All published articles of this journal are available on ScienceDirect.

Personal and Environmental Hygiene Practices of Mothers in Selected Primary Health Centers in Ekiti State, Nigeria: A Cross-Sectional Study
Authors Info & Affiliations
Abstract
Introduction
Maintaining personal and environmental hygiene is crucial for preventing infections, such as diarrhea, among children under five years of age. This study has assessed the personal and environmental hygiene practices of mothers attending primary health centers in Ekiti State, Nigeria.
Methods
A descriptive cross-sectional design was employed to evaluate the hygiene practices of mothers attending baby wellness clinics. Data were collected using a semi-structured questionnaire and a checklist. The results were analyzed using descriptive statistics, presented in tables and charts.
Results
The findings revealed that 60.3% of respondents consistently washed their hands with soap and water before feeding their children, while 60.9% only occasionally washed their hands after using the toilet. The majority (78.8%) of breastfeeding mothers reported washing their brassieres weekly. In terms of environmental hygiene, 71.52% of respondents cleaned their surroundings daily, though 24.51% still disposed of their waste by the roadside. Overall, the hygiene level of mothers was low, with an average index value of 0.5428.
Conclusion
The study has found poor hand hygiene practices to be prevalent among the mothers surveyed. There is a need for increased health education and public awareness campaigns focusing on personal and environmental hygiene practices.
1. INTRODUCTION
Diarrhea remains one of the leading causes of morbidity and mortality among children under five years of age in developing countries [1]. In 2016, diarrhea contributed to 8% of global under-five deaths [2]. According to Oloruntoba et al. [3], approximately 2.5 million children under five years of age experience episodes of diarrhea annually, with the situation remaining unchanged for two decades. In 90% of cases, poor maternal hygiene is a major contributing factor [4].
Hygiene plays a pivotal role in health promotion and illness prevention. It involves practices that promote a clean and habitable environment, thus supporting individual well-being and reducing illness incidence [5]. The concept of hygiene, rooted in nursing principles, emphasizes illness prevention and health promotion, with cleanliness being central to these objectives [6].
Environmental hygiene is particularly crucial for the health of pregnant women and their unborn children, underlining the importance of maintaining hygienic practices to prevent infections [7]. While personal hygiene focuses on maintaining the individual's cleanliness, environmental hygiene pertains to the cleanliness of one's surroundings [8]. Though both men and women are responsible for environmental cleanliness, societal expec- tations often place this burden on women. For instance, Uchem and Ngwa [9] assert that despite the hard work exhibited by many African women, they continue to face discrimination and are often relegated to menial roles within the household.
Poor environmental and personal hygiene contributes significantly to under-five diarrhea cases. Many of these cases result from maternal negligence in maintaining cleanliness during child feeding [4], leading to severe illnesses that may require hospitalization. According to WHO [10], children under five suffering from diarrhea represent a significant portion of hospital admissions, with cases often linked to poor feeding practices.
Nun et al. [11] emphasized that proper hygiene involves more than personal cleanliness, extending to behaviors that prevent disease transmission. Personal hygiene practices include grooming, skin care, oral hygiene, and handwashing [7]. Given the critical role of environmental hygiene in health promotion, this study aimed to assess the current personal and environmental hygiene practices of mothers of under-five children in Ekiti State. Furthermore, this study sought to determine the hygiene index using the parameters observed.
2. METHODS
2.1. Study Design
This cross-sectional study was conducted among mothers of children under five attending three primary healthcare facilities in Ekiti State, Nigeria, between May 1 and June 30, 2017. The study has assessed the personal and environmental hygiene practices in relation to infant morbidity profiles.
2.2. Study Setting
This study was conducted in Ekiti State, located in the southwestern region of Nigeria (Fig. 1). Situated entirely within the tropics, Ekiti State lies between longitudes 4°51' and 5°45' east of the Greenwich Meridian and latitudes 7°15' and 8°51' north of the Equator. The state is bordered to the north by Kwara and Kogi States, to the east by Osun State, and to the south and west by Ondo State, covering a total area of 5,887.89 square kilometers. Ekiti State came into being on October 1, 1996, with Ado-Ekiti as its capital. Administratively, the state is divided into 16 Local Government Areas (LGAs) [12]. The population of Ekiti State was recorded by the National Population Commission in the 2006 census to be 2,384,212, with an estimated annual growth rate of 3.1% [13]. By 2016, the National Bureau of Statistics projected the state's population at approximately 3,270,798 [14].
