All published articles of this journal are available on ScienceDirect.

Educational Programme to Implement Skin-to-skin Contact for Preterm Infants in the Intensive Care Units: Qualitative Study Proposal
Authors Info & Affiliations
Abstract
Introduction
Skin-to-skin contact (SSC) has been widely adopted as an efficacious and useful approach to neonatal care. Despite the endorsement of this practice by the World Health Organization (WHO) over a decade ago, healthcare institutions in South Africa, particularly in the North West Province (NWP), have shown limited progress with regard to its implementation. Of particular concern is the fact that South Africa accounts for 60% of the global mortality rate among low birth weight (LBW) preterm infants. Therefore, an educational programme can be beneficial for both parents and nurses in implementing SSC for preterm infants in intensive care units, with the aim of reducing the neonatal mortality rate.
Aim
The aim of this research is to develop an educational programme to implement SSC for preterm infants in intensive care units of the NWP.
Methods
This study will be conducted in three phases. Phase 1: An integrative literature review (ILR) will be conducted by following these five steps: formulation of the review question, search strategy, critical appraisal, data analysis, synthesis and conclusion. Phase 2 represents an empirical study using a qualitative exploratory and descriptive design. Purposive sampling will be used to select two populations. Population one will be parents of preterm infants and population two will be registered nurses and midwives. Semi-structured focus group discussions (FGDs) with a minimum of six participants will be used to collect data in both populations until reaching data saturation. Data will then be analyzed using steps proposed by Creswell and Clark. Phase 3 consists of the development of an educational programme to implement SSC for preterm infants in intensive care units, using Kellogg’s Logic Model (KLM). The following three KLM steps will be used for the development of an educational programme: inputs and activities, identifying outputs, outcomes, and outcomes indicators.
Conclusion
The study furnishes an introduction to the research, the aim and objectives of the research as well as the research methodology that will be adhered to. The results obtained from phases 1 and 2 will be used to form the basis for the development of an education programme in phase 3.
1. INTRODUCTION
The definition of a preterm infant, as established by the World Health Organization (WHO), encompasses those infants who are born prior to 37 weeks of gestation and possess a birth weight of less than 2500g [1]. An estimated 1 million children succumb annually as a result of complications arising from preterm birth. On a global scale, prematurity serves as the primary cause of mortality among children under the age of 5 years [2]. It is worth noting that the majority of preterm births occur within the African and Southern Asian regions [3]. Nonetheless, preterm births stand as a true global predicament. Hence, a marked disparity emerges in the survival rates of infants born prematurely, contingent upon the geographic location of their birth. Staggeringly, more than 90% of neonates born extremely preterm in Low Income Countries (LICs) die within the initial days of life, while less than 10% of their counterparts in High Income Countries (HICs), a mere fraction in comparison, meet the same fate [1, 2].
Approximately 14.2% of the preterm infants delivered in South Africa (SA) do not survive, despite the fact that the majority of premature births take place within healthcare facilities. This phenomenon poses a significant threat to the overall outcomes of childhood [1]. However, it is important to note that these statistics may not accurately represent the true extent of preterm birth in South Africa thus far. The discrepancy is due to incomplete registration data caused by under-reporting and delayed registrations [4]. The current under-5 years mortality rate of 128 per 1000 live births falls short of the recommended target of 12 per 1000 live births for neonates as set forth in the Sustainable Development Goals (SGDs) for the year 2030 [5]. Much work remains to be done in order to expedite the reduction in infant mortality and meet the new target outlined in goal 3 of SDG 2030 [6].
The endorsement of skin-to-skin contact (SSC) by the WHO was made official through the publication of a practice guideline in 2003 [7]. The endorsement was intended to facilitate the development of policies, protocols and training manuals in relation to SSC. In the context of the North West, a province with limited resources, there are numerous medical challenges that arise due to the high rate of preterm births [8]. Despite significant progress made in the past decade, concerns still remain regarding the survival and morbidity of preterm and low birth weight (LBW) neonates [9]. The implementation of SSC has been shown to decrease the mortality rate in newborns and if widely adopted, it has the potential to reduce the deaths of premature infants, particularly in LICs that lack the financial means to provide incubators. Additionally, it has been demonstrated that SSC improved maternal interactive behaviour and social competence as well as cognitive development in children [10, 11].
