (14.1%) | 130 (28.3%) | ||
| 31-40 | 35 (7.6%) | 46 (10.0%) | 81 (17.6%) | ||
| 41-60 | 54 (11.7%) | 70 (15.2%) | 124 (27.0%) | ||
| >60 | 28 (6.1%) | 28 (6.1%) | 56 (12.2%) | ||
| Occupation | Farmer | 20 (4.3%) | 34 (7.4%) | 54 (11.7%) | 0 |
| Student | 3 (0.7%) | 41 (8.9%) | 44 (9.6%) | ||
| Worker | 30 (6.5%) | 29 (6.3%) | 59 (12.8%) | ||
| Without | 123 (26.7%) | 139 (30.2%) | 262 (57.0%) | ||
| Other | 15 (3.3%) | 26 (5.7%) | 41 (8.9%) | ||
| Method of suicide | Intoxication | 5 (1.1%) | 18 (3.9%) | 23 (5.0%) | 0.073 |
| Hanging | 181 (39.3%) | 248 (53.9%) | 429 (93.3%) | ||
| Other | 5 (1.1%) | 3 (0.7%) | 8 (1.7%) | ||
| Environment | Rural | 131 (28.5%) | 216 (47.0%) | 347 (75.4%) | 0.004 |
| Urban | 60 (13.0%) | 53 (11.5%) | 113 (24.6%) | ||
| Season | Autumn | 39 (8.5%) | 57 (12.4%) | 96 (20.9%) | 0.474 |
| Summer | 43 (9.3%) | 68 (14.8) | 111 (24.1%) | ||
| Winter | 37 (8.0%) | 61 (13.3%) | 98 (21.3%) | ||
| Spring | 72 (15.7%) | 83 (18.0%) | 155 (33.7%) | ||
| Study level | Illiterate | 175 (38.0%) | 213 (46.3%) | 388 (84.3%) | 0.001 |
| Primary | 7 (1.5%) | 17 (3.7%) | 24 (5.2%) | ||
| Secondary | 5 (1.1%) | 34 (7.4%) | 39 (8.5%) | ||
| University | 4 (0.9%) | 5 (1.1%) | 9 (2.0%) | ||
| - | Variables | Follow-up | - | - | |
| - | Yes | No | Total | p-value | |
| Gender | Feminine | 31 (6.7%) | 98 (21.3%) | 129 (28.0%) | 0.149 |
| Masculine | 102 (22.2%) | 229 (49.8%) | 331 (72.0%) | ||
| Marital status | Single | 76 (16.5%) | 182 (39.6%) | 258 (56.1%) | 0.719 |
| Divorced | 6 (1.3%) | 11 (2.4%) | 17 (3.7%) | ||
| Married | 46 (10.0%) | 126 (27.4%) | 172 (37.4%) | ||
| Widowed | 5 (1.1%) | 8 (1.7%) | 13 (2.8%) | ||
| Province | Chefchaouen | 37 (8.0%) | 135 (29.3%) | 172 (37.4%) | 0.023 |
| Ouezzane | 41 (8.9%) | 77 (16.7%) | 118 (25.7%) | ||
| Tetouan | 55 (12.0%) | 115 (25.0%) | 170 (37.0%) | ||
| Number of children | 0 | 90 (19.6%) | 217 (47.3%) | 307 (66.9%) | 0.950 |
| 1-3 | 19 (4.1%) | 47 (10.2%) | 66 (14.4%) | ||
| 4-6 | 16 (3.5%) | 45 (9.8%) | 61 (13.3%) | ||
| >=7 | 8 (1.7%) | 17 (3.7%) | 25 (5.4%) | ||
| Age (years) | 0-20 | 4 (0.9%) | 65 (14.1%) | 69 (15.0%) | 0.000 |
| 21-30 | 43 (9.3%) | 87 (18.9%) | 130 (28.3%) | ||
| 31-40 | 29 (6.3%) | 52 (11.3%) | 81 (17.6%) | ||
| 41-60 | 41 (8.9%) | 83 (18.0%) | 124 (27.0%) | ||
| >60 | 16 (3.5%) | 40 (8.7%) | 56 (12.2%) | ||
| Occupation | Farmer | 10 (2.2%) | 44 (9.6%) | 54 (11.7%) | 0.000 |
| Other | 11 (2.4%) | 30 (6.5%) | 41 (8.9%) | ||
| Student | 2 (0.4%) | 42 (9.1%) | 44 (9.6%) | ||
| Worker | 15 (3.3%) | 44 (9.6%) | 59 (12.8%) | ||
| Without | 95 (20.7%) | 167 (36.3%) | 262 (57.0%) | ||
| Method of suicide | Other | 4 (0.9%) | 4 (0.9%) | 8 (1.7%) | 0.101 |
| Intoxication | 3 (0.7%) | 20 (4.3%) | 23 (5.0%) | ||
| Hanging | 126 (27.4%) | 303 (65.9%) | 429 (93.3%) | ||
| Environment | Rural | 89 (19.3%) | 258 (56.1%) | 347 (75.4%) | 0.007 |
| Urban | 44 (9.6%) | 69 (15.0%) | 113 (24.6%) | ||
| Seasons | Autumn | 33 (7.2%) | 63 (13.7%) | 96 (20.9%) | 0.085 |
| Summer | 25 (5.4%) | 86 (18.7%) | 111 (24.1%) | ||
| Winter | 23 (5.0%) | 75 (16.3%) | 98 (21.3%) | ||
| Spring | 52 (11.3%) | 103 (22.4%) | 155 (33.7%) | ||
| Study level | Illiterate | 123 (26.7%) | 265 (57.6%) | 388 (84.3%) | 0.010 |
| Primary | 3 (0.7%) | 21 (4.6%) | 24 (5.2%) | ||
| Secondary | 4 (0.9%) | 35 (7.6%) | 39 (8.5%) | ||
| University | 3 (0.7%) | 6 (1.3%) | 9 (2.0%) | ||
The results presented in Table 5 show that psychiatric follow-up may be significantly related to the occupation of individuals who have committed suicide (p=0.00), as well as to the region and province of their residence (p<0.05), their age (p=0.00), and study level (p=0.01). However, no significant association was found between gender, marital status, and method of suicide.
