All published articles of this journal are available on ScienceDirect.

Determinants of Prevalence and Factors Associated with Anemia among Pregnant Women in Gambia: A Multivariate Analysis using DHS Data
Abstract
Background
Anemia is a prevalent public health concern in The Gambia and other developing nations. While previous studies relied on binary logistic regression, the Multinomial Survey Logistic Regression Model was developed to address complexities in survey design, including sampling weights, stratification, and clustering. Multiple Imputation with Chained Equations (MICE) was employed to address missing data in variables such as anemia level, contraceptive use, and malaria drug intake during pregnancy.
Aim/Objective
This study aims to determine the prevalence and factors of anemia among pregnant women across eight local government areas in The Gambia. The research focuses on Kanifing, Kuntaur, Mansakonko, Kerewan, Janjanbureh, Basse, Brikama, and Banjul. Given the limited research on anemia among pregnant women in The Gambia, there is a need for further investigation into this topic.
Methods
MICE were utilized to address missing data due to their validity in handling uncertainty. This method generates multiple reasonable datasets for imputation and analyzes them accurately. A survey logistic regression model was employed to assess data fitness, considering the complex sample design. Anemia levels were measured among 11,865 pregnant women aged 15 to 49 using a systematic questionnaire. The multinomial survey logistic regression model was utilized to account for sampling weights, stratification, and clustering, relaxing the premise of observation independence violated by conventional logistic regression.
Results
The study involved 11,865 expectant mothers, revealing mild, moderate, and severe cases of anemia with a prevalence of 44.6%. Factors associated with anemia included place of residence, local government area, contraceptive use, age, literacy level, and current pregnancy status.
Conclusion
Socio-economic, demographic, and environmental factors significantly impact anemia levels among reproductive women in The Gambia. Addressing factors such as place of residence, local government areas, contraceptive use, literacy level, and current pregnancy status is crucial in mitigating anemia risk. Government initiatives, such as improving access to sanitation facilities and offering free check-ups, could effectively address this public health concern.
1. INTRODUCTION
1.1. Anemia
Anemia is a disorder when the body's Red Blood Cell (RBC) production or carrying capacity of oxygen is inadequate for physiological functions [1]. This disorder affects one-fourth of the world's population, which is a challenge for global public health [2], and sadly, the high rate of anemia among African women experiencing pregnancy is quite an issue [3]. The World Health Organization (WHO) asserts categorically that in global anemia databases, anemic women experiencing pregnancy accounted for 19.3 million (55.8 percent) of the population in Africa between 1993 and 2005. In Togo, for instance, 15.2% of African refugees had anemia, and in Ethiopia, 84.4 percent had anemia [4].
Anemia can be caused by several things in pregnant women. These things include nutritional deficiencies, notably iron and folate deficiencies, gastric flea infection, malaria, and chronic sickness [5]. In addition, infectious diseases such as intestinal parasite infection and malaria can dramatically increase the rate of anemic occurrence among women experiencing pregnancy [6].
Anemia affects millions (32.4) of pregnant women globally, with the regions of Southeast Asia and Africa accounting for over 90 percent of this predicament [7]. It is estimated that about 17.2 million women experiencing pregnancy are expected to have this deficiency. Africa, especially the Sub-Sahara, has the highest rate of anemic deficiency among pregnant women [7].
Pregnancy anemia is common in East African countries, Rwanda and Uganda, at 20 and 32.5 percent, respectively [3]. Anemia, particularly among pregnant women, is of concern because severe iron deficiency increases the risk of premature birth, low birth weight babies, and even postpartum depression [3]. In addition, it varies across different countries and territorial boundaries. Iron deficiency, caused by a persistently negative ratio of iron concentration, is what instigates anemic occurrence among reproductive or fertile women, and this accounts for 50% of all global cases [6].
A negative ratio of iron can be caused by inadequate iron consumption or assimilation during dieting, an increase in body demand for iron during pregnancy, and increased iron loss due to monthly blood flow in women, infestation by worms, and certain infections [8]. To prevent anemia during pregnancy, there is a recommen- dation by the World Health Organization (WHO) for supplementation of intermittent iron and folic acid to be conductedduring monthly flows for women residing in areas where the rate of anemic occurrence is high, stay 20% and above [9].
Many national nourishment programs and methods for preventing and controlling micronutrient deficiencies have been created to lessen anemia in expectant mothers [10]. Despite all efforts, a significant public health issue is maternal anemia because as hemoglobin levels fall, death-risking outcomes become more apparent [11]. Since limited studies on this subject exist [11], this study, therefore, is carried out as a new investigation in Gambia to evaluate the extent to which anemia has become rampant among pregnant women living in eight local government areas of Gambia.