Data collection took place in three primary healthcare facilities within Ado-Ekiti: Okeyinmi Comprehensive Primary Health Care Center (OKCPHCC), Odo-Ado Basic Health Care Center (OABHCC), and Oke-Oniyo Basic Health Care Center (OOBHCC).
Okeyinmi Comprehensive Primary Health Care Center (OKCPHCC) was established in 2012 and is located in the Ado local government area. This center includes a consulting room, delivery room, recovery room, pharmacy, and health records department. The staff comprises one full-time doctor, three full-time nurses, two full-time midwives, and three Community Health Extension Workers (CHEWs). The facility is equipped with an improved water supply, electricity, vaccine freezers, and sanitation infrastructure. Services provided include antenatal care, deliveries, family planning, child health services, malaria treatment, maternal health services, measles immunization, emergency trans- port, and skilled birth attendance.
Odo-Ado Basic Health Care Center (OABHCC) is a public hospital located in Odo-Odo, Ado-Ekiti. Established on January 1, 1978, the facility operates 24 hours a day and is registered as a primary health centre (facility code 13/01/1/1/2/0016). It offers a wide range of specialized clinical services, including antenatal care, deliveries, immuni- zation, pediatric clinics, HIV/AIDS services, childhood disorder treatments, newborn development moni- toring, family planning, nutritional support, immunization, health education, and community mobilization. The center also has an onsite laboratory and pharmacy.
Oke-Oniyo Basic Health Care Center (OOBHCC) is a public hospital located in Ekute, Ado-Ekiti, and was established on January 1, 1984. The center operates around the clock and is registered under the Nigerian Ministry of Health as a primary healthcare facility (facility code 13/01/1/1/1/0012). Its services include antenatal care, family planning, delivery, ultrasound scanning, immunization, pediatric clinic, health education, and community mobili- zation.
These three health centers were selected for the study based on their functional status and central location within Ekiti State, making them accessible to both urban and rural residents.
2.3. Study Participants
The source population comprised women of child- bearing age (20 to 45 years), attending clinics across the various primary health centers in Ekiti state. Participants included mothers of children aged two years and below who were attending baby wellness clinics at the selected centers. The study unit included mothers randomly selected from the total mothers visiting the selected health centers. Mothers who did not provide consent were excluded from the study.
2.4. Study Variables
- Dependent variable: Morbidity profile of children under five.
- Independent variables: The personal and environmental hygiene practices of mothers, as well as household information that may influence these practices.
2.5. Data Collection and Measurement
Data were collected using a pre-tested, self-adminis- tered questionnaire consisting of 47 items. The question- naire, adapted from previous studies, was divided into four sections:
1. Section A: Socio-demographic information of the mothers.
2. Section B: Household information of the respondents.
3. Section C: Personal and environmental hygiene practices.
4. Section D: Morbidity profile of children under five.
To assess the validity of the instrument used, a copy of the questionnaire was reviewed by experts in the relevant field. Both face and content validity were considered to ensure that the instrument was aligned with the study's objectives. The questionnaire was evaluated for its relevance, coverage of the subject matter, and content appropriateness by the research supervisor and subject matter experts.
To ensure reliability, the test-retest method was employed. This involved administering the same question- naire to the same group of participants under similar conditions on two separate occasions. The group consisted of 10% of the total sample size (15 women with characteristics like the intended study participants), with a two-week interval between the tests. The pre-test assessed the consistency of the responses, and the reliability coefficient was calculated to measure internal consistency. A reliability coefficient of 0.8 was obtained, indicating the instrument to be highly reliable. After data collection, the questionnaires were thoroughly reviewed for completeness.
2.6. Bias Control
To minimize bias in participant selection, proportional sampling was used to determine the number of parti- cipants from each healthcare facility. A random sampling technique, based on a numbering system, was employed to ensure an unbiased selection of participants.
2.7. Study Size
The sample size was determined using Fisher’s formula:
 |
Where, n is the desired sample size, a is the standard normal deviation being usually 1.96, b is the prevalence being 11% or 0.11, c is equal to 1-b = 0.89, and d is the degree of freedom usually being 0.05.
 |
Thus, the desired sample size for the study was 151 participants.
Three hundred and twenty registered mothers were attending Okeyinmi Comprehensive Primary Health Care Center (OKCPHCC), 146 mothers were registered at Odo-Ado Basic Health Care Center (OABHCC), and 124 were registered at Oke-Oniyo Basic Health Care Center (OOBHCC) during the period of the study, totaling 590 mothers. From this sample frame, 151 respondents were recruited for the study.
