All published articles of this journal are available on ScienceDirect.

Musculoskeletal Discomfort and Musculoskeletal Injuries in Firefighters of the City of Cape Town Fire and Rescue Service
Abstract
Objective
The prevalence of work-related musculoskeletal injuries is reported to be noticeably high amongst firefighters, which augments the dangers of the job and the difficulties that firefighters must face daily. Therefore, this study aimed to firstly determine the prevalence and characteristics of work-related musculoskeletal injuries (MSIs) and musculoskeletal discomfort (MSD) and, secondly, to determine the relationship between MSD and MSIs in firefighters.
Methods
Using random systematic sampling, 309 firefighters from the City of Cape Town Fire and Rescue Service were recruited to participate. A researcher-generated questionnaire was used to retrieve data on musculoskeletal injuries and musculoskeletal discomfort. Data was analysed using the T-tests, Cochran-Armitage trend test, Jonckheere-Terpstra test, and Binary logistic regression. A p-value of less than 0.05 was used to indicate statistical significance.
Results
Male (p = 0.036) and older firefighters (p<0.001) with more years of experience (p = 0.002) were most likely to report a musculoskeletal injury. Falls, jumps, slips, and trips were the most common injuries (39.7%), which most often occurred on the fireground (41.1%). Most firefighters (73.3%) reported experiencing discomfort 1-2 times a week of moderate (60.1%) severity that interfered slightly with their ability to work (58.2%). Multivariable analysis showed that the age groups of 40-49 years and 50-65 years and the rank of station commander increased the risk for MSIs by a factor of 2.39, 2.67, and 3.83, respectively. In addition, MSD was associated with an increase in the likelihood of firefighters reporting MSIs (p <0.001).
Conclusion
Older male firefighters with more years in service were most likely to experience MSIs. Regular physical activity and work-related training should be implemented to increase the fitness for duty and to reduce the prevalence of injuries in firefighters.
1. INTRODUCTION
Firefighting is considered to be one of the most physically demanding professions globally [1]. Besides extinguishing and controlling fires, firefighters have additional responsibilities, such as providing emergency resuscitation, civil rescue, etc. Moreover, they are routinely exposed to hazardous chemicals and fumes while also experiencing tremendous strain in their daily work activities, which may contribute to the high prevalence of musculoskeletal injuries (MSIs) [2, 3]. These extreme conditions highlight the need for pre-habilitative and rehabilitative interventions to reduce the prevalence of injuries among firefighters on duty [4-6].
It has been noted that older firefighters have a high likelihood of sustaining MSIs, which has been linked to ageing and the general attrition to the musculoskeletal system due to the “wear and tear” associated with firefighting [5-7]. In addition, the ranks and duties of firefighters were also found to be linked to MSIs [5, 6, 8]. Moreover, it has been shown that females are particularly susceptible to sustaining MSIs [4], with a large portion of this attributed to ill-fitting equipment [9]. Although extensive personal protective equipment (PPE) is used by firefighters, they remain at high-risk for sustaining MSIs that could be minimised or avoided with the assistance of updated and specialised PPE [9-13]. Firefighters have been reported to have restricted mobility in different regions of the body due to their PPE [4, 10]. Chinese firefighters, similarly, reported increased lower body restrictiveness, leading to an increase in injuries sustained in the ankles, legs, and lower back [10]. Firefighters in the US reported more upper body discomfort and, subsequently, more upper body injuries [10]. Hence, firefighters in different regions and countries sustained different types of injuries in different anatomical locations. Previous studies have consistently reported that the commonly injured body regions are the lower back, shoulder, and ankle [4, 6, 7, 14], likely due to these areas being most susceptible to overuse and repetition [6] and PPE-related restrictions [9, 11]. Similarly to MSIs, musculoskeletal discomfort (MSD) has been noted to be a frequent issue in firefighters, where firefighters often report pain and discomfort in the back and lower limb regions of their body [15-17]. Moreover, firefighters have also reported that these symptoms of discomfort limit their physical output and work-related output [15, 17].
Common predisposing factors that increase the risk of injury and discomfort include static postures, repetitive movements, and over-exertion [1, 2]. The leading types of injuries sustained by firefighters include musculoskeletal sprains and strains sustained during falls, trips, and carrying heavy equipment [4, 6, 7]. When undue strain is placed on tendons and muscles, they are pushed beyond their ability to cope, and musculoskeletal injuries may arise [1]. In less severe cases, these may manifest as moderate to severe discomfort, predisposing firefighters to more severe injuries if these symptoms are not treated [15, 16]. Injuries have been found to be a cause of abrupt movements and overloaded systems [2, 13, 18]. Therefore, the purpose of the study was to, firstly, determine the prevalence and characteristics of work-related musculoskeletal injuries and musculoskeletal discomfort and, secondly, to determine the association between MSD and MSIs in firefighters of the City of Cape Town Fire and Rescue Service and their demographic factors.
2. METHODS
2.1. Study Design and Population
This was a descriptive, quantitative and cross-sectional study design. A total of 309 full-time firefighters, males and females, aged between 20 and 65 years, were recruited using random systematic sampling from the City of Cape Town Fire and Rescue Service (CoCFFRS). For musculoskeletal injuries, one firefighter did not complete the injuries questionnaire and was removed from the analysis (n = 308). The CoCTFRS employs approximately 1000 full-time firefighters, and using the finite population sample size calculation, a minimum sample size of 278 is needed to ensure the precision and statistical power of the results. Firefighters who were on administrative duty and sick leave at the time of the study and those employed part-time or on a seasonal basis were excluded from participation in this study. Written informed consent was obtained from each participant prior to participating in the study. Using a researcher-generated questionnaire, the sociodemographic characteristics of the firefighters were collected, including age, sex, and injury history. In addition, the questionnaire retrieved data on firefighters’ lifestyle information, including cigarette smoking status and physical activity levels. The previously validated Nordic Musculoskeletal Disorders questionnaire was evaluated as appropriate (α > 0.9) to collect data on the anatomical locations of musculoskeletal injuries and the characteristics and mechanisms of injury [19]. The Cornell Musculoskeletal Discomfort Questionnaire was used to retrieve information on MSD in firefighters. The questionnaire has been validated and found to be a reliable tool for research purposes [20]. The questionnaire was self-administered, under the guidance of a researcher, to ensure accuracy and took approximately 25 minutes to complete.
