All published articles of this journal are available on ScienceDirect.

Effectiveness of the Health Education Intervention using Facebook and LINE on Intention to Reduce Alcohol Consumption among Entertainment Girls in Bangkok, Thailand: A Randomized Controlled Trial
Authors Info & Affiliations
Abstract
Introduction
The global concern of alcohol consumption among entertainment girls (En' Girls) requires targeted interventions to address this pressing issue. This study aimed to study the effectiveness of the health education program using Facebook and Line (instant messaging application) on intention to reduce alcohol consumption among En’ Girls in Bangkok, Thailand.
Methods
This study, conducted in Bangkok, Thailand from 2020 to 2021, employed a randomized controlled trial. Forty-four En’ Girls were randomly assigned to either the Facebook intervention or LINE control group. The 12-week health education intervention on Facebook included various media formats covering alcohol-related themes. LINE served as the control group with the same content as Facebook, excluding live broadcasts. Assessments at baseline, the 4th week, and the 12th week measured outcomes which were health knowledge, intention to reduce alcohol consumption, expected number of drinks per night, and the Alcohol Use Disorders Identification Test score. Baseline homogeneity was assessed with independent t-tests and chi-square tests, while changes were analyzed using Cochran's Q test and chi-squared test. Mean changes were compared with independent t-tests and repeated measures ANOVA. Statistical significance was determined at a significance level of P < 0.05.
Results
Over the 12-week period, the intervention group significantly improved health knowledge, intentions to reduce alcohol consumption, and the expected number of drinks per night compared to the baseline and control groups.
Conclusion
The findings of this study suggest lasting behavioral effects, underscoring the value of culturally tailored health interventions via social media for addressing global alcohol-related health issues.
1. INTRODUCTION
Light to moderate alcohol intake is often advised for its potential health benefits, including a lowered risk of various cardiovascular issues such as heart disease and ischemic stroke [1]. The consumption of alcohol, especially in excessive amounts, constitutes a significant risk factor for numerous health issues, contributing significantly to the global burden of disease [2]. Alcohol abuse is harmful and linked to more than 200 diseases and injuries. It is accountable for 3 million deaths a year, or 5.3% of all deaths globally.
Men drink more alcohol than women do on a global scale, and they are also linked to a higher rate of alcohol-related harm to others and themselves [3]. According to a study by GBD 2016 Alcohol Collaborators covering 195 countries and territories, global alcohol consumption in 2016 was 32.5%, with 25% of females and 39% of males being current drinkers [4]. It was also reported that this amounts to 2.4 billion global current drinkers, comprising 1.5 billion males and 0.9 billion females. In recent decades, alcohol consumption patterns among girls and women have shifted, revealing a paradox where, despite drinking less than men, women may experience greater harm even at lower alcohol levels, such as an increased risk of developing breast cancer, osteoporosis, heart disease, and reproductive issues, including infertility. This underscores the critical need for interventions tailored specifically to address alcohol-related risks among women [3, 5, 6].
The National Statistical Office of Thailand reported that the prevalence of alcohol consumption among individuals aged 15 and above was 28.4% in 2017 [7]. Following the implementation of the Alcohol Beverage Control Act B.E. 2551, alcohol advertising is prohibited in Thailand [8]. In response, beer companies and local establishments have devised alternative methods to market beer brands, utilizing beer promoters to reach customers [9]. The nightlife of Bangkok stands as a prominent feature in Thailand's tourism and entertainment sectors, underscoring the significance of tourists' perceptions of its overall image. International tourists perceive Thailand's nightlife as uniquely different from that of other countries. It extends beyond alcohol sales to include diverse entertainment options and various venues offer female entertainers known as “Entertainment Girls” or “alcohol promoters” to enhance the overall experience. This present study uses the word “En’ Girl” to entertain girls and alcohol promoters.
Because of the demands of their job and the city's nightlife, En’ Girls in Bangkok operate in an environment where heavy drinking is a common practice, especially during work hours. Targeted interventions that address their specific difficulties with alcohol intake are necessary because of the lack of health awareness and support resources available to them. Current literature on En' Girls in Thai nightlife is lacking including health knowledge and intention to reduce alcohol consumption, particularly in the context of Thailand's unique cultural and social dynamics. This study aimed to study the effectiveness of the health education program using Facebook and Line (instant messaging application) on intention to reduce alcohol consumption among En’ Girls in Bangkok, Thailand.