A proportional sampling technique was adopted for the determination of the number of respondents for the survey from the sub-population (OKCPHCC, OABHCC, and OOBHCC), while random sampling was employed for the selection of participants from each sub-population. This is explained in Table S1.
2.8. Proportionate Allocation of Respondents based on Primary Health Centers
OKCPHCC (sample frame from hospital register = 320)
 |
OABHCC (sample frame from hospital register = 146)
 |
OOBHCC (sample frame from hospital register = 124)
 |
2.9. Quantitative Variables
Each section of the questionnaire was analyzed to estimate the frequency and percentage of each response. The hygiene index of mothers was determined on a scale of 0–1. This was estimated from all the hygiene para- meters (personal and environmental). The authors employed a scale of zero to unity to define the hygiene index [15]. The indices were calculated as a fraction. It was computed by finding the ratio of the highest hygiene level over 100 with 1 representing a perfect hygiene practice.
2.10. Statistical Methods
The data collected were first checked for errors, cleaned, and carefully entered into the analysis software to avoid missing data/cases. The analysis was conducted using IBM Statistical Package for Social Sciences (SPSS) version 21. Data results have been summarized and presented in descriptive statistics using tables, frequency, charts, and percentages. The relationship among the variables was tested via Chi-square analysis with a statistical significance level set to 0.05.
2.11. Ethical Consideration
Ethical clearance was obtained from the ethics and research committee of Afe Babalola University, Nigeria. Permission to conduct the study was obtained from the coordinators of primary health care centers, where the study was carried out. Informed consent was obtained from all participants. Participation was voluntary. The privacy and confidentiality of the respondents were strictly adhered to. Confidentiality was observed as the question- naire bore no name of the respondent or any identifying information. All methods were performed in accordance with Helsinki's relevant guidelines and regulations.
3. RESULTS
Out of a target population of 590, 151 mothers were proportionately recruited from three primary healthcare centers. Each participant was randomly selected from each primary healthcare facility.
3.1. Socio-demographic Characteristics
Table 1 shows the sociodemographic characteristics of respondents. The mean age of mothers was 32 ± 2.7 years. A higher percentage (49%) of the respondents had children aged 3-5 years, 38% had children aged 1-3 years, while about 12.5% had children less than 1 year old. Most (66.89%) of the respondents were married. Regarding the educational status of mothers, almost half (47.68%) of the respondents had secondary school education, 11.26% had tertiary education, and 25.83% had only primary education. The occupation status showed 23.54% of the participants to be civil servants, 3.31% to be housewives, 37.75% to be in business, 20.53% to be farmers, and 14.57% to be involved in the sale of crafts.
3.2. Household Information of Respondents
The household information of respondents is presented in Table 2. The majority of the participants (71.53%) used a closed drainage system. Concerning building type (place of residence of the respondents), 61.59% lived in bungalows, while 38.41% lived in “face-me-i-face-you” apartments (a low-cost house with multiple rooms facing each other rented out to individuals or multiple families with shared facilities), with none were living either in duplex or other living arrangements. The results showed 17.88% of the participants to obtain their drinking water from pipe water, 11.26% from open wells, 43.05% from borehole water, 27.81% from sachet water, and none from bottled water. 19.21% of the participants obtained water for food preparation from pipe water, 26.49% from open wells, 54.31% from borehole, and none from other sources, respectively. The water used for other household activities was obtained as follows: 22.52% obtained pipe water, 73.51% borehole water, 3.97% from rivers or streams, and none from other sources of water.
