All published articles of this journal are available on ScienceDirect.

Child Survival Status and its Drivers in Kenya and Other Three East-African Countries: A Literature Review
Abstract
Child mortality continues to be a significant public health concern, particularly in the East African region. Understanding the factors associated with child mortality is crucial for developing effective interventions. This literature review aims to explore the relationship between various factors such as breastfeeding, sex of a child, type of place of residence, education level, and family size influencing child mortality in Africa, particularly the East African region. This article also assesses the level and trends of child mortality in East African Countries. Search engines such as PubMed, Google Scholar, and relevant institutional repositories were utilised to harvest literature between 2000 and 2021. The study adopts a conceptual framework by Mosley and Chen and focuses on factors viewed as an important driver of child survival beyond the fifth birthday amongst the four countries. The study sees the need to look at the difference in child mortality in the countries and look at the combined estimates, which have been limited in studies of factors associated with under-five mortality through frequentist meta-analysis, Bayesian meta-analysis and space and time regarding child mortality. In doing so, this allows better improvement of existing and implementing policies related to reducing child mortality in regards to child improving child survival and further identifies regions with less progress in achieving Sustainable Development Goals by 2030 by policymakers, governments, and relevant parties involved in developing policies focusing on improving under-five child survival.
1. INTRODUCTION
Under-five mortality refers to the number of deaths occurring in children under the age of five per 1,000 live births. It is a key indicator of child health and well-being and reflects the overall health system, socio-economic conditions, and access to healthcare services in a country or region [1]. Globally, there has been significant progress in reducing under-five mortality over the past few decades. According to the United Nations Inter-agency Group for Child Mortality Estimation (UN IGME), the global under-five mortality rate declined from an estimated 93 deaths per 1,000 live births in 1990 to 39 deaths per 1,000 live births in 2019 [1, 2]. However, it is important to note that there are regional disparities, and progress varies across countries and regions [2]. The issue of the under-five mortality rate has remained a cause of concern over the past decades, but figures that remain high can be reduced through the implementation of public policies and remain the common issue on the agenda for the United Nations (UN) [1].
In the East African region, under-five mortality rates have also shown a decline, although the pace of progress may differ between countries [1, 2]. Factors such as healthcare infrastructure, access to services, economic conditions, and social determinants of health contribute to these variations. For example, countries like Rwanda, Tanzania, and Ethiopia have significantly reduced child mortality rates through various interventions, including improved access to healthcare, immunisation programs, nutrition interventions, and community-based initiatives.
Globally, the under-five mortality rate has remained a cause of concern over the past decades, but figures that remain high can be reduced through the implementation of public policies and remain the common issue on the agenda for the United Nations (UN) [2, 3]. Based on the United Nations Inter-agency Group for Child Mortality Estimation (UN IGME) mentioned above, the global child survival rate has significantly improved over the past few decades. Despite such remarkable progress, under-five child mortality remains a concern, particularly in the sub-Saharan African region. If such trends continue, approximately nineteen countries are likely to miss the Sustainable Development Goal to end preventable deaths of newborns and children under five years in Eastern and Southern Africa [3, 4]. Disparities in countries exist in infant mortality that may be due to the difference in registration for premature infants [5]. The leading preventable causes of child deaths include pneumonia, birth complications, diarrhoea and malaria [4, 6].
The tracking of global under-five mortality is part of international development that started in 1990 at the World Summit to reduce preventable under-five deaths by a third between 1990 and 2000 [7, 8]. A proposed two-third reduction in under-five child deaths was adopted by 193 countries at the United Nations (UN) in 2000 as part of the eight Millennium Development Goals (MDGs) at the Millennium Summit [9]. In 2015, Sustainable Development Goals were adopted by the UN and its agencies and funds, which reflected further strengthening of the development agenda [10]. Currently, as part of the Sustainable Development Goals, goal 3,2 aims to end preventable under-five child deaths and reduce the under-five mortality rate to at least 25 per 1,000 live births by 2030 [10, 11]. It has been reported that a 53% reduction has been achieved globally between 1990 to 2015 [12]. However, the sub-Saharan African region has been the slowest in under-five mortality reduction, with 37 out of 48 countries failing to meet the MDG target in 2015 [12]. Tanzania, Kenya, and Uganda are part of the 37 countries that could not achieve the SDG 4 target and are classified as low-income group countries, including Rwanda [13, 14]. Failure to meet the target may result from low-income earnings, weak institutions, poor governance and lack of infrastructure. Many well-documented studies use Demographic and Health Survey Data, such as providing a snapshot at a given time, which sometimes leads to misleading inferences. In addition, some well-documented studies used panel data on under-five mortality, providing limited insight into socio-economic, environmental and social change processes.