There are often significant barriers to consistently implementing SSC in intensive care units. Barriers encountered by parents include shock from an unexpected early birth, overwhelming the intensive care environment due to seeing their infant connected to wires, electrodes and intravenous lines and unfamiliar equipment such as incubators and ventilators [12]. This unexpected stressful event can cause a feeling of loss of parental control when their infant is quickly taken away for medical care [12]. The neonatal nurses, situated at the bedside at all hours of the day and night, hold a strategic position as the main purveyors of information, catering to the emotional and educational requirements of parents [13].
Several hospitals have implemented educational programmes for implementing SSC for preterm infants in intensive care units. The effectiveness of these programmes has been evaluated in different studies. One study conducted in neonatal intensive care units at Khartoum State Hospital, Sudan, found that the application of kangaroo care or SSC led to significant improvements in weight gain, oxygen saturation, heart rate, and respiratory rate of preterm infants [14]. Another study guided the process of implementing an educational intervention aimed at an evidenced-based change in the practice of SSC and showed some positive results, such as a longer duration of SSC and improved parent education [15]. This model may need to be adapted in SA, with the aim of reducing the neonatal mortality rate.
An educational programme can be beneficial for both parents and nurses in implementing SSC for preterm infants in intensive care units. A study carried out in Canada examined the advancement of digital educational programmes involving parents of premature infants and neonatal nurses. The findings demonstrated that the implementation of digital educational programs enhanced the knowledge of parents and facilitated communication between parents and caregivers [16]. Another randomized controlled trial, which took place in Iran, was conducted to examine the impact of continuous education and monitoring during treatment at home. The results of this study demonstrated positive outcomes in terms of parent-child interaction, child development, and children's participation in preschool [17]. Interestingly, there is a growing interest in implementing a similar program known for parents with preterm infants’ admitted in intensive care units and neonatal nurses. To the best of our knowledge, this is the first investigation to develop an educational programme for implementing SSC for preterm infants in intensive care units of the North West Province (NWP).
1.1. Problem Statement
Globally, there has been a rise in the incidence of morbidity and mortality rates among preterm infants [7]. This trend is also evident in the context of South Africa, particularly in the NWP, where premature infants face a higher risk of death due to inadequate and costly care [4]. Several countries have made efforts to explore and implement educational and training initiatives, which have proven to enhance parents’ perception, value, competency, and comfort in caring for their preterm infants [16, 17]. However, it is important to note that the implementation of such initiatives in NWP health facilities is lacking as a midwife with three years of experience in intensive care units, one of the researchers has observed that SSC has not been extended beyond the labour ward. Additionally, there is a lack of formal parental orientation classes or educational training for infant care in the intensive care units at local healthcare facilities in the NWP. Consequently, the aim of this study is to develop an educational programme aiming at the implementation SSC for preterm infants in intensive care units of the NWP.
1.2. Research Questions
Based on the above problem statement, the following questions were posed:
- What are the key components of an educational programme for preterm infants in intensive care units?
- What are the perceptions of parents with preterm infants regarding the implementation of SSC in the intensive care units?
- What are the perceptions of registered nurses and midwives on an educational programme to implement SSC for preterm infants in intensive care units?
- How should the educational programme to implement SSC for preterm infants in intensive care units of the NWP be developed?
1.3. Aim
The aim of this study is to develop an educational programme to implement SSC for preterm infants in intensive care units of the NWP in an effort to reduce the preterm mortality rate.
1.4. Objectives
- To describe the key components of an educational programme for implementing SSC preterm infants in intensive care units by means of an integrative literature review (ILR).
- To explore and describe the perceptions of parents with preterm infants regarding the implementation of SSC in the intensive care units of the NWP.
- To explore and describe the perceptions of registered nurses and midwives regarding an educational programme for implementing SSC for preterm infants in intensive care units of the NWP.
