All published articles of this journal are available on ScienceDirect.

Can Hibiscus Sabdariffa Decrease Blood Pressure in Menopause Women with Hypertension?
Authors Info & Affiliations
Abstract
Background
Cases of hypertension in menopause have doubled since 1990 worldwide. During menopause, endothelial cells are destroyed due to estrogen depletion. Endothelial damage further triggers plaque in the blood while stimulating blood pressure to rise. In this case, the anthocyanin content in Hibiscus sabdariffa is an effective vasodilator of smooth muscle and blood vessels to lower blood pressure.
Purpose
This research aimed to know the effect of Hibiscus sabdariffa on blood pressure in menopause women with hypertension.
Methods
Quasi-experiment with pretest-posttest control group design was conducted. Ninety participants were divided into two groups, namely intervention group (45 participants) and control group (45 participants), selected from a public health center, using simple random sampling. The intervention group was given standard care and rosella extract as much as 1 x 1 with a dose of 500 mg for five days, while the control group only received standard care.
Results
Based on the paired Sample T-Test results in the experimental group, both systole and diastole pressures showed the same significant results with p-value of 0.000. Meanwhile, in the control group, the results showed a systole p-value of 0.279 and a diastole p-value of 0.132. Furthermore, the difference in posttest systole and diastole in the intervention and control groups is p-value 0.000.
Conclusion
The provision of roselle (Hibiscus sabdariffa) can reduce blood pressure in menopause women who experience hypertension. This study is expected to help health workers provide rosella extract to menopause women who experience hypertension as an alternative treatment.
1. INTRODUCTION
The population of menopause women in the world in 2030 is estimated to reach 1.2 billion, which is three times the number of menopause women census figures in 1990 [1]. The total population of women over 45 years old in East Java in 2020 was 6,901,410 [2]. Based on the preliminary study results, it is known that the number of women aged more than 45 years old in the Balowerti Health Center working area in 2022 was 5917. In this case, 50-year-old women who will experience menopause can have an increased risk of developing cardiovascular diseases, one of which is hypertension.
One of the main risk factors for both cardiovascular and cerebrovascular diseases is hypertension [3]. An estimated 1.28 billion adults globally, aged 30 to 79, suffer from hypertension; the majority of these individuals, or two-thirds, reside in low- and middle-income nations. Between 1990 and 2019, the number of adults aged 30-79 years old who had hypertension doubled, from 331 million women and 317 million men to 626 million women and 652 million men [4]. In this case, as many as 41% of the world's menopause women suffer from hypertension [5]. New research shows that many middle aged women live with hypertension and are not diagnosed because symptoms of the condition, including chest pain, fatigue, headaches, palpitations, and sleep disturbances, are mistakenly attributed to menopause [6]. Whatever age a woman experiences menopause, environmental causes may influence genes to modulate hypertension [7]. Many studies show that menopause is associated with a 2-fold increased risk of hypertension in terms of age and body mass index [3]. The rate of hypertension increases after menopause when estrogen levels drop [8]. Hypertension and pre-hypertension in menopause women are highly prevalent and increase sharply with age [9].
In the treatment of hypertension during menopause, several non-pharmacological ways can be applied, such as exercise, which has a positive effect on cardiovascular disease in hypertensive post-menopause women [10]. In post-menopause women with hypertension, combined exercise training enhances cardiovascular health and can lower the risk of cardiovascular disease [11]. According to research published in 2017, there are implications for both the prevention of cardiovascular disease and the maintenance or enhancement of post-menopause women's health when it comes to exercise, combining resistance and aerobic elements [12]. Another method that can be carried out is acupuncture which is performed for 24 months, and can affect blood pressure in menopausewomen who have stage 1 hypertension [13]. In addition, mindfulness and relaxation also have an effect on reducing diastolic and systolic pressure [14].