4. DISCUSSION
Globally, suicide affects all age groups, with nearly 75% of suicides occurring in third-world countries or developing countries. The rates of suicide are higher among individuals aged 70 years or older; however, some countries reported that youngsters are more affected [17].
Improved identification of risk factors and protective measures is essential to prevent suicide and suicidal behavior [18].
Thus, the issue of suicide attracts the attention of both government authorities, non-governmental organizations, and the public due to its severity and magnitude on individuals and society, consequently, a significant influence on sustainable development, which one of its objectives is to quickly reduce the global suicide rate [19].
Furthermore, several studies have attempted to describe the epidemiological profile and determine the factors involved in suicide attempts [7-12], but few have invested in understanding suicide itself [13].
Therefore, suicide, which cannot be exclusively attributed to mental health problems, is undoubtedly influenced by a series of biological, psychological, and social factors [20]. The results of this study show that the age group between 21-30 and the age group between 41-60 represent each quarter (28%; 27% respectively), and that the suicide rate in the age group up to 40 years is 61% which remains high. This is consistent with the results of Barrimi et al. who found a percentage of 75% for the same age group [21]. In their study, Na et al. refuted the hypothesis that older individuals develop attitudes towards suicide. Our sample supports this finding, revealing a rate of only 12% among suicide victims over 60 years old [22].
Regarding gender, suicide affects men (75%) more than women (25%), which is consistent with the findings of the 5th report of the National Suicide Observatory where the number of suicides is higher among men (n=6.278) than among women (n=2.088) with a ratio of 3/1. The age-adjusted death rate is 3.5 times higher among men, which promotes the idea that age differences between these two subpopulations do not explain this gap between the two genders [23]. Similarly, according to Freeman, this behavior tends to lean towards the male side in the European Union [11]. Another Ecuadorian study calculated standardized global suicide rates by age from 2001 to 2014 for all age groups and found that it was 7.1 per 100,000 and that men were three times more likely to die by suicide than women, an idea supported by several studies [15, 24-27].
In relation to the marital status of the cases studied in this research, 56% were single and 37% were married. A study found that most suicide deaths were single (64.2%), followed by married (18.6%) and divorced individuals (14.2%) [28]. Our results are almost identical to those published in the study conducted by Agoub et al. (2006) on 400 men and 400 women, where they found that singles accounted for 58% of the population, while 35.3% of them were married [29], as well as those of Ortiz-Prado, Besnier et al. [16, 18].
Furthermore, three-quarters of the suicides (75%) reported in this study resided in rural areas. This evidence contradicts the findings of Troya et al. who found higher suicide rates in urban regions, for both men and women [30]. However, according to Li and Cao, these rates have been increasing in rural areas, particularly where there is a low level of education in China, before 2000 [31]. Additionally, Hu found a rate of 23.6% in the same regions among elderly individuals living alone [32]. Our results suggest that suicide is a behavior that remains predominantly rural in the Moroccan context.
Similarly, we investigated the possible effect of rural dwelling and its association with other factors. In fact, a significant association was found with gender, age, province, presence of psychiatric disorders, psychiatric follow-up, and employment status. The latter contributed significantly and predominantly (57%) to the increase in suicide cases in our study. This unemployment rate exceeds twice the rate calculated in a previous study conducted in a Moroccan metropolitan area (24.1%) [29, 32]. In another study conducted at Hassan II University Hospital Center in Fez, 65% of patients were unemployed [21]. Additionally, a 2.5% increase in suicide mortality rate is observed for every 10% increase in the unemployment rate [33-36]. The forestry and agricultural sectors are also associated with an increased risk of suicide mortality in men [37].