2. MATERIALS AND METHODS
2.1. Study Area
Bangkok, renowned as the global entertainment and party capital, was deliberately selected for this study due to its exciting nightlife, encompassing diverse options such as bars, restaurants, karaoke spots, and lounges that contribute to the vibrant city atmosphere. The En' Girl, often known as beer promoters or drink escorts, is a major player in the vibrant nightlife of Bangkok. These people add a special touch to the city's nightlife since they represent a special fusion of entertainment, hospitality, and companionship. These performers are essential elements of the whole experience, contributing significantly to the nature of Bangkok's drinking and nightlife culture and elevating the ambiance as guests mingle and engage.
2.2. Study Design and Study Period
This study, conducted from 2020 to 2021, utilized a randomized controlled trial with intervention and control groups to assess the effectiveness of a health education program using Facebook and Line on intention to reduce alcohol consumption among En' Girls in Bangkok, Thailand.
2.3. Participants
The targeted population comprised En' Girls employed in Bangkok. The inclusion criteria were (i) women aged between 18 – 35 years old, (ii) working fulltime in restaurants, bars, karaoke, clubs, lounges, or at a private place, (iii) excellent in reading, writing, listening and understanding Thai language, (iv) women who were willing to participate the study from the beginning until completing the project, (v) women who had their own active Facebook accounts and/or LINE, some created create new one and be able to use Facebook’s features and LINE on their own, (vi) women who were able to use social networking sites (Facebook, YouTube, and Messenger) either on mobile phone, PC or notebook., (vii) women who were able to access and to participate on the Facebook page for a proper time at least 30 minutes per visit as convenience time to get content and/or having activities which provided on Facebook/LINE, (viii) women who were willing to absorb the internet fees for using Facebook, LINE, YouTube and Goodgle Form. Women who failed to attend live sessions three sessions out of ten continuously and those who failed to respond to the test, questionnaire three times out of ten continuously were excluded.
2.4. Sample Size
This study utilized the G-power program to determine the necessary sample size for population estimation [10]. The calculated sample size was 18 for each group. To account for potential missing data, withdrawals, and loss to follow-up, 10% was added to the sample size, bringing the total to 20 individuals per group. A total of 22 persons participated in each group.
2.5. Intervention and Control Groups
The Facebook group was treated as the intervention group. The health education intervention transpired within the Facebook group named “EPC: Empowering Positive Choices”. The content on Facebook was organized into sessions, focusing on knowledge about alcohol consumption, encompassing both its advantages and disadvantages. The content structure included tiers of Alcohol Use Disorders Identification Test (AUDIT) scores, such as low-risk drinker, hazardous drinker, and harmful use. Utilizing an infographic pattern and video clips, the content featured diverse formats, including polls, textual content, images, videos, instant messaging, and live broadcasts. The program spanned 12 weeks, encom- passing various topics: understanding types of alcohol (Week 1), exploring alcohol-related diseases (Week 2 and 3), concluding session and posttest (Week 4), elucidating the harms of drinking alcohol (Week 5, 6, and 7), sharing personal experiences (Week 8), delving into a case study highlighting the detrimental effects of heavy drinking on one En' Girl (Week 9 and 10), a final interlude (Week 11), and summarizing the entirety of the 12 weeks (Week 12).
The line group served as the control group for the study. The content on LINE was organized into categories, including text, videos, and pictures, excluding live broadcasts, undergoing a 12-week program covering diverse subjects: alcohol types (Week 1), alcohol-related diseases (Week 2 and 3), posttest (Week 4), experience sharing (Week 5), understanding the harmful effects of heavy drinking (Week 6 and 7), further experience sharing (Week 8), engaging in discussions on a case study featuring an En' Girl (Week 9 and 10), a concluding interlude (Week 11), and summarizing the entire 12-week duration (Week 12).
2.6. Outcomes
The study assessed four main outcomes: (1) health knowledge, (2) intention to reduce alcohol consumption, (3) expected number of drinks per night, and (4) Alcohol Use Disorders Identification Test (AUDIT) score. All outcome measures were assessed at three-time points: baseline, the 4th week, and the 12th week. This structured evaluation schedule allowed for a comprehensive understanding of the changes in health knowledge, intention to reduce alcohol consumption, expected number of drinks per night, and AUDIT scores during the study.