The main aim of this paper is to assess trends and review some of the risk factors associated with under-five mortality in Kenya and three other East-African countries, namely Rwanda, Uganda and Kenya, using panel data obtained from the World Bank database in website World Bank: https://data.worldbank.org/
2. METHODOLOGY
The study uses the definition of child mortality in assessing the causes and consequences of child death before the fifth year birthday. To achieve the aim of the study, we consider the mortality of children before their fifth birthday. Therefore, we consider the period for the study to be 2000 - 2021 as a comparative.
2.1. Data Source
For reviewing purposes, the searches are done to obtain journal articles in Google Scholar, ScienceDirect, and ResearchGate. We included the name East Africa to retrieve information on countries of interest. Panel data were also retrieved from the World Bank database to study the trends in each of the four countries. In addition, the infant and under-five mortality estimates were extracted from the UNICEF data portal to assess the level and trends in child mortality in 2019 for countries in the East African region, Kenya, Rwanda, Tanzania and Uganda.
2.2. Search Strategy and Inclusion Criteria
A comprehensive search of electronic databases, including PubMed, Google Scholar, and relevant institutional repositories, was conducted. The keywords used for the search included “child mortality,” “breastfeeding,” “sex of a child,” “residence,” “education level,” “family size,” and “East Africa.” Studies published between 2000 and 2021 were included. Only English-language articles were considered. The search yielded a total of 70 articles, of which 22 were included in this review based on their relevance and quality.
3. RESULTS
3.1. Level and Trends of Under-mortality
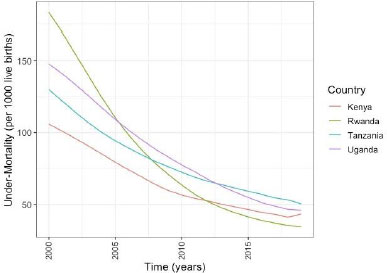
At the national level, the goal set out for Kenya at the World Summit for Children was not achieved by 2000. The country only managed to reduce under-five mortality to 102 per 1000 live births instead of the set target of 70 per 1000 live births. Additionally, a 66.67% reduction target set out as part of MDG 4 was also not achieved nationally [15]. The under-five mortality rate in Kenya has since fallen to 43 deaths per 1,000 live births in 2019. However, every day, 64500 children still die before age five, mostly from preventable causes. Fig. (1) shows the trends of the under-five of the four countries. Rwanda has managed to reduce under-five mortality faster than the other three countries. Kenya's under-five mortality has been declined but slower Fig. (1) compared to the other three countries.
3.2. Risk factors of under-five mortality
The current paper adopts the conceptual framework by Mosley and Chen [16], which focuses on the sex of a child, education level, family size, economic well-being, place of residence, breastfeeding status, and lack of facility. These are some of the risk factors for childhood mortality that have been widely documented in the literature [17, 18].
3.3. Sex of a Child
The sex of a child is one of the important drivers of infant and under-five mortality. Male children have an increased risk of dying before their fifth birthday [2, 19, 20]. Studies have been conducted and well documented in the literature [2, 15, 18]. Gender disparities in child mortality were evident in the East African region [15, 17, 18]. In many countries, male children had higher mortality rates compared to females. The reasons behind this disparity varied, including biological factors, gender-based discrimination, and differences in healthcare-seeking behaviours.