| Variable | Frequency (n=151) | Percentage (%) |
|---|---|---|
| Age of mother (years) | ||
| 20-29 years | 63 | 41.72% |
| 30-39 years | 41 | 27.15% |
| 40-50 years Mothers’ mean age |
47 32 years |
31.13% |
| Age of child (years) | ||
| < 1 year | 19 | 12.58 |
| 1-3 years | 58 | 38.41 |
| 3-5 years | 74 | 49.01 |
| Sex of child | ||
| Male | 92 | 60.93 |
| Female | 59 | 39.07 |
| Marital status of the mother | ||
| Single | 6 | 4.00 |
| Married | 122 | 80.79 |
| Divorced | 23 | 15.23 |
| Religion | ||
| Christianity | 97 | 64.25 |
| Islam | 43 | 28.49 |
| Traditional | 11 | 7.26 |
| Educational status | ||
| None | 10 | 6.62 |
| Primary | 39 | 25.83 |
| Secondary | 72 | 47.68 |
| Tertiary | 17 | 11.26 |
| Occupation | ||
| Civil servant | 36 | 23.84 |
| Housewife | 5 | 3.31 |
| Business/trading | 57 | 37.75 |
| Farming | 31 | 20.53 |
| Crafts | 22 | 14.57 |
| Variable |
Frequency (n=151) |
Percentage |
|---|---|---|
| Drainage facility available in respondents' homes | ||
| Open | 43 | 28.48% |
| Closed | 108 | 71.53% |
| Housing type in which respondents live | ||
| Bungalow | 93 | 61.59% |
| “Face-me-i-face-you” | 58 | 38.41% |
| Duplex | - | - |
| Household source of drinking water | ||
| Piped water | 27 | 17.88% |
| Open well | 17 | 11.26% |
| Borehole | 65 | 43.05% |
| Bottled water | - | - |
| Sachet water | 42 | 27.81% |
| Household source of water for cooking | ||
| Piped water | 29 | 19.21% |
| Open well | 40 | 26.49% |
| Borehole | 82 | 54.31% |
| Source of water for other household activities | ||
| Piped water | 34 | 22.52% |
| Borehole | 111 | 73.51% |
| River/stream | 6 | 3.97% |
3.3. Personal Hygiene Practices of Mothers
Regarding the personal hygiene practices of mothers, 60.27% responded that they always washed their hands with soap and water before feeding their children, while 32.45%, 6.62%, and 0.66% washed their hands occasionally, rarely, and never washed their hands, respectively, before feeding their children. The majority (60.93%) of the respondents showed that they occasionally washed their hands after using the toilet. Similarly, 64.90%, 32.45%, and 2.65% always, occasionally, and rarely cleaned their cooking and feeding utensils before and after use, respectively (Table 3). Table 4 further revealed some personal hygiene practices of mothers in this study. The table reveals that all of the participants took bath daily, 20.52% once daily, and 78.15% twice daily, while it varied for 1.33% of the participants. 93.38% reported to wash their hands before breastfeeding their children, while 6.62% did not, and of those who reported to wash their hands before breastfeeding, 94.70% reported to do this occasionally, while 5.29% of the participants reported to do it rarely. With respect to how often the participants washed their bra, 19.21% said that they wash it daily, 78.81% reported that they wash their bra weekly, while 31.99% reported to wash it monthly.
3.4. Environmental Hygiene Practices of Mothers
Regarding the environmental hygiene practices of mothers (Table 5), 71.52% of the respondents reported to clean their surroundings daily, while 21.19% and 1.99% reported to clean their surroundings weekly and monthly, respectively. With regards to clearing the bushes or grasses around the house, 2.65% of the participants reported to not clear bushes or grasses, 5.96% of the respondents reported to clear them daily, 58.94% weekly, 24.50% monthly, and 7.95% any time the bush or grass around their surrounding are ground. 15.23% of the respondents stated that they have stagnant water around their houses, while 84.77% of the respondents stated an absence of stagnant water around their houses. Finally, the frequency of opening the windows was considered and 30.46% of the participants stated that they keep their windows open always, 62.92% reported that they often open their windows, while 6.62% of the participants reported to rarely open their windows, respectively.
