All published articles of this journal are available on ScienceDirect.

Knowledge of and Attitudes Toward Work-Related Musculoskeletal Injuries in Firefighters in Cape Town, South Africa – A Cross-sectional Study
Authors Info & Affiliations
Abstract
Background
Firefighters encounter dangerous conditions in their work environment that place them at risk of severe injury. Musculoskeletal injuries (MSIs) are one of the primary injuries sustained by firefighters, which may be due to the firefighters’ lack of knowledge and poor attitudes toward MSIs. Therefore, the aim of the study was to determine firefighters’ knowledge of and attitudes toward work-related MSIs in the City of Cape Town Fire and Rescue Service.
Methods
The study made use of convenient sampling and recruited 226 firefighters in the City of Cape Town Fire and Rescue Service. A self-administered researcher-generated questionnaire was used to collect information on the firefighters’ knowledge and attitudes about work-related MSIs. To ensure the validity and reliability of the questionnaire, the questionnaire underwent face and content validity, as well as a pilot study was conducted to ensure the questionnaire was suitable for research purposes. Mann-Whitney-U test, Kruskal-Wallis-H test, Spearman’s rank correlation and linear regression were utilized for data analyses. Statistical significance was set at a p-value less than 0.05.
Results
The results showed that most firefighters (62.6%) had good knowledge of work-related MSIs, and the majority (59.0%) had negative attitudes toward work-related MSIs. In addition, positive correlations were present between overall knowledge of work-related MSIs and overall attitudes toward work-related MSIs (r = 0.423, p <0.001) and between attitudes toward physical activity (r = 0.439, p <0.001). Overall knowledge of MSIs was linearly related to overall knowledge of MSIs (β = 0.383, p <0.001).
Conclusion
The majority of firefighters had good knowledge of work-related MSIs, but-negative attitudes toward MSIs. The promotion of educational programmes using short courses, workshops and webinars on the factors contributing to the high injury prevalence should be implemented and encouraged.
1. INTRODUCTION
While on active duty, firefighters encounter dangerous conditions that place them at risk of injury, and even death [1]. Musculoskeletal injuries (MSIs) are one of the most common injuries sustained within the firefighting profession [2]. This may, likely, be due to the firefighters’ lack of knowledge and poor attitudes toward MSIs, leading to ineffective safety behaviours concerning work-related MSIs [3]. A study conducted on firefighters in Cape Town reported that 27.4% of firefighters reported injuries that increased as firefighters aged and their years of experience increased [4]. Similarly, a later study reported a significantly higher injury prevalence of 42.1%, which also noted that injuries increased as firefighters aged and became more experienced [5].
Multiple factors contribute to the susceptibility of firefighters sustaining injuries, ranging from a lack of knowledge of personal protective equipment (PPE) − to dealing with rapid postural adjustments in body position that place excessive strain on muscles and joints, thereby contributing to musculoskeletal injury [6]. Previous studies indicated that MSIs occurred in all regions of the body, with the most common areas being the legs, trunk, and lumbar region of the back [1, 7, 8]. This was due to various reasons, such as carrying heavy equipment, obesity, and using incorrect PPE [9]. According to Szubrt et al. [10], firefighters with more years of experience in the fire service had a lower injury rate than firefighters with fewer years of experience, likely due to an increase in age and subsequent “wear and tear” over several years of firefighting. Potts et al. [11] reported on the various barriers that firefighters encountered when reporting injuries and showed that 53.2% of injuries were due to their cultural attitudes in accepting that pain was a natural part of the job. Other cultural barriers include the stigma of being a firefighter and healthy firefighter (29.3%), jeopardizing the future of their current career (31.2%), disappointing their fellow firefighters (32.2%), difficulty with workers’ compensation claims (40.1%), and their inability to determine if the injury was work-related (44.6%) [11]. Moreover, Potts et al. noted that most firefighters ignored minor injuries and failed to address these ailments timeously, which often led to these minor injuries progressing in severity, thereby placing their health and lives at risk [11]. Carrying an injury while on duty, negatively affected how swiftly firefighters responded to an emergency, as well as the quality of service provided [12]. This is supported by a study conducted by Ras et al. who reported that firefighters who carried an injury or had musculoskeletal discomfort performed tasks that focused on the injured or discomforted area, performed significantly worse on occupational specific tasks.
A previous study indicated that a positive relationship existed between firefighters’ knowledge and attitudes toward MSIs [13]. Firefighters with low levels of knowledge and poor attitudes about MSIs were more likely to sustain an injury while on duty compared to firefighters with more knowledge and positive attitudes about injuries [14]. Therefore, the aim of this study is to determine the relationship between firefighters’ knowledge of work-related MSIs and their attitudes toward work-related MSIs in firefighters in Cape Town. We hypothesize that firefighters who have a better knowledge of MSIs will have more positive attitudes toward MSIs. Although numerous studies have been conducted on the prevalence and causes of MSIs in firefighters, as well as the effect on work performance [8, 15-17], there have not been any studies conducted on the knowledge of firefighters on work-related MSIs or their attitudes toward MSIs. This places a significant gap in the literature, which the current study is looking to address.
2. METHODS
The study used a cross-sectional research design, where 226 full-time firefighters were conveniently in the City of Cape Town Fire and Rescue Service (CoCTFRS). Information on the study was provided to each participant before written informed consent was obtained from all firefighters who agreed to voluntarily participate in the study. The study took place between July and August 2022, which coincided with the annual wellness and fitness testing period. Ethical approval for the study was obtained from the Biomedical Research Ethics Committee at the University of the Western Cape (Ethics reference: BM22/4/13). In addition, when collecting data, the ethical standards of the Declaration of Helsinki were followed to ensure all ethical considerations were adhered to.