- To develop an educational programme to implement SSC for preterm infants in intensive care units using Kellogg’s logic model.
1.5. Theoretical Framework
In this study, the Bandura self-efficacy model will be used as a theoretical framework. Self-efficacy is defined as belief in one’s abilities to organize and execute the courses of action required to produce a given attainment [18]. The four sources of self-efficacy are 1) Mastery Experience, 2) Vicarious Experience, 3) Verbal Persuasion, and 4) Physiological and Emotional States (Fig. 1: Bandura).
1.5.1. Mastery Experience
The first and most important source of increasing self-efficacy is having a direct experience of mastery [18]. Experience of success by parents and nurses regarding the implementation of SSC and the feeling of mastery enhance self-efficacy, while regular failure decreases self-efficacy. Once the parents and nurses developed a strong self-efficacy with this intervention, one failure does not have much influence. Experience with behaviour and the attributions of success and failure are an important source for the development of expectations of efficacy.
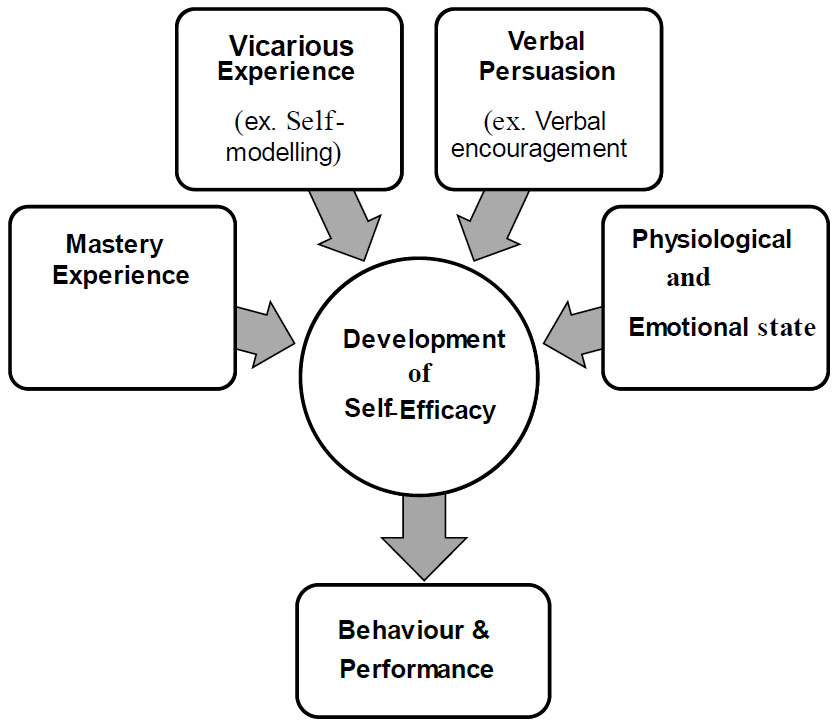
1.5.2. Vicarious Experience
The second source of self-efficacy is a vicarious experience [18]. Seeing others perform successfully is also an important source of self-efficacy. Other persons can serve as an example (role model) and supply information about the degree of difficulty of a specific kind of behaviour. In this study, nurses and midwives will serve as role models to the parents of preterm infants on the successful implementation of SSC for preterm infants in intensive care units.
1.5.3. Verbal Persuasion
Verbal persuasion is the third source of self-efficacy [18]. It involves giving instructions, suggestions, and advice to nurses and midwives to try to convince parents that they can succeed in the difficult task of caring for preterm infants in intensive care units. If parents of preterm infants are convinced of their abilities, they will be more inclined to persevere and will not give up easily.
1.5.4. Physiological and Emotional States
The last source for improved self-efficacy is physiological and emotional states [18]. Information on the human body can also influence a person’s estimation of his or her capability to show a specific behaviour. In judging their own capacities, persons use information about their physiological and emotional situation [18]. For example, what parents and nurses believe about SSC intervention for preterm infants can influence the self-efficacy to practice this intervention. These four sources influence each other and can improve behaviour and performance.