| S. No. | Item | Always | Occasionally | Rarely | Never |
|---|---|---|---|---|---|
| 1 | How often do you wash your hands with soap and water before feeding your child? | 60.27% | 32.45 | 6.62% | 0.66% |
| 2 | How often do you wash your hands with soap and water before and after using the toilet? | 31.78% | 60.93% | 7.29% | -(-) |
| 3 | How often do you clean cooking and feeding utensils before and after use? | 98(64.90%) | 49(32.45%) | 4(2.65%) | -(-) |
| 4 | How often do you take your bath with soap and water? | 99.34% | 0.66% | -(-) | -(-) |
| Variable | Frequency (n=151) | Percentage |
|---|---|---|
| How many times do you take your bath a day? | ||
| None | - | - |
| Once | 31 | 20.52% |
| Twice | 118 | 78.15% |
| Others | 2 | 1.33% |
| How many times do you wash your bra? | ||
| Daily | 29 | 19.21% |
| Weekly | 119 | 78.81% |
| Monthly | 3 | 1.99% |
| Variable | Frequency (n=151) | Percentage |
|---|---|---|
| Where is your place of food preparation? | ||
| Indoor | 88 | 58.29% |
| Outdoor | 63 | 41.72% |
| Others (specify) | - | - |
| How often do you clean your surroundings? | ||
| Daily | 108 | 71.52% |
| Weekly | 32 | 21.19% |
| Monthly | 3 | 1.99% |
| Never | - | - |
| Others (specify) (regularly) | 8 | 5.30% |
| How often do you sweep your house? | ||
| Never | - | - |
| Daily | 150 | 99.34% |
| Weekly | 1 | 0.66% |
| Monthly | - | - |
| Others (specify) | - | - |
| How often do you mop your house? | ||
| Never | - | - |
| Daily | 56 | 37.09% |
| Weekly | 94 | 62.25% |
| Monthly | 1 | 0.66% |
| Others (specify) | - | - |
| How often do you clear bushes or grass around your house? | ||
| None | 4 | 2.65% |
| Daily | 9 | 5.96% |
| Weekly | 89 | 58.94 |
| Monthly | 37 | 24.50% |
| Others (specify) (any time it is grown) | 12 | 7.95% |
| Do you have stagnant water around your house? | ||
| Yes | 23 | 15.23% |
| No | 128 | 84.77% |
| How often do you open your windows for ventilation? | ||
| Always | 46 | 30.46% |
| Often | 95 | 62.92% |
| Rarely | 10 | 6.62% |
| Never | - | - |
The waste disposal methods practiced by respondents are shown in Fig. (1). 35.76% of the participants reported to dispose waste in the dustbin, 7.95% stated that they burn their waste, 12.58% disposed their waste by throwing it into the bush, 1.32% buried their waste in the ground, 24.51% disposed it along the roadside, and 17.88% of the participants disposed their waste at the general refuse dump. Information regarding the toilet facilities used by respondents is shown in Fig. (2) where the majority reported to use a water closet (the modern toilet), although very few participants used the pit latrine and very few did not have a toilet at all.
Table 6 shows the morbidity profile/status of under-five children as reported by their mothers. 22.5% had suffered a cold in the past 1 month and the majority (94.7%) claimed that their child did not have diarrhea episodes in the past 1 month.
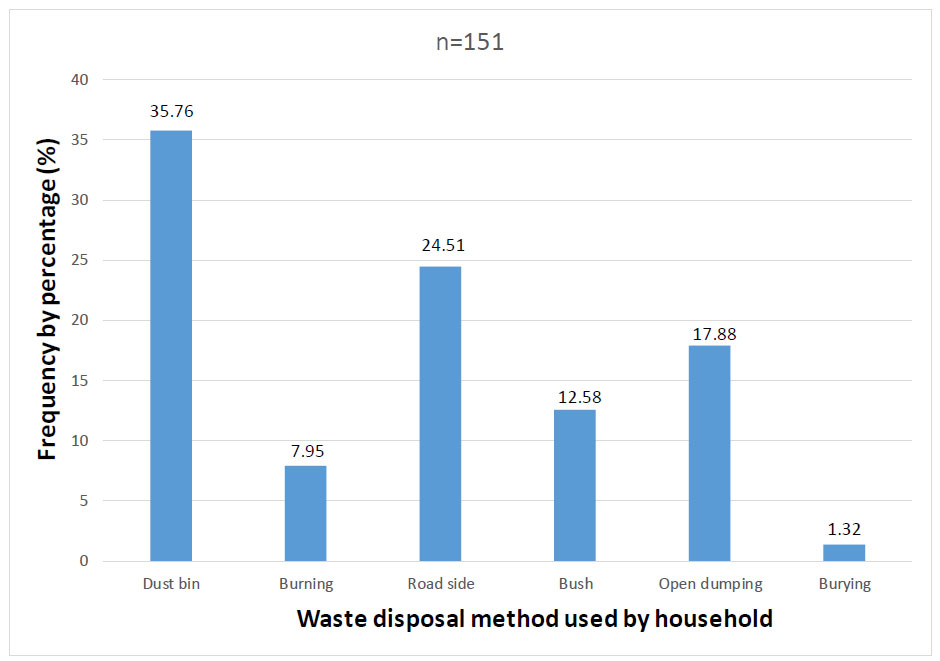
Household method of waste disposal.