1.2. Literature Review and Knowledge Gap
Numerous researchers have worked on risk factors associated with anemia. For example, using current demographic and Health Surveys, a previous study [3] investigated the frequency and causes of anemia in pregnant women in the eastern part of Africa. The research examined secondary data from eleven East African countries' Demographic and Health Surveys. The study enlisted the help of 8583 pregnant women (weighted sample). To determine the level of anemia, a Poisson regression with robust error variance in a multilevel mixed-effects generalized linear model was fitted. Anemia was found to be prevalent in 41.82 percent of pregnant women (95 percent confidence interval: 40.78, 42.87), with prevalence varying greatly between countries, varying between 57.10 percent in Tanzania and 23.36 percent in Rwanda. Anemia during pregnancy was more common in pregnant teenagers (PR = 1.22; 95% CI:1.02, 1.40), unmarried women (aPR = 1.14; 95% CI:1.02,1.28), pregnant women with inadequate toilet facilities (aPR = 1.17; 95% CI:1.06,1.27), and pregnant women from countries with low literacy rates (aPR = 1.12; 95% CI:1.07,1.18). Another research [9] also conducted a study to ascertain how often and what influences anemic presence in pregnant women visiting prenatal clinics (ANC) at a tertiary referral medical center in Northern Ghana. At Tamale Teaching Hospital, 400 expected mothers receiving prenatal care participated in a cross-sectional study. Information on women's socio-demographic traits, health habits, variety of diets, awareness of anemia, and a semi-structured questionnaire and a 24-hour meal recall were used to measure hemoglobin levels. The Chi-square test and logistic regression analysis were employed to identify the independent causes of pregnancy anemia. The average age of the women was 28.3 (4.5) years, and their hemoglobin levels were 10.81 (1.41) g/dl. During the third trimester of pregnancy, anemia became more common, with 50.8 percent of the women anemic (95 percent confidence interval (CI): 45.8-55.7). At the time of the interview, the women's understanding of anemia and the third term of pregnancy, as well as the socio-demographic, nutritional, and preventive health service factors examined, were independent drivers of anemia in pregnancy. Women with the least amount of awareness about anemia (AOR = 2.63, 95% CI: 1.50-4.61) and medium anemia awareness were three and two times more likely to be anemic, respectively (AOR = 1.92, 95 percent CI: 1.12-3.27), respectively than those with the highest (AOR = 2.63, 95 percent CI: 1.50-4.61). Similar to this, third-trimester pregnant women had a four-fold increased risk of anemia at the time of interview than those in their first trimester (AOR = 3.57, 95 percent CI: 1.91–6.67). A previous study conducted a cross-sectional research among pregnant women who presented to the prenatal clinic between June 2016 and December 2017 [12]. To compare the frequency and causes of anemia in women with and without HIV and in addition to laboratory testing to assess hemoglobin levels and CD4 count (for HIV-positive women), information on socio-demographic factors was acquired. The total number of pregnant women was 350, having an equal number of females who were HIV positive and negative. Utilizing the social sciences software program version 20, the variables were compared between the two groups. Statistical significance is defined as a p-value of less than 0.05 with a 95% confidence level. HIV-positive and negative people had an average age of 31.544.1 and 29.03 years, respectively, whereas HIV-positive and negative people had an average gestational age of 20.418.11 and 22.377.34 weeks at booking. The HIV-positive group's average parity was 2.021.5, while the HIV-negative group's average parity was 2.561.2. At booking, HIV-positive women's hemoglobin levels were 9.921.8 g/dl, while HIV-negative women's hemoglobin levels were 10.61.1 g/df. At the time of booking, the CD4+ count in the HIV-positive group was 478251 per microliter. Anemia affected 36.6 percent of the population, regardless of HIV status. According to the study, anemia was observedin 44.6% of women with HIV and 28.6% of women without HIV. Anemia and HIV status had a statistically significant connection (p=0.002). These studies on anemia in Gambia are not adequate in solving this issue; thus, more studies are required to investigate this issue and propose ways to solve it completely, especially among pregnant women.
1.3. Rationale and Motivation
Pregnancy anemia, or in other words, anemia among pregnant women, has continued as a common issue in Gambia over the past years. This is no longer an issue to be contended with and must be dealt with decisively. Hence, this research. The Gambia has limited studies concerning pregnancy anemia [11]. Therefore, there is a need for more studies to be conducted in this area to help ascertain the emergence of this disorder and to equip further studies with data to proffer solutions.