2. MATERIALS AND METHODS
This section provides a broad overview of the research methods to be followed in the study.
2.1. Phase 1: Integrative Literature Review (ILR)
In the integrative literature review, the authors aim to address the key components of an educational programme as a phenomenon by identifying, critically evaluating and integrating the findings from all relevant studies that address one or more research questions. These five steps were followed in generating ILR: formulation of the review question, search strategy, critical appraisal, data analysis and synthesis and conclusion [19].
2.1.1. Step 1: Formulation of the Review Question
The review question pertains to the formulation of the problem, commencing with a precise discernment of the problem statement, elucidations and crafting of the review inquiry to contend with the review question [20]. The review question was constructed by utilizing the population, intervention, outcome and timeframe (PIOT) format [20]. For the purpose of this study, the population (P) refers to parents of preterm infants. Interventions (I) comprise key components of educational programmes to implement SSC for parents with preterm infants admitted in intensive care units. The outcome (O) measure is an indicator of health and wellbeing of both parents and preterm infants. The time frame (T) is the time spent by preterm infants in the intensive care units. Based on the outcomes of the PIOT, the following review question was formulated: “What is stated in the published literature regarding the key components of an educational programme for implementing SSC for preterm infants in intensive care units?”
2.1.2. Step 2: Search Strategy
The second step in the review process was to develop a search strategy. The inclusion criteria will be all national and international literature (research and non-research) on key components of an educational programme to implement SSC for preterm infants admitted in intensive care units, published from 2019 to 2023, to provide recent evidence [21]. Only studies written in English will be included since it is the language shared by all the review team members. The types of literature included in this review include studies that use qualitative, quantitative and mixed methods [21]. This includes systematic reviews, documents, interventions, reports, components or strategy reviews, theses and dissertations.
2.1.2.1. Exclusion Criteria
Prefaces, letters to editors and editorials will be excluded since they comprise opinions and are not regarded as primary research. Duplicated articles will also be excluded after deciding which one (if they are not identical) provides the most comprehensive data regarding the study. During the search stage of the ILR, studies or documents that did not discuss key components of an educational programme in the title, abstract, or text will be excluded. Titles of each study or article will be read to determine the relevance to the study topic. Studies or articles will be excluded if they are not accessible to the researcher via the university’s library or inter-lending options or by contacting the authors via email.
2.1.2.2. Literature Search
Studies will be collected using multiple data platforms, while a clear description of inclusion and exclusion criteria guides the search process. The search will be conducted from February to June 2023 on the following databases, namely: Electronic reference databases: CINAHL, MEDLINE, PsycINFO, ProQuest, Health Source: Nursing/Academic Edition and Health Source-Consumer Edition using different keywords and reference lists from the bibliography of the documents sampled from the previous stages [21].
The search strategy will follow the phrase approach of combining any search terms and keywords such as AND, OR and the wild card symbol (*) to yield more relevant results. The following search phrases will be used: key components of an educational programme OR intervention AND skin to skin contact OR care OR kangaroo mother care AND parents* OR mothers AND preterm infants* OR premature AND infant or newborn* AND intensive care units OR neonatal units. Along with the electronic platform search, a hand search of reference lists of selected records will be conducted to search for additional documents or studies that could be considered for inclusion.
