All published articles of this journal are available on ScienceDirect.

Awareness and Knowledge of Congenital Cytomegalovirus as an Agent of Hearing Loss: A Descriptive Evidence from Nigeria
Authors Info & Affiliations
Abstract
Background
Neonatal hearing loss has become a serious public health concern over the last two decades, largely because of the increasing number of reported cases associated with prelingual causes.
Objective
This study provided a descriptive report on the awareness and knowledge of congenital cytomegalovirus (cCMV) as a causative agent of hearing loss in the Nigerian population.
Methods
The study adopted a multistage sampling procedure. Data generation for analysis was achieved using a structured research questionnaire. A questionnaire on the issue of cCMV and hearing disability was sent to a total of 324 relevant stakeholders, and 324 completed questionnaires were received in return. The data was carefully coded and analyzed using descriptive and inferential statistical procedures.
Results
Experience sharing among professional colleagues, particularly those in the healthcare sector, remains the major source of information about cCMV in Nigeria. A significant association was found between the respondents’ professional work experience, organizational type, highest educational qualifications, and awareness and knowledge of cCMV. No predictive likelihood could be established between gender differences (male or female), organizational type (private or public), and awareness or knowledge of cCMV.
Conclusion
Information from and experience sharing among professional colleagues, family and friends and through the internet were major sources of information about cCMV in Nigeria. Work experience, organizational type, and educational qualifications determine the level of awareness and knowledge about cCMV in Nigeria.
1. INTRODUCTION
Several studies on cultural and religious ideologies have revealed that many people believe that ailments, illnesses, and disabilities occur as a result of ancestral curses or ‘punishments’ by deities or gods [1-3]. The authors of this study assumed that these superstitious belief systems could have changed based on the recent coronavirus pandemic and thus also assumed that any changes in peoples’ superstitious beliefs about the causes of disabilities or illnesses could advance the assumptions of the health belief model (HBM) [4, 5]. According to the HBM, an individual’s perception of their health is influenced by their general health values, which include concern and interest in their health, specific health beliefs about their vulnerability to a particular health threat, and their beliefs about the consequences of the health problem. In line with the foregoing statement, a Nigerian common man’s concept of a ‘virus’ is based on the effects of COVID-19, and they conceptualize a virus as potentially deadly and a threat to the well-being of an individual. Although there is a growing awareness of the importance of healthy living among Nigeria’s population of over 220 million, the rise in the population of those with pre-lingual and post-lingual hearing loss is rapid [6, 7]. Hearing loss is a heterogeneous condition that affects the sensitivity of the organ of hearing that collects and processes sound signals for adequate interpretation of such signals into meaningful sounds.
Individuals with hearing loss thus have significant difficulties responding to auditory-verbal stimuli through the organ of hearing [8]. There is as yet no categorical evidence that assertively states the number of people with hearing loss in Nigeria, but existing studies have shown that hearing loss in Nigeria, as in many countries in Sub-Saharan Africa, is caused by various factors. Such causative factors include, but are not limited to, infections of the middle ear, diseases such as measles and meningitis, and ototoxicity. While these remain the major causative factors, there are also causative factors of genetic origin [9-12]. Research evidence has increasingly linked hearing loss to viral infections. For instance, COVID-19 has been linked to progressive post-lingual hearing loss and neonatal (pre-lingual) hearing loss [13-19]. There is ongoing research on the association between COVID-19 and hearing loss.
Neonatal hearing screening is being advocated for in Nigeria, but the role of congenital cytomegalovirus (cCMV) in neonatal hearing loss is yet to be given the required attention. According to a patient information factsheet published by University Hospital Southampton (UHS), cytomegalovirus (CMV) is a common virus among humans [20]. As stated in the patient information factsheet, cytomegalovirus is usually harmless, but it shares similar characteristics with herpes, which can cause painful blisters, ulcers, cold sores, and chickenpox. Despite being usually harmless, UHS, as well as Gupta and Shorman, states that CMV is a life-threatening viral infection in immunocompromised patients [20, 21].
CMV is characterized by a large, complex, double-stranded DNA genome, and Louten and Singh and Gaidhane reported that CMV infection is usually asymptomatic, ubiquitous, and relatively common among women of reproductive age [22, 23]. Transmission of CMV is said to occur both vertically and horizontally. Vertical transmission of CMV infection occurs through direct contact with infected body fluids, while vertical transmission occurs from mother to child via the placenta (congenital CMV [cCMV] infection), during childbirth, or through breast milk [21, 22, 24]. The increasing number of cases of cCMV has become a serious public health concern over the last two decades, largely because of the increasing number of reported cases of hearing loss in infants [23]. Existing studies have reported that sensorineural hearing loss is commonly associated with cCMV, and some studies have established that variability exists in the types and severities of hearing loss linked to cCMV [24-28]. According to Aldè et al., the approximate prevalence rate of cCMV infections among infants is 0.6% in various developed countries [29].