2.2. Ethical Considerations
Participation in the study was voluntary, and all subjects gave their informed consent before participating in the study. The study protocol was approved by the Humanities and Social Sciences Research Ethics Committee (HSSREC) (Ethics number: HS22/4/34) at the University of the Western Cape. Permission to conduct the study was obtained from the chief fire officer and the district manager of the City of Cape Town Fire and Rescue Service.
2.3. Questionnaire Scoring/Design
The Nordic Musculoskeletal Disorders questionnaire comprised 11 questions, divided into three sections and nine categories. This was answered by indicating a yes or no response to the nine anatomical sites to indicate if a participant did or did not experience injury/trouble to one or more regions during their time as a firefighter. The anatomical locations included the neck, shoulders, elbows, wrist/hand, upper back, lower back, hips/thighs, knees, and ankles/feet. If a participant did not answer yes to having discomfort or pain in a specific region/body location, there was no need to answer the follow-up questions. If yes was ticked, then a participant had to answer the following questions, specifically, the time of initial onset of the condition, the participant’s age at onset, whether hospitalised because of the condition, whether reassigned jobs or duties (even temporarily, because of the condition), whether symptoms (ache, pain, discomfort) were experienced at any time during the last 12 months or at any time during the last month (4 weeks) or at any time on the day, and whether a participant was prevented from doing their normal work (at home or away from home) at any time during the last 12 months. In addition, information was retrieved on the mechanism of injury, type of injury, and type of duty performed that incited the injury. For the Cornell Musculoskeletal Discomfort Questionnaire, the sections were divided into the following body regions: neck, shoulder, upper back, upper arm, lower back, forearm and elbow, wrist and hand, hip, thigh, knee, lower leg and foot and ankle. The questionnaire inquired on the frequency that firefighters experienced aches, pain, and discomfort and how often, categorised into the categories of never, 1-2 times last week, 3-4 times last week, once every day and several times a day. Next, the severity of the discomfort was inquired on, categorized as slightly uncomfortable, moderately uncomfortable, and very uncomfortable. Lastly, the questionnaire inquired on the interference of the discomfort on the ability to work and categorized as not at all, slightly interfered, and substantially interfered. The questionnaire encompassed a section on physical activity based on the International Physical Activity Questionnaire (IPAQ) [21], where total weekly physical activity was converted to weekly metabolic equivalent (MET) minutes using the recommended calculations.
3. DESCRIPTIVE MEASURES
3.1. Height, Weight, and BMI
When measuring stature, firefighters were asked to stand barefoot on the level stadiometer base, with the heels together and the heels, buttocks and upper back touching the stadiometer rod of a portable stadiometer (Seca model 700, Gmbh & Co., Germany). Weight was measured using the Tanita© (Tanita©, Tokyo, Japan) BC-1000 Plus bioelectrical impedance (BIA) analyser. When taking body mass, firefighters were requested to wear minimal clothing and to stand barefoot, upright, with feet apart. Obesity was classified as a body mass index (BMI) of ≥30 kg•m-2.
3.2. Statistical Analysis
All data were captured by double-entry into a Microsoft Office Excel spreadsheet and then cleaned of errors. Following this, the data were exported to the Statistical Package for the Social Sciences (SPSS) version 28 for descriptive and inferential data analysis. The data were separated into injury prevalence, injury location, injury mechanism, injury type, and injury anatomical location. Descriptive analysis was used to indicate the prevalence of MSIs and MSD, specifically, the mechanism, type, location and duty performed while sustaining the injury, and the location of discomfort and severity of discomfort. The Cochran-Armitage trend test and the Jonckheere-Terpstra test were used to determine the association between MSI and MSD prevalence among firefighters according to demographic characteristics. T-tests were performed to determine if statistical differences existed between MSIs and MSD according to age and years of experience. Univariable and multivariable logistic regressions were used to determine the association between MSIs (0, 1) and MSD (0, 1) according to sex (1, 2), age group (1, 2, 3, 4), rank (1, 2, 3, 4, 5, 6), and years of experience (1, 2, 3, 4). All covariates adjusted for were evidence-based and reported in previous literature to be significantly associated with MSIs and MSD in firefighters. In order to ensure that there was no collinearity present, a VIF of less than 0.5 was used. Secondly, independent variables with a correlation >0.6 were not included in the same model to remove the possibility of autocorrelation. In the multivariable analysis, age and years were separated to reduce collinearity in the covariates. Therefore, two models were used, i.e., in model 2, variables adjusted for included age (continuous), sex (categorical), body mass index (continuous), and weekly MET minutes (continuous) and in model 3, variables adjusted for included years of experience (continuous), sex (categorical), body mass index (continuous), and weekly MET minutes (continuous). A p-value of less than 0.05 was used to indicate statistical significance.