| Criteria | Yes (2) | Partial (1) | No (0) | |
|---|---|---|---|---|
| 1 | Question/objective sufficiently described? | - | - | - |
| 2 | Study design evident and appropriate? | - | - | - |
| 3 | Context for the study clear? | - | - | - |
| 4 | Connection to a theoretical framework/wider body of knowledge? | - | - | - |
| 5 | Sampling strategy described, relevant and systematic? | - | - | - |
| 6 | Data collection methods clearly described and systematic: | - | - | - |
| 7 | Data analysis clearly described and systematic? | - | - | - |
| 8 | Use of verification procedures to establish credibility? | - | - | - |
| 9 | Conclusions supported by the results? | - | - | - |
| 10 | Reflexivity of the account? | - | - | - |
| Criteria | Yes (2) | Partial (1) | No (0) | N/A | |
|---|---|---|---|---|---|
| 1 | Question/ objective sufficiently described? | - | - | - | - |
| 2 | Study design evident and appropriate? | - | - | - | - |
| 3 | Method of subject/comparison group selection or source of information/input variables described and appropriate? | - | - | - | - |
| 4 | Subject (and comparison group, if applicable) characteristics sufficiently described? | - | - | - | - |
| 5 | If interventional and random allocation was possible, was it described? | - | - | - | - |
| 6 | If interventional and binding of investigators was possible, were they reported? | - | - | - | - |
| 7 | If interventional and binding of the subject was possible, was it reported? | - | - | - | - |
| 8 | Outcome (if applicable) exposure measures well defined and robust to measurement/misclassification bias? Means of assessment reported? | - | - | - | - |
| 9 | Sample size appropriate? | - | - | - | - |
| 10 | Analytic methods described/justified and appropriate? | - | - | - | - |
| 11 | Is some estimate of variance reported for the main results? | - | - | - | - |
| 12 | Controlled for confounding? | - | - | - | - |
| 13 | Results reported insufficient details? | - | - | - | - |
| 14 | Conclusions supported by the results? | - | - | - | - |
2.1.3. Step 3: Critical Appraisal
The third step in the ILR process entails an in-depth appraisal of the relevant documents identified during the searches. Critical appraisal is necessary in order to determine substandard documents that should be omitted due to their lack of methodological excellence and thoroughness, thereby enhancing the credibility of the evidence incorporated in the final ILR [22]. Each article will be appraised for methodological validity by using a quality appraisal checklist that contains ten-question criteria, ranging from 0 (No) to 2 (Yes), both for qualitative studies and for quantitative studies [18]. Scores will be interpreted based on the recommended criteria: 50-100 percent denotes a “good” study, while less than 50 percent indicates a “poor” study. Tables 1 and 2 present checklists for assessing the quality of qualitative and quantitative studies.
2.1.4. Step 4 Data Analysis and Synthesis
Data collected by the researcher will be analyzed and then synthesized into a unified statement during this stage. This step aims to synthesize the separate data points collected into a unified statement about the research problem. In order to describe the key components of an educational programme for preterm infants from the documents appraised and found to be good quality, the data from primary sources will be extracted based on author, reference, country, focus, question, design, sample, method and findings.
2.1.5. Step 5: Presentation of Findings
After synthesizing the data, it is recommended that a summary of the evidence should be written. In order to give a summary and interpretation of the outcomes and characteristics of the included documents, the review usually provides both text and tables [23]. The ILR report will include an integration of concepts, thoughts, definitions or other relevant information that was derived from the included documents on the phenomenon being studied. Concluding statements will be developed and derived from the analysis and discussion of the information synthesized.
2.2. Phase 2: Empirical Study
Phase two will be the empirical phase, with two populations chosen based on the objectives of the study. In addressing these objectives, the researcher will use a qualitative exploratory and descriptive design. An exploratory and descriptive research design is a method of exploring and describing the area of human experience in order to understand a person’s world perception [24]. An explorative approach will be used in this phase because of its ability to discover new knowledge in an unfamiliar setting and give the researcher an insight into the problem under investigation [25]. Parents’, registered nurses and midwives’ perceptions of an educational programme for implementing SSC for preterm infants in intensive care units will be explored.
2.3. Study Context
Study context refers to the specific place where data will be collected [26]. This particular investigation will be carried out in the NWP, a region that lacks sufficient resources and does not have a Level 3 referral hospital. The primary focus of this research is on the intensive care units in Level 2 hospitals within the NWP, as it has been found that 52% of all preterm deaths occur in such hospitals in SA [27]. These Level 2 hospitals are capable of accommodating all preterm infants and offer a greater array of resources and specialists compared to Level 1 hospitals. However, it is important to note that Level 2 hospitals are not as well resourced (including staffing and equipment) as Level 3 hospitals, which boast full-time specialists available on-site 24 hours a day.