Prevention and reduction of hypertension can be done by using natural herbal medicines with antihypertensive potential and fewer side effects can be a good substitute for synthetic drugs [15]. Roselle is an herbal plant that has been widely used in many countries as a beverage and source of medicine. In this case, the part used is the petals of the roselle flower. Roselle is widely used as an antihypertensive drug because it has affordability in terms of price in people with hypertension [16]. Hibiscus sabdariffa tea effectively reduces blood pressure in patients with stage 1 hypertension [17]. Consuming roselle tea can have beneficial effects on controlling glycemic status and blood pressure in adults [18]. The administration of roselle extract at a dose of 40 mg/kg body weight is effective for reducing systole by 27.74% and diastole by 33.18% [19].
This study used standardized roselle extract so that the dose is controlled and accurate. This study aims to analyze the effect of roselle extract (Hibiscus sabdariffa) on blood pressure in menopause women.
2. METHODS
2.1. Research Design
This research is a quantitative study using a quick experimental design with a pretest and posttest control group design method. The research technique applied is by giving roselle extract preparation (Hibiscus sabdariffa) to menopause women with hypertension, where the blood pressure levels of the subject group were observed before being given the roselle and after being given roselle (day 6). The population in this study were all menopause women in the working area of a Public Health Center in Kediri City.
2.2. Setting and Samples
The sample in this study were all menopause women with hypertension who were in a Public Health Center in Kediri City. To reduce participant bias, researchers determined inclusion and exclusion criteria, and separated the intervention group and control group based on region. The inclusion criteria in this study were menopause women suffering from high blood pressure, were in good health (stable) to be given therapy, had blood pressure of at least 140/90 mmHg, and were willing to be participants. Meanwhile, the exclusion criteria in this study were menopause women who had physical or cognitive impairments and illness/obstacles during the research process.
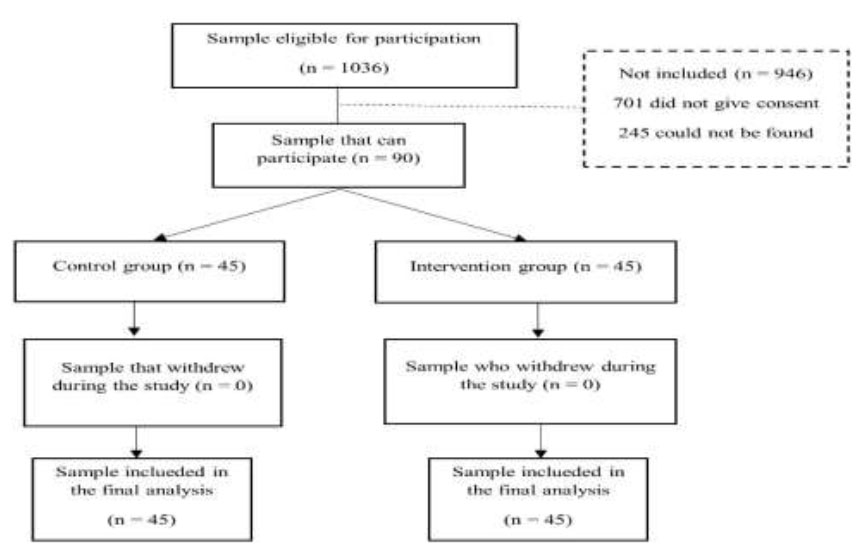
The number of samples that met the requirements of participants was 1036 menopause women. Among them, 946 were excluded with the details that 701 would not give consent and 245 people could not be found, so the participants included were 90 menopause women who were divided into 2 groups, namely the intervention group (45 participants) and control group (45 participants) who fit the inclusion criteria. In this case, this study used simple random sampling (Fig. 1).
2.3. Intervention (Applies to Experimental Studies)
Data collection was carried out by collecting participants at the Integrated Service Post in Ngadirejo Village area in the intervention group (45 participants) and the Integrated Service Post in Semampir area in the control group (45 participants). After that, the researcher explained the objectives, benefits, and implementation procedures of the study and provided informed consent for proof of consent to become a respondent. In this case, the respondents of both groups filled their data and participated in the pretest of blood pressure measurements using a digital tensimeter (media tech). Roselle extract (Hibiscus sabdariffa) 1x500 mg in capsule form was given for 5 consecutive days in the intervention group. Capsules were taken at 8 to 9 am at least 30 minutes after food intake.