2.1. Data Collection, Instruments, and Procedures
During the yearly physical fitness exam, the question- naires were filled out in person during the annual firefighter physical fitness assessment. Firefighters who voluntarily agreed to take part in the study were given a paper-based, self-administered questionnaire (Supple- mentary) to fill in their attitudes and knowledge of work-related MSIs. To ensure firefighters were able to complete the questionnaire, firefighters were approached prior to completing the physical ability test while they were awaiting their turn to perform the physical ability test. Firefighters who were unable to complete the question- naire were approached after completing the physical ability test. Eight components (sections A-H) made up the questionnaire. The following includes an explanation of each section of the questionnaire:
2.1.1. Section A: Personal Information
This section initiates the questionnaire by collecting demographic data, ensuring confidentiality, and estab- lishing the anonymity of respondents. It includes inquiries about age, years of service, marital status, gender, health status, and health-seeking behaviors related to MSIs and smoking habits.
2.1.2. Section B: Knowledge on Work-related MSIs and Injury Management
This section questioned respondents' cognitive comprehension of common MSIs, their etiology, and appropriate management strategies are assessed. The section comprised statements prompting respondents to indicate their level of agreement or disagreement regarding various aspects of MSIs and their prevention.
2.1.3. Section C: Knowledge of Personal Protective Equipment (PPE)
Focusing on PPE, this section evaluated respondents' understanding of its significance in preventing MSIs, as well as their knowledge regarding its selection, usage, and maintenance. Statements addressed specific aspects, such as the effectiveness of firefighting boots and the potential hazards associated with PPE.
2.1.4. Section D: Knowledge of Physical Fitness (PF)
In this section, respondents' awareness of the role of physical fitness in MSI prevention and management was explored. Statements examined beliefs about the impact of exercise, dietary habits, and overall physical health on reducing MSI risk.
2.1.5. Section E: Attitudes About Diet
This section evaluated respondents' attitudes toward dietary habits, obesity, and their perceived influence on MSI risk. Statements assess beliefs regarding the relation- ship between obesity, decreased performance, mobility issues, and their potential impact on MSIs.
2.1.6. Section F: Attitudes About Firefighting Culture
Addressing cultural norms within firefighting, this section explored attitudes toward injury reporting practices, seeking medical assistance, and potential stigmatization associated with injury disclosure.
2.2. Questionnaire Scoring
The 20 items in the knowledge section of the questionnaire (Sections B to D) carried a five-point score, ranging from strongly disagree (1) to strongly agree (5), for a total of 100 points (20x5). Sections E through H of the questionnaire, which assessed attitudes toward MSIs, included 23 items that were identical to those in the preceding section. The overall score was 115 points (23×5). Knowledge of MSIs was graded as “Good” ≥80% or “Poor” <80%. All questions were given an equal score accumulating to the 100 points allocated for knowledge and 115 points allocated for their attitudes score. Firefighters’ attitudes toward MSIs were graded as “positive” ≥80% or “negative” <80%. The pass/ fail percentage for knowledge was based on previous studies that investigated knowledge scores indicating that 80% was a good indicator for knowledge which was based on previous studies [18-21]. In addition, the attitudes were graded based on studies that used a similar percentage [18-21]. When scoring the firefighters' overall knowledge and attitudes, their knowledge score was added, based on their correct responses, and divided by the total score. For each correct response, one to five points were awarded.
2.3. Validity and Reliability of the Questionnaire
The questionnaire was developed using previous questionnaires and using previous literature, each section and question was developed. To ensure the reliability and validity of the questionnaire, the questionnaire underwent face and content validity [22-24] by experts in the field (LL, JR, MM, GA). In addition, to ensure the content validity, a pilot study was conducted on a subsample of firefighters. The questionnaire was found to accurately retrieve the information it was intended to ascertain and was the content was found to be reliable using Cronbach’s alpha statistic (α = 0.679).
2.4. Statistical Analysis
A Microsoft Office Excel spreadsheet for cleaning the data using the double-entry method. For the double-entry methods, two data-entry teams were formed, each required to input their data into he Excel spreadsheet. Once complete, the Excel sheets were compared and any errors were removed. In addition, to ensure the accuracy of data input, each variable’s mean and standard deviation, as well as range, was calculated and compared to ensure the accuracy of the inputted data. Thereafter, Statistical Package for the Social Sciences (SPSS) version 28 was then used to import the data and analyze it both descriptively and inferentially. A Shapiro-Wilk test was conducted to discern the distribution of the data, which was shown to be not normally distributed. Descriptive statistics, such as means, standard deviations, and frequencies. In addition, due to the data’s deviation from normality, non-parametric inferential statistics were preferred, such as Mann-Whitney-U test and Spearman’s rank correlation coefficient, to determine the relationship between firefighter’s knowledge of and attitudes toward work-related MSIs. For the percentages, firefighters that had a good and poor knowledge and positive and negative attitudes toward MSIs were presented. In addition, firefighters’ knowledge and attitudes percentages were separated by gender, age category, years of experience, and marital status. For the Mann-Whitney U test, differences were determined between firefighters’ knowledge and attitudes based on their individual sex, age category they fell into and their years of experience. For the Spearman’s rank correlation, relationships were determined between age, years of experience, and each main subsection of the questionnaire, such as age, years of experience, overall knowledge on injuries, knowledge on injuries, knowledge on PPE, knowledge of physical fitness, overall attitudes, attitudes toward diet and obesity, attitude toward firefighting culture, attitudes toward physical activity, attitudes toward musculoskeletal injuries. Univariable linear regression was performed to test the linear relationship between firefighter knowledge of and attitudes toward MSIs and each individual section of the questionnaire, namely, overall knowledge on injuries, knowledge on injuries, knowledge on PPE, knowledge of physical fitness, overall attitudes, attitudes toward diet and obesity, attitude toward firefighting culture, attitudes toward physical activity, attitudes toward musculoskeletal injuries. In addition, standardized beta-coefficients were used to indicate the strength of the relationship. In the multivariable analysis, the independent variables were adjusted for age, as this was found to be a significant factor in the knowledge and behaviours of firefighters, particularly, as firefighters are older and gain more years of experience, they naturally accumulate more knowledge, which may influence their attitudes [18-21]. When conducting the regression analysis on the statistical software, linear regression was performed using the conventional dropdown method. In addition, a forward stepwise method of analysis was used. A p-value of less than 0.05 was used to indicate statistical significance.