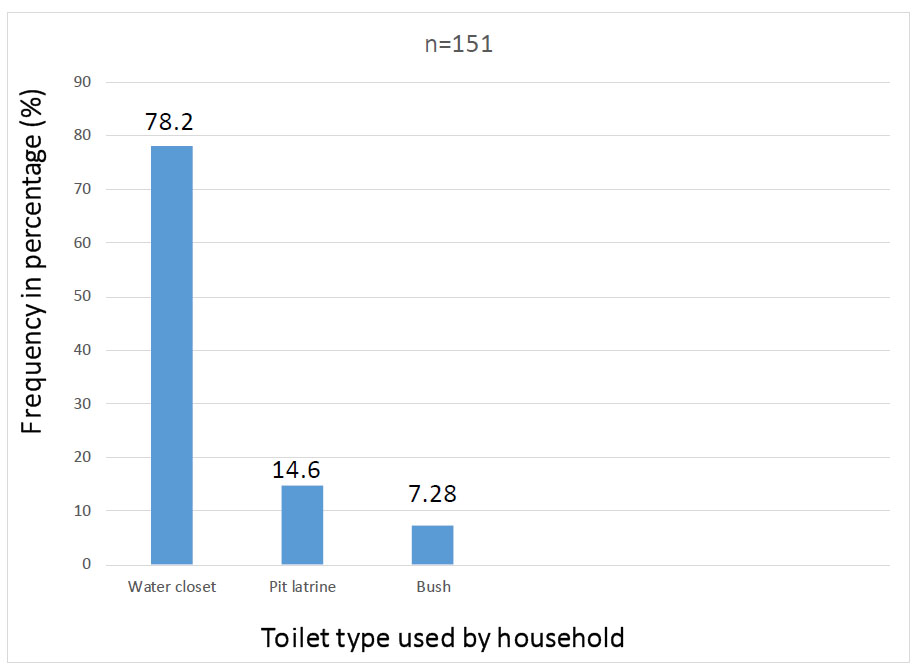
Toilet facility used by household.
3.5. Hygiene Index of Mothers
On a scale of 0 to unity, the study has determined the level of hygiene of mothers selected for the study using all the hygiene parameters (personal and environmental) employed for this study. The highest hygiene level for each parameter was converted to a fraction and is presented in Table 7. An average index value of 0.5428 was obtained for the hygiene parameters.
Table 8 shows the overall hygienic practices categories. We classified respondents with a score of 75% or more as having “good” practices, and otherwise “poor” practices. This estimate suggests that 39.46% of the respondents had good personal and environmental hygiene practices, while 60.54% had poor hygiene practices.
| Variable | Frequency (n=151) | Percentage | |
|---|---|---|---|
| 1. Has your child suffered from a cough or cold in the past 1 month? | |||
| Yes | 34 | 22.52% | |
| No | 117 | 77.48% | |
| 2. Has your child had diarrhea in the past 1 month? | |||
| Yes | 8 | 5.30% | |
| No | 143 | 94.70% | |
| 2. Has your child been admitted to the hospital in the past 1 month? | |||
| Yes | 13 | 8.61% | |
| No | 138 | 91.39% | |
| 6. If yes, what was the diagnosis? | |||
| Specify | Pyrexia of unknown origin | ||
| Hygiene Index | Value |
|---|---|
| Hand washing | 0.6027 |
| Hand washing with soap and water | 0.3178 |
| Cleaning of cooking utensils | 0.6490 |
| Bathing with soap and water | 0.9934 |
| Twice-daily bathing | 0.7815 |
| Daily washing of bra | 0.1921 |
| Drainage facility | 0.7153 |
| Household source of drinking water | 0.2781 |
| Household source of water for cooking | 0.5431 |
| Source of water for other household activities | 0.2252 |
| Place of food preparation | 0.5829 |
| Frequency of cleaning the surrounding | 0.7152 |
| Frequency of sweeping the house | 0.9934 |
| Frequency of mopping the house | 0.3709 |
| Frequency of bush clearing | 0.0596 |
| Presence of stagnant water around the house | 0.8477 |
| Frequency of window opening for ventilation | 0.3046 |
| Waste disposal | 0.3600 |
| Toilet facility | 0.7800 |
| Average hygiene index | 0.5428 |
| Hygiene practice | Frequency | Percentage (%) |
|---|---|---|
| Poor hygiene practices | 91 | 60.54% |
| Good hygiene practices | 60 | 39.46% |
| Total | 151 | 100% |
| Variables | Morbidity (+ve diarrhea Hx) n(%) | Morbidity (-ve diarrhea Hx) n(%) | x2 | df | p-value |
|---|---|---|---|---|---|
| Drainage facility | |||||
| Open | 6 (14.0) | 37 (86.0) | 8.977 | 1 | 0.003* |
| Closed | 2 (1.85) | 106 (98.15) | |||
| Housing type | |||||
| Bungalow | 2 (2.15) | 91 (97.85) | 4.781 | 1 | 0.029* |
| “Face-me-I-face-you” | 6 (10.34) | 52 (89.66) | |||
| Household source of drinking water | |||||
| Piped water | 1 (3.70) | 26 (96.30) | 5.967 | 3 | 0.113 |
| Open well | 3 (17.65) | 14 (82.35) | |||
| Borehole | 2 (3.08) | 63 (96.92) | |||
| Sachet water | 2 (4.76) | 40 (95.24) | |||
| Household source of cooking water | |||||
| Piped water | 1 (3.45) | 28 (96.55) | 2.400 | 2 | 0.301 |
| Open well | 4 (10.00) | 36 (90.00) | |||
| Borehole | 3 (3.66) | 79 (96.34) | |||
| Source of water for household activities | |||||
| Piped water | 1 (2.94) | 33 (97.06) | 29.089 | 2 | 0.000* |
| Borehole | 3 (2.70) | 108 (97.30) | |||
| River/stream | 3 (50.00) | 3 (50.00) | |||
| Personal and environmental hygiene | |||||
| Good hygiene practices | 0 (0.00) | 60 (100.00) | 5.570 | 1 | 0.018* |
| Poor hygiene practices | 8 (8.80) | 83 (91.20) | - | - | - |
| Frequency of cleaning surroundings | |||||
| Daily | 2 (1.85) | 106 (98.15) | 15.679 | 2 | 0.000* |
| Weekly | 3 (9.38) | 29 (90.63) | |||
| Occasionally | 3 (12.50) | 7 (87.50) | |||