Meanwhile, the control group was not given intervention but received standard care in the form of captopril of 12.5 mg and nifedipine of 10 mg. After 5 days of intervention, the researcher conducted a posttest, namely checking blood pressure using a digital tensimeter (Meditech) and the examination results on the participants' observation sheets in both groups were recorded. After all the data were collected, the data were processed and analyzed.
The effect of roselle (hibiscus sabdariffa) on blood pressure in menopause women in the public health center working area of Kediri city [20].
2.4. Measurement and Data Collection
Data was measured using a Mediatech brand digital tensimeter and collected by the researchers.
2.5. Data Analysis
Since there were more than 30 participants in the normality test, Kolmogorov Smirnov was used. If the sig value is more significant than 0.05, the data is normally distributed; if it is less than 0.05, the data is not normally distributed. In this case, the Lavane homogeneity test was employed in this investigation. The premise of decision-making was that if the data group originated from a population with the same variance (homogeneous), as indicated by the significant value of sig. > 0.05, then the data group originated from a population with different variances (heterogeneous). Only each variable was described using univariate analysis. Data on demographic status, including age, occupation, level of education to date, and blood pressure, were investigated in this study. When two variables needed to be evaluated, bivariate analysis was employed. The independent sample t-test measured the difference between the two groups, and the paired sample t-test was the statistical test employed. SPSS version 26.0 was used to analyze the data.
2.6. Ethical Considerations
The Helsinki Declaration was followed in evolving human subjects in the study. The ethical permit used was based on four basic principles of research ethics: Respect for persons (others), beneficence, which is the principle of doing good, and non-maleficence by reducing harm to subjects and protecting subjects. Informed consent was obtained from the participants for this study. Justice emphasizes that everyone deserves something according to their rights regarding distributive justice and balanced distribution (equitable). The ethical submission number at the Health Polytechnic of Ministry of Health of Malang Research Ethics Commission was No.DP.04.03/F.XXI. 31/878/2023.
3. RESULTS
The results of the characteristics of 90 participants involved, namely menopause women with hypertension, were divided into two groups: an intervention group and control group.
| Characteristics | Group | P-Value | |||||||
|---|---|---|---|---|---|---|---|---|---|
| (n = 45) Intervention Group |
(n=45) Control Group |
||||||||
| F/M | %/SD | F/M | %/SD | ||||||
| Age | 64.22 | 100% | 68.08 | 100% | 0.068a | ||||
| Education | - | - | - | - | 0.501a | ||||
| 1. Elementary | 26 | 57.7% | 25 | - | 55.5% | ||||
| 2. Secondary | 13 | 28.8% | 11 | 24.4% | - | ||||
| 3. Tertiary | 6 | 13.3% | 9 | 20% | - | ||||
| Job Status | - | - | - | - | 0.264a | ||||
| 1. Employed | 21 | 46.6% | 25 | 55.4% | - | ||||
| 2. Unemployed | 24 | 53.3% | 20 | 44.4% | - | ||||
| Hypertension | - | - | - | - | - | ||||
| • Systolic | - | - | - | - | 0.90b | ||||
| • Diastolic | - | - | - | - | 0.720 b | ||||
| 1. Stage 1 hypertension | 21 | 42.6% | 33 | 73.3% | - | ||||
| 2. Stage 2 hypertension | 24 | 53.3% | 12 | 26.7% | - | ||||
| Blood Pressure | Intervention Group (n=45) | P-Value | |
|---|---|---|---|
|
Pretest F(%) |
Posttest F(%) |
||
| Normal | 0 (0%) | 1 (2.2%) | - |
| Pre Hypertension | 0 (0%) | 11 (24.4%) | - |
| Stage 1 hypertension | 21 (46.7%) | 19 (42.2%) | 0.000 |
| Stage 2 hypertension | 24 (53.3%) | 14 (31.1%) | - |
| Total | 45 (100%) | 45 (100%) | - |
Based on the details in Table 1, the average age of participants from the intervention group is 64.22 years old, while the average age of the control group is 68.08 years old. Based on the latest education, most participants in both the intervention group and control group have primary level education with 51 participants (56.6%). Based on employment, most participants in the intervention and control groups were employed totalling to 46 participants (51.1%). The level of hypertension in the intervention group was dominated by stage 2 hypertension with a total of 24 participants (53.5%) and the control group was dominated by stage 1 hypertension with a total of 33 participants (73.3%).