2. MATERIALS AND METHODS
2.1. Design of Study
This study aimed to learn more about the sociodemographic, socioeconomic, and communal characteristics of pregnant Gambian women living in the sampled regions of the country, as well as the frequency of anemia (determined at one point in time) along with the risk factors associated with it.
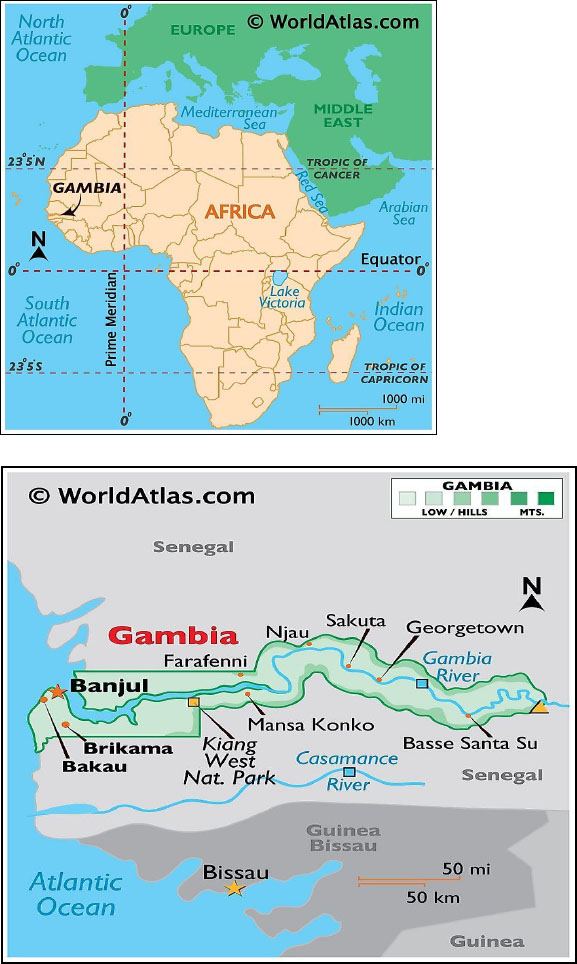
Maps of Gambia.
2.2.1. Study Area - Maps of Gambia (Fig. 1)
2.2. Study Population
Pregnant women are the participants in the study. They range in age from 15 to 49 years and live in eight sampled local government areas in Gambia. Pregnant women who lived outside of the study's chosen area were not required to participate since they were not part of the study area. Ethnicity, wealth index, type of toilet facilities, region, place of residence, highest educational level, religion, sex, literacy, occupation, type of cooking fuel, type of mosquito bed net, currently pregnant, taking malaria drug in pregnancy, and current marital status are among the variables examined in this study. Secondary data for this research work came from the 2019/2020 Gambia Demographic and Health Survey.
2.3. Data Source
Reviewing current public-domain survey datasets freely accessible online served as the foundation for this investigation. The original author received authorization to download and utilize the NDHS data sets found at http: //www.dhsprogram.com/data/dataset.Admin/login main.cfm.
2.4. Data Sampling and Design
A large sample size of 11,865 people was employed in the study. Well-designed questionnaires were given out during the interview sessions to obtain the data. Numerous topics, including demography, sociology, economy, and local variables, were covered by the questionnaire. Anemia during pregnancy, usage of antimalarial medications throughout pregnancy, breastfeeding, and specific information regarding contraception were all gathered and recorded as “yes” or “no.” The acquired data was entered into the SPSS software, version 23, and then saved. Primary data was acquired for this inquiry.
During the interview sessions, a well-designed questionnaire was used to elicit important information from participants. The questionnaire had sections for demographic, sociological, economic, and community information. The use of contraception, breastfeeding, using antimalarial medications while pregnant, and having anemia while pregnant were all determined based on the participants' responses and categorized as “yes” or “no.” The data was all inputted and saved using version 23 of the SPSS software. For this investigation, primary data was gathered.
3. DATA ANALYSIS
3.1. Outcome Variable
The existence or absence of anemia is the variable of dependence in this study. This condition is determined by the hemoglobin level in the blood cells, which is measured in grams per deciliter (g/dL). Anemic degree during pregnancy is divided into three groups. If hemoglobin concentration exists, it is between 10.0–10.9 g/dL. It is classified as moderate depending on the hemoglobin concentration, which should lie between 7.0 g/dL. The severity of anemia occurs when the hemoglobin concentration is less than 7.0 g/dL and is non-anemic when the hemoglobin concentration is < 11.0 g/dL [13]. In this study, a pregnant woman between the ages of 15 and 49 was deemed anemic if her hemoglobin level, smoking status, and altitude were all less than 12 g/dL and considered non-anemic if it was greater than 12 g/dL.