Data obtained from a cohort study indicates that cCMV occurs in 3 to 12 newborns per 1000 in Canada, Europe, and the United States [30]. While Bates et al. have remarked that cCMV has not been given the research attention needed in Sub-Saharan African countries, some published studies have noted the presence of cCMV in live births [31]. For instance, a study conducted by Schopfer et al. in Ivory Coast reported a prevalence of 1.4% in a cohort of 2032 neonates, while another study in the Gambia by Bello and Whittle recorded a prevalence of 14% among live births [32, 33]. A follow-up study by van der Sande et al. [34] later reported the prevalence of cCMV in 5.4% of the live births in the Gambia. Pathirana et al. [35] found a prevalence rate of 1.4% among HIV-unexposed infants from low-middle-income households in South Africa. In Nigeria, while a few studies have found the occurrence of CMV leading to hearing loss in children, there is yet no comprehensive statistical report on the prevalence of hearing loss due to CMV in Nigeria. However, Olusanya et al. [36-49], in a study that screened and tested 263 neonates in Lagos, Southwest Nigeria, found that about 10% of the infants with hearing loss had CMV as an etiological factor. In another study conducted in North Central Nigeria, Usman et al. [50] noted that CMV infection accounts for about 10-15% of factors that cause neonatal hearing loss in Kaduna State, with a percentage ratio of about 45.5% males and 54.5% females. Based on their findings, Olusanya et al. [49] and Usman et al. [50] advocated for public awareness about cCMV. Although since the publications of Olusanya et al. [48] and Usman et al. [49], there have been several developments in public health issues across Nigeria, the state of public health-related issues and a paucity of studies that measure the societal knowledge and awareness of cCMV in Nigeria are still a matter of concern. Thus, this study found it imperative to examine the extent of awareness and knowledge of cCMV infection as a causative agent of hearing loss in Nigeria. Therefore, the following research objectives guided the conduct of the study.
- To ascertain the sources of information or knowledge on congenital cytomegalovirus infection (cCMV) as an agent of hearing loss in the respondents of this study.
- To establish if there will be any significant association between the demographic characteristics of the respondents and their awareness and knowledge of cCMV.
- To determine the likelihood that the respondents’ gender differences and organizational types will be predictive of their knowledge and awareness of cCMV.
2. RESEARCH QUESTION
1. What are the sources of information or knowledge on congenital cytomegalovirus infection (cCMV) as the agent of hearing loss in the respondents of this study?
2. Is there a significant association between the demographic characteristics of the respondents and their awareness and knowledge of cCMV?
3. What is the likelihood that the respondents’ gender differences and organizational types will be predictive of their knowledge and awareness of cCMV?
3. LITERATURE REVIEW
Information available to individuals about hearing loss in Africa has largely been shaped by cultural and religious beliefs and ideologies [1, 3, 36]. However, Oyewumi and Adigun [36] suggested that the lack of adequate and necessary information about health issues may expose individuals to various health risks. Muldoon et al. [37] asserted that adequate information is required to advance awareness and knowledge of cCMV. In their study on physical therapists in the United States, Muldoon et al. [37] noted that information about cCMV was largely circulated within the workplace by word-of-mouth. The next most common source of information on the virus was the internet. Other sources of information were graduate schools, friends, and relatives.
Earlier studies on the sources of cCMV information available to pregnant women have underscored the relevance of web-based information [38-40]. Price et al. [39] found that most cCMV information was provided by physicians (e.g., obstetricians and pediatricians), and the information received from the physicians further prompted many pregnant women to search the internet for additional information about the virus and its effects. Price et al. [39] also found that a less frequently used source of information on the virus was direct communication with friends and family members. Contrary to the findings reported in the study by Muldoon et al. [37], Thackeray et al. [40] and Jeon et al. [41] showed that information about cCMV was largely obtained from healthcare professionals. Thus, while there is existing evidence on the sources of information on cCMV, it was noticed that there is no recent evidence that shows the current sources of information on cCMV available to various stakeholders dealing with the issue of hearing loss, particularly in Nigeria.
The general lack of awareness of the existence of cCMV and its effects on the sense of hearing, among the other potential dangers of cCMV in live births, has raised concern globally [29, 39, 41-44].