2.7. Randomization
After confirming the eligibility of the En' Girls and securing informed consent, each participant was systematically assigned a unique number from 1 to 44. To ensure a randomized distribution, a computer-generated sequence was employed to allocate participants evenly between the education group and the control group [11, 12]. This rigorous randomization process aimed to minimize bias and facilitate a more robust evaluation of the intervention's impact on the respective groups.
2.8. Data Collection Tools and Procedure
The questionnaire consisted of six sections, covering (i) sociodemographic characteristics, (ii) work and drinking characteristics, (iii) health knowledge, (iv) intention to reduce alcohol consumption, (v) expected number of drinks per night and (vi) the AUDIT tool. The Health Knowledge questionnaire, which comprises 24 questions related to general knowledge about alcohol drinking, harms, and diseases, was developed using information from the Health Education Division of Thailand and previous literature [13-16]. Participants responded with “Yes,” or “No,” or “Not sure”. The intention to reduce alcohol consumption questionnaire, comprising 10 questions, used a Likert scale ranging from 1 to 5 to evaluate participants' intentions and practices in reducing alcohol consumption. It was developed based on previous literature [17-19]. The expected number of drinks question aimed to assess the anticipated number of drinks per night, allowing participants to respond in terms of glasses. The Alcohol Use Disorders Identification Test (AUDIT), a validated tool from the World Health Organization, was used to screen and identify individuals at risk of developing alcohol problems [20, 21]. This test included 10 questions, with responses rated on a Likert scale from 0 to 4.
The questionnaire sets underwent a thorough validation process involving four experts in the field, utilizing the Item-Objective Congruence (IOC) index [22]. To ensure reliability, assessments were conducted using both the KR-20 and Cronbach alpha coefficient, yielding satisfactory results. This rigorous validation process enhances the credibility and trustworthiness of the study's instruments.
The primary researcher and assistants conducted the data collection process. In preparation, the principal investigator and research assistants reviewed the questionnaires and discussed interview techniques, including rapport-building strategies. Data were collected at baseline, the 4th week, and the 12th week of the study period for both the intervention and control groups.
The study flow chart is shown in Fig. (1).
2.9. Data Analysis
Intention-to-treat (ITT) analysis was conducted in accordance with the study protocol. Categorical data were described using frequency and percentage, while continuous variables were interpreted by mean and standard deviation. To assess baseline homogeneity between intervention and control groups, independent t-tests and chi-square tests were employed for continuous and categorical data, respectively, with significance set at P < 0.05. Changes within and between groups were analyzed using Cochran's Q-test and the chi-squared test. To compare the mean changes in “intention to reduce alcohol consumption,” “expected number of drinks per night,” and “AUDIT” between control and intervention groups, independent t-tests were utilized, and repeated measures ANOVA was applied to examine changes within each group.
3. RESULTS
3.1. Socio-demographic Characteristics
Table 1 provides a comprehensive overview of the socio-demographic characteristics of the respondents. Notably, no statistically significant differences were observed between the intervention and control groups across these variables. In the intervention group, respondents averaged 24.9 years, while in the control group, it was 23.6 years. Most had vocational certificates, and the majority were single in both groups. Parental status differed, with more in the control group having children.
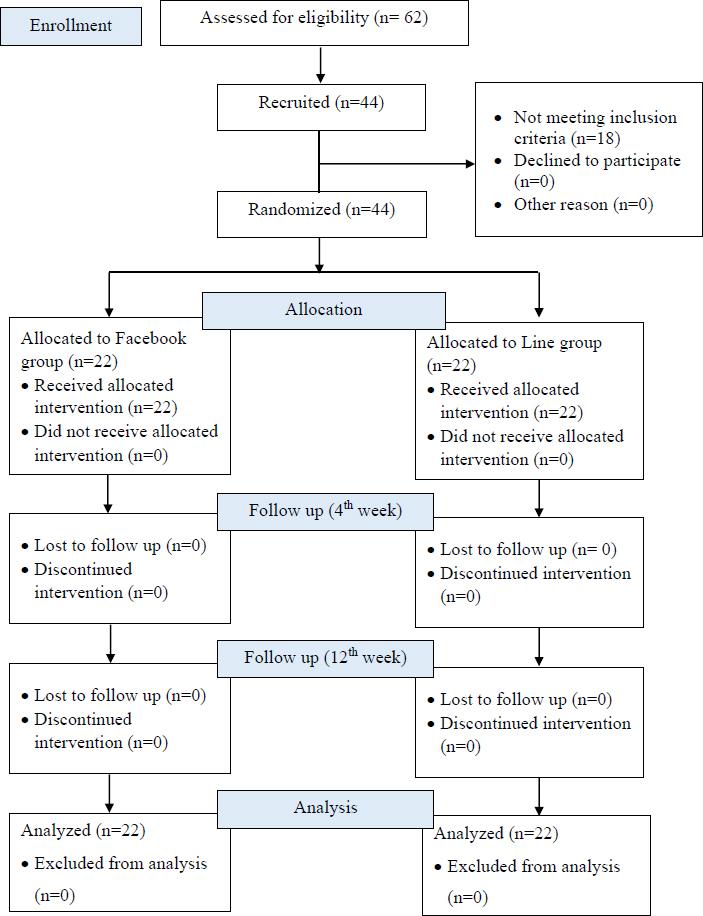
Study flowchart.