It is evident from our results that illiteracy is an undeniable determinant in the use of suicidal behaviors (84%). Attachment to school protects against suicidal thoughts and attempts, but prevention efforts in schools appear to have no manifest effect on suicide rates [38]. In the same vein, men, and those with a low level of education are more susceptible to suicide [30, 39].
Also, among the entire study population (n=460), only 42% were diagnosed with a psychiatric disorder, and two-thirds (71%) of suicide cases did not receive any psychiatric support. Current evidence shows that mental illnesses, such as depression, constitute a significant risk factor for suicide. A study asserted that over 80% of individuals who died by suicide suffered from a mental illness or psychiatric disorder, with more than 90% of young people experiencing addiction-related disorders [38]. In another study conducted in South Korea, authors estimated that 87% of suicidal individuals had a mental health problem prior to their death, but only 15.2% received treatment or counseling [14]. Suicide is frequently used as an indicator of a population’s mental health [20]. Similarly, studies support that suicide rates are closely linked to the presence of mental disorders, regardless of their nature, with a significant percentage related to substance use problems, personality, affective and depressive disorders. and especially geographical factors [32, 40-43].
Additionally, our results indicate that hanging is the most common suicide method (93%). This corroborates with other studies on the same topic [16, 24, 30], but different from other contexts where jumping from height remains the most common method [44].
During the analysis of the results of the present study, we were struck by the fact that the number of suicide cases increases during spring, particularly in June, and that there is a correlation between the increase in the number of children and the reduction in the suicide rate. Conversely, in another study conducted by Soumah et al, it is noteworthy that the frequency of suicide cases focuses on peri-urban areas where suicides are committed during the cold season, particularly during the first three months of each year [24].This goes in line with the study carried out by Zakharof et al. [45].
However, the current study has some limitations: First, the availability of data from only the forensic unit service in three provinces. It may not represent the broader population or consider cases that did not come under forensic investigation. Second, other variables such as the socio-economic situation, need to be explored to better describe the epidemiology of suicide in the studied provinces. Third, the lack of financial support to conduct an exploratory epidemiological investigation among the families of suicide victims was also a hurdle. Fourth, due to the transfer of some suicide cases from the northern region to Rabat for further judicial investigation, some case records were not explored. Fifth, the unavailability of a psychological autopsy limits a deeper understanding of the underlying psychological factors behind suicide. Lastly, there is likely an underestimation of suicidal behavior due to the taboo still surrounding it in many cultures, including Morocco. It is quite common for some suicides to be classified as domestic accidents or other types of mishaps.
CONCLUSION
This study represents a pioneering effort in the investigation of suicide in the northern region of Morocco and potentially the entire country. It sheds light on the prevalence and demographic profile characterization of individuals dying by suicide, encompassing a wide array of variables. Our findings indicate that the incidence of suicide is primarily concentrated among young and adult males who are unmarried, living in rural areas, lacking education, employment, and medical care, with hanging being the most common method employed. Nonetheless, our results also suggest that marriage and parenthood may have a mitigating effect on suicidal behaviors.
Although Morocco has a high rate of suicide cases, no official interventions have been undertaken yet. Recently, Morocco intends to adopt a national suicide prevention strategy for the 2023-2030 period, but details are still undisclosed. Indeed, the results of the current study may provide useful insights for future interventions.
Further multidimensional investigations, incorporating additional variables and larger sample sizes, are highly warranted.
AUTHORS’ CONTRIBUTIONS
All authors contributed significantly to the conception, study design, execution, acquisition of data, analysis, and interpretation of this work or in all these areas. AE and HK contributed to conceptualization. AE contributed to data collection. AE and HG contributed to data analysis and drafted the initial manuscript. ME. YE and HK contributed to the revision of the manuscript. HK supervised the study. All authors edited and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| LMICs | = Low- and middle-income countries |
| SPSS | = Statistical Package for the Social Sciences |
| WHO | = World Health Organization |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was conducted in accordance with ethical principles and regulatory requirements. Prior to data collection, appropriate ethical clearance was obtained, including authorization from the relevant officials in the study regional directory of health (authorization number 2920/21) and a favourable opinion from the ethics committee for biomedical research at the Faculty of Medicine and Pharmacy, Mohammed V University of Rabat (approval number N: 13/23).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committees and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Consent for publication was obtained from all participants’ next of kin, and identities have been protected in accordance with ethical guidelines.
AVAILABILITY OF DATA AND MATERIALS
The data collection procedure was initiated by the authors themselves who, in the medical forensic unit, classified death cases and focused on suicide deaths. Data and materials used in this study are available upon request from the corresponding author. The dataset analyzed during the current study is not publicly available due to privacy and ethical restrictions, but de-identified data may be made available from the corresponding author upon reasonable request and with appropriate institutional approvals.
ACKNOWLEDGEMENTS
We are grateful to the regional director and the provincial health delegates of the Tetouan Tangier El Hoceima region for their collaboration. Also, we are grateful to all health professionals working in the service of forensic units located in the three provinces for their help in the data collection.