For example, Price et al. compared respondents’ knowledge of viral infections that posed a danger to foetuses and showed that about 75% of the non-Hispanic women who participated in their study were unaware of the existence of cCMV [39]. Jeon et al. [41] and Lazzaro et al. [44] also agreed that the level of awareness of cCMV was low. In their survey of 643 women, Jeon et al. [41] found that only 22% of their respondents had heard of cCMV. Jeon et al. [41] and Muldoon et al. [37] reported that increased levels of education, older ages, work experience, geographical location, and present or previous employment in the healthcare sector were directly proportional to increased awareness of cCMV. Jeon et al. [41] also showed that there was no significant difference in awareness of CMV among present or past daycare workers, based on income and race/ethnicity. In their study, which employed the multivariate logistic regression model for the analysis of data collected from 300 respondents, Doutre et al. [42] noted that gender and education level significantly predicted the level of awareness of cCMV. Doutre et al.’s [42] model showed that females had greater odds of awareness than males. Doutre et al. [42] also noted a significant association between the level of educational qualification and awareness of cCMV, and each unit increase in education had a greater predictive value for the odds of awareness of cCMV.
In agreement with the assumption of the HBM [4, 5], Adigun [10] and Wong et al. [5] affirmed that individuals’ perceptions of their health are informed by their general state of awareness. Adigun et al. [45] noted that the general level of awareness among the population of individuals who are deaf and have hearing issues has shaped their knowledge about COVID-19. In other words, Adigun et al. [45] asserted that awareness about a health condition is linked with the knowledge domain of the particular health condition. In terms of knowledge about cCMV, several studies have discussed the general population’s lack of knowledge about this congenital virus and its potential effects [29, 42, 43, 46], as knowledge about CMV appears to be limited to healthcare practitioners and women of reproductive age [37, 41-43, 46, 47]. The study by Baer et al. [48] at Baylor University, USA, also found significant differences in the level of knowledge about cCMV of healthcare students across the different years of study. The implication of this finding presented by Baer et al. [48] is that it points to the fact that a higher level of education is directly associated with a higher level of knowledge about the virus. Similar findings were reported in the studies by Doutre et al. [42], Muldoon et al. [37], and Price et al. [39].
Other studies have noted that informal education has a substantial influence on the knowledge gained about cCMV and its effects. For instance, women had increased knowledge about cCMV after exposure to health education materials in the study by Price et al. [39]. Price et al. [39] averred that respondents were more likely to adopt prevention behaviors based on the material provided, thereby reducing their risk of CMV infection. Similarly, knowledge about cCMV and its association with hearing loss was found to have improved significantly after 134 women (mean age = 34) read a health information leaflet presented to them by Lazzaro et al. (2019). Existing literature on cCMV and hearing loss has shown the absence of extensive investigation of the virus in developing countries like Nigeria. Hence, this current study descriptively assessed the awareness and knowledge of cCMV among samples of the population in Nigeria, and the HBM was used as the theoretical lens [4, 5]. This study was deemed important as it bridged the existing research gap and contributed to existing literature on the issues relating to cCMV and hearing loss.
4. MATERIALS AND METHODS
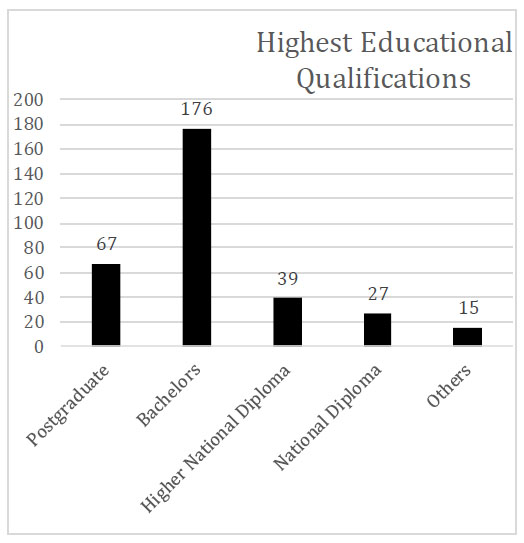
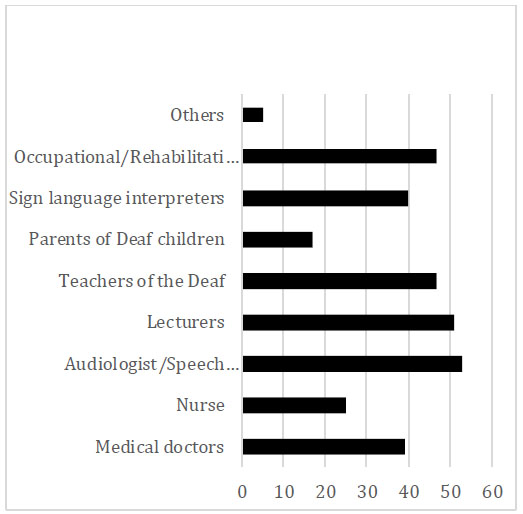
Design and respondents’ selection: This study was approached using the descriptive survey research design to assess the basic knowledge and awareness of cCMV in Nigeria. A multistage sampling technique was used [51] to select both the study location and the respondents. This study adopted the multistage sampling procedure because the cluster size was relatively large. At first, three states, namely, Lagos, Ogun, and Oyo, were purposively selected from the six states that make up the South-West region of Nigeria. Further, a simple random sampling procedure was adopted to sample 324 individuals who responded to the research instrument. The 324 respondents (Lagos = 26%, Ogun = 40%, and Oyo = 24%) were stakeholders (Figs. 1 and 2) in the issues of disability and health management. Participants in this study were selected based on their affinity with issues of hearing loss. Of these respondents, 87% were associated with the private sector and 13% were associated with the public sector. As shown in Fig. (1), the majority of the respondents in this study had a bachelor’s degree as their highest educational qualification, while 67 others had postgraduate qualifications. Further, Fig. (2) reveals the diverse professional affiliations of the respondents, which included medical doctors (n = 39), nurses (n = 25), and teachers of deaf children (n = 47). Data was also collected from 17 parents of deaf children across the three states in the South-West region of Nigeria.