| Socio-demographic Characteristics |
Intervention (N=22) |
Control (N=22) |
P-value |
|---|---|---|---|
| N (%) | N (%) | ||
| Age | |||
| Mean ± SD (Min-Max) |
24.9 ± 3.9 (18-34) |
23.6 ± 3.6 (19-35) |
0.254 |
| Education | |||
| Middle school | 4 (18.2) | 5 (22.7) | 0.569 |
| High school | 1 (4.5) | 2 (9.1) | |
| Vocational certificate | 16 (72.7) | 12 (54.5) | |
| Bachelor degree | 1 (4.5) | 3 (13.6) | |
| Marital status | |||
| Single | 8 (36.4) | 10 (45.5) | 0.764 |
| Married | 4 (18.2) | 2 (9.1) | |
| Divorced/ Separated | 3 (13.6) | 2 (9.1) | |
| Boyfriend/ partner | 7 (31.8) | 8 (36.4) | |
| Having a child | |||
| Yes | 5 (22.7) | 10 (45.5) | 1.000 |
| No | 17 (77.3) | 12 (54.5) | |
3.2. Work and Drinking Characteristics
Table 2 provides a comprehensive overview of the work and drinking characteristics of the respondents. Notably, no statistically significant differences were observed between the intervention and control groups across these variables except “source of information for knowledge regarding alcohol drinking (p= 0.003)”. In the intervention group, En’ Girls started at 22.7 years, while in the control group, it was 22.1 years. Notably, more control group En’ Girl worked over 15 days per week, aimed for “3-5 years” in expected work duration, and consumed “11-20 glasses” per night (22.7%). Both groups reported health issues, and a higher proportion of control group members worked in nightlife venues.
|
Work and Drinking Characteristics (n= 44) |
Intervention (N=22) |
Control (N=22) |
P-value |
|---|---|---|---|
| N (%) | N (%) | ||
| Age of becoming En' girl | |||
| Mean ± SD (Min-Max) |
22.7 ± 5.48 17-25 |
22.1 ± 5.36 18-25 |
0.679 |
| Days of work per month | |||
| Less than 7 days | 8 (36.4) | 4 (18.2) | 0.344 |
| Between 8 and 15 days | 6 (27.3) | 6 (27.3) | |
| More than 15 days | 8 (36.4) | 12 (54.5) | |
| Expected years to work from now on | |||
| Less than 1 year | 0 (0.0) | 2 (9.1) | 0.069 |
| 1 - 2 years | 8 (36.4) | 9 (40.9) | |
| 3 - 5 years | 7 (31.8) | 10 (45.5) | |
| 5 years and above | 7 (31.8) | 1 (4.5) | |
| Amount of drinks per night (in glasses) | |||
| less than 10 | 6 (27.3) | 7 31.8) | 0.102 |
| 11 - 20 glasses | 11 (50.0) | 5 (22.7) | |
| 21 - 30 | 3 (13.6) | 2 (9.1) | |
| 31 - 40 | 2 (9.1) | 3 (13.6) | |
| more than 41 | 0 (0.0) | 5 (22.7) | |
| Health issues regardless of drinking | |||
| Yes | 22 (100.0) | 22 (100.0) | NA |
| No | 0 (0.0) | 0 (0.0) | |
| Work location | |||
| Self-management: private En'girl | 10 (45.5) | 5 (22.7) | 0.203 |
| Clubs, bars, restaurants, karaoke bars and lounges |
12 (54.5) | 17 (77.3) | |
| Source of information for knowledge regarding alcohol drinking | |||
| Social media (eg: Facebook) | 12 (54.5) | 2 (9.1) | 0.003* |
| Websites | 4 (18.2) | 16 (72.7) | |
| Friends | 2 (9.1) | 2 (9.1) | |
| Relatives | 2 (9.1) | 2 (9.1) | |
| None | 2 (9.1) | 0 (0.0) | |
| Health Knowledge |
Facebook Group (n=22) |
Line Group (n= 22) |
P-valuea |
|---|---|---|---|
| N (%) | N (%) | ||
| Baseline | |||
| High | 10 (43.5) | 13 (56.5) | 0.365 |
| Low | 12 (57.1) | 9 (42.9) | |
| 4th week | |||
| High | 6 (25) | 18 (75) | <0.001* |
| Low | 16 (80) | 4 (20) | |
| 12th week | |||
| High | 19 (82.6) | 4 (17.4) | <0.001* |
| Low | 3 (14.3) | 18 (85.7) | |
| P-valueb | <0.001*** | <0.001*** | |
*Highly significant at p< 0.001.
