All published articles of this journal are available on ScienceDirect.

To Risk or Not to Risk? Evaluating Self-medication Practices among Ecuadorian Adults During COVID-19 Lockdown
Authors Info & Affiliations
Abstract
Background
Self-medication involves using drugs to treat self-diagnosed disorders or symptoms. According to WHO, it is associated with a high risk among the general population, exacerbated by the COVID-19 pandemic.
Objective
This study aimed to assess self-medication practices, risks, and severity index among Ecuadorian adults during the first COVID-19 lockdown period in April 2020, using a descriptive non-experimental research design and a hazard risk assessment score analysis.
Material and Methods
A descriptive non-experimental research design was used to assess self-medication practices, risk, and severity index among 364 Ecuadorian adults during the first COVID-19 lockdown period in April 2020. The study utilized an online survey and Hazard-Risk-Assessment-Score (HRAS) analysis of clinically relevant questions. Descriptive statistics were mainly used, integrating Chi-square and ANOVA analysis using R.
Results
Despite a high level of education among the surveyed population, there was a significant risk of medication-related problems, with 63.1% and 26.72% of respondents at the third and fourth risk levels, respectively. Furthermore, 55% were at severe risk of self-medication, while 35% opted for medication therapies recommended on television, social media, or by influencers instead of consulting health professionals. Another 39% took medication before receiving recommendations from a doctor or pharmacist.
Conclusion
The study highlights the need to improve the image of pharmaceutical chemists as part of multidisciplinary health teams, monitor prescriptions of the doctors, and reduce drug side effects to mitigate the risks associated with self-medication.
1. INTRODUCTION
Self-medication is a global phenomenon with reported prevalence rates from 11.2% to 93.7%, as documented by Chautrakarn et al. in 2021 [1]. Notably, the extent of self-medication varies among nations, prominently manifesting in developing countries. The utilization of self-adminis- tered treatments is dominated by analgesics and antipyretics, accounting for 44.3% of cases, followed by non-steroidal anti-inflammatory drugs at 36.4%, and antihistamines at 8.5%, according to research by Machado-Alba et al. in 2014 [2].
Of paramount significance is the rapid evolution of technology and the pervasive influence of the Internet, enabling the general populace to access a wealth of medical and pharmacological information, thus mitigating the need for expert intervention and inadvertently fostering an environment conducive to heightened self-medication practices [3]. Concurrently, a series of comprehensive studies have underscored a range of concerns arising from self-medication, including adminis- tering subtherapeutic doses, indiscriminate use of antibiotics, and the potentially injudicious reliance on natural remedies. A notable finding from a cross-sectional and observational study spanning 14 countries, including Ecuador, reveals that approximately 44.9% of instances pertain to self-medication [4].
During the COVID-19 pandemic, health awareness was a great factor that contributed to increased hesitancy to health regulations and recommendations, including self-medication. Social studies conducted in Russia showed significant similarities with Latin American health behavior changes during the lockdown. A survey with 2771 participants showed that 57,5% were unwilling to get vaccinated, and 28.6% were in denial of meeting the basic sanitary recommendations, being more likely to contract COVID-19 and other diseases [5]. In another study, the global population was more likely to develop some grade of depression, anxiety, and loneliness due to the lockdown, leading to an increase of at least 30% in the consumption of alcohol and other substances as a coping mechanism without awareness of health damage [6].
Along with many other regions, Ecuador is immersed in a crisis of multiple dimensions encompassing health, economy, social fabric, and politics. The country has already dealt with a precarious financial situation and is on the verge of facing the COVID-19 pandemic [7]. This landscape of formidable crisis, exacerbated by the overwhelming surge of COVID-19 patients, high mortality rates, and complex cases resulting from adverse drug reactions, has left the healthcare system and public institutions in a delicate state, making them more susceptible to the needs of citizens. Consequently, in the country, people have sought different alternatives to conventional medical care and have begun to intensively engage in self-medication [8, 9].
Given that in Ecuador, 70% of drug acquisitions are subject to prescription regulations within the Integral Public Health Network (RPIS), evidence has shown that many of these medications can be acquired without a medical prescription. This trend is not unique to Ecuador; it is also observed in various Latin American countries [10-12]. Consequently, the Centers for Disease Control and Prevention (CDC) and the World Health Organization (WHO) have devised risk classification tools and checklists that emphasize the importance of mitigating the repercussions of self-medication. To quantify these risk factors and assess their severity, both organizations have employed the Hazard Risk Assessment Score (HRAS) tool [13, 14].
Based on this background, our study aimed to identify the self-medication and possible risks associated with drugs of Ecuadorians during the COVID-19 lockdown in Ecuador in 2020.
2. MATERIALS AND METHODS
This survey was developed during the first home lockdown in Ecuador, starting the outbreak peak from April 1 to April 20, 2020. The “Comité Nacional Expedito para Investigación sobre COVID-19” has approved the study as part of the “autosalud” proposal project MSP-MSP-2020-1113-O.