5. MEASURES
A self-developed, closed-ended questionnaire was used for data collection. This data collection instrument was divided into four sections that collected relevant information on the respondents’ levels of knowledge and awareness of cytomegalovirus and hearing loss. Section A of the questionnaire comprised eight items that collected the relevant biographical information about the respondents. Section B comprised 12 items that inquired about their awareness of cCMV. Section C comprised six items that sought the knowledge of the respondents about cCMV, and Section D (8 items) sought information on the source of the respondents’ knowledge about cCMV. A sample statement in Section B was, “I have heard of the word ‘cytomegalovirus’”. The “human cytomegalovirus can be acquired congenitally by mother-to-fetus transmission during pregnancy and can cause disease” was one of the items in Section C of the questionnaire. A sample statement in Section D was, “I learned about cytomegalovirus through continuing education, e.g., a seminar, workshop, or conference”. Sections B to D were designed in a five-point Likert format of “1 = strongly agree, 2 = agree, 3 = undecided, 4, disagree and 5 = strongly disagree”.
6. INTERNAL CONSISTENCY AND PROCEDURE FOR DATA COLLECTION
Internal consistencies of the questionnaire were established using content validity for the correctness of the sentence structure of each of the test items. Split-half reliability testing was also conducted to further ascertain the reliability of the questionnaire. The overall reliability coefficient of the items on the questionnaire was 0.81. Data collection was achieved with the assistance of research assistants who were recruited and trained to assist the researchers. The locations of the research assistants were considered before they were recruited to ensure that they had easy access to the potential research respondents. All respondents were adequately briefed on the purpose of the study and the potential benefits of their candid responses. All respondents provided either verbal or written consent before they were allowed to respond to the questionnaire. They were all assured of their confidentiality and were given the option of voluntary withdrawal if they wished to withdraw at any point.
7. DATA ANALYSIS
The SPSS statistical package v22 was used to code the responses and analyze the data collected. Descriptive statistics involving the measures of central tendencies and bar charts were used to analyze the demographic data and provide the answer to research question one. The answer to research question two was provided with the use of Chi-square analyses, and the answer to research question three was obtained using binary logistic regression, with p < 0.05.
8. ETHICAL CONSIDERATION
The respondents voluntarily provided their informed verbal and written consent to participate in the study. The study was approved by the institution’s Institutional Review Board of the National University of Lesotho, Lesotho. Research and Ethics Committee (NULREC 59-20230612). In addition, all ethics of social sciences and humanities research adopted by the Declaration of Helsinki involving human subjects were strictly adhered to.
9. RESULTS
9.1. Research Question One
What are the sources of information or knowledge on congenital cytomegalovirus infection (cCMV) as an agent of hearing loss in the respondents in this study?
The following sources of information about cCMV as the agent of hearing loss were identified in this study: educational institutions; professional development programs such as workshops and seminars; personal reading of peer reviews and grey literature; audio-visual materials from various platforms; offline print media such as magazines and newspapers; semi-formal education; relevant information provided at religious organizations/ gatherings; and relevant information sharing and sharing of experiences during colleagues’, friends’, and families’ informal conversations. Conversations about cCMV and sharing of experiences about it among professional colleagues, friends, and families were the major sources of information for the study respondents (shown in Table 1); therefore, this source was ranked first. The second most prevalent source of information on cCMV was the respondents’ efforts to learn more about it through reading for professional development in research and thesis and dissertation writing.
The information on cCMV derived from social media platforms and through continued education were ranked third and fourth, respectively, in terms of the sources of information on CMV available to the respondents in this study. Information derived from coursework/modules in higher educational programs was ranked seventh and last as a source of information on cCMV available to the respondents. The findings thus implied that professional development, whether through personal or institutional/ professional effort, proved to be a substantial source of information on cCMV for those who participated in this study. The role of social media as a source of information on the virus was also well acknowledged by the study’s respondents. Based on the information sources as indicated in Table 1, it can be inferred that respondents had requisite knowledge about cCMV as an agent of hearing loss. Hence, they are aware of the potential effect of cCMV infection as a causative agent of congenital hearing loss.