3. RESULTS
The mean age of the firefighters was 38.16±10.7 years, ranging from 20 to 65 years. Males and females had a mean age of 38.01±10.50 and 38.73±7.89 years, respectively. According to age groups, the 20–29 age group made up 22.1% of the sample, the 30-39 age group made up the largest percentage (28.1%), the 40–49 age group made up 26.2%, the 50–59 age group made up 11.1%, and the 60–65 age group made up the smallest percentage of study participants (1.8%) (Table 1).
A total of 37.4% were reported to have a poor knowledge of MSIs and 62.6% of firefighters were reported to have a good knowledge of MSIs. The majority (59%) of firefighters reported negative attitudes toward MSIs, and 41% reported positive attitudes toward MSIs. Knowledge of and attitudes toward MSIs were similar among sexes of firefighters; however, males tended to be more knowledgeable and have a better attitude toward injuries. According to gender, 63.3% of men and 61.5% of females reported good knowledge of MSI, whereas 36.7% of males and 38.5% of females reported poor knowledge of MSIs. Negative attitudes toward MSIs were reported in 55.1% of males and 61.5% of females, and positive attitudes toward MSIs were reported in 44.9% of males and 38.5% of females. The youngest age group of 20-29 years and the older age-group had the best knowledge of MSIs; however, the 40–49 years age-group had the poorest attitudes toward MSIs. Based on experience, firefighters with 6-10 years of experience had the best knowledge and had the poorest attitudes toward MSIs.
Table 2 delineates the means and standard deviations, as well as significant differences between firefighters’ knowledge of and attitudes toward MSIs according to sociodemographic characteristics. The mean percentage score for knowledge of MSIs was 80.5± 11.1 and 77.1 ± 9.6 for attitudes toward MSIs, which was found to be significantly different (p <0.001). In males, the knowledge the mean percentage score for knowledge of MSIs was 81.3±8.0 and 77.4 ± 8.2 for attitudes toward MSIs, which was found to be significantly different (p <0.001). The mean knowledge score and mean attitudes score for the age group 20-29 years were 81.8±6.8 and 78.5±7.1, respectively, which were found to be significantly different (p = 0.009). The mean knowledge percentage and mean attitudes percentage for the age group 30-39 years were 80.8±6.9 and 77.7±7.6, respectively, which were found to be significantly different (p = 0.015). The mean knowledge percentage and mean attitudes percentage for the age group 40-49 years were 80.7±8.3 and 77.4±7.0, respectively, which were found to be significantly different (p = 0.013). In addition, the mean knowledge percentage score and mean attitudes percentage score for the age group 50-65 years were 81.5±10.7 and 75.3±10.3, respectively, which were found to be significantly different (p = 0.002). Regarding years of experience, the mean knowledge and attitudes towards MSIs percentage score were 81.9±7.6 and 78.1±6.9 for the 0-5 years of experience group, which was found to be significantly different (p = 0.007). For firefighters with 6-10 years of experience, the mean knowledge of and attitudes towards MSIs percentage scores were 81.9±5.8 and 77.7±6.1, respectively, which was found to be significantly different (p = 0.009). The mean knowledge of and attitudes towards MSIs percentage scores were 81.7±8.9 and 77.6±9.4, respectively, which were found to be significantly different (p <0.001). Single firefighters had a mean knowledge of and attitudes towards MSIs percentage score of 81.8±7.9 and 77.3±7.0, which was significantly different (p <0.001). Married firefighters had a mean knowledge of and attitudes toward MSIs with a percentage score of 81.3±7.2 and 78.6 ±7.1 and were found to be significantly different (p = 0.014).