3.2. Independent Variable
Socio-demographic, economic characteristics and community levels of respondents are considered in this study due to their generality to all participants, i.e., what they have in common, and because those variables have been utilized in other research such as [14] and [15]. This is the theoretical foundation of this research, and the variables of independence include the participant's age (classified in years:15-19, 20-24, 25-29, 30-34, 35-39, 40-44, 45-49) and wealth index of the respondent(poor, middle class, and the rich), respondents educational level (no education, primary education, secondary and tertiary), type of religion practiced (Islam or Christianity), toilet facility type (improved, unimproved and others), cooking fuel type (old, modern, and others), respondent uses mosquitoes bed net (Yes, No), Use of contraception (Yes, No), respondents' ethnicity (Gambian, Non-Gambian, and others), level of literacy (Illiterate, literate), breastfeeding (Yes/No), marital status (never married, now married, and formerly married), responder currently pregnant (Yes, No), took SP/Fansidardrug for malaria during pregnancy (Yes, No), and local government area (Banjul, Kanifing, Brikama (Rural or Urban).
3.3. Statistical Analysis
Version 23 of SPSS was employed for the exportation of relevant data. The management and cleaning of data was carried out using R Software of version 4.2.1. To analyze the complete data collected for this study on the presence of missing observations in two different variables. MICE was therefore employed to fill in the missing observations present in the data collected. The analysis employed both descriptive and inferential statistics and summarized using frequency and percentage. We fitted the model with R software's built-in base package. Each independent variable was subjected to a multinomial logistic regression to identify the factor that influenced the outcome of interest, and the 95 percent confidence interval and the crude odds ratio were derived. The statistical strength and adjusted odds ratio was also calculated using logistic regression.
4. RESULTS
4.1. Descriptive Statistics (Anemia)
Cross-tabulation analysis served as the foundation for the basic exploratory data analysis, and a summary of the findings was made. Table 1 shows a statistically important correlation between anemia and educational level, wealth index, toilet faculty, cooking fuel, contraceptive use, ethnicity, age, literacy level, marital status, place of residence, current pregnancy, and local government area among females of childbearing age. The overall frequency of anemia in Gambia among reproductive women was 44.6%. Members per household ranged in age from 15 to 49 years old, with a mean of 28.36 and a median of 27.00. The minimum number of family members was one, with a maximum of 189, a mean of 33.37, and a median of 27. According to the table, in the Gambia, anemia was more common in women without formal education than it was in women with formal education (52.9% vs. 47.1%, p-value 0.001). It was also shown from the results that anemia was significantly influenced by the wealth index, with the poorest families having a higher rate of anemia (54.1%) than the richer families (45.5%) and the richest families (43.5%) in Gambia respectively with the p-value of 0.000. Anemia was more prevalent in women who used the Improved toilet facilities than among those using the Unimproved toilet facilities (51.2% and 45.0%, respectively, p-value=0.001). Similarly, according to the findings, anemia was more common among women who did not utilize contraception (49.9%) compared to women who used it (44.4%). More specifically, the prevalence of anemia varied with literacy level. Table 1 shows that literate women had a higher prevalence of anemia (52.2%) and 45.3% among illiterate women. It was also observed that ethnicity contributed significantly to the prevalence of anemia in Gambia. Thus, non-Gambians are more prone to anemia than Gambians (50.4% and 49.4%, p-value=0.02. Furthermore, the findings showed that women with anemia were more likely to be currently married (50.6%) followed by formerly married women (47.5%) than women who never married (46.7%), respectively. Also, women who were rural residents were more vulnerable to anemia (53.9%) than those who were urban residents (45.7%). A larger percentage of pregnant women had anemia than non-pregnant women (54.7%) and lower in non-pregnant women (48.9%, p-value=0.0007). It was also revealed that the local government area contributed significantly to the anemia level, in which women living in the Kuntaur local government were more prevalent with anemia (56.9%) than among women living in any other region with a p-value (0.001).