2.1. Study Design
A non-probability sampling for convenience pilot online survey was conducted with 363 participants from different regions and cities of Ecuador during the lockdown. This survey adopted a descriptive non-experimental research design to investigate the awareness and practice of self-medication conducted in April 2020 during the nationwide lockdown and increasing the number of positive COVID-19 cases. Because it was not feasible to do a community-based sampling survey during this outbreak period, we decided to collect data online by convenience sampling and adopted the snowball sampling method. Instead, we used an open web-based survey using Google Forms (Appendix), distributed via social media platforms, such as WhatsApp and social networking (Instagram and Facebook). The survey was established based on the Hazard Risk Assessment Score (HRAS) tool. Before engaging in the web-based questionnaire, participants were allowed to provide informed consent voluntarily. The questionnaire briefly introduced the background, objective, procedure, voluntary nature of participation, declaration of anonymity and confidentiality, and notes for filling in the online questionnaire.
The inclusion criteria were participants with internet access and >18 years. We excluded all participants not in Ecuador during the first lockdown, those without internet, participants who did not carry out the lockdown, health professionals, and participants under 18 years old. To minimize bias during participant selection, the question- naire with the questions of age, confinement, and population, which was not the objective of the study, was discarded.
2.2. Survey Design and Hazzard Risk Assessment Score
The survey questionnaire was grouped into nine sections, the first of which included participant confir- mation and data protection disclosure before being carried out. The survey scheme involved the following stages. One is introducing the self-medication survey during COVID-19, in which we informed the primary objective of the study. Two, acceptance of the study, in which the participants could accept or decline participation. Third, Patient identification, in which we determine the age, gender, residency city, quarantine city, and educational level. Fourth, the etiology of self-medication, the focalization of the questionnaire was determined by three questions if, during the quarantine period, they have ever suffered any pain or discomfort associated with COVID-19; if they ever took or will take some drugs to treat the pain or discomfort, and if they knew the OTC medications. Fifth, the symptoms (related to the current Pandemic), which determined the main symptoms and the intensity, include fever, cough, back pain, sore throat, headache, shortness of breath, nasal congestion, loss of smell, loss of taste, or other symptoms. The sixth section, drug information, allows us to determine the severity of self-medication. We asked the participants about who recommended the drug and the frequency of the recommendation, the reason they took the medication without any medical consultation, where the participant obtained the medications, and which medication they consumed during the period if they read the instructions of the drug and if they understood the instruction of the medications. The seventh section is about the consumption of Medicines, in which we ask how the participants knew the doses of the medication, if they have been taking the same drugs but with different commercial brands or different pharmaceutical laboratories, how they consumed the medication, with coffee, water or another beverage. At this moment, did the participant decide to finalize the medication used, the treatment period, and if they had any other symptoms or discomfort related to the drug consumption? The eighth section is about possible adverse events related to medications. This question was addressed to those participants who answered that they suffered some discomfort after consuming the drug in the last section, and it was asked about the most common symptoms and their severity. It asked about what the participant did after presenting some of the symptoms. The last section was about the Image of the pharmacist professional, in which we asked the participants if they knew about the healthcare role and image of the pharmacist and if they trusted the pharmacist (Fig. 1).
The overall score of the survey was derived from its minimum and maximum scores, encompassing both survey responses and clinically relevant indicators of predis- posing self-medication factors [15-17]. The questionnaire scores ranged from a minimum of 15 to a maximum of 245 points. The scores were categorized, with 18 points indicating minimal risk of self-medication and 115 points signifying entire self-medication risk. The Self-medication Survey score, also known as the Hazard risk score in the context of COVID-19, was further delineated: a minimum hazard risk score of under 40 points indicated the minimal risk of self-medication behavior and a low likelihood of adverse drug reactions. A hazard risk score between 40 and 80 points indicated a moderate risk of mild behavior and potential adverse reactions to medications, cate- gorizing this group as yellow in the Hazard identification and risk score system [18]. A severe hazard score exceeding 115 points corresponded to participants with high self-medication risks, potentially leading to adverse medication reactions, higher healthcare center visits, and an elevated risk of self-inflicted COVID-19. To assess the Hazard Risk Assessment Score, we meticulously analyzed the questionnaire's responses, focusing on indicators of self-medication behavior. The survey questions were stratified to establish the self-medication risk (Appendix). The arrangement of the queszthe Hazard Risk Assessment and Score (HRAS) matrix was guided by the Cardiff Vale University Health Board's Risk and Frequency Matrix, which categorized queries based on their presented risk and frequency in the study.
2.3. Statistical Analysis
The study carried out a data pre-treatment, which involved removing aberrant data, such as repeated surveys and missing data, that could distort the outcomes. Given that most variables in the database are qualitative and categorical, the analysis primarily revolved around frequencies and percentages as descriptive statistics. Inferential statistics were performed through the application of Fisher's exact test for independence. The “R Project” in the Rx64 4.0.2 version was employed for statistical analysis.