| Variable | n. | % | Knowledge of Injuries (%) | Attitudes toward Injuries (%) | ||
|---|---|---|---|---|---|---|
| - | - | - | Good* | Poor | Positive* | Negative |
| Total | 226 | 100.0 | 62.6 | 37.4 | 41.0 | 59.0 |
| Gender | 222 | 100.0 | - | - | - | - |
| Male | 196 | 86.7 | 63.3 | 36.7 | 44.9 | 55.1 |
| Female | 26 | 11.5 | 61.5 | 38.5 | 38.5 | 61.5 |
| Age category (years) | 202 | 100.0 | - | - | - | - |
| 20-29 | 50 | 22.1 | 70.0 | 30.0 | 46.0 | 54.0 |
| 30-39 | 64 | 28.1 | 59.4 | 40.6 | 48.4 | 51.6 |
| 40-49 | 59 | 26.2 | 57.6 | 42.4 | 37.3 | 62.7 |
| 50-59 | 25 | 11.1 | 72.0 | 28.0 | 48.0 | 52.0 |
| 60-65 | 4 | 1.8 | 100 | 0.0 | 75.0 | 25.0 |
| Years of experience | 190 | 100.0 | - | - | - | - |
| 0-5 | 52 | 23.0 | 63.5 | 36.5 | 48.1 | 51.9 |
| 6-10 | 34 | 15.1 | 70.6 | 29.4 | 41.2 | 58.8 |
| 11-15 | 26 | 11.5 | 65.4 | 34.6 | 46.2 | 53.8 |
| 16 + | 78 | 34.5 | 64.1 | 35.9 | 46.2 | 53.8 |
| Marital status | 202 | 100.0 | - | - | - | - |
| Single | 86 | 38.0 | 65.1 | 34.9 | 43.0 | 57.0 |
| Married | 96 | 42.6 | 61.5 | 38.5 | 47.9 | 52.1 |
| *Other | 20 | 8.8 | 75.0 | 25.0 | 45.0 | 55.0 |
*Poor knowledge and negative attitudes < 80%.
*Other including cohabiting, divorced, widowed or separated.
| Variable | n. | Knowledge of MSIs x̅ ± SD |
Attitudes toward MSIs x̅ ± SD |
p-value |
|---|---|---|---|---|
| Total | 228 | 80.5± 11.1 | 77.1 ± 9.6 | <0.001** |
| Sex | 226 | - | - | |
| Male | 200 | 81.3±8.0 | 77.4 ± 8.2 | <0.001 |
| Female | 26 | 80.8±9.2 | 78.1±8.1 | 0.138 |
| Age category (years) | 202 | - | - | - |
| 20-29 | 49 | 81.8±6.8 | 78.5±7.1 | 0.009** |
| 30-39 | 65 | 80.8±6.9 | 77.7±7.6 | 0.015* |
| 40-49 | 59 | 80.7±8.3 | 77.4±7.0 | 0.013** |
| 50-65 | 49 | 81.5±10.7 | 75.3±10.3 | 0.002** |
| Years of experience | 190 | - | - | - |
| 0-5 years | 52 | 81.9±7.6 | 78.1±6.9 | 0.007** |
| 6-10 years | 34 | 81.9±5.8 | 77.7±6.1 | 0.009** |
| 11-15 years | 26 | 81.4±7.9 | 79.8±7.9 | 0.225 |
| 16 + years | 78 | 81.7±8.9 | 77.6±9.4 | <0.001** |
| Marital status | 202 | - | - | - |
| Single | 86 | 81.8±7.9 | 77.3±7.0 | <0.001** |
| Married | 96 | 81.3±7.2 | 78.6 ±7.1 | 0.014* |
| *Other | 20 | 80.5±12.8 | 76.6±14.2 | 0.102 |
In Fig. (1), firefighters' knowledge is presented according to each specific category, i.e., knowledge of PPE, knowledge of work-related MSIs, and knowledge of physical fitness. Overall, 59.7% of all respondents had a good knowledge of MSIs, while 40.3% had poor knowledge of MSIs. The proportion of firefighters with good knowledge of PPE was 50.9% and 49.1% for firefighters with poor knowledge of PPE. The proportion of firefighters with good knowledge of work-related MSIs was 59.3% and 40.7% for firefighters with poor knowledge of MSIs. The proportion for good knowledge of physical fitness was 79.6% for firefighters and 20.4% for firefighters with poor knowledge of physical fitness.
In Fig. (2), the firefighters' knowledge is presented according to each specific category, i.e., attitudes toward diet and obesity, attitudes toward firefighting culture, attitudes toward physical activity and attitudes toward MSIs. Overall, 41.6% of all respondents had a positive attitude toward MSIs, while 58.4% had negative attitudes toward MSIs. A higher proportion of firefighters had negative attitudes toward firefighting culture (35.0% vs. 65.0%), diet and obesity (39.8% vs. 60.2%), and toward MSIs (42.5% vs. 57.5%). The proportion of firefighters with positive attitudes toward physical activity was 63.0% and 27.0% of firefighters with negative attitudes toward physical activity.