3.4. Mother's Education Level
Maternal education plays a crucial role in child survival. The maternal education level of a mother has a direct relationship with child health, and this has been shown over the past three decades [19]. Studies consistently demonstrated a positive association between higher levels of maternal education and lower child mortality rates [2, 18, 19]. For example, the study by Le and Nguyen [19] found a positive relationship between a mother's education and the child's health. Such favourable effects may be attributed to fertility behaviour, better usage of healthcare facilities or better health knowledge, and labour market outcomes [19]. Hence, maternal education is important in improving economics and the conditions of developing regions. This has been shown by the study by Chen and Li [20] that a mother's education is an important factor even after controlling the number of siblings, income and other socio-economic variables. In addition, Bbaale and Buyinza [21] confirm the need to educate women in developing countries. Educated mothers were more likely to adopt healthy practices, seek appropriate healthcare, and have access to information about child health.
3.5. Family Size
Family size has been seen as one of the contributors to childhood mortality and has been documented in the literature in the past three decades. However, a study by Åslund and Grönqvist [22] found no evidence of a long term of family size on child health. However, a small negative effect of family impact on the compulsory and secondary school may be due to vulnerability to restriction of parental investments [22]. However, one may expect a larger family size to be associated with increased child mortality rates. This relationship may be attributed to resource constraints, decreased caregiver attention, and increased risk of infectious diseases within crowded households [2, 5, 18, 19].
3.6. Breastfeeding Status
Several studies highlighted the protective effect of breastfeeding on child mortality [2 , 15, 19]. A mother's education level is regarded as a factor that influences breastfeeding from birth, and the impact increases with age, at least up to six months, according to public health recommendations. However, this has been influenced by the age of the mother and her level of education [23]. Exclusive breastfeeding for the first six months of life was associated with a lower risk of mortality among infants. Timely initiation of breastfeeding and continued breastfeeding were also linked to reduced child mortality rates. Breastfeeding is a public health strategy for reducing under-five mortality, improving maternal morbidity, and controlling health care. Breastfeeding has a relationship with reduced risk of obesity, respiratory illness, ovarian cancer and hypertension. Exclusive breastfeeding is regarded as a source of food and nutrition that provides health protection for the first six months of life [24]. Breastfeeding is one important determinant of childhood mortality. However, disparities still exist mainly due to socio-economic status, country of origin and geographic location [24]. Child undernutrition remains a concern in sub-Saharan African regions and contributes to under-five child deaths [25]. Undernutrition has short-term and long-term effects on a child's well-being; this brings illness and influences the development of a child as a result of Environmental conditions, socio-economic circumstances and breastfeeding duration or status, which limit and set physical growth of children [25]. Undernutrition may be more common in children with diarrhoea, a product of multiple births and children born small in size.
3.7. Household Economic Well-being Group
Household economic well-being is another contributor to the children's survival before their fifth birthday. Poor household results in childhood stunting, wasting and underweight children in SSA [25]. A child from a socioeconomically disadvantaged household lacks access to modern medicine and reproductive norms that favour early and more rapid childbearing [26, 27]. Studies have shown poor household is associated with childhood mortality. Economic conditions may significantly impact a family's ability to provide adequate healthcare, nutrition, and living conditions for their children. Other factors, such as access to healthcare infrastructure, quality of healthcare services, maternal education, and cultural practices, also interact with household economic well-being to determine child health outcomes. Addressing economic disparities and improving household economic well-being is a crucial step toward reducing child mortality rates.
3.8. Place of Residence
There have been disparities in childhood mortality between urban and rural areas in developing countries, which could be mainly due to better health facilities and living conditions well documented [26]. A study by Fox and Heaton [27] found that child from rural areas has a high risk of nutrition mainly due to socio-economic disparities between urban and rural areas and the lack of access to medical care facilities. Studies conducted in developing countries have mainly associated child mortality with children from rural areas. Rural areas often experience higher child mortality rates compared to urban areas [26, 27]. Limited access to healthcare facilities, inadequate sanitation, and poverty were identified as key factors contributing to higher child mortality rates in rural regions.