4.2. Multivariate Logistic Regression
This study, in Table 2 below, summarizes the outcomes of logistic regression in a multivariate survey. The research work showed various variables that increase the risk of anemia in reproductive-age women in Gambia, which includes respondents' place of residence, local government area, use of contraceptives, age, literacy level, size of household, educational level, wealth index, respondent’s toilet facility, marital status of respondent and pregnancy status. This study found no association between the size of the household and the possibility of anemia in Gambian women who are sexually active (OR: 0.99, p-value=0.43). According to the findings of the study, respondents' place of residence was significantly associated with an increased risk of anemia among women of reproductive age in the rural area and were1.13 (P-value 0.051) times more likely to be anemic than women in the urban area.
| Variables | Categories | Anemia Level | P-Value | |
|---|---|---|---|---|
| - | - | YES(%) | NO(%) | - |
| Educational level | No education | 2627 (52.9) | 2336 (47.1) | <0.001 |
| - | Primary | 975(49.4) | 997 (50.6) | - |
| - | Secondary | 1982(45.9) | 2333(54.1) | - |
| - | Higher | 277(45) | 338(55) | - |
| Religion | Islam | 5728 (49.4) | 5856 (50.6) | 0.6944 |
| - | Christianity | 132(47.5) | 146(52.5) | - |
| - | Others | 1(33.3%) | 2(66.7%) | - |
| Wealth Index | Poorest | 1805(54.1) | 1529(45.9) | 0.000 |
| - | Poorer | 1154(51.2) | 1099(48.8) | - |
| - | Middle | 1118(49.3) | 1152(50.7) | - |
| - | Richer | 925(45.5) | 1110(54.5) | - |
| - | Richest | 859(43.5) | 1114(56.5) | - |
| Toilet Faculty | Improved | 3966 (51.2) | 3781(48.8) | <0.001 |
| - | Unimproved | 1591(45) | 1943(55) | - |
| - | Others | 304(52.1) | 280(47.9) | - |
| Cooking-Fuel | Old | 5529(49.4) | 5653(50.6) | 0.7437 |
| - | Modern | 117(47) | 132(53) | - |
| - | Others | 215 (49.5) | 219(50.5) | - |
| Use of Mosquitoes net | Yes | 2764(50.2) | 2747(49.8) | 0.129 |
| - | No | 3097(48.7) | 3257(51.3) | - |
| Use of Contraceptive | Yes | 477(44.4) | 597(55.6) | 0.00069 |
| - | No | 5384(49.9) | 5407(50.1) | - |
| Ethnicity | Gambian | 5225(49.4) | 5355(50.6) | 0.0538 |
| - | Non-Gambian | 606(50.4) | 594(49.6) | - |
| - | Others | 30(36.6) | 52(63.4) | - |
| Literacy | Illiterate | 2177(45.3) | 2632(54.7) | <0.001 |
| - | Literate | 3684(52.2) | 3372(47.8) | - |
| Current breastfeeding | Yes | 1478(49.8) | 1492(50.2) | 0.6594 |
| - | No | 4383(49.3) | 4512(50.7) | - |
| Marital status | Currently married | 4091(50.6) | 1720(53.3) | 0.0005 |
| - | Never Married | 1506(46.7) | 3992(49.4) | - |
| - | Formerly Married | 264(47.5) | 292(52.2) | - |
| Place of Residence | Urban | 2977(45.7) | 3533(54.3) | <0.001 |
| - | Rural | 2884(53.9) | 2471(46.1) | - |
| Current pregnancy | Yes | 533(54.7) | 442(45.3) | 0.0007 |
| - | No | 5328(48.9) | 5562(51.1) | - |
| Use of Malaria Drug | Yes | 5710(49.5) | 5827(50.5) | 0.238 |
| - | No | 151(46) | 177(54) | - |
| Type of Drinking water | Protected | 1132(51.1) | 1085(48.9) | 0.220 |
| - | Unprotected | 4524(49) | 4708(51) | - |
| - | Others | 205(49.3) | 211(50.7) | - |
| Smoking | Yes | 16(47.1) | 18(52.9) | 0.919 |
| - | No | 5848(49.4) | 5986(50.6) | - |
| Local Govt. Areas | Banjul | 438(46.3) | 509 (53.7) | <0.001 |
| - | Kanifing | 724(44.9) | 888(55.1) | - |
| - | Brikama | 1060(45) | 1295(55) | - |
| - | Mansakonko | 531(51.6) | 499 (48.4) | - |
| - | Kerewan | 709(51) | 682 (49) | - |
| - | Kuntaur | 751(56.9) | 568 (43.1) | - |
| - | Janjanbureh | 648(51.3) | 614(48.7) | - |
| - | Basse | 1000(51.3) | 949 (48.7) | - |
| Parameter | Estimate | Stand Error | Pr(>|Z|) | Adj OR (95% Cl) |
|---|---|---|---|---|
| Intercept | -0.2554 | 0.1907 | 0.1805 | 1.33(0.98,1.83) |
| Place of residence (ref = Urban) | - | - | - | - |
| Rural | 0.1252 | 0.0642 | 0.05123 | 1.13 (1,1.29) |
| Local govt. Area (ref = Banjul) | - | - | - | - |
| Kanifing | -0.0735 | 0.0839 | 0.3806 | 0.93 (0.79,1.1) |
| Brikama | -0.2169 | 0.0939 | 0.0208 | 0.8 (0.67,0.97) |
| Mansakonko | -0.2160 | 0.1304 | 0.0976 | 0.81 (0.62,1.04) |
| Kerewan | -0.2427 | 0.1322 | 0.0663 | 0.78 (0.61,1.02) |
| Kuntaur | -0.1643 | 0.1601 | 0.3047 | 0.85 (0.62,1.16) |
| Janjanbureh | -0.4283 | 0.1948 | 0.0279 | 0.65 (0.44,0.95) |