4. RESULTS
Table 1 describes the prevalence of injuries sustained by firefighters according to sociodemographic characteristics. The majority of firefighters were male (88.7%) and 10.9% were female (Table 1). Female firefighters were more likely to report an MSI compared to male firefighters (p = 0.036). Based on age, younger firefighters were most likely not to have an injury (73% reported no injuries), and firefighters older than 30 years were more likely to report having sustained an injury, which was highest in the 50-65 years age group (p <0.001). The more experienced firefighters, especially those with 11 or more years of experience, were more likely to report a musculoskeletal injury and were the highest in the group with over 31 years of experience (p = 0.002). Obese firefighters were more likely to report an MSI. Based on musculoskeletal discomfort, females were more likely to experience MSD. In addition, non-obese firefighters were more likely to experience MSD.
Table 1.
| Parameters | Not Injured | Injured | P-value | No Discomfort | Discomfort | - |
|---|---|---|---|---|---|---|
| N (%) | 178 (57.9) | 130 (42.1) | - | 179 (55.6) | 130 (40.4) | - |
| Sex ¶ | - | - | - | - | - | - |
| Male | 110 (40.0) | 165 (60.0) | <0.001** | 163 (59.3) | 112 (40.7) | 0.174 |
| Female | 13 (41.2) | 20 (58.8) | 16 (47.1) | 18 (52.9) | ||
| Age group † | - | - | - | - | - | - |
| 20-29 years | 19 (73.6) | 19 (26.4) | <0.001** | 45 (62.5) | 27 (37.5) | 0.324 |
| 30-39 years | 57 (59.4) | 30 (40.6) | 57 (59.4) | 39 (40.6) | ||
| 40-49 years | 42 (50.6) | 41 (49.4) | 44 (53.0) | 39 (47.0) | ||
| 50-65 years | 27 (46.6) | 31 (53.4) | 33 (56.9) | 25 (43.1) | ||
| Experience † | - | - | - | - | - | |
| 0-10 years | 80 (67.2) | 39 (32.8) | 0.002** | 73 (61.3) | 46 (38.7) | 0.372 |
| 11-20 years | 57 (57.6) | 42 (42.4) | 56 (56.6) | 43 (43.4) | ||
| 21-30 years | 29 (48.3) | 31 (51.7) | 32 (53.3) | 28 (46.7) | ||
| ≥31 | 13 (41.9) | 18 (58.1) | 18 (58.1) | 13 (41.9) | ||
| Current rank † | - | - | - | - | - | - |
| Junior firefighter | 45 (70.3) | 19 (29.7) | <0.001** | 38 (59.4) | 26 (40.6) | 0.581 |
| Firefighter | 96 (59.6) | 65 (40.4) | 95 (59.0) | 66 (41.0) | ||
| Senior firefighter | 17 (51.5) | 16 (48.5) | 18 (54.5) | 15 (45.5) | ||
| Platoon commander | 9 (56.3) | 7 (43.8) | 9 (56.3) | 7 (43.8) | ||
| Station commander | 8 (28.6) | 20 (71.4) | 13 (46.4) | 15 (53.6) | ||
| Divisional commander | 3 (50.0) | 3 (50.0) | 5 (83.3) | 1 (16.7) | ||
| Marital status † | - | - | - | - | - | - |
| Single | 81 (66.4) | 41 (33.6) | 0.014* | 80 (65.6) | 42 (34.4) | 0.027* |
| Married | 86 (53.1) | 76 (46.9) | 86 (53.1) | 76 (46.9) | ||
| Divorced | 11 (47.8) | 12 (52.2) | 11 (47.8) | 12 (52.2) | ||
| Education † | - | - | - | - | - | - |
| Matric | 129 (57.1) | 97 (42.9) | - | 127 (56.2) | 99 (43.8) | - |
| Diploma | 27 (61.4) | 17 (38.6) | 0.625 | 23 (52.3) | 21 (47.7) | 0.173 |
| Certificate | 12 (54.5) | 10 (45.5) | - | 15 (68.2) | 7 (31.8) | - |
| Degree | 11 (64.7) | 6 (35.6) | - | 14 (82.4) | 3 (17.6) | - |
* Indicates statistical significance <0.05.
** indicates statistical significance <0.01.
Fig. (1) shows the mechanism of injuries and the job duty/site that was the cause of injuries. Falls, jumps, slips, or trips were the most common injuries, accounting for 39.7% of injuries, followed by carrying or using heavy equipment with 11.9% and contact with an object with 7.8% (Fig. 1A). In addition, most injuries were sustained on the fireground, i.e., 41.1%, followed by the fire station, i.e., 21.3%, an active call-out, i.e., 19.3%, and during training, i.e., 18.3% (Fig. 1B). Sprains and strains were the most common type of injuries sustained by firefighters (68.4%) (Fig. 1C). Nearly half (49.4%) of all falls, jumps, slips or trip injuries occurred on the fireground, and 42.3% of injuries related to carrying or using heaving equipment also occurred on the fireground (supplementary table).
Fig. (2) shows the musculoskeletal discomfort of firefighters. Most (73.3%) firefighters reported experiencing discomfort 1-2 times a week, followed by several times a day with 13.1%. Based on severity, most (60.1%) firefighters reported moderate severity, followed by slight discomfort (37.0%). Based on the discomfort interfering with their ability to work, 58.2% of firefighters reported slight interference.