2.3.1. The Four Level 2 Hospitals in the NWP are the Following
- Potchefstroom and Klerksdorp/Tshepong complex hospitals in the Dr. Kenneth Kaunda district
- Mafikeng hospital in the Ngaka Modiri Molema district
- Rustenburg hospital (Job Shimankana Tabane Provincial Hospital) in the Bojanala district
Rustenburg is situated in the Bojanala region, Mafikeng in the Ngaka Modiri Molema district, while Klerksdorp/Tshepong and Potchefstroom are situated in the Dr Kenneth Kaunda district. Klerksdorp/Tshepong’s population is 334 497, Potchefstroom’s is 166 772, Mafikeng’s is 255 658 and Rustenburg’s population is 370 910 [22]. The health system of the NWP consists of four (4) Level 2 hospitals, 17 Level 1 district hospitals, and 9 community hospitals.
2.4. Population and Sampling
The target population for this study is divided into two main categories.
2.4.1. Population One
Population one will comprise all parents of preterm infants admitted to Level 2 hospitals in the NWP during the period of the study. This includes parents of preterm infants who are still alive and were admitted or discharged in the intensive care units before the study took place. Approximately 24 parents of preterm infants will be included in the FGDs until reaching data saturation (the point where no new information is generated). The reason for choosing parents who have practiced SSC is that they are considered to have experience and could share information based on the practice of SSC in intensive care units.
2.4.2. Population Two
Population two will comprise registered nurses and midwives working in the intensive care units of Level 2 hospitals in the NWP. Approximately 20 registered nurses and midwives will be included in the FGDs until reaching data saturation. The reason for choosing nurses and midwives is the vital role they play in supporting parents of preterm infants, starting from antenatal care and labour ward care up to postnatal care and intensive care. They can share useful information regarding an educational programme to implement SSC for preterm infants in the intensive care units. Only registered nurses and midwives with at least 12 months of working experience in the intensive care units and volunteersparticipating in this study will be selected to participate.
2.5. Sampling
For the purpose of this study, the researcher will use non-probability sampling, called purposive sampling, to select both populations. The aim is to learn as much as possible about participants’ perceptions regarding the implementation of SSC for preterm infants in intensive care units. The utilization of purposive sampling offers the researcher an advantage by permitting the selection of the sample to be guided by participants’ knowledge of the phenomenon under investigation [25].
2.5.1. Data Collection
Data will be collected in the following two stages:
2.5.1.1. Stage 1
Prior to the initiation of data collection, the lead researcher will introduce herself to the participants and explain the rationale for her presence in the unit. Subsequently, a comprehensive account of the study’s scope will be presented. The researcher will also outline the ethical considerations of confidentiality and anonymity as well as the participants’ right to self-determination. Participants will be informed that their participation in this study is voluntary and that they are free to withdraw from it at any time without facing any consequences. Data will be collected by the researcher in a private room.
Semi-structured FGDs will be employed to explore the perceptions of parents’ regarding the implementation of SSC for their preterm infants. Firstly, the researcher will gather the demographic information of the participants. Following the capturing of demographic information, the following question will be asked: “What do you understand by the word skin-to-skin contact and its’ benefits?” Data will be gathered in a private room over a period of four to eight (4–8) weeks, utilizing two languages: English and Setswana. A minimum of six (6) participants will be included in each FGD until data saturation is reached. Participant responses will be documented and recorded through the use of an audio recorder. The FGDs will consist of open-ended questions. All forms, including the consent form, will be securely stored in a locked cupboard for safekeeping, while electronic data will be stored on a password-protected computer belonging to the lead researcher.
2.5.1.2. Stage 2
A similar process to Stage 1 will be followed in Stage 2 of the study before data collection commences. Data will be collected for a period of two to four (2–4) weeks. FGDs will be conducted to explore the perceptions of registered nurses and midwives regarding an educational programme for implementing SSC for preterm infants in intensive care units of the NWP. A minimum of five (5) participants per FGD will be included until data saturation is reached. FGDs will be guided by five open-ended questions. A similar process to Stage 1 will be followed.