Based on Table 2, it can be seen that in the pretest, the majority were in stage 2 hypertension by 24 participants (53.3%) and in the posttest, the majority were in stage 1 hypertension by 19 participants (42.2%).
Based on Table 3, regarding the results of hypertension analysis in the intervention group, data shows that the average systole at the pretest in the intervention group was 163.244 mmHg and the average diastole was 153.31 mmHg. In comparison, the average systole at the posttest in the intervention group was 101.84 mmHg and the average diastole was 87.09 mmHg. Based on the average pretest and posttest, data shows that there was a decrease in blood pressure in the intervention group. The paired t-test results on blood pressure for the intervention group showed significant results with p-value of 0.000. It can be concluded that blood pressure in hypertensive patients decreased after being given rosella extract in the intervention group.
Based on Table 4 regarding the frequency distribution of blood pressure in the control group, it can be seen that at the pretest, most participants were in the stage 1 hypertension category with 33 participants (73.3%), and at the posttest, most participants remained in the stage 1 hypertension category with 20 (44.4%) participants.
Based on the results of hypertension analysis in the control group as shown in Table 5, the average systole in the pretest in the control group was 153.76 mmHg and the average diastole was 95.44 mmHg. Meanwhile, the average systole at posttest in the control group was 151.51 mmHg and the average diastole was 97.82 mmHg. Based on the mean pretest and posttest score, data shows that there was no significant decrease in blood pressure in the control group. The paired t-test results on blood pressure for the control group showed significant results with p p-value of 0.251. Hence, it can be concluded that blood pressure did not decrease significantly after being given rosella extract in the control group.
| Variable | Intervention Group (n=45) | P-Value | |
|---|---|---|---|
| Pretest | Posttest | ||
| Mean±SD | Mean±SD | ||
| Systolic | 163.244 ± 18.548 | 101.84 ± 10.675 | 0.000 |
| Diastolic | 153.31 ± 19.878 | 87.09 ± 14.077 | 0.000 |
| Blood Pressure | Control Group (n=45) | P-Value | |
|---|---|---|---|
|
Pretest F(%) |
Posttest F(%) |
||
| Normal | 0 (0%) | 0 (0%) | - |
| Pre Hypertension | 0 (0%) | 9 (20%) | - |
| Stage 1 hypertension | 33 (73.3%) | 20 (44.4%) | 0.000 |
| Stage 2 hypertension | 12 (26.7%) | 16 (35.6%) | - |
| Total | 45 (100%) | 45 (100% | - |
| Variable | Control Group (n=45) | P-Value | |
|---|---|---|---|
| Pretest | Posttest | ||
| Mean±SD | Mean±SD | ||
| Systolic | 153.76 ± 14.869 | 151.51 ± 14.491 | 0.279 |
| Diastolic | 95.44 ± 3.882 | 97.82 ± 10.859 | 0.132 |
| Variable | Intervention Group | Control Group | P-Value | ||
|---|---|---|---|---|---|
| (n=45) | (n=45) | ||||
| Mean | ±SD | Mean | ±SD | ||
| Systolic | 101.84 | ±10.675 | 151.51 | ±14.491 | 0.000 |
| Diastolic | 87.09 | ±14.077 | 97.82 | ±10.859 | 0.000 |
Based on Table 6, in order to determine the difference in blood pressure in the two groups, namely the intervention group and the control group, after being given roselle and standard care, an independent sample t-test was conducted. The analysis results showed that the mean post-test systole in the intervention group was 101.84 mmHg and the mean diastole was 87.09 mmHg. Meanwhile, the mean posttest systole in the control group was 151.51 mmHg and the mean diastole was 97.82 mmHg. The results of the independent sample t-test test on blood pressure in both groups showed significant results with p p-value of 0.000. This shows that there is a difference in blood pressure in both groups after getting roselle and standard care.