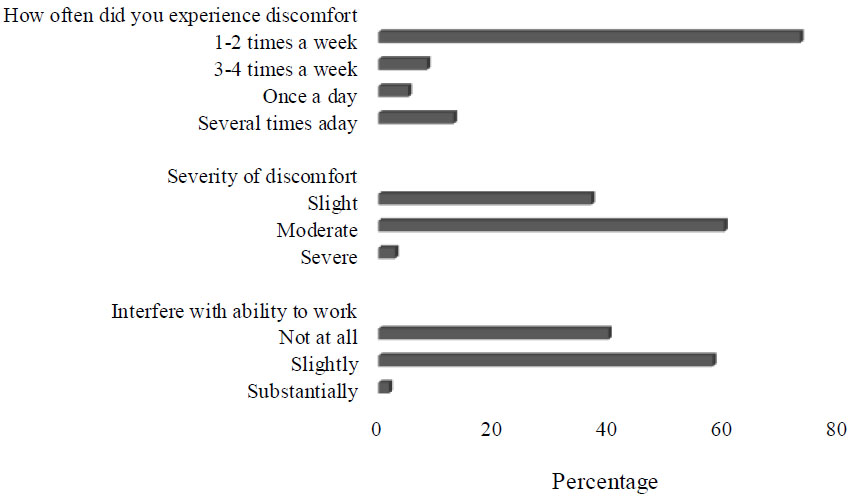
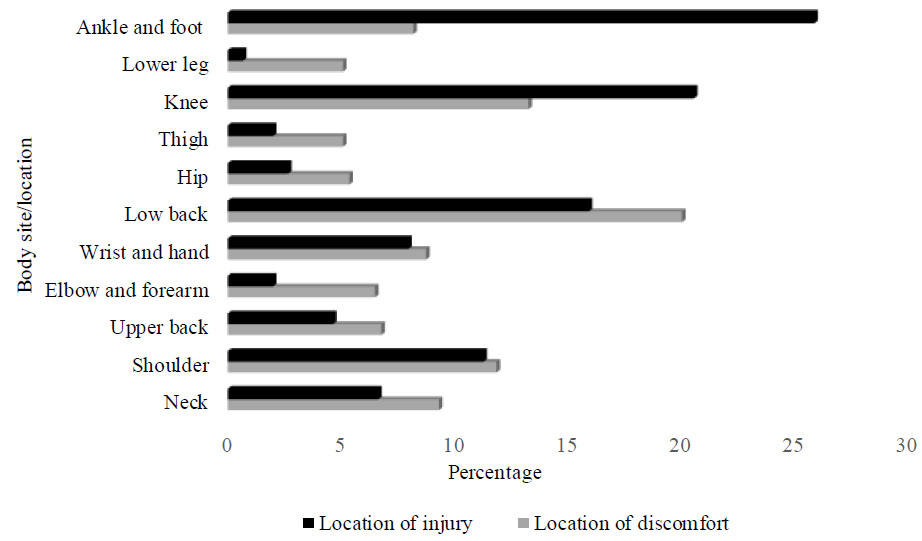
Fig. (3) shows the prevalence of musculoskeletal injuries and musculoskeletal discomfort according to the injury locations in firefighters. The ankle and foot regions were the most common injured sites (25.8%), followed by the knee (20.5%) and lower back region (15.9%). Based on MSD, the firefighters experienced the most discomfort in the lower back (20.0%), followed by the knee (13.2%) and shoulder (11.8%).
| - | Injury | - | Discomfort | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| - | Age | - | Years of Experience | - | Age | - | Years of Experience | |||||||||||||||
| - | Injury | No Injury | - | Injury | No Injury | - | Discomfort | No Discomfort | - | Discomfort | No Discomfort | - | ||||||||||
| - | N | x̄±SD | N | x̄±SD | p | N | x̄±SD | N | x̄±SD | p | N | x̄±SD | N | x̄±SD | p | N | x̄±SD | N | x̄±SD | p | ||
| Neck | 10 | 41.5±12.6 | 299 | 39.1±10.4 | 0.482 | 10 | 17.3±11.6 | 299 | 10.6±10.6 | 0.461 | 33 | 39.7±9.6 | 276 | 39.2±10.6 | 0.776 | 33 | 15.3±9.2 | 276 | 14.7±10.8 | 0.729 | ||
| Shoulder | 17 | 44.9±9.0 | 292 | 38.9±10.4 | 0.020* | 17 | 19.5±9.2 | 292 | 14.5±10.6 | 0.032* | 42 | 40.1±10.0 | 267 | 39.1±10.5 | 0.565 | 42 | 16.4±10.3 | 267 | 14.5±10.6 | 0.284 | ||
| Upper back | 7 | 47.0±10.3 | 302 | 39.0±10.4 | 0.050 | 7 | 22.6±13.1 | 302 | 14.5±10.5 | 0.093 | 24 | 36.7±8.7 | 285 | 39.4±10.6 | 0.215 | 24 | 11.9±8.6 | 285 | 14.9±10.7 | 0.182 | ||
| Elbow and forearm | 3 | 39.3±6.0 | 306 | 39.2±10.5 | 0.912 | 3 | 12.0±11.8 | 306 | 14.8±10.6 | 0.642 | 23 | 40.2±10.1 | 286 | 39.1±10.5 | 0.538 | 23 | 15.7±11.4 | 286 | 14.6±10.5 | 0.415 | ||
| Wrist and hand | 12 | 42.8±7.7 | 297 | 39.1±10.5 | 0.180 | 12 | 17.2±7.7 | 297 | 14.6±10.7 | 0.229 | 31 | 39.2±8.2 | 278 | 39.2±10.7 | 0.994 | 31 | 15.0±8.9 | 278 | 14.7±10.8 | 0.846 | ||
| Lower back | 24 | 42.2±8.6 | 285 | 38.9±10.6 | 0.119 | 24 | 19.0±9.3 | 285 | 14.4±10.6 | 0.019* | 71 | 40.9±9.5 | 238 | 38.7±10.7 | 0.133 | 71 | 16.9±10.0 | 238 | 14.1±10.7 | 0.042* | ||
| Hip | 4 | 43.8±14.7 | 305 | 39.2±10.4 | 0.442 | 4 | 18.3±12.9 | 305 | 14.7±10.6 | 0.561 | 19 | 39.6±9.8 | 290 | 39.2±10.5 | 0.873 | 19 | 15.6±11.4 | 290 | 14.7±10.5 | 0.702 | ||
| Thigh | 3 | 33.7±12.0 | 306 | 39.3±10.4 | 0.384 | 3 | 9.0±7.2 | 306 | 14.8±10.6 | 0.387 | 18 | 39.1±9.9 | 291 | 39.2±10.5 | 0.968 | 18 | 15.9±10.7 | 291 | 14.7±10.6 | 0.633 | ||
| Knee | 31 | 42.2±11.0 | 278 | 38.9±10.4 | 0.082 | 31 | 17.3±10.9 | 278 | 14.4±10.5 | 0.138 | 47 | 39.8±10.2 | 262 | 39.1±10.5 | 0.380 | 47 | 15.6±9.8 | 262 | 14.6±10.7 | 0.501 | ||
| Lower leg | 1 | 27.0 | 308 | 39.3±10.4 | - | 1 | 7.0 | 308 | 14.8±10.6 | - | 18 | 37.3±9.5 | 291 | 39.3±10.5 | 0.420 | 18 | 13.3±9.3 | 291 | 14.8±10.7 | 0.550 | ||
| Ankle and foot | 39 | 42.8±9.3 | 207 | 38.7±10.6 | 0.020* | 39 | 19.7±10.6 | 270 | 14.0±10.4 | 0.002** | 29 | 39.3±9.9 | 280 | 39.2±10.5 | 0.956 | 29 | 15.6±10.5 | 280 | 14.6±10.6 | 0.648 | ||
* Indicates statistical significance <0.05.