9.2. Research Question Two
Is there a significant association between the demographic characteristics of the respondents and their awareness and knowledge of cCMV?
Table 2 provides an indication of the association between some of the demographic characteristics of the study’s respondents and their awareness and knowledge about cCMV. As shown in the table, the study established that a significant association existed between the respondents’ professional work experience (χ2 = 44.056; p < .05), work experience (χ2 = 7.444; p < .05), organizational type (χ2 = 12.029; p < .05), highest educational qualifications (χ2 = 12.159; p < .05), and their awareness of cCMV. This study similarly found a significant association between the respondents’ professional work experience (χ2 = 46.565; p < .05), work experience (χ2 = 11.037; p < .05), highest educational qualifications (χ2 = 10.760; p < .05), and the respondents’ knowledge of cCMV.
| I Learned about cCMV as a Causative Agent of Hearing Loss: | SA | A | U | D | SD | Mean | Std Dev | Rank |
|---|---|---|---|---|---|---|---|---|
| as a part of my course work in a higher institution. | 108 (33.3) | 162 (50.0%) | 10 (3.1%) | 25 (7.7%) | 19 (5.9%) | 2.03 | 1.09 | 7th |
| through continuing education e.g., seminars, workshops, conferences, etc. | 96 29.6%) | 142 (43.8%) | 25 (7.7%) | 49 (15.1%) | 12 (3.7) | 2.19 | 1.13 | 4th |
| through personal formal study e.g., research, thesis, and dissertation. | 80 (24.7%) | 168 (51.9%) | 17 (5.2%) | 40 (12.3%) | 19 (5.9%) | 2.23 | 1.13 | 2nd |
| through informal internet/online activities e.g., blog, YouTube, social media and television/radio broadcasts. | 75 (23.1%) | 168 (51.9%) | 31 (9.6%) | 31 (9.6%) | 19 (5.9%) | 2.23 | 1.09 | 3rd |
| through informal offline activities e.g., magazines and newspapers. | 92 (28.4) | 174 (53.7%) | 7 (2.2%) |
51 (15.7%) | 0 (0.0%) | 2.05 | 0.97 | 5th |
| through semi-formal education e.g., clinic day lecture, town hall meeting, public address. | 91 (28.1%) | 182 (56.2%) | 12 (3.7%) | 27 (8.3%) | 12 (3.7%) | 2.03 | 0.99 | 6th |
| through programs organized by religious organizations e.g., church, mosque, etc. | 94 (29.0%) | 186 (57.4%) | 12 (3.7%) | 25 (7.7%) | 7 (2.2%) | 1.97 | 0.92 | 8th |
| through colleagues, friends and families’ informal conversation and experience sharing. | 72 (22.2%) |
161 (49.7%) | 12 (3.7%) | 66 (20.4%) | 13 (4.0%) | 2.34 | 1.15 | 1st |
| Variables | Low Level of Awareness | High Level of Awareness | χ2 | Df | Sig | Low Level of Knowledge | High Level of Knowledge | χ2 | Df | Sig | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Profession | Medical doctors | 20 (51.3%) | 19 (48.7%) | 44.056 | 8 | .000 | 2 (5.1%) | 37 (94.9%) | 46.565 | 8 | .000 |
| Nurse | 0 (0.0%) | 25 (100%) | 0 (0.00%) | 25 (100.0%) | |||||||
| Audiologist/ Speech pathologist |
23 (43.4%) | 30 (56.6%) | 12 (22.6%) | 41 (77.4%) | |||||||
| Lecturers | 29 (56.9%) | 22 (43.1%) | 12 (23.5%) | 39 (76.5%) | |||||||
| Teachers of the Deaf | 28 (59.6%) | 19 (40.4%) | 26 (55.3%) | 21 (44.7%) | |||||||
| Parents of Deaf children | 23 (57.5%) | 17 (42.5%) | 10 (25.0%) | 30 (75.0%) | |||||||
| Sign language interpreters | 14 (82.4%) | 3 (17.6%) | 5 (29.4%) | 12 (70.6%) | |||||||
| Occupational/ Rehabilitation therapist |
29 (61.7%) | 18 (38.3%) | 20 (42.6%) | 27 (57.4%) | |||||||
| Others | 0 (0.0%) | 5 (100.0%) | 0 (0.0%) | 5 (100.0%) | |||||||
| Years of work experience | 0 – 5 years | 83 (58.9%) | 58 (41.1%) | 7.444 | 2 | .024 | 51 (36.2%) | 90 (63.8%) | 11.037 | 2 | .004 |
| 6 – 10 years | 15 (36.6%) | 26 (63.4%) | 8 (19.5%) | 33 (80.5%) | |||||||
| Above 10 years | 68 (47.9%) | 74 (52.1%) | 28 (19.7%) | 114 (80.3%) | |||||||
| Type of organization | Private | 32 (76.2%) | 10 (23.8%) | 12.029 | 1 | .001 | 11 (26.2%) | 31 (73.8%) | 0.011 | 1 | .917 |
| Public | 134 (47.5%) | 148% (52.5%) | 76 (27.0%) | 206 (73.0%) | |||||||
| Gender | Male | 70 (53.8%) | 60 (46.2%) | 0.593 | 1 | .441 | 35 (26.9%) | 95 (73.1%) | 0.001 | 1 | .981 |
| Female | 96 (49.5%) | 98 (50.5%) | 52 (26.8%) | 142 (73.2%) | |||||||
| Highest Qualification | Postgraduate | 22 (32.8%) | 45 (67.2%) | 12.159 | 4 | .016 | 12 (17.9%) | 55 (82.1%) | 10.760 | 4 | .029 |
| Bachelor’s degrees | 98 (55.7%) | 78 (44.3%) | 56 (31.8%) | 120 (68.2%) | |||||||
| Higher National Diploma | 24 (61.5%) | 15 (38.5%) | 12 (30.8%) | 27 (69.2%) | |||||||
| Nigeria Certificate of Education | 14 (51.9%) | 13 (48.1%) | 7 (25.9%) | 20 (74.1%) | |||||||