4. DISCUSSION
The results showed some differences between the two groups. The average age of participants from the intervention group was 64.22 years old and the control group was 68.08 years old. Previous research found that women above 61 years old are at risk of hypertension due to arterial stiffness [21]. Age-related increases in blood pressure occur most quickly in those over 60. Compared to diastolic hypertension, systolic hypertension is more closely linked to cardiovascular illness and is more common in older adults [22]. Blood pressure rises as someone ages.
Based on the characteristics of participants in terms of their last education, most are primary education graduates. Global cardiovascular risk was greater in the less highly educated sample. This could be due to poor communication between doctors and patients or a lack of risk perception by patients. Finally, lack of education may adversely affect selfish behavior or access to health care [23]. Conversely, a study carried out in Nepal revealed that the prevalence of hypertension is twice as high in higher education or wealthier categories than in low-income and unemployed groups. This is because Nepal has experienced an epidemiological shift and has adopted unhealthy lifestyle choices associated with urbanization; additionally, early-stage economic development raises the risk of hypertension, particularly in highly educated and wealthier populations. Those living in rural areas tend to consume processed foods containing high fat and lead a sedentary lifestyle, which affects the risk of cardiovascular disease [24].
Based on the characteristics of participants in terms of occupation, the majority of both groups were employed. In previous studies, it was mentioned that there was an association between working as a housewife and the incidence of hypertension; women who were unemployed or housewives were at higher risk of suffering from hypertension compared to women who were employed. This may be due to the lack of activity done by housewives. Elevating one's cardiorespiratory fitness and engaging in moderate to intense physical activity, particularly aerobic exercise, can drop blood pressure and decrease the prevalence of hypertension. By lowering vascular resistance and repressing the sympathetic nervous system and the renin-angiotensin system, physical activity lowers the risk of hypertension. Heart rates are often higher in those who are not physically active. The heart has to work harder to contract at a higher heart rate, which also increases the strain on the artery wall [25].
Based on Table 2, the average blood pressure systole decreased by 61.404 mmHg, while diastole decreased by 66.22 mmHg. Hence, it can be concluded that blood pressure has decreased after being given an intervention in the form of rosella extract (Hibiscus sabdariffa) to menopause women. In a previous study in Iraq, 76 participants who were involved in the intervention group were given 10 mg of roselle extract for 6 weeks, while the other 45 participants who were in the control group did not receive any treatment. It was found that there was a difference in the average decrease in systole of 23.1 mmHg and diastole of 12.0 mmHg, while for the control group, there was only a decrease in systole of 4.4 mmHg and diastole of 3.6 mmHg [26].
In another study, 42 participants in the intervention group consumed rosella extract by 320 mg 2 x 1 for 28 days with 41 participants who took the antihypertensive drug ramipril 5 mg/day experienced a decrease in blood pressure by 11.2 mmHg (systolic) and 6 mmHg (diastolic), and for the ramipril user group there was a decrease of 16 mmHg (systolic) and 5 mmHg (diastolic) [16]. This shows that consuming roselle is effective for treating hypertension. Roselle is effective for lowering blood pressure because it contains anthocyanins, which function to lower blood pressure. Anthocyanins in roselle flowers can inhibit the oxidation of low-density lipoprotein (LDL), which can reduce the process of atherosclerosis in blood vessels [17]. In addition, the decrease in blood pressure by anthocyanins is associated with a decrease in ACE anthocyanins provide antihypertensive effects through the inhibition of angiotensin converting enzyme II (ACE) into a vasodilating effect that acts directly on the smooth muscle of arterial vessels by stimulating or activating endothelium-derived relaxing factor (EDRF) [27].
The flavonoid content in Hibiscus sabdariffa flowers that plays the most role is anthocyanins. Anthocyanins will accumulate in endothelial cells and can protect endothelial cells from the influence of free radicals, to maintain Nitric Oxide Synthase (NOS) as a powerful vasodilator. Oxidizing stress can reduce the bioavailability of Nitric Oxide Synthase (NOS) so that the blood vessel relaxation response [28]. Anthocyanins can reduce blood pressure through the mechanism of maintaining endothelial function through increasing Nitric Oxide Synthase (NOS) because anthocyanins can act as antioxidants so that they can overcome oxidative stress [29].