** indicates statistical significance <0.01.
Table 2 describes the differences between MSIs and MSD locations according to age and years of experience in firefighters. Firefighters who reported MSIs in the shoulder (p = 0.020) and ankle and foot (p = 0.020) regions were significantly older than those who did not report MSIs. In addition, firefighters who had more years of experience were more likely to report MSIs in the shoulder (p = 0.032), lower back (p = 0.019), and ankle and foot (p = 0.002) regions. Based on MSD, firefighters who reported MSD in the lower back (p = 0.042) regions had significantly more years of experience.
Table 3 describes the association between MSIs and sociodemographic characteristics in firefighters. Univariable analysis indicated that females of age groups 30-39 years, 40-49 years, 50-65 years, 21-30 years with experience of 31+ years, married, and station commanders had an increased risk of MSIs by a factor of 2.14 (1.03, 4.42), 2.02 (1.03, 3.95), 2.87 (1.45, 5.71), 3.38 (1.61, 7.11), 2.18 (1.16, 4.14), 2.84 (1.26, 6.38), 1.75 (1.1, 2.84), and 5.92 (2.22, 15.77), respectively. In the multivariable analysis, in model 1, after adjustment for covariates, the 40-49 years and 50-65 years of age groups and rank of station commander increased the risk for MSIs by a factor of 2.39 (1.17, 4.89), 2.67 (1.22, 5.81), and 4.36 (1.16, 12.70), respectively. Univariable analysis indicated that age increased the risk of firefighters reporting MSIs in the shoulder and ankle and foot by a factor of 1.06 (1.01, 1.11) and 1.04 (1.00, 1.07), respectively. After adjustment for BMI, weekly physical activity was not associated with MSIs in the shoulder and ankle. Univariable analysis indicated that years of experience increased the risk of MSIs in the ankle and foot and lower back by a factor of 1.05 (1.02, 1.08) and 1.04 (1.00, 1.08), respectively. In the multivariable analysis, in model 2, years of experience increased the risk of MSIs in the ankle and foot by a factor of 1.05 (1.01, 1.09). Univariable analysis indicated that married firefighters had an increased risk of MSD by a factor of 1.66 (1.02, 2.70). After multivariable analysis, it was found that married firefighters had an increased risk of 1.89 (1.04, 3.41) for MSIs. In addition, years of experience increased the risk of MSD in the lower back by a factor of 1.03 (1.01, 1.05) but was not associated after adjustment for covariates.
Table 3.