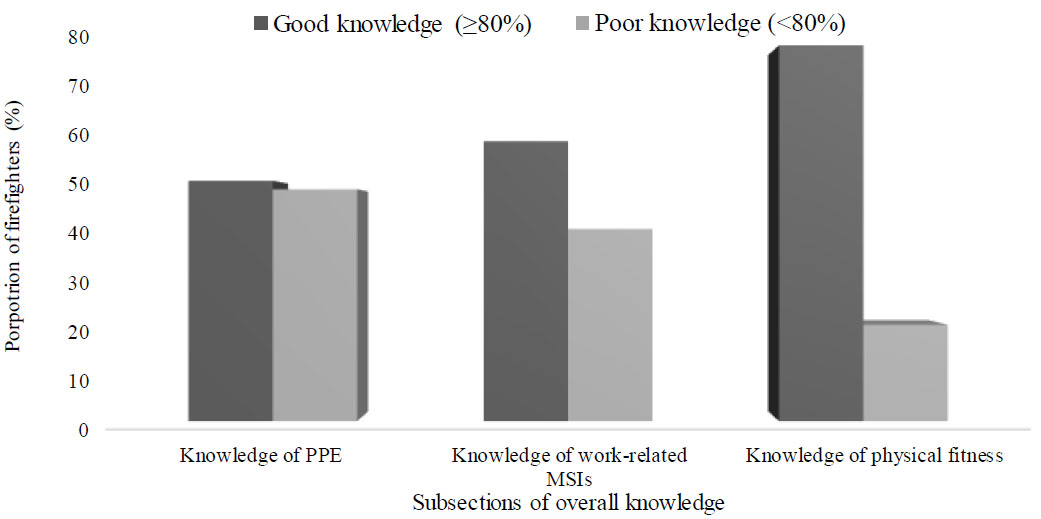
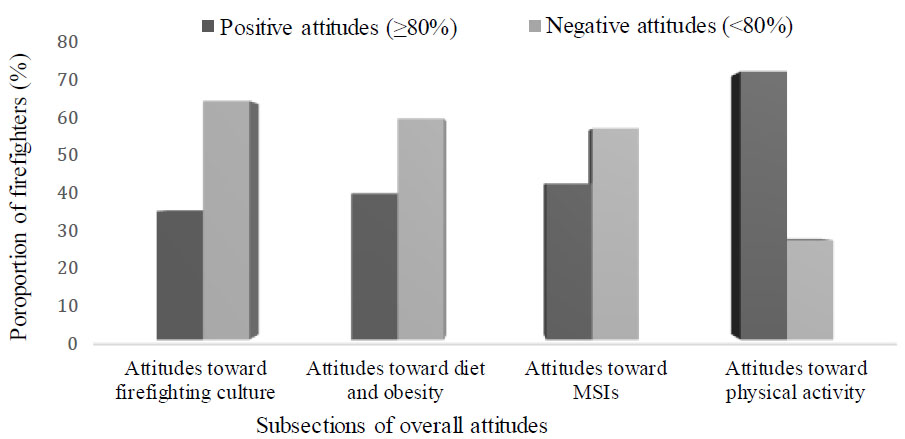
Table 3 describes the correlation between knowledge of and attitudes toward MSIs in firefighters. Age had a weak and negative correlation with knowledge of MSIs (r = -0.234, p <0.001), and overall knowledge and knowledge of PPE (r = -0.188, p < 0.003), knowledge of physical fitness (r = -0.283, p <0.001), attitudes toward firefighting culture (r = -0.234, p <0.001), and attitudes toward physical activity (r = 0.274, p <0.001) and negatively and moderately correlated with attitudes toward diet and obesity (r = -0.322, p <0.001). Overall knowledge of MSIs had a weak positive correlation and attitudes toward diet and obesity (r = 0.188, p = 0.004), attitudes toward firefighting culture (r = 0.228, p <0.001) and moderate positive correlations with overall attitudes toward MSIs (r = 0.423, p <0.001), and attitudes toward physical activity (r = 0.446, p <0.001) and attitudes toward MSIs (r = 0.382, p <0.001). Knowledge of injuries had a weak positive correlation with overall attitudes toward MSIs (r = 0.282, p <0.001), and moderate correlations with attitudes toward diet and obesity (r = 0.319, p <0.001), attitudes towards firefighting culture (r = 0.467 p <0.001) attitudes toward physical activity (r = 0.407, p <0.001) and attitudes toward MSIs (r = 0.325, p <0.001). Knowledge on PPE had a weak positive correlation with overall attitudes toward MSIs (r = 0.286, p <0.001), and moderate positive correlations with attitudes toward diet and obesity (r = 0.393, p <0.001), attitudes toward firefighting culture (r = 0.431, p <0.001) and attitudes toward physical activity (r = 0.485, p <0.001) and attitudes toward MSIs (r = 0.174, p <0.001). Knowledge of physical activity had a moderate positive correlation with overall attitudes toward MSIs (r = 0.395, p <0.001), attitudes toward diet and obesity (r = 0.480, p <0.001), attitudes toward firefighting culture (r = 313; p <0.001), attitudes toward physical activity (r = 0.705, p <0.001) and attitudes toward MSIs (r = 0.317, p <0.001).
| - | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|
| Years of experience | 0.493** | - | - | - | - | - | - | - | - |
| Overall knowledge on musculoskeletal injuries | 0.220 | 0.079 | - | - | - | - | - | - | - |
| Knowledge on injuries | -0.234** | 0.094 | 0.767** | - | - | - | - | - | - |
| Knowledge on PPE | -0.188** | 0.058 | 0.730** | 0.578** | - | - | - | - | - |
| Knowledge of physical fitness | -0.283** | 0.008 | 0.554** | 0.356** | 0.286** | - | - | - | - |
| Overall attitudes toward musculoskeletal injuries | -0.059 | 0.060 | 0.423** | 0.282** | 0.456** | 0.395** | - | - | - |
| Attitudes toward diet and obesity | -0.322** | -0.041 | 0.188** | 0.319** | 0.393 ** | 0.480** | 0.707** | - | - |
| Attitudes toward firefighting culture | -0.234** | 0.096 | 0.218** | *0.467 | 0.431** | 0.313** | 0.638** | 0.400** | - |
| Attitudes toward physical activity | -0.274** | 0.058 | 0.439** | 0.407* | 0.485** | 0.705** | 0.689** | 0.564** | 0.376** |
| Attitudes toward musculoskeletal injuries | -0.109 | 0.068 | 0.382** | 0.325* | 0.174** | 0.317* | 0.686** | 0.416** | 0.689** |
| - | Univariate Models a | Multivariable Analysis b | ||||||
|---|---|---|---|---|---|---|---|---|
| β | SE | R2 | p-value | β | SE | R2 | p-value | |
| Model: Overall attitudes toward musculoskeletal injuries | - | - | - | - | - | - | - | - |
| Overall knowledge of musculoskeletal injuries | 0.383 | 0.420 | 0.191 | <0.001** | 0.423 | 0.073 | 0.189 | <0.001** |
| Knowledge on injuries | 0.294 | 0.066 | 0.081 | <0.001** | 0.281 | 0.079 | 0.085 | <0.001** |
| Knowledge on PPE | 0.360 | 0.093 | 0.063 | <0.001** | 0.404 | 0.116 | 0.069 | <0.001** |
| Knowledge of physical fitness | 0.553 | 0.086 | 0.156 | <0.001** | 0.530 | 0.105 | 0.159 | <0.001** |
| - | - | - | - | - | - | - | - | - |
| Model: Attitudes toward diet and obesity | - | - | - | - | - | - | - | - |
| Overall knowledge of musculoskeletal injuries | 0.130 | 0.046 | 0.035 | 0.005** | 0.163 | 0.064 | 0.040 | 0.012* |
| Knowledge on injuries | 0.009 | 0.055 | 0.000 | 0.867 | - | - | - | - |
| Knowledge on PPE | 0.311 | 0.072 | 0.077 | <0.001** | 0.219 | 0.094 | 0.048 | 0.020* |
| Knowledge of physical fitness | 0.173 | 0.075 | 0.023 | 0.022* | 0.318 | 0.087 | 0.098 | <0.001** |
| - | - | - | - | - | - | - | - | - |
| Model: Attitudes toward firefighting culture | - | - | - | - | - | - | - | - |
| Overall knowledge of musculoskeletal injuries | 0.108 | 0.033 | 0.045 | 0.001** | 0.092 | 0.052 | 0.024 | 0.076 |
| Knowledge on injuries | 0.140 | 0.039 | 0.054 | <0.001** | 0.083 | 0.052 | 0.019 | 0.116 |
| Knowledge on PPE | 0.162 | 0.054 | 0.039 | 0.003** | 0.161 | 0.075 | 0.033 | 0.033* |
| Knowledge of physical fitness | 0.029 | 0.054 | 0.001 | 0.594 | - | - | - | - |
| - | - | - | - | - | - | - | - | - |
| Model: Attitudes toward physical activity | - | - | - | - | - | - | - | - |
| Overall knowledge of musculoskeletal injuries | 0.223 | 0.031 | 0.184 | <0.001** | 0.272 | 0.046 | 0.206 | <0.001** |
| Knowledge on injuries | 0.107 | 0.040 | 0.031 | 0.008** | 0.102 | 0.051 | 0.029 | 0.048* |
| Knowledge on PPE | 0.239 | 0.054 | 0.081 | <0.001** | 0.241 | 0.073 | 0.060 | 0.004** |
| Knowledge of physical fitness | 0.492 | 0.045 | 0.352 | <0.001** | 0.525 | 0.056 | 0.384 | <0.001** |
| - | - | - | - | - | - | - | - | - |
| Attitudes toward musculoskeletal injuries | - | - | - | - | - | - | - | - |
| Overall knowledge of musculoskeletal injuries | 0.101 | 0.016 | 0.144 | <0.001** | 0.131 | 0.024 | 0.184 | <0.001** |
| Knowledge on injuries | 0.091 | 0.020 | 0.084 | <0.001** | 0.100 | 0.025 | 0.105 | <0.001** |
| Knowledge on PPE | 0.079 | 0.028 | 0.034 | 0.005** | 0.133 | 0.037 | 0.089 | <0.001** |
| Knowledge of physical fitness | 0.135 | 0.027 | 0.102 | <0.001** | 0.143 | 0.035 | 0.112 | <0.001** |
| - | - | - | - | - | - | - | - | - |
Table 4 shows the relationship between the knowledge of and attitudes toward physical activity. Univariable analysis indicated that overall knowledge of MSIs (β = 0.383, p <0.001), knowledge of injuries (β = 0.294, p <0.001), knowledge of PPE (β = 0.360, p <0.001) and knowledge of physical fitness (β = 0.553, p <0.001) was a significant predictor of overall attitudes towards MSIs in firefighters. For every one-unit increase in overall knowledge of MSIs, knowledge of injuries, knowledge of PPE, and knowledge of physical fitness, attitudes toward MSIs increased by 0.383, 0.294, 0.360 and 0.553 points, respectively. After adjustment for age, all subsections remained significant predictors of overall attitudes of MSIs. Attitudes toward diet and obesity were found to be significant predictors of overall knowledge of MSIs (β = 0.130, p = 0.005), knowledge on PPE (β = 0.311, p <0.001) and knowledge of physical fitness (β = 0.173, p = 0.022). For every one-unit increase in attitudes towards diet and obesity, overall knowledge of MSIs, knowledge of PPE and knowledge of physical fitness increased by 0.130, 0.311 and 0.173 points, respectively. In the multivariable analysis, after the inclusion of age, overall knowledge of MSIs, knowledge of PPE and knowledge of physical fitness remained significant predictors of attitudes toward diet and obesity. Overall knowledge of MSIs (β = 0.108, p = 0.001), knowledge of injuries (β = 0.140, p <0.001) and knowledge of PPE (β = 0.162, p = 0.003) was found to be a significant predictor of attitudes toward firefighting culture in firefighters. In addition, for every one-unit increase in overall knowledge of MSIs, knowledge of injuries and knowledge of PPE, there was an increase of 0.108, 0.140 and 0.162 points in the attitudes of firefighters toward firefighting culture. After adjustment for age, knowledge of PPE remained a significant predictor of attitudes toward firefighting culture. Overall knowledge of MSIs (β = 0.223, p <0.001), knowledge of injuries (β = 0.108, p = 0.008), knowledge of PPE (β = 0.239, p <0.001) and knowledge of physical fitness (β = 0.492, p <0.001) was a significant predictor of attitudes toward physical activity in firefighters. Moreover, every one-unit increase in overall knowledge of MSIs, knowledge of injuries, knowledge of PPE and knowledge of physical fitness was associated with an increase of 0.223, 0.108, 0.239 and 0,.492, respectively, in attitudes toward physical activity. After adjustment for age, all subsections remained a significant predictor of attitudes toward physical activity. Overall knowledge of MSIs (β = 0.101, p <0.001), knowledge of injuries (β = 0.091, p <0.001), knowledge of PPE (β = 0.079, p = 0.005) and knowledge of physical fitness (β = 0.135, p <0.001) were significant predictors of attitudes toward physical activity in firefighters. Furthermore, every one-unit increase in overall knowledge of MSIs, knowledge of injuries, knowledge of PPE and knowledge of physical fitness was associated with an increase of 0.101, 0.091, 0.079 and 0.135 points in firefighters' attitudes toward physical activity. After adjustment for age, all subsections remained significant predictors of attitudes toward MSIs.