| Basse | -0.5345 | 0.2461 | 0.0299 | 0.59 (0.36,0.95) |
| Use of Contraceptive (No) Yes |
-0.2179 | 0.0665 | 0.0011 | 0.8 (0.71,0.92) |
| Literacy (ref = illiterate) | - | - | - | - |
| Literate | -0.1429 | 0.0617 | 0.02053 | 0.87 (0.77,0.98) |
| Wealth index (ref = Poorest) | - | - | - | - |
| Poorer | -0.2352 | 0.1964 | 0.2307 | 0.79(0.54,1.16) |
| Middle Richer Richest |
-0.4051 -0.783 -0.6007 |
0.2167 0.268 0.2682 |
0.062 0.0034 0.025 |
0.67 (0.44,1.02) 0.46(0.27,0.77) 0.55(0.32,0.93) |
| Toilet (ref=Others) | - | - | - | - |
| Improved | -0.802 | 0.498 | 0.0002 | 0.44(0.29,0.68) |
| Unimproved | -1.5075 | 0.959 | 0.007 | 0.22(0.07,0.66) |
| Currently Pregnant(ref=No) | - | - | - | - |
| Yes | 0.1478 | 0.0693 | 0.0331 | 1.16 (1.01,1.33) |
The local government area of residence in The Gambia has a significant effect on anemia in women of reproductive age. It was discovered from the results that a Brikama woman, Janianbureh and Basse was 0.8, 0.65, and 0.59, respectively (P-value 0.021, P-value 0.028, and P-value 0.0299) less likely to have anemia than a woman from Banjul local government area of The Gambia.
According to this study in Table 2, the use of contraception was statistically connected with a risk factor for anemia among Gambian women who were sexually active. It was discovered that women who used a contraceptive method were 0.8 (P-value 0.001) and had a higher risk of having anemia than women who did not use a contraceptive method.
Among Gambia women of reproductive age, literacy level significantly influenced anemia status (P-value 0.021). Women with literacy had a 0.87 times reduced risk of anemia than women without literacy (OR: 0.87(CI 0.77, 0.98)). The type of toilet facility was discovered to be a crucial risk factor for anemia in those Gambian women who were sexually active. The research showed that women who used modern restrooms had a decreased incidence of anemia (flush of the toilet, septic tank, or piped sewer system), which was 0.44 times lower than women using other toilet facilities (Bush or field, and respondents with no toilet facility). The outcome also showed a significant relationship between pregnant women and an elevated incidence of anemic occurrence in Gambian women who were sexually active (P-value = 0.03). It was discovered further that anemia risk among women who were currently pregnant was 1.16 times (OR: 1.16) higher than women who were not.
According to this study in Table 2, the anemic rate among women of fertility in Gambia decreases as the household wealth index rises. The family's wealth index was discovered to be a major factor associated with the anemia status of Gambian women, with a woman from a richer household being 0.46 (P-value 0.003) times less likely to be anemic than a woman from an extremely poor home. Women from the richest families were also found to be 0.55 (P-value 0.025) times compared to women from the lowest wealth index class. They are less likely to be anemic.
The model fit statistics for the tests using the log-likelihood (LL), Akaike Information Criterion (AIC), and Bayesian Information Criterion (BIC) are shown in Table 3. To compare the models of intercept versus intercept with covariates. The intercept and covariate models were found to have smaller AIC and BIC values than the intercept-alone model, which had higher values in all criteria. This suggests that the model that fits best has an intercept and covariate.
| Model Fitting Information | ||
|---|---|---|
| - | Intercept Only | Intercept and Covariates |
| AIC | 16449 | 16351.99 |
| LL | -8223.33 | -8152.99 |
| BIC | 16456.04 | 16387.47 |
4.3. Missing Data with MICE (Multiple Imputation with Chained Equations)
A comparative analysis of fitted models for missing data and imputed data was obtained in this study. We employed the use of Multiple Imputation by Chained Equations (MICE), which is a form of prediction from different regression models, to fill in missing values (making it more accurate to use) while considering the co-linearity of the dataset. Given specific presumptions regarding the mechanism of missing data, this approach replaces missing data values in a data collection (e.g., the missing data are fully random and at random intervals) [16].