| Others | 8 (53.3%) | 7 (46.7%) | 0 (0.00%) | 15 (100.0%) | |||||||
No significant association was found between the respondents’ gender and their awareness of cCMV (χ2 = 0.593; p >.05) or between the respondents’ gender (χ2 = 0.001; p >.05), organizational type (χ2 = 0.011; p >.05), and their knowledge of cCMV. The findings presented in Table 2 indicate that gender had no observable significant influence on the respondents’ level of awareness or knowledge about cCMV. In addition, organizational type failed to show a significant influence on the extent of the knowledge that the respondents exhibited about the issues related to cCMV. The findings derived from the analysis provided in Table 2 motivated the next research question.
9.3. Research Question Three
What is the likelihood that the respondents’ gender differences and organizational types will be predictive of their knowledge and awareness of cCMV?
The authors wanted to know if there was any likelihood of the predictive potential of the dichotomous variables of gender (male and female) and the organizational type (private establishments and publicly funded establish- ments) on the respondents’ awareness and knowledge of cCMV.
A binary logistic regression analysis was adopted to ascertain the likelihood of predictive capacity and to provide a response to research question three, and all assumptions were checked and ascertained in this study. For instance, multicollinearity was confirmed, and the assumption of multicollinearity among the variables in the study was violated. The omnibus test of the model coefficients was also conducted to establish the fitness of the data to the model for the prediction of the predictive likelihood of the independent variables (gender differences and organizational type) on the dependent variables (awareness and knowledge of cCMV). The model was statistically significant (χ2(n = 324) = 435.952; p < 0.05) for awareness and knowledge (χ2(n = 324) = 248.145; p < 0.05) of cCMV. The foregoing statements imply that the model was capable of distinguishing between the independent and dependent variables.
The model was, however, able to explain between 1% and 2% of the Cox and Snell R2, as well as the Nagelkerke R2, for the variance in gender differences for awareness and knowledge of cCMV. The model was similarly able to explain 5% and 10% of the Cox and Snell R2, as well as the Nagelkerke R2, for the variance in organizational type for awareness and knowledge of cCMV.
| - | B | S.E. | Wald | Df | Sig. | Exp (B) |
95% C.I.for EXP(B) | ||
|---|---|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||||
| Step 1a | Awareness of cCMV | .007 | .013 | .305 | 1 | .581 | 1.007 | .982 | 1.034 |
| Knowledge of cCMV | -.001 | .033 | .001 | 1 | .974 | .999 | .937 | 1.065 | |
| Constant | .163 | .456 | .127 | 1 | .721 | 1.177 | - | - | |
| - | B | S.E. | Wald | Df | Sig. | Exp(B) | 95% C.I.for EXP(B) | ||
|---|---|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||||
| Step 1a | Awareness of cCMV | .029 | .023 | 1.556 | 1 | .212 | 1.029 | .984 | 1.077 |
| Knowledge of cCMV | -.045 | .051 | .787 | 1 | .375 | .956 | .865 | 1.056 | |
| Constant | 1.677 | .659 | 6.478 | 1 | .011 | 5.350 | - | - | |
Using the regression coefficients, the odds ratios (OR) for the independent variables as predictors were calculated as exponents (Exp). The exponents (Exp) were used to estimate the variation in the odds of membership in the dependent variable, that is, awareness and knowledge of cCMV (see Table 3). Further analysis of the binary logistic regression revealed whether gender difference had any predictive likelihood of predicting any change in the level of awareness (OR = 0.007, 95% CI [0.982, 1.034], p > .05) or knowledge (OR = -0.001, 95% CI [0.937, 1.065], p > .05) of cCMV. The organizational type was similarly assessed to see if it had any predictive likelihood of predicting any change in the level of awareness (OR = 0.029, 95% CI [0.984, 1.077], p > .05) or knowledge (OR = -0.045, 95% CI [0.856, 1.056], p > .05) of cCMV. The foregoing results implied that the level of awareness or knowledge derivatives of cCMV were not predicted by gender differences (male or female) or the organizational type (private or public). In other words, other factors, such as those confirmed by research question two, could be considered as major predictive factors.