2.6. Data Analysis
The process of data analysis starts by organizing and preparing data from the participants in order to give the data meaning [26]. Qualitative data will be transcribed verbatim, and themes and sub-themes will be deduced from the participants’ rich data. The researcher will analyse and discuss data as one set of data using the following steps proposed by Creswell and Clark [27].
2.6.1. Step 1: Reading through the Data
The researcher will acquire a comprehensive understanding of the data by thoroughly examining all of the transcriptions. This will provide insights into the segments of data and their characteristics or significance. She will then document the meaning that emerges during the reading process, noting down all ideas as they arise. She will carefully and repeatedly review the transcriptions of all participants in order to comprehend them.
2.6.2. Step 2: Reduction of the Collected Data
The researcher will categorize the data based on the presence or frequency of concepts found in the transcriptions and subsequently compile a list of all topics that emerge during the reduction process. Similar themes will be grouped together and notes will be made on the margins of the transcriptions.
2.6.3. Step 3: Asking Questions about the Meaning of the Collected Data
The researcher will revisit the transcriptions and conduct an analysis. This time, she will pose questions to herself regarding the transcriptions of the reviewer, utilizing the codes that were determined based on concept frequency. The questions will revolve around identifying descriptive words and uncovering the underlying meaning.
2.6.4. Step 4: Abbreviation of Topics to Codes
The researcher will then begin to condense (abbreviate) the topics that emerged as codes. These codes will be noted on the margins of the paper alongside the corresponding data, using a different coloured pen than in Step 3.
2.6.5. Step 5: Development of Themes and Sub-themes
The researcher will then develop themes and sub-themes from the coded data and the associated texts and reduce the total list by grouping topics that relate to one another.
2.6.6. Step 6: Compare the Codes, Topics and Themes for Duplication
The researcher will re-examine the work from the outset, checking for any duplication and refining the codes, topics and themes as necessary. Additionally, similar codes will be grouped together.
2.6.7. Step 7: Initial Grouping of all Themes and Sub-themes
The data pertaining to each theme will be consolidated into a single column and a prelimary analysis will be conducted. This will be followed by a meeting between the lead researcher and the independent co-coder, in order to establish a consensus on the independently identified themes and sub-themes.
2.7. Phase 3: Development of An Educational Programme
This phase addresses the main objective of the study, which entails the development of an educational programme for implementing SSC for a preterm infant in intensive care units of the NWP. The process of ILR and empirical data collected from the participants will form the basis of this phase. The Kellogg’s Logic Model (KLM) will be utilized in this study. The adoption of a KLM has proven effective in programme planning, implementation, and performance management in various fields, including primary care. A logic model is defined as a graphical or textual representation that outlines how a programme is intended to operate. It establishes connections between outcomes, processes, theoretical assumptions, resources, activities, and results as they relate to a specific programme [28]. The following KML steps will be used:
2.7.1. Step One: Agree on the Vision, Mission and Target Audience
A vision statement serves as the inspiration and framework for an organisation’s strategic planning. It addresses the questions of what the organization wants to become and where it wants to go [28]. The focus is on determining the long-term direction of the organization. A mission statement, on the other hand, defines the unique purpose for which an organization exists. It answers the questions of who the organization is and what it does [28].
2.7.2. Step Two: Identify and Describe Assumptions, Inputs and Activities
The development of an educational programme for implementing SSC for preterm infants in intensive care units is influenced by assumptions. Inputs refer to the resources that are available or required for the operation of the programme [28]. In this programme, the human resources team consists of the role players involved in the care of parents and preterm infants in intensive care units. Non-human resources include equipment used in health facilities, records, policies, guidelines, and protocols. According to the Kellogg Foundation [28], the identified available resources are utilized to carry out the planned activities. In this study, these activities include orientation, education and in-service training, and any other form of support.