| - | Univariate models a | Multivariate models b | - | - | ||
|---|---|---|---|---|---|---|
| - | Model 1 | Model 2 c | Model 3 d | - | ||
| - | OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p |
| Model: Musculoskeletal injury | - | - | - | - | - | - |
| Sex (female) | 2.14 (1.03, 4.42) | 0.039* | 2.08 (0.99, 4.40) | 0.055 | - | - |
| Model: Musculoskeletal injuries § | - | - | - | - | - | - |
| 20-29 years (reference) | - | - | - | - | - | - |
| 30-39 years | 2.02 (1.03, 3.95) | 0.041* | 1.83 (0.94, 3.69) | 0.074 | 1.46 (0.69, 3.08) | 0.322 |
| 40-49 years | 2.87 (1.45, 5.71) | 0.003** | 2.39 (1.17, 4.89) | 0.017* | 1.59 (0.59, 4.27) | 0.356 |
| 50-65 years | 3.38 (1.61, 7.11) | 0.001** | 2.67 (1.22, 5.81) | 0.014* | 1.58 (1.02, 6.69) | 0.533 |
| Model: Musculoskeletal injuries ¶ | - | - | - | - | - | - |
| 0-10 years of experience (reference) | - | - | - | - | - | - |
| 11-20 years of experience | 1.51 (0.87, 2.63) | 0.143 | - | - | 1.09 (0.68, 2.29) | 0.828 |
| 21-30 years of experience | 2.18 (1.16, 4.14) | 0.015* | - | - | 1.47 (0.53, 4.09) | 0.458 |
| 31+ years of experience | 2.84 (1.26, 6.38) | 0.001** | - | - | 1.98 (0.46, 8.46) | 0.356 |
| Model: Musculoskeletal injuries | - | - | - | - | - | - |
| Single (reference) | - | - | - | - | - | - |
| Married | 1.75 (1.1, 2.84) | 0.025* | 1.46 (0.79, 2.723) | 0.229 | 1.29 (0.83, 2.03) | 0.253 |
| Divorced | 2.16 (0.88, 5.30) | 0.095 | - | - | - | - |
| Model: Musculoskeletal injuries | - | - | - | - | - | - |
| Junior firefighter | - | - | - | - | - | - |
| Firefighter | 1.60 (0.86, 2.99) | 0.137 | - | - | - | - |
| Senior firefighter | 2.23 (0.94, 5.31) | 0.070 | - | - | - | - |
| Platoon commander | 1.84 (0.59, 5.67) | 0.287 | - | - | - | - |
| Station commander | 5.92 (2.22, 15.77) | <0.001** | 4.36 (1.31, 14.57) | 0.017* | 3.55 (0.95, 13.27) | 0.060 |
| Divisional commander | 2.37 (0.44, 12.81) | 0.317 | - | - | - | - |
| Model: Musculoskeletal injuries | - | - | - | - | - | - |
| Obesity | 1.80 (1.09, 2.98) | 0.022* | 1.49 (0.65, 3.43) | 0.350 | 1.47 (0.64, 3.39) | 0.368 |
| Model: Shoulder injury | - | - | - | - | - | - |
| Age § | 1.06 (1.01, 1.11) | 0.023* | 1.04 (0.99, 1.09) | 0.127 | - | - |
| Years of experience ¶ | 1.04 (0.99, 1.09) | 0.060 | - | - | 1.03 (0.98, 1.09) | 0.185 |
| Model: Ankle and foot injury | - | - | - | - | - | - |
| Age § | 1.04 (1.00, 1.07) | 0.038* | 1.03 (0.99, 1.07) | 0.126 | - | - |
| Years of experience ¶ | 1.05 (1.02, 1.08) | 0.002** | - | - | 1.05 (1.01, 1.09) | 0.006** |
| Model: Lower back ¶ | - | - | - | - | - | - |
| Years of experience | 1.04 (1.00, 1.08) | 0.044* | - | - | 1.03 (0.99, 1.08) | 0.109 |
| Model: Musculoskeletal discomfort | - | - | - | - | - | - |
| Sex (female) | 1.63 (0.79, 3.32) | 0.182 | - | - | - | - |
| Model: Musculoskeletal discomfort | - | - | - | - | - | - |
| Single (reference) | - | - | - | - | - | - |
| Married | 1.66 (1.02, 2.70) | 0.040* | 1.89 (1.04, 3.43) | 0.033* | - | - |
| Divorced | 2.05 (0.84, 5.05) | 0.117 | - | - | - | - |
| Model: Musculoskeletal discomfort | - | - | - | - | - | - |
| Obese | 1.46 (0.88, 2.42) | 0.140 | - | - | - | - |
| Model: Lower back ¶ | - | - | - | - | - | - |
| Years of experience | 1.03 (1.01, 1.05) | 0.046* | - | - | 1.70 (0.83, 3.51) | 0.149 |
* indicates statistical significance <0.05.
** indicates statistical significance <0.01.
Table 4.
| - | Univariate models a | Multivariate models b | - | - | ||
|---|---|---|---|---|---|---|
| - | Model 1 | Model 2 c | Model 3 d | - | ||
| - | OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p |
| Model: Musculoskeletal discomfort | - | - | - | - | - | - |
| Musculoskeletal injuries | 3.45 (2.15, 5.55) | <0.001* | 3.46 (2.11, 5.56) | <0.001** | 3.55 (2.17, 5.81) | <0.001** |
| Model: Shoulder discomfort | - | - | - | - | - | - |
| Shoulder injury | 8.79 (3.18, 24.37) | <0.001** | 12.21 (3.89, 38.34) | <0.001** | 12.24 (3.90, 38.37) | <0.001** |
| Model: Forearm and elbow discomfort | - | - | - | - | - | - |
| Forearm and elbow injury | 6.43 (0.56, 73.74) | 0.135 | 5.68 (0.49, 66.17) | 0.165 | 5.95 (0.51, 69/55) | 0.155 |
| Model: Wrist and hand discomfort | - | - | - | - | - | - |
| Wrist and hand injury | 37.36 (9.43, 148.06) | <0.001 | 51.20 (10.82, 242.23) | <0.001 | 50.85 (10.75, 240.33) | <0.001 |
| Model: lower back discomfort | - | - | - | - | - | - |
| Lower back injury | 13.08 (4.95, 34.53) | <0.001 | 12.62 (4.72, 33.72) | <0.001 | 12.22 (4.57, 32.67) | <0.001 |
| Model: Knee discomfort | - | - | - | - | - | - |
| Knee injury | 14.08 (6.19, 32.02) | <0.001 | 15.90 (6.63, 38.13) | <0.001 | 15.37 (6.46, 37.02) | <0.001 |
| Model: Ankle and foot discomfort | - | - | - | - | - | - |
| Ankle and foot injury | 4.54 (1.93, 10.69) | <0.001 | 4.78 (1.94, 11.77) | <0.001 | 4.70 (1.89, 11.71) | <0.001 |
* indicates statistical significance <0.05.