4. DISCUSSION
The results showed that the majority of firefighters had good knowledge of MSIs and had negative attitudes toward work-related MSIs. The age category of 60-65 years had the highest knowledge related to work-related MSIs and also displayed positive attitudes toward work-related MSIs. In addition, knowledge of MSIs was significantly and linearly related to attitudes toward MSIs, suggesting that knowledge of MSIs may be integral in bettering firefighters’ attitudes toward MSIs. Ras et al. [18] reported that in the CoCTFRS less than half of firefighters (47.2%) had good knowledge of cardiovascular disease risk factors, whereas the majority (90%) had positive attitudes about cardiovascular disease risk factors, highlighting the importance of increasing knowledge of firefighters to better their behaviors related to maintaining their health. Moreover, the results of the current study suggest that although increasing overall knowledge may be important, this may not always translate to better attitudes toward MSIs in firefighters. Studies have suggested that firefighters tend to become more negative as they progress through their careers, often due to the stressors of the profession and lack of career progression [18, 19, 21].
The results found in the present study indicated that the majority of firefighters had negative attitudes toward MSIs. In addition, we found that knowledge of MSIs was significantly associated with attitudes toward MSIs. Reinhardt-Klein [25] stated that firefighters’ attitudes were strong predictors of firefighters’ risk-taking intention, leading to a higher number of injuries within the fire service. Although they were unaware of their body weight, firefighters in the current study had a good attitude toward their bodies as to how they should look or the condition they are in. Additionally, firefighters preferred to exercise as a means to control their weight, as opposed to adopting healthier dietary practices. We found that firefighters in the age categories 20-29, 50-59 and 60-65 years had good knowledge of MSIs. Soederbeg Miller [26] reported that as individuals become older, the longer they are part of that working environment, their knowledge of their working environment will increase accordingly. In contrast, Smith et al. [27] reported that firefighters presented with poor knowledge of MSIs, which contributed to poor attitudes toward MSIs in firefighters. In the current study, the majority of firefighters in all age categories, as well as firefighters across all years of experience, had a good knowledge of MSIs. Firefighters’ knowledge may not be influenced by their private lives but rather by the skills they have acquired during training [28]. Ras et al. [18] reported that the majority of firefighters had poor knowledge of their health, with the exception of the age category 30-39 years, who had good knowledge of their health. We found that firefighters in all age categories, except for the 60-65-year age category, had negative attitudes toward work-related MSIs. Similarly, the current study also reported that all firefighters, regardless of their years of experience in active service, had negative attitudes toward MSIs. Firoozeh et al. [28] and Ras et al. [18] reported that financial strain and marital obligations could influence firefighters’ attitudes toward their careers, as well as general unhappiness in their careers. Another contributing factor to the negative attitudes toward firefighters is that firefighting is a stressful profession, and firefighters are constantly exposed to dangerous and gruesome scenes that often break down their mental resilience and morale [29]. The results of the current study found that knowledge of MSIs and attitudes toward MSIs tended to differ between each category of experience. Ras et al. [18] also reported that firefighters with six or more years of experience had good knowledge of their health and tended to have a positive attitude toward their health. This is in contrast to the present results, where firefighters across the experience categories tended to have poor attitudes, with the most experienced firefighters having the poorest attitudes toward MSIs.