Table 9 presents the relationship among hygienic practices, housing characteristics, and morbidity profile, which has revealed “Face-me-I-face-you” housing, poor hygiene, and occasional cleaning practices, leading to significantly higher diarrhea morbidity. Additionally, households using rivers/streams for water had the highest morbidity (50%) (p < 0.05).
4. DISCUSSION
4.1. Personal Hygiene Practices of Mothers
The knowledge of personal and environmental hygiene plays a crucial role in reducing the incidence of diarrhea among children under five, particularly when mothers are aware of its importance. When mothers understand how infections are transmitted to their children, causing gastrointestinal issues, they are likely to take additional precautions regarding personal and environmental hygiene. More than half of the respondents (60.27%) reported consistently washing their hands with soap and water before and after feeding their children. While this is a positive proportion, it is concerning that over one-third of the participants (39.73%) did not adhere to this safe hygiene practice before feeding. This finding contrasts with the study by Nizame et al. [16], which reported that only 18% of respondents washed their hands prior to preparing their children's meals, and 15% of participants associated diarrhea with poor hygiene. Similarly, Oloruntoba et al. [3] noted a higher risk of diarrhea in children whose mothers did not wash their hands with soap before meal preparation (OR = 3.0, p < 0.05).
If mothers of children under five become more aware of the dangers of poor hygiene, they may develop a heightened aversion to dirt and a strong commitment to cleanliness, thus preventing diarrhea. Vivas et al. [17] also reported that hand washing is highly effective in removing contaminants that can lead to illness. The perceived value of cleanliness, they added, is often shaped by the background of those practicing hand hygiene.
It is worth noting that only 31.78% of respondents consistently washed their hands with soap and water after using the toilet, while a larger proportion (60.93%) did so only occasionally. This is a risky behavior, highlighting the need for targeted interventions. In contrast, Rafath and Bhavani [18] found that 79.3% of respondents washed their hands with soap and water after using the toilet, and only 17.3% cited the lack of a washing facility as a reason for not doing so. Such poor hygiene practices can promote the spread of microorganisms, increasing the risk of infections in children. Public health practitioners must emphasize the importance of good hygiene practices among mothers to reduce the incidence of diarrhea in children under five [17]. Gupta et al. [19] similarly stressed that hand washing with soap is key to reducing diarrhea rates among young children.
A majority of respondents (78.15%) reported bathing twice daily. Although there are no specific guidelines on how often a mother should bathe, cleanliness and avoiding dirt or foul odors can serve as indicators. Gander [20] observed that Australians are known for their cleanliness, with 90% of women bathing daily. However, many women in the United Kingdom skip daily bathing due to fatigue, with one in three going up to three days without a bath, despite 57% recognizing the importance of hygiene [20].
Additionally, 78.81% of respondents reported washing their bras weekly, a practice that could harbor micro- organisms and pose a threat to children's health. While mothers may wash their hands before breastfeeding, an unclean bra could still expose the child to harmful bacteria. Urbaniak et al. [21] suggested that micro- organisms from the breast surface could enter the mammary ducts, potentially causing gastrointestinal issues in breastfed children.