Missing data are values that are absent from a dataset; they may consist of a single value missing from a single transaction or a complete observation being absent (rows). Both continuous and categorical variables may have missing data (e.g., heights and gender of a population) [17].
In this study, missing observations were present in three variables, which are anemia level, taking SP/Fansidar drug for malaria during pregnancy (Malaria drug in pregnancy), and use of contraceptive parameters accounted for 50.16%, 51.18%, and 4.31% respectively, and other variables have 0% missingness.
Multiple Imputation by Chained Equations, also called sequential regression or multiple imputation, is a reliable and informative method for addressing missing data in datasets [18]. Through an iterative succession of prediction models, the process 'fills in' (imputes) missing data in a dataset. It aims to accommodate for uncertainty around missing data by producing numerous plausible imputed data sets and effectively integrating the results from each one. Because it uses numerous complete data sets and provides both within-imputation and between-imputation variability, it outperforms traditional multiple imputation. It is a crucial Imputation approach since it can handle both numerical and categorical variables. This technique entails grouping missing values in a column and assigning them to a new value that is far beyond the column's range [19]. MICE has a problem in that data sets frequently have hundreds of variables, and imputations can be created using any one of them. All of these variables cannot be included due to multicollinearity and computational issues. It is thus not required. In linear regression, the explained variance' increase after the best factors have been summed is frequently negligible in research like [20]. Picking a good subset of data with no more than 15 to 25 variables is ideal for imputation purposes. MICE is a great option for our inquiry because we are using seventeen (17) variables.
In our analysis, we employed MICE to fill in the missing observations in anemia levels and took malaria drugs during pregnancy. For a category with two levels, it uses logistic regression prediction; for categories with more than two levels, it uses polynomials; and for continuous variables, it uses a linear regression. To attain the best results, we chose the model with the lowest standard error from those that were fitted for anemia level, took malaria drugs in pregnancy, and used contraceptive variables in the data with missing observations and those that were filled using MICE, as shown in Table 4 below. It was revealed that the imputed data using MICE was the best fit for the anemia data collected in Gambia. This is in consanguinity with previous research [21, 22], asserting that the imputed approach performs best.
| Variable |
Std.Error (Missing Data) |
Std.Error (Imputed Data) |
|---|---|---|
| Anemia Level | 0.0000845 | 0.0000421 |
| Malaria Drug in Preg | 0.0000294 | 0.0000138 |
| Use of Contraceptive | 0.0000253 | 0.0000242 |
5. DISCUSSIONS
In this study, some risk factors related to anemia in pregnant women were examined and assessed. This study used the 2019–2020 Gambia Demographic and Health Survey data set. A regression model called multinomial survey logistic was adopted to assess the risk factors associated with anemia in pregnant Gambian women. Standard logistic regression violates the condition of observation independence, whereas this model relaxes it and considers stratification, clustering, and sample weights.
In the multinomial survey logistic regression model, the succeeding socioeconomic, bio-data, and environ- mental features exhibited a statistically substantial correlation with anemia among pregnant women, which are place of residence, local government area, usage of contraceptives, age, literacy level, and pregnancy status with a strong connection with anemia while the present study failed to discover any statistically significant correlation between family size, educational level, wealth index, toilet facility, and marital status among Gambian women in survey logistic regression of multivariate nature.