Several studies explained that roselle is an herb that has the potential for treating hypertension, so it is necessary to test its antihypertensive activity to determine the dose of its use for humans that can provide optimal effects. A dose of 250 mg/kg of dried roselle extract has antihypertensive activity with a systole inhibition presentation of 27.74% and diastole of 33.18%. The dose conversion to humans that produces a blood pressure-lowering effect is 2.8 grams/70 kg or 40 mg/kg [30]. In this study, researchers relied on the dose that has been regulated in the Regulation of the Minister of Health of the Republic of Indonesia Number 6 of 2016 concerning the Indonesian Herbal Medicine Formulatorium, namely 1 x 1 capsule (500 mg extract) per day. However, other results found that there was insufficient evidence to determine the effectiveness of roselle compared to placebo for controlling blood pressure in people with hypertension. This is due to methodological limitations, imprecision, and unsustainability [31].
The similarities of the above studies are the administration of roselle with extract preparations and using a sample size of more than 30 people. The difference is in the weight of the extract preparation and the duration of the intervention. According to the theories described above, it can be concluded that systolic and diastolic blood pressure after being given rosella (Hibiscus sabdariffa) decreased compared to before being given to the intervention group.
Table 3 shows that the average systolic blood pressure increased by 1.91 mmHg and diastolic blood pressure decreased by 6.77 mmHg. It can be concluded that the decrease in blood pressure in menopause women is not significant. There are several non-pharmacological ways to lower blood pressure using hypertension exercises. Hypertension exercises that are done regularly with certain movements can affect blood pressure. A study conducted in 2020 stated that there was an effect of giving hypertension exercises on blood pressure in the elderly [32].
Consuming foods with high fat content and excessive portions can increase cholesterol levels, which result in disturbances in blood vessels and an increase in blood pressure. An unhealthy diet can cause high blood pressure to increase because foods that are high in sodium and high in fat with large portions or more than needed are consumed. Foods high in sodium and fatty foods will cause fat in the body to accumulate and result in obstructed blood flow. Blood cannot flow to the heart due to the accumulation of fat. The accumulation of fat results in high blood pressure called hypertension. Dietary Pattern 2 is associated with higher blood pressure and thus chronic disease risk, supporting evidence that diets high in energy and sodium and low in potassium from vegetables and dairy products are detrimental to heart health [33].
Plant-based diets are among the suggested diets; American research involving 21,604 participants indicates that vegetarian diet intake is linked to lower average blood pressure than omnivore diet consumption. Furthermore, compared to meat eaters, vegetarians and vegans had reduced blood pressure, according to the study. Compared to non-vegetarians, vegans had mean systolic and diastolic blood pressure values that were 6.8 mm Hg and 6.9 mm Hg lower, respectively, after controlling for gender and age [34].
The similarity of the above studies is that they did not provide pharmacological interventions, but were limited to complementary interventions. The difference is that each study had different types of interventions ranging from gymnastics to dietary modifications. According to the theories described above and the results of the research, the researchers concluded that the mean blood pressure of systole and diastole decreased but not significantly in the control group after being given standard care.
Table 6 shows that the intervention group's mean systole blood pressure was 101.84 mmHg and its mean diastole blood pressure was 87.09 mmHg, whereas the control group's mean systole blood pressure was 155.67 mmHg and its mean diastole blood pressure was 88.67 mmHg. After giving rosella to women going through menopause, it may be stated that there is a difference in blood pressure in both groups.
Rosella (Hibiscus sabdariffa) is a plant widely known and utilized in various countries including Indonesia. For Indonesia, rosella flowers are more widely known as flowers that can be used as raw materials for making herbal tea or, in some areas, referred to as red tea. Various anti-oxidant contents contained in roselle petals make tea derived from roselle have many benefits, one of which is being a diuretic. The general mechanism of medicinal plants provides a dilating effect on blood vessels and inhibits angiotensin-converting enzymes (ACE). Inhibition of the renin-angiotensin system may reduce the ability of the kidneys to increase blood pressure [35].