10. DISCUSSION
Hearing loss is a condition that is usually noticed when two-way communication that involves an auditory-verbal exchange of words is required [8]. Globally, the presence of at least one individual with hearing loss is noticeable in every community. Thankfully, the heterogeneous nature of hearing loss has raised some degree of concern among relevant stakeholders. Several beliefs influence the social and emotional growth and well-being of individuals with hearing loss in communities, particularly in communities in Sub-Saharan African countries such as Nigeria [2, 3, 6, 11, 12]. Various superstitious beliefs about the etiology of hearing loss have regrettably worsened the psychosocial wellness of persons with hearing loss, especially those belonging to Nigeria’s rural and semi-urban communities [12]. However, such belief systems may have changed following the recent effects of the coronavirus pandemic. The etiology of hearing loss was associated with various causes prior to the emergence of COVID-19 [2, 6, 11, 12, 36], but little was said in Nigeria about the association between cCMV and hearing loss. This study, therefore, assessed the sources of information, awareness, and knowledge about cCMV and hearing loss in Nigeria.
Our findings regarding the sources of information on cCMV information indicated that sharing of experiences among professional colleagues, particularly those in the health care sector, remains the major source of information about cCMV, followed by discussions about the virus and its effects with friends and family members. It is suspected that such discussions within families and among friends can arise because of information shared by healthcare workers about suspected or identified cases of hearing loss in infants. This study also found that education through organized and informal institutions has significant potential to inform the populace about cCMV. Social media has also played a significant role in providing relevant information to the populace about cCMV.
This current study supports the evidence reported in the studies by Cannon et al. [38]; Jeon et al. [41]; Muldoon et al. [37]; Price et al. [39]; and Thackeray et al. [40]. The foregoing researchers showed that quality information about the origin and effects of cCMV in terms of hearing loss is available and shared in healthcare centers. The finding of this current study confirmed the assertion by Ogunkeyede et al. [6] that there has been an increase in the amount and type of health information available in Nigeria. The increase in the amount and type of health information in Nigeria presently can be linked to the rapid rise in health information made available during the ravaging COVID-19 pandemic and perhaps the increase in the government’s commitment to the health sector, as well as calls for an inclusive society in line with the government’s commitment to achieving the country’s Sustainable Development Goals.
This current study has added to existing literature that states that information about cCMV is being sought on various social media platforms. It is, however, assumed that the search for further information about cCMV on the internet may be motivated by prior information that the online information seekers may have obtained from healthcare facilities and healthcare professionals. Our finding of the internet as a source of information about cCMV corresponded with the finding reported by Muldoon et al. [37]. Muldoon et al. [37] also noted that information about cCMV was largely sourced within the workplace, followed by the internet. The respondents in Muldoon et al.’s [37] study reported that the other sources of information concerning cCMV were graduate schools, friends, and relatives. The finding of this study thus confirmed the report by Muldoon et al. [37]. The finding of this study also agreed with the evidence reported by Cannon et al. [38], Price et al. [39], and Thackeray et al. [40].
Research question two sought to determine the association between the demographic characteristics of the study’s respondents and their awareness and knowledge of cCMV. The findings showed that a significant association existed between the respondents’ professional work experience, their organizational type, highest educational qualifications, and their awareness of cCMV. The respondents’ awareness of cCMV could not be separated from their perceptions of it as individuals. The HBM assumed that the respondents in this study based their awareness and perception of cCMV on their observation of the emergence of hearing loss in infants [4, 5]. The respondents queried all of the causative factors responsible for the occurrence of neonatal hearing loss. The prevalence of neonatal hearing loss necessitates further investigation of the possibility of cCMV as the causative agent [29, 39]. Our findings, therefore, agreed with those of Jeon et al. [41], Kobayashi et al. [43], and Muldoon et al. [37].