The results of the current study found that attitudes toward physical activity were predicted by firefighters' knowledge of MSIs, knowledge of PPE and knowledge of physical fitness. Similarly, a study by Ras et al. [21] reported that an increase in knowledge of physical activity was associated with an increase in behaviours related to physical activity. Firefighters who had a poorer attitude toward physical activity may likely be physically inactive and, perhaps, overweight or obese, which has been linked to MSIs in firefighters [8, 30, 31]. In addition, studies have shown that firefighters often reported having negative attitudes toward diet and obesity [29, 32]. Firefighters reported having insufficient time to prepare healthy foods and often opted for fast foods, which were easy to acquire. In addition, as firefighters became older, gained more years of experience and became more disgruntled with their profession, their motivation to remain physically active diminished. Moreover, previous studies have shown that firefighters' attitudes toward physical activity were significantly correlated with overall health knowledge and specific knowledge of MSIs [3, 11, 29]. This indicated that as firefighters' knowledge of MSIs increased, so did their attitudes toward physical activity. The results of the present study echoed these findings as it was shown that firefighters who had a better knowledge of MSIs, subsequently, had better overall attitudes toward MSIs and for each subsection of the questionnaire section on attitudes toward MSIs. Poston et al. [33], reported that body composition did not have a significant impact on the overall injuries of firefighters. In contrast, Shaikha et al. [14] reported that poor attitudes toward injuries have also been shown to increase the risk of injuries. Shaikha et al. [14] also stated that this affected how swiftly firefighters could respond to emergencies. There was linear relationship between overall knowledge and overall attitudes about work-related MSIs. Firefighters had good knowledge about MSIs, but this did not translate into a positive attitude toward MSIs, and was not prominent in the 20-29 and 30-39 years age groups, and those with 6-10 years of experience. The disparity in health knowledge and attitude could be attributed to an increase in knowledge accumulated with age and experience [34]. In contrast, Smith [35] reported that poor health knowledge in firefighters likely caused the poor attitudes seen in firefighters. This suggests that when implementing policies and training programs, younger firefighters should be targeted as bettering their knowledge may lead to better attitudes early in their careers, potentially reducing the likelihood of injuries, the reporting of injuries, and seeking out appropriate medical care when the need arises [2, 8].
In the current study, the majority of the firefighters were aware that poor quality firefighting boots, ill-fitting personal protective equipment, a lack of muscular strength training, and poor physical fitness levels all contributed to causing MSIs in firefighters. In a study by Garner et al. [1], the objective was to compare two boot styles that firefighters frequently wear on duty in terms of posture and lower limb muscular fatigue. The primary findings of this study were that wearing rubber boots caused more muscle fatigue in each of the lower limbs' examined musculature and increased the velocities of anterior/posterior and medial/lateral sway in all postural tests. The findings of this study confirm earlier findings that postural instability increased with increasing exposure time in work or fire boots. By comparing the two types of recognized footwear, this study builds on earlier research and contends that firefighters who wear rubber boots run the risk of developing postural problems [1]. Moreover, studies have shown that firefighting PPE is often designed for males and tend to be ill-fitting to female firefighters [36]. This tended to increase the risk of injury in female firefighters [36], which has often been seen in this population, and especially in firefighters in Cape Town [4, 5, 37]. Educating firefighters on the injury risk of ill-fitting PPE may allow them to actively seek out better-fitting equipment, reducing injury risk.
4.1. Strengths and Limitations
This study provides valuable evidence of knowledge and attitudes toward MSIs among firefighters in an understudied population, specifically in the City of Cape Town, South Africa. Additionally, the current study was the first conducted in South Africa to compare the knowledge of and attitudes toward work-related MSIs related to socio-demographic characteristics, such as age, gender, years of experience, and marital status. The study was limited by convenient sampling and a relatively small sample size, which impacted the study's external validity. In addition, the use of convenient sampling may introduce potential bias and reduce the generalizability of the findings to firefighters in the region. A relatively small sample size further restricts the generalizability of the study’s findings. Female firefighters were also underrepresented in the study, which reduces the generalizability of the study to the female firefighting population, as well has limits the ability to conclude gender-specific differences in knowledge and attitudes toward MSIs.
CONCLUSION
Good knowledge about work-related MSIs was generally related to firefighters’ age and years of experience in the fire service. Hence, firefighters aged between 50-59 and 60-65 years had a good knowledge of work-related MSIs. In contrast, poor knowledge about work-related MSIs was most prevalent in the 40-49 year age group. The majority of firefighters had negative attitudes toward work-related MSIs. However, positive attitudes were most prevalent across all age categories of firefighters, except for the firefighters aged 60 years and older. Firefighters’ overall knowledge and their overall attitudes about work-related MSIs were significantly related. This study highlighted the high prevalence of negative attitudes toward work-related MSIs among Cape Town firefighters, as well as the need for educationalbased training measures to improve firefighters' attitudes. The promotion of educational programs on the factors contributing to the high injury prevalence, and the proper safety measures could assist in improving firefighters' knowledge about work-related MSIs and promote positive attitudes toward MSIs. In addition, the shift in attitudes toward MSIs may reduce the likelihood of MSIs by improving firefighters' knowledge and increasing the amicability of firefighters in seeking out preventative measures to reduce the incidence of injuries, and in doing so, increasing firefighter well-being and longevity.
RECOMMENDATIONS
It is suggested that future studies utilize random sampling and ensure the study is sufficiently powered to ensure external validity. An equitable representation of firefighters according to age category and gender should be included in the sampling strategy, which was a shortcoming of the current study.
AUTHORS' CONTRIBUTION
It is hereby acknowledged that all authors have accepted responsibility for the manuscript's content and consented to its submission. They have meticulously reviewed all results and unanimously approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| EMTs | = Emergency Medical Technicians |
| MSIs | = Musculoskeletal injuries |
| PPE | = Personal Protective Equipment |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical approval for the study was obtained from the Biomedical Research Ethics Committee at the University of the Western Cape (Ethics reference: BM22/4/13).
HUMAN AND ANIMAL RIGHTS
When collecting data, the ethical standards of the Declaration of Helsinki were followed to ensure all ethical considerations were adhered to.
CONSENT FOR PUBLICATION
Information about the study was provided to the participants in person, and after, written informed consent was obtained online for voluntary participation in the study.
AVAILABILITY OF DATA AND MATERIALS
The data and supportive information are available within the article.