** indicates statistical significance <0.01.
Table 4 presents the association between MSD and MSIs in firefighters. The results indicated that musculoskeletal discomfort was associated with an increase in the likelihood of firefighters reporting MSIs (p <0.001). Firefighters who experienced shoulder, wrist and hand, lower back, knee, and ankle and foot discomfort were more likely to report shoulder, wrist and hand, lower back, knee, and ankle and foot injuries. After adjustment, firefighters remained more likely to report musculoskeletal injuries if they experienced MSD (p <0.001). In addition, in Model 2 and Model 3, firefighters who reported shoulder, wrist and hand, lower back, knee, and ankle and foot discomfort were more likely to report MSIs (all p <0.001).
5. DISCUSSION
This was the first study conducted on firefighters from the City of Cape Fire and Rescue Services, which has been a historically understudied population. The results of the current study indicated that a high prevalence of firefighters had sustained MSIs and reported MSD. We found that MSIs were significantly associated with sex, age and years of experience, rank and marital status. In addition, the present results reported that over 40% of firefighters experienced MSD while on active duty, most commonly in the lower back regions, which was related to aging and an increase in years of experience. These results are consistent with previous studies, which have indicated that as firefighters aged and remained longer in the profession, the attrition of the musculoskeletal system was associated with the increased prevalence of MSIs [4-6] and MSD [1, 15, 22] in firefighters. Furthermore, MSD was found to be significantly associated with MSIs in firefighters.
The most frequent mechanisms for injury were falls, jumps, slips or trips (39.7%), which occurred most frequently while firefighters were on the fireground (41%). The most common type of injury among firefighters was sprains and strains (68.4%). Similarly, Vaulerin et al. [14] and Nazari et al. [4] reported sprains among firefighters to be the most prevalent type of musculoskeletal injury. Hong et al. [5] reported falls, slips, and jumps to be the leading causes of injury (22.5%). A potential contributor to this commonly occurring injury mechanism may be due to the biomechanical differences and differences in physical fitness [4]. Foot and ankle injuries (25.8%) were the most prevalent injuries, closely followed by knee (20.5%) and lower back injuries (15.9%), which were more commonly sprains and strains (68.4%). Vaulerin et al. [14] reported ankle injuries to be the most common location of injury amongst French firefighters (77%). Contrary to these findings, Nazari et al. [4] reported that shoulder and knee injuries were more prevalent among male firefighters (5% and 8%, respectively), whereas female firefighters experienced more head, neck, arm, back, and thigh injuries (3%, 5%, 10.7%, 11%, and 6%, respectively). The current results indicated that firefighters who experienced back injuries and back discomfort were significantly older than those who did not report any injuries or discomfort. This is consistent with the findings of a study by Damrongsak et al. [16], who reported that age had a positive association with lower back pain and injuries in firefighters. Moreover, the present findings indicated that firefighters with more years of experience, especially those with 20 or more years of experience, were more likely to experience MSIs. The present study demonstrated that every year increase in ankle and foot injuries increased the risk of injuries by 4%. In addition, after adjustment for BMI and weekly physical activity, the association between age and lower back injuries and shoulder injuries did not remain significant. Similarly, findings from a study by Hong et al. [5] reported that the most commonly reported injuries were strains and sprains (74%) and lower back injuries (54%) and that firefighters with more than 17 years of experience were more likely to report injuries. This can possibly be due to the fact that firefighters with more experience are exposed to the strenuous working conditions of firefighting for a longer period than firefighters with less experience. This was also reported in a study by Hong et al. [5], who stated that firefighters with more than 17 years of working in the fire service were three times more likely to report an injury than those with less than 17 years of experience. Similarly, Frost et al. [6] also reported that firefighters with more years of experience reported more serious injuries than those who had fewer years of experience. Phelps et al. [23] also reported that firefighters who reported work-related injuries had more years in the service (16.5 years of experience) than those who did not report work-related injuries (14.6 years of experience). Firefighters are routinely required to carry heavy equipment while ambulating in difficult environments, contorting the body in unnatural directions, which may predispose the lower back and ankle regions to injury [18, 24]. In addition, ill-fitting footwear may add an additional burden to firefighters as boots are generic and not designed to cater toward distinct ankle and foot biomechanics in each firefighter [25, 26], which has been reported to be particularly problematic in female firefighters [27, 28]. Studies have indicated that weekly physical activity is necessary to maintain the MSH of firefighters [29-31]. In addition, higher body fat percentages place more strain on the musculoskeletal system, predisposing firefighters to injury [2, 29, 30], explaining why the associations found in the present study were reduced after adjustment for physical activity and BMI.
In the current study, females were more likely to report MSIs, particularly those in the age categories of 40-49 and 50-65 years, who were senior firefighters, station commanders, and divisional commanders. In addition, the 40-49 years and 50-65 years age groups and station commander increased the risk for MSIs by a factor of 2.39, 2.67 and 3.83, respectively. Similarly, Hong et al. [5] reported that firefighters with injuries (46.0 years) were significantly older than those without injuries (42.7 years) and that older firefighters were ten times more likely to suffer from work-related injuries than private-sector workers. The notion that the physically demanding nature of firefighting exposes firefighters to cumulative trauma and raises their sensitivity to impairment is consistent with the higher occurrence of work-related injuries in senior firefighters [32]. Campbell [33] reported that firefighters with older careers of 30 to 39 and 40 to 49 years accounted for 60% of the injuries reported, while the ages 20 to 29 years only accounted for 18% of all injuries. Similarly, Phelps et al. [23] also reported that increasing age was associated with a greater likelihood of work-related injuries. In contrast, Campbell [33] reported that in volunteer firefighters, the age group 20-29 years reported 35% of the total injuries, whereas older firefighters aged 30 to 39 years accounted for 22% of injuries, and the age group 40 to 49 years accounted for 17% of the total injuries. This may likely be due to volunteer firefighters being generally younger and inexperienced. This finding is in line with the findings of a study by Negm et al. [7], where the most reported injury types in firefighters older than 42 years were muscle, ligament, and joint injuries.