Angiotensin II, ACE, and aldosterone plasma levels were significantly lowered by both cold and hot extracts, according to the findings of an Egyptian study that aimed to establish the optimal aqueous extraction technique for hibiscus sabdariffa antihypertensive metabolites and validate the plant's antihypertensive potential in vivo. Additionally, both extracts were found to have improved results concerning iNOS (inducible nitric oxide synthase) and eNOS (endothelial nitric oxide synthase) in the myocardium and aorta, as well as increased plasma NO levels. These findings may indicate a potential antihypertensive effect [36].
A previous study was conducted in Nigeria involving 75 participants who were divided into three groups, namely group A given a placebo of 150 mg/kg/day once a day after breakfast for four weeks, group B given lisinopril 10 mg/kg/day given orally once a day for four weeks, and group C given Hibiscus sabdariffa water extract 150 mg/kg/day orally once a day after breakfast for four weeks. In this case, researchers used a double-blind controlled randomized clinical method with a pretest and posttest controlled group design. The results of the study of roselle petals managed to achieve a 76% reduction in blood pressure to normal levels while Lisinopril reached 65%. Roselle petals significantly reduced systolic blood pressure at week 2, week 3-4, while lisinopril significantly reduced systolic blood pressure only at week 4. As for the effect of roselle petals on diastolic blood pressure, it was significant at weeks 3-4 compared to placebo but not significant when compared to each other throughout the study. The results showed that roselle petal extract was more significant in reducing systolic blood pressure with lisinopril in patients with mild to moderate hypertension. In contrast, the results on diastolic blood pressure were more significant at weeks 3-4 compared to the placebo group.
The similarity of the above study is that the administration of roselle, together with pharmacological interventions, has the most significant results. The difference is the type of antihypertensive treatment given. According to the theories described above and the results of the study, the researchers assessed by looking at the average and the results of the analysis of the two groups, namely the intervention and control groups; where it can be concluded that there is a significant difference in blood pressure in the two groups after receiving rosella (Hibiscus sabdariffa) intervention in menopause women.
5. IMPLICATION AND LIMITATIONS
Based on the results of the study, several implications can be used for improvement in the field of midwifery, including that health workers must be able to increase information about alternative treatments for high blood pressure and anxiety so that this research can be used as a reference for health worker intervention actions to provide information to sufferers of high blood pressure, especially in menopause women. In addition, it is a document and material to increase knowledge for midwifery students regarding the administration of rosella (Hibiscus sabdariffa) to high blood pressure in menopause women. The limitations of this study were that the pretest data collection was carried out in the middle of the month so that almost all Integrate Health Service Posts (Posyandu) activities had been carried out. Hence, the data collection was carried out door to door so it was not efficient in time and energy. In addition, due to the large number of participants and inadequate research personnel, the post-test data collection was carried out at a different time, so it might cause bias in the results.
In addition, this study did not observe and deepen the biomarker of high blood pressure in the elderly, namely the lack of the hormone estrogen. So, it is hoped that further research can be conducted to review whether roselle affects estrogen levels in menopause women.
CONCLUSION
Based on the analysis of the results and discussion of the administration of rosella (Hibiscus sabdariffa) against hypertension in menopause women, it can be concluded that the systole and diastole blood pressure of hypertensive patients decreased after the provision of rosella (Hibiscus sabdariffa) and standard care. In this case, menopause women can consume 500 mg of roselle (Hibiscus sabdariffa) extract per day as an additional treatment to lower blood pressure more effectively.
LIST OF ABBREVIATIONS
| ACE | = Angionteni Converting Enzyme II |
| EDRF | = Endothelium-Derived Relaxing Factor |
| LDL | = Low-density Lipoprotein |
| NOS | = Nitric xide Synthase |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by the Health Polytechnic of the Ministry of Health of Malang, Research Ethics Commission, Indonesia. The ethical submission number is No.DP.04.03/F.XXI.31/878/ 2023.
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.