2.7.3. Step Three: Identify Outputs, Outcomes, and Outcome Indicators
Outputs refer to the direct tangible results that stem from the programme activities [28]. The outcomes and outcome indicators denote specific changes in knowledge, skills, or level of functioning that are expected to arise from programme activities. These outcomes are often expressed at an individual level and can be categorized as short-term and long-term outcomes [28].
2.8. Trustworthiness
The following criteria for ensuring trustworthiness will be adhered to [29]: Credibility will be assured through prolonged engagement during the process of collecting data. Throughout the FGDs, the authors will interpret and evaluate the data obtained from members of diverse audiences and groups from whom the data is requested. Moreover, the voices of the participants will be incorporated to mitigate any biases. Dependability will be attained by ensuring consistency and usability of the data. An independent coder will be employed to code the transcribed data, and the findings will be presented to the supervisors. Transferability will be assured by providing a comprehensive description of the participants, the context and the setting of the research study. To ensure conformability, an audit procedure will be conducted to validate whether the transcripts resemble the raw data on the tape and are transcribed verbatim.
3. RESULTS AND DISCUSSION
SSC can be seen as an ongoing process of identifying gaps in the functionality of an already implemented program and negotiating changes, which would address these gaps, and is a complex, multifaceted process. The qualitative study described in this protocol sits within a multiphase research project that aims to develop an educational programme to implement SSC for preterm infants in intensive care units of the NWP. It is important to acknowledge that a study with these characteristics is advantageous within the qualitative approach of the investigation [29]. Consequently, this study will explore and describe the perceptions of parents with preterm infants and registered nurses and midwives regarding the educational programme to implement SSC for preterm infants in intensive care units of Level 2 hospitals in the NWP. Approximately 24 parents of preterm infants and 20 registered nurses and midwives will be included in the study until data saturation is reached. Results from the data analysis will be presented in the form of themes and sub-themes.
4. STRENGTHS AND LIMITATIONS
Certain limitations of this study should be pointed out. The execution of the study in a specific setting, such as a single province, may impede the generalizability of the collected data. However, employing a purposive sampling strategy will enable authors to acquire a diverse sample that reasonably represents both populations of the NWP. The utilization of semi-structured FGDs could be considered a limitation due to the possibility of the information being influenced by the interviewer’s perspective. Nevertheless, an FGD approach is necessary, given the personal nature of the topic being discussed. Additionally, the process of recording and transcribing the FGDs, and the subsequent triangulation during the coding and analysis of the data will aid in surpassing these potential methodological obstacles [30].
CONCLUSION
The birth of preterm infants is unexpected and often stressful for parents. Nurse-mother interaction and provision of support in areas like SSC would empower mothers and promote their physical and psychological well-being and help them to obtain the best health status for their babies. The high rate of mortality and morbidity of preterm infants contribute to population in the countries of North West society. It seems necessary to explore and describe perceptions’ of parents as well as registered nurses and midwives regarding an educational programme for implementing SSC for preterm infants in intensive care units.
LIST OF ABBREVIATIONS
| CEO | = Chief Executive Officer |
| DoH | = Department of Health |
| FGDs | = Focus Group Discussions |
| HREC | = Human Research Ethic Committee |
| ILR | = Integrative Literature Review |
| KLM | = Kellogg’s Logic Model |
| LBW | = Low Birth Weight |
| LICs | = Low Income Countries |
| NWP | = North West Province |
| NWU | = North-West University |
| SA | = South Africa |
| SGDs | = Sustainable Development Goals |
| SSC | = Skin-to-Skin Contact |
| STROBE | = Strengthening the Reporting of Observational Studies in Epidemiology |
| WHO | = World Health Organization |
ETHICAL STATEMENT
Approval was from the following entities:
• Scientific approval was obtained from the Scientific Review Committee of Quality in Nursing and Midwifery (NUMIQ).
• Ethical approval was obtained from Health Research Ethics Committee (HREC) at NWU (NWU-00006-23-A1).
• Permission to conduct the study was obtained from North West Department of Health (DoH).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
In order to comply with the ethical considerations in this study, consent will be obtained from the participants who volunteer to participate in the study and information of the participants will be kept confidential.