| Variables |
Facebook Group (n=22) |
Line Group (n=22) |
P-valuea |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| Intention to reduce alcohol consumption | |||
| Baseline | 21.3 ± 8.2 | 19.9 ± 6.4 | 0.555 |
| 12th week | 34.6 ± 2.2 | 19.9 ± 9.3 | < 0.001** |
| P-valueb | < 0.001** | 0.950 | |
| Expected number of drinks per night | |||
| Baseline | 70.0 ± 16.9 | 62.7 ± 8.8 | 0.081 |
| 12th week | 23.2 ± 4.5 | 19.3 ± 4.2 | 0.005* |
| P- valueb | < 0.001** | < 0.001** | |
| AUDIT tool | |||
| Baseline | 1.9 ± 0.84 | 1.6 ± 0.7 | 0.123 |
| 4th week | 1.7 ± 1.0 | 1.8 ± 0.9 | 0.906 |
| 12th week | 1.8 ± 0.9 | 1.9 ± 0.9 | 0.659 |
| P-valueb | 0.623 | 0.458 | 0.752 |
3.3. Effects of Health Education Intervention between and within Groups
Table 3 shows the change in health knowledge between and within groups at baseline, 4th week and 12th week after the intervention. Initially, the intervention group had similar knowledge to the control group (p=0.365). In the 4th week, the control group had higher knowledge (p<0.001), but by the 12th week, the intervention group surpassed them (p<0.001). The intervention group showed significant knowledge improvement over time (p<0.001), reaching higher levels in the 12th week.
Table 4 shows the change in intention to reduce alcohol consumption, expected number of drinks per night, and AUDIT scores between and within groups. Initially comparable (p= 0.555) in intention to reduce alcohol consumption, the intervention group outperformed the control in the 12th week (p< 0.001), showing significant improvement and a higher mean value (34.6 ± 2.2 versus 21.3 ± 8.2). Initially similar (p= 0.081), the intervention group's expected drinks per night surpassed the control group significantly in the third month (p< 0.005), with a substantial reduction over time (p< 0.001), achieving a lower mean value at the 12th week (23.2 ± 4.5 versus 70.0 ± 16.9). The intervention group's AUDIT tool mean score in the 12th week (p= 0.659) did not substantially differ from the control group, while it was initially similar (p= 0.123). Additionally, there were no statistically significant changes in the intervention group over time (p= 0.623).
4. DISCUSSION
Socio-demographic, work and drinking characteristics succinctly outline the important information about En’ Girl in Bangkok, Thailand. The absence of significant differences between control and intervention groups underscores the success of the randomization in ensuring baseline comparability [23]. The mean age at which En’ Girls begin working in the entertainment industry is notably youthful [24]. This aligns with the typical age range associated with employment in the entertainment sector [25]. En’ Girls are typically young enough to fit the industry's emphasis on freshness and exuberance, as well as the general public's desire for a lively presence in nightclubs. This age group serves the target market for the industry and embodies the perceived vitality of this sector. A significant portion of the control group drinks “11–20 glasses” per night, according to the variable “expected number of drinks per night,” which helps to understand patterns of alcohol consumption. This observation can point to increased alcohol consumption brought on by external influences like peer pressure or working conditions that En’ Girls got drunk with the clients [26].