The results indicated that 40.4% of firefighters experienced MSD, which was moderate in severity and slightly interfered with their work, with most firefighters only experiencing discomfort one-to-two days a week. Nazari et al. [15] reported that 17% reported one painful site, 19% reported two painful sites, and 21% reported three or more painful sites, accounting for 57% of firefighters reporting experiencing musculoskeletal pain. In addition, the study noted that the spine was the most frequently reported painful site (41%). MacDermid et al. [22] reported that 46.4% of firefighters reported minor musculoskeletal health, and 13.1% reported moderate musculoskeletal health. In a study, only a few reported major musculoskeletal health problems (2.1%), which is consistent with the present study, where 2.9% reported severe MSD. The current results indicated that most (20.0%) firefighters experienced MSD in the lower back, followed by the knee (13.2%) and shoulder (11.8%). Similarly, Azmi et al. [34] reported that MSD in the lower back was the most prevalent region among firefighters. This was supported by Saremi et al. [35], who noted that the most common discomfort was in the upper and lower regions of the back, with 20% and 16.8%, respectively. Female firefighters were more likely to report MSD, especially those who were married. Moreover, married firefighters had an increased risk of 1.88 for MSIs. A study by Chenot et al. [36] reported that females were more likely to experience lower back pain than males. The additional strain of firefighting may also further predispose female firefighters to experience lower back pain compared to male firefighters. It was found that married firefighters were more likely to report MSD. This may be due to married firefighters opting against receiving medical treatment due to the extra financial expenses that may be incurred [37, 38]. The results of the study indicated that firefighters who experienced MSIs were significantly more likely to report MSIs. This finding is supported by previous studies, where it has been reported that MSD was significantly associated with MSIs in the future [39-41]. It is plausible that firefighters remain on active duty while experiencing MSD, eventually leading to MSIs [5, 42, 43]. To assist in reducing the incidence of MSIs in firefighters, invention strategies, such as regular physical activity should be encouraged, which has been shown to reduce the incidence of injuries [44-46]. Moreover, access to health professionals when experiencing MSD and receiving adequate treatment may reduce the likelihood of sustaining severe long-term injuries.
5.1. Strengths and Limitations
This study provides data on the prevalence and characteristics of musculoskeletal injuries and discomfort in firefighters from the City of Cape Town Fire and Rescue Service according to their age, sex, years of experience, rank, marital status, and education levels, which has been underreported in the literature in South Africa. Moreover, this is the first study published on the prevalence of injuries and the mechanisms of injuries in this understudied population, particularly in a South African context. Only a small number of the sample was female, which under-represented this sex within the firefighting community. In addition, due to this study being observational, it precludes the assumption of causality.
5.2. Recommendations for Future Research
Longitudinal studies are warranted in this population to determine causal factors that contribute to the high incidence of MSIs and MSD in firefighters. In terms of equal representation in the sampling, equal representation based on age and sex should be included, as female firefighters were underrepresented in the present study. Future studies should also use a larger sample size to increase the generalisability of the results. Moreover, future studies should conduct intervention studies, particularly related to rehabilitation and strength and conditioning, to establish exercise programmes to reduce the incidence of MSIs and MSD in firefighters.
CONCLUSION
Musculoskeletal injuries to the lower back, ankles and feet were the most prevalent anatomical locations for injury among firefighters, with falls, jumps, slips, and trips being the leading mechanisms of injury. Firefighters with more years of experience were more likely to have a higher prevalence of injuries, particularly in the shoulder, lower back, and ankle and foot regions. Moreover, firefighters experiencing more MSD were more likely to report MSIs. The high prevalence of ankle and lower back injuries may be attributed to the heavy equipment, poor fitting PPE, and extreme fatigue experienced during emergency callouts. The occurrence of ankle injuries may be due to the generic protective footwear distributed to the firefighters, leading to instability and poor support. This study highlights the high prevalence of work-related MSIs and MSD in firefighters of the City of Cape Town and the sociodemographic factors associated with these injuries, highlighting the need for educational interventions and preventative training strategies to decrease the injury and discomfort occurrence in firefighters.
AUTHORS’ CONTRIBUTIONS
J.R., I.P., G.N., and L.L. contributed to the study’s design. J.R., I.P., and G.N. participated in data collection. J.R., I.P., and G.N. contributed to the analysis and writing of the final manuscript. J.R. and L.L. contributed to the editing and finalization of all sections of the paper.
LIST OF ABBREVIATIONS
| MSIs | = Musculoskeletal Injuries |
| MSD | = Musculoskeletal Discomfort |
| CoCFFRS | = City of Cape Town Fire and Rescue Service |
| IPAQ | = International Physical Activity Questionnaire |
| SPSS | = Statistical Package for the Social Sciences |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study protocol was approved by the Humanities and Social Sciences Research Ethics Committee (HSSREC) (Ethics number: HS22/4/34) at the University of the Western Cape. Permission to conduct the study was obtained from the chief fire officer and the district manager of the City of Cape Town Fire and Rescue Service.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Participation in the study was voluntary, and all subjects gave their informed consent before participating in the study.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article is not available due to a data privacy agreement with the City of Cape Town Fire and Rescue Service. However, on request, we will send the files for use by researchers, upon formal request and after they sign an agreement with the researchers and City of Cape Town Fire and Rescue Service indicating they will follow the strict data protection rules set by the Fire and Rescue Services.
FUNDING
This research was funded by the National Research Foundation (NRF) (grant number 141282) and The Ryoichi Sasakawa Young Leaders Fellowship Fund (SLYFF). Neither funding bodies were involved in the study design, data collection or interpretation of the data. There is no conflict of interest between the funding agencies and the authors.