Research findings revealed that respondents' anemia levels were not significantly influenced by the size of the household (OR: 0.99, P-value=0.43). It was also shown that participants’ place of residence was a risk factor linked to anemia (OR: 1.13, P-value=0.05). In other words, the prevalence of anemia varied significantly between residents in rural and urban areas, respectively. These findings are in line a previous study [23], whichused logistic regression in modeling the prevalence of anemia and found that a strong correlation exists between the place of residence and anemia. Similarly, the study participants' educational level was not influential on anemia (P-value>0.05). Furthermore, the findings of this investigation also showed that few of the respondents' local government areas have a significant influence on the participants’ anemia status (P-value=0.02), which is in line with the work of [24], who used a generalized linear mixed-effects model in checking the contributing risk factors of anemia. Their results revealed that age, educational level, employment status, place of residence, wealth index, availability of antenatal care, place of delivery, history of using family planning in a health facility, current pregnancy, and visits by fieldworkers within the previous 12 months are all factors that are significantly associated with anemia in lactating mothers. Furthermore, according to this study's findings, anemia status and the use of contraceptive methods are significantly correlated. Women who presently use contraception have been reported to, compared to women who do not now take contraception, have a decreased incidence of anemia. This finding is synonymous with the findings by [14], who used Rwanda Demographic and Health Survey datasets from 2014–2015 to examine socioeconomic, demographic, and environmental factors. Their research showed that 6,680 women between the ages of 15 and 49 had their anemia status evaluated and that 19.2 percent of the women in this childbearing age range had anemia. A further finding of the study was that body mass index, use of birth control, and anemia in Rwandan women of childbearing age were all related to the use of mosquito bed nets, marital status, household size, household wealth quintile, literacy, use of tobacco, type of cooking fuel, nature of restrooms, nature of water supply, and province of habitation. This result is further supported by the findings of previous reaseach [25] and [26], which show that the prevalence of anemia was significantly lower in women taking hormonal contraceptives (36% vs. 56%, P-value=0.04) than in non-users. Additionally, there was a strong correlation between literacy level and anemia level (OR: 0.87; P-value = 0.002). This result is consistent with findings [27]. Their study indicated that the frequency of anemia was 35.1% and that there was a strong correlation between anemia and the parents' literacy levels. More specifically, according to a study, pregnant women are more likely than non-pregnant women to be anemic. This result is consistent with research by [28] and [29-32] who found that anemia was more common in pregnant women (21.6%) than in non-pregnant women (17.4%) and third-trimester women (10.5%).
In multivariate survey logistic regression, the current study found no statistically significant relationship between educational attainment, religion, tobacco use, malaria medication use, type of drinking water, breast-feeding status, use of a mosquito bed net, type of cooking fuel, marital status, household size, or anemic occurrence among women that are sexually active in the Gambia.
6. LIMITATIONS AND STRENGTHS
This study is limited to the region of Gambia and, more specifically, to the eight local government areas of the country. It only considers the extent to which anemia is prevalent among pregnant women but does not offer practical solutions to the issue. However, the study has high statistical power, and its results can be used in further studies to offer practical solutions to the issue of pregnancy anemia in Gambia.
CONCLUSION
The results of this study show a substantial correlation between anemia status and the use of contraceptive methods. It has been noted that anemia is less common among women who are currently using contraception compared to those who are not. Other findings also allude to the prevalence of anemia among pregnant women in the Gambia.
However, it is recommended that further studies be conducted.
- Generic solutions to the problems of anemia in Gambia.
- Specific solutions to the issue of anemia among pregnant women in Gambia.
- The prevalence of anemia as a disorder in the whole West African region.
- Health Standards about Anemia in Africa and Improvement.
- Lifestyle and its contribution to anemic prevalence in third world countries.
The main objective of this study was to determine the prevalence of anemia and anemia risk factors among pregnant women in Gambia Local Government Areas. In this study, only place of residence, local government area, contraceptive use, age, literacy level, and pregnancy status among women of reproductive age among all these risk variables were linked to anemia, and the findings were consistent with previous findings. However, anemia among Gambian women was not related to marital status, cooking fuel use, or educational level. The present research can assist the Gambian government in improving some of the country's prevalence determinants among sexually active women. A longitudinal analysis with more trends and patterns might be seen for future consultation on anemia prevalence in each community, which could also be undertaken to establish the causes and therapy for anemia. Summarily, this study's only drawback is that the data are cross-sectional.
AUTHORS’ CONTRIBUTION
It is hereby acknowledged that all authors have accepted responsibility for the manuscript's content and consented to its submission. They have meticulously reviewed all results and unanimously approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| MICE | = Multiple Imputation with Chained Equations |
| OR | = Odd Ratio |
| CI | = Confidence Interval |
| APGAR | = Appearance Pulse, Grimace, Activity and Respiration |
| g/dL | = Grams per Deciliter |
| aPR | = Annual Percentage Rate |
| AOR/Adj | = Adjusted Odds Ratio |
| Pr | = Probability |
ETHICAL STATEMENT
This study is based on secondary data from the 2019/2020 Gambia Demographic and Health Survey (DHS). The original DHS survey obtained ethical clearance, including informed consent from participants. We have added a statement in the methods section confirming that the study adhered to the Helsinki Declaration and that all necessary ethical approvals and informed consents were obtained in the original DHS survey.