In terms of health knowledge, a significant shift occurred by the 12th week, with the intervention group surpassing the control group in knowledge levels. This underscores the effectiveness and adaptability of health education initiatives, particularly when tailored to the specific needs and context of niche populations, such as En’ Girls. Cultural, socioeconomic, and occupational issues are considered while designing health education for varied populations, ensuring its relevance and impact [27, 28]. This adaptability fosters meaningful interactions and long-lasting beneficial effects by responding to the dynamic nature of niche populations.
Evaluating changes in intention to reduce alcohol consumption at baseline and 12th week post-intervention reveals the effectiveness of the health education program for both groups. The notable disparity in the 12th week, with the intervention group exhibiting significantly higher values than the control group, emphasizes the impactful outcome of the intervention. Further supporting its effectiveness, the intervention group demonstrates significant and statistically meaningful changes from baseline to the third month (p < 0.001), indicating substantial improvements in intentions and drinking-related behaviors. Existing literature indicates that brief interventions in primary care settings can help people successfully reduce their drinking, resulting in long-lasting reductions in consumption, which validates the current study's findings on intention to reduce alcohol consumption [29].
The results for the 12th week indicate a substantial decrease (p<0.001) in the mean value of the expected number of drinks per night (23.2 ± 4.5) in the intervention group when compared to the baseline (70.0 ± 16.9). These findings imply that health education initiatives can affect participants' expectations and intentions regarding alcohol use, urging them to drink responsibly. This change might represent an awareness of the risks associated with binge drinking and a movement toward attainable standards.
It appears that the health education intervention had a minor impact on these risk assessments for alcohol use disorders for three time points (baseline, 4th week and 12th week), as there were no significant changes in AUDIT scores over time (p= 0.623) in the intervention group. Due to non-significant differences in AUDIT scores, the program did not significantly lower the likelihood of developing an alcohol use disorder. The lack of a significant intervention effect on the AUDIT tool could be explained by the instrument's predominant emphasis on detecting risky alcohol intake instead of recognizing alcoholism or dependence. The goal of the AUDIT tool is to intervene before the onset of alcohol dependence by identifying drinking patterns that may be hazardous either now or in the future [30]. Since the health education program focused more on risky drinking than on more severe forms of alcohol use disorders like alcoholism, it is possible that it had minimal impact on AUDIT scores.
One of the study's limitations is its small sample size of 44 participants, which may not accurately reflect the wide community of En’ Girls. Self-reported assessments may introduce biases, and the 12-week program may restrict the ability to understand the long-term impact of interventions. The unique culture of Bangkok city may raise concerns about generalizability, while internal validity is called into question by subjective measures and possible selection bias. Regulations on the platform may also limit the use of Facebook for private health information. The study's reliance on social media platforms like Facebook and LINE for health education interventions may introduce bias by potentially excluding individuals who lack access to or cannot use these platforms. The contextual elements of the study, introduced during the COVID-19 epidemic, may limit its generalizability to other time periods.
This groundbreaking study assessed the effects of a health education intervention on En’ Girls using a randomized controlled trial study design. The study's distinct focus, internal validity assurance, direct comparison of the intervention and control groups, and use of essential outcome measures allow for a thorough assessment. Particularly in light of Bangkok's exciting nightlife, the intervention group's prospective benefits are highlighted by notable improvements in health knowledge, intention to reduce alcohol consumption and expected number of drinks per night in the 12th week. The applicability of the study for health promotion is highlighted by its practical ramifications, which also demonstrate how relevant and flexible it is for practical application.
CONCLUSION
This study shows how effective a health education intervention using Facebook and LINE is for Bangkok's En’ Girls. In comparison to the baseline and control groups, the intervention dramatically increased health knowledge, intentions to reduce alcohol consumption, and reduced in expected number of drinks per night over the course of 12 weeks. The study emphasizes the usefulness of social media platforms for education and the significance of culturally competent health interventions. All things considered, it presents a viable strategy to treat alcohol-related health problems in communities that are at risk worldwide. Future interventions should consider diverse communication channels beyond social media, incorporate biochemical verification for validity, extend follow-up periods, and ensure cultural sensitivity for maximum relevance.
ABBREVIATIONS
| AUDIT | Alcohol Use Disorders Identification Test |
| En’ Girl | Entertainment Girl |
| COVID-19 | Coronavirus Disease |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The Research Ethics Review Committee for Research Involving Human Research Participants, Group 1, Chulalongkorn University, approved this study (COA 074/2565).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
All participants provided informed written consent and granted the publication of the findings.