This current study did not classify the level of awareness of cCMV, unlike previous studies that did so, and found that there was a low level of awareness among the various groups of study respondents [37, 39, 41, 43]. Despite the foregoing studies, this study ascertained that an increase in the years of work experience and education levels could positively influence the level of awareness about cCMV. This was previously also found by Doutre et al. [42], Jeon et al. [41], and Muldoon et al. [37]. This study found a significant association between the respondents’ professional work experience, their highest educational qualifications, and their knowledge of cCMV, but no significant association between their gender, organizational type, and knowledge of the virus. Earlier studies also revealed that knowledge about cCMV is still very low among the general populace, but professionals in the healthcare sector, women of reproductive age, and those with an educational qualification (in healthcare) have significantly more knowledge about this virus [29, 37, 41-43, 46-48].
Lastly, while this study’s findings agreed with those of Aldè et al. [29] and Baer et al. [48], we could not establish alignment with the findings reported by Doutre et al. [42] on the possible association between gender differences and knowledge about cCMV. Our study instead revealed that awareness or knowledge about cCMV could not be predicted by gender differences (male or female) or the organizational type (private or public establishment) of the respondents. In order words, there was no evidence that gender affiliation or place of work could define respondents’ levels of awareness and knowledge about cCMV. This current finding deviated from that of Doutre et al. [42], who reported a significant difference in the level of awareness and knowledge about cCMV between males and females. They found females to be two times more likely to be aware of and knowledgeable about cCMV than their male counterparts. Jeon et al. [41] also did not find that gender differences had predictive potential in this regard, but these authors did state that age differences could significantly predict the differential likelihood of an increase in awareness and knowledge about cCMV.
11. IMPLICATION OF FINDINGS FOR PUBLIC HEALTH POLICY AND INTERVENTIONS
The findings of this study underscore the need to scale up public health awareness as an approach to mitigate the effect of cCMV as a causative agent of neonatal hearing loss. Thus, the finding further is a testament to the fact that regular social sensitization of healthy living, genetic counseling and effective antenatal care is important as a measure to reduce the possibility of prelingual hearing loss in neonates. The implication of this study, therefore, provides support for existing studies that have advocated for recurrent public sensitization on the potential negative effect of late antenatal registration or self-care in Nigeria. It is, therefore, imperative that the Ministry of Health enforces the policy of neonatal hearing screening in Nigeria. To ensure the effectiveness of the enforcement of neonatal hearing screening in Nigeria, the Ministry of Health needs to work in synergy with the National Orientation Agency and other relevant mass media outlets. More importantly, professionals at all primary healthcare centers should be adequately equipped with the required instruments for ear screening.
12. RECOMMENDATIONS
Based on the findings, the expansive creation and dissemination of health information are recommended that center on the implications of cCMV for Nigerians. In other words, there is a need for all relevant governmental agencies, namely the Ministry of Health, Ministry of Women Affairs and Child Development, Ministry of Social Welfare, and the National Oriental Agency, at the federal, state, and local government levels to start intensive awareness and sensitization campaigns about cCMV and its potential to cause childhood disabilities such as pre-lingual hearing loss. In-service training is important for professionals in the health and educational sectors to increase their knowledge about the transmission and effects of cCMV. Such training should be monitored closely, and trainees should be subjected to intermittent evaluation of the knowledge gained.
It is strongly recommended that the information about cCMV be disseminated at the community level in order to reach secondary school learners and adults at schools, public venues, and places of worship. Radio and television programs can be used effectively to aid the dissemination of relevant information about cCMV to all Nigerians. It is believed that mass media can lead to improved societal awareness about the implication of CMV and, therefore, expand the knowledge of the populace about the implication of cCMV among infants and young children in Nigeria and beyond. Therefore, opportunities provided by mass media and the internet should be harnessed by government and development agencies to educate the Nigerian populace about congenital cytomegalovirus and its potential to cause hearing loss.
CONCLUSION
This study concluded that the sharing of experiences among professional colleagues, particularly those in the healthcare sector, remained the major source of information about cCMV in Nigeria. Discussion about cCMV among family members and friends and information on the internet (social media) also remain viable routes for information dissemination about the virus in Nigeria. This study established a significant association between the respondents’ professional work experience, the type of organization that they worked for (organizational type), their highest educational qualifications, and their awareness and knowledge about cCMV, but there was no predictive likelihood that gender differences (male or female) and their organizational type (private or public) impacted their awareness and knowledge about cCMV.
AUTHORS’ CONTRIBUTION
It is hereby acknowledged that all authors have accepted responsibility for the manuscript's content and consented to itssubmission. They have meticulously reviewed all results and unanimously approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| cCMV | = Congenital cytomegalovirus |
| CMV | = Cytomegalovirus |
| HBM | = Health Belief Model |
| UHS | = University Hospital Southampton |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was approved by the institution’s Institutional Review Board of the National University of Lesotho, Lesotho. Research and Ethics Committee (NULREC 59-20230612).
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institute and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
The respondents voluntarily provided their informed verbal and written consent to participate in the study.