4.2. Environmental Hygiene Practices
Maintaining environmental hygiene should be a collective effort within the community, not solely the responsibility of women. However, traditional gender roles often place the burden of environmental care on women. In this study, 71.52% of respondents cleaned their surroun- dings daily, and 35.76% used dustbins for waste disposal. These findings align with those of Duru et al. [22], who reported low environmental sanitation practices, with 20.8% of semi-urban communities in Orlu, Nigeria, managing solid waste effectively. Moreover, some respondents in this study reported using open dumping and roadside dumping for waste disposal, which Duru et al. [22] also found in their study, where 65.3% of respondents noted the lack of designated waste collection points.
Further, 87% of Nigerians have reported using unsanitary waste disposal methods [23]. A majority of respondents (78.15%) in this study reported using water closets, which aligns with the study performed by Ekong [24], who found 83.8% of respondents to use water cisterns and 63.8% to cover their toilets. Proper toilet coverage prevents flies from spreading contaminants, reducing the risk of diarrhea in young children. Using water closets also ensures sanitary conditions in the household, thereby lowering the likelihood of diarrheal disease.
It is concerning that many respondents reported to still engage in open dumping of waste. In the 21st century, such unhygienic practices could lead to outbreaks of infection. Effective waste management is essential for safeguarding the health of individuals, families, and the wider community [11]. The reliance on groundwater, as revealed in this study, could also pose radiological health risks due to exposure to radon and other natural radionuclides [25, 26]. Furthermore, Esan et al. [27] opined in their study that educational programs should be designed and implemented to increase awareness of disease prevention among the female population. Also, the bivariate analysis outcome has revealed poor housing, poor hygiene, and infrequent cleaning practices to be related to a higher incidence of diarrhea, suggesting the need to control these factors being crucial in reducing diarrhea morbidity in the studied population. Hence, there is a need to implement public health intervention programs to tackle some of the socio-economic, demographic, and environmental indicators that are attributed to public health disorders and consequently the spread of diarrheal diseases, especially among vulnerable populations and internally displaced people [28]. Finally, the role of Exclusive Breastfeeding (EBF) practices in reducing the episodes of diarrhea and other diarrheal-related diseases among under-five children cannot be overemphasized. Several studies [29, 30] have opined that EBF boosts an infant’s immune response to infectious pathogens and reduces mortality among this age group by providing the necessary immunoglobulins, co-factors, and nutrients, essential for optimal growth and development. Hence, nursing mothers should be adequately informed by healthcare providers on the benefits of EBF practice.
4.3. Strengths, Limitations, and Generalizability
This descriptive quantitative study was conducted in three local government facilities in Ekiti State, Nigeria. The findings may not represent hygiene practices among mothers in other parts of the country or globally. While the study has addressed a significant gap in the literature, caution is advised when generalizing these findings.
CONCLUSION
This study has assessed personal and environmental hygiene practices among mothers of children under five in Ekiti State, Nigeria. The results have revealed poor hand hygiene in several instances, particularly after using the toilet and before feeding children. Although other hygiene practices have been satisfactory, there have been concerns about the infrequent washing of bras, which could expose children to infections. Additionally, waste disposal practices, such as open dumping and burning waste, have been prevalent among the respondents. Overall, the hygiene level among mothers in the study area has been low, with an average index value of 0.5428. These findings highlight the need for targeted public health interventions aimed at improving hygiene practices among mothers.
Implications for Practice
Government, public health experts, and other stakeholders should plan interventions to empower mothers with knowledge and resources in order to ensure personal and environmental hygiene, thereby preventing disease outbreaks among children under five.
The small sample size used in this study may limit the generalization of findings to other regions in Southwest Nigeria, and this limitation should be acknowledged.
AUTHORS’ CONTRIBUTION
D.T.E. and I.D.O.: Designed the study; D.T.E and J.M.: Conducted the research; J.M., I.D.O, E.O.A, D.T.O, and D.T.E: Performed the literature review; E.O.A, A.A.S, Y.A., and O.A: Analyzed and interpreted the data. D.T.E, I.D.O, E.O.A, and A.A.S.: Drafted the manuscript; Y.A., A.A.S, and C.G.R.: Revised it; D.T.E., D.T.O., and C.G.R.: Ensured that the manuscript met journal specifications.
LIST OF ABBREVIATIONS
| LGAs | = Local Government Areas |
| OABHCC | = Odo-Ado Basic Health Care Center |
| OKCPHCC | = Okeyinmi Comprehensive Primary Health Care Center |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical clearance was obtained from the ethics and research committee of Afe Babalola University, Ado-Ekiti, Nigeria.
HUMAN AND ANIMAL RIGHTS
All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.