4. DISCUSSION
The main objective of this study was to highlight several factors associated with child mortality in the East African region and assess levels and trends for the period 2000 to 2019 trends and possible risk factors associated with under-five mortality in four East African countries (Kenya, Rwanda, Uganda and Kenya). The higher mortality that was observed in Rwanda in 1994 was the consequence of genocides which claimed millions of lives [28]. Since then, Rwanda has made great progress in reducing child mortality due to the central government; the country has been expanding access to basic health and strengthening the health system, including social support [29]. Progress in the reduction of under-five mortality has been observed in Kenya, Uganda and Tanzania. However, under-five mortality remains an issue of concern in the SSA region as opposed to other regions.
Several studies have been conducted and have shown that child sex is associated with under-five mortality. A study by Alotaibi et al. [30] has shown high hazard rates for male compared to female children. However, a similar study reported lower hazard rates in males compared to females in Niger. In addition, studies by Ayiko [31], Ettarh and Kimani [32] and Nasejje et al. [33] pointed out that the sex of a child (female) reduces the risk of experiencing child mortality before the fifth birthday.
The study also highlighted the importance of breastfeeding and the mother's level of education to the survival of children before their fifth birthday, which is well documented in studies by Ayiko [31], Ettarh and Kimani [18, 31] and Nasejje et al. [32]. They point out that child children from an educated mother have a higher chance of survival beyond their fifth birthday. However, public health encourages breastfeeding from birth to at least six months [26]. This may influence mothers who are mostly at work for most of the day, which affects the time mothers spend breastfeeding too long hours of work, particularly those who are the household head. Ayiko et al. [31] and Ssengonzi [33] further pointed out the importance of the type of place of residence and the mother's education level as an important contributor to under-five child survival in Uganda. This was also pointed out by the study by Susuman and Hamisi [34] conducted in Tanzania. These studies have ignored survey design during the analysis, which may result in misleading statistical inferences. The study sees the need to consider both cross-sectional and panel data in studying factors associated with child mortality with the application of beta regression, additive model, analysis of variance, extended Cox regression, Meta-Analysis and Survey Bayesian Meta-Analysis.
CONCLUSION AND RECOMMENDATION
This literature review highlights several factors associated with child mortality in the East African region. Breastfeeding, sex of a child, type of place of residence, education level, and family size were identified as significant determinants of child mortality. The study further assessed levels and trends of under-five mortality in four East African countries. The study shows a reduction that has been observed in the reduction of under-five mortality. Notably, Rwanda has been in the right direction of further achieving Sustainable Development Goal 3.2 by 2030, having experienced more child deaths during the 1990 decades and surpassing the other three countries in terms of improving child survival in recent decades. Understanding these several factors can inform policymakers and healthcare professionals in developing targeted interventions to reduce child mortality rates in the region.
The study recommends promoting breastfeeding practices, addressing gender disparities, improving access to healthcare in rural areas, enhancing maternal education, and implementing family planning initiatives are essential steps towards improving child survival in East Africa. Further research and comprehensive strategies are warranted to tackle this critical public health issue effectively. This will play a crucial role in achieving Sustainable Development Goal 3.2 by 2030, following Millenium Development Goal 4 in the past decades. The recent non-observed variable involves the recent COVID-19 pandemic with its variants.
AUTHOR'S CONTRIBUTIONS
WJD conceptualised and analysed the literature. All others were involved in the drafting process and helped in comparison and analysis. All authors read and approved the final manuscript.
LIST OF ABBREVIATIONS
| UN IGME | = United Nations Inter-agency Group for Child Mortality Estimation |
| UN | = United Nations |
| MDGs | = Millennium Development Goals |
CONSENT FOR PUBLICATION
Not applicable.
FUNDING
No funding associated with this research.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise..
ACKNOWLEDGEMENTS
The authors acknowledge the University of Zululand and the University of KwaZulu-Natal Department of Mathematical Science, the School of Mathematics, Statistics and Computer Science for the support to conduct this research work, the authors on the literature and UNICEF for the data to study the levels and trends.