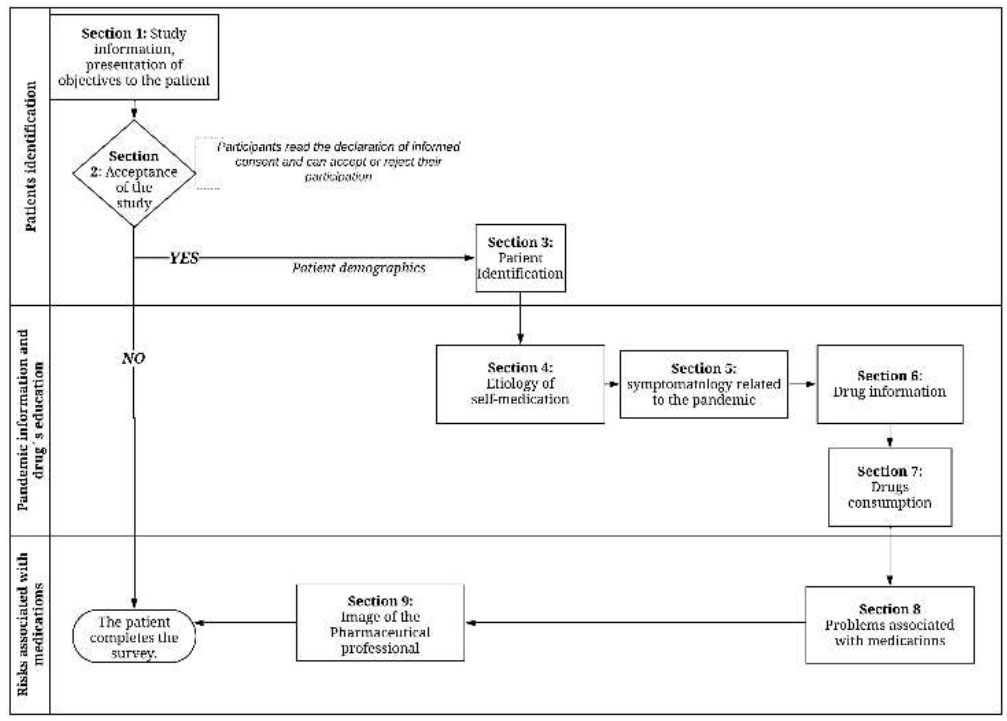
Study design of the self-medication survey COVID-19.
2.4. Ethical Considerations
All participants were informed about the objectives and purpose of the study, and all participants provided electronic informed consent. This study was conducted by the Declaration of Helsinki and was approved by the Expedited Ethics Committee of the Ecuadorian Health Ministry (Approval No. 024–2020).
3. RESULTS
3.1. Prevalence of Self-medication during Lockdown
During the onset of the global COVID-19 lockdown in 2020, a period in which Ecuador faced its most significant surge in contagion and a notable increase in excess deaths, a comprehensive collection of responses was gathered from 363 participants who engaged in the questionnaire aimed at assessing the risk for self-medication. The demographic results established that 64% of the population held a higher level of education, while 27% attained postgraduate degrees, as presented in Table 1. Most surveyed individuals spent the lockdown period in different locations: 69% in Guayaquil, one of the largest cities of Ecuador; 6.3% in Manabí; 5% in Santa Elena; and the remaining 19.7% chose to stay confined in rural areas. Furthermore, specific queries regarding the knowledge of the public about medications were subjected to analysis. The results revealed that 74% reported using medication to alleviate their symptoms. Remarkably, 60% of those surveyed demonstrated a broad understanding of medicine, particularly Over-The-Counter (O.T.C.) medi- cations.
About 67% of the population suffered pain or discomfort related to COVID-19 symptoms, and 74% indicated they took any medication to treat the condition. Additionally, 60% of Ecuadorians indicated a common knowledge about medicine, the O.T.C. medication.
The percentage of self-medication was determined by questions 7 and 8 (Table 2). The 25% of the population knew the drug dose by asking relatives or friends or reviewing the medicine leaflet, presuming indications of self-medication. An alarming number of 26% indicated that they were acquiring medicines elsewhere.
| - | Frequency (Percentage) |
|---|---|
| Gender | |
| Male | 99 (27%) |
| Female | 265 (73%) |
| Age range | |
| 16-21 | 14 (3,9%) |
| 22-30 | 134 (36,8%) |
| 31-45 | 128 (35,2%) |
| 46-65 | 88 (24,1%) |
| Educational level | |
| Primary | 1 (0,30%) |
| Secundary | 33 (9,1%) |
| Third Level (University) | 232 (62,9%) |
| Forth level (postgrade) | 97 (26,7%) |
| Pandemic Location | |
| Guayas | 252 (69,2%) |
| Carchi | 2 (0,6%) |
| Cuenca | 2 (0,6%) |
| El Oro | 7 (1,9%) |
| Esmeraldas | 1 (0,3%) |
| Foreign | 7 (1,9%) |
| Loja | 15 (4,1%) |
| Los Ríos | 7 (1,9%) |
| Manabi | 23 (6,3%) |
| Napo | 6 (1,7%) |
| Pichincha | 18 (4,9%) |
| Santa elena | 19 (5,2%) |
| Santo Domingo | 4 (1,1%) |
| Zamora | 1 (0,3%) |
| Question | Total, Population | Higher Education | Basic Education | p-value | |
|---|---|---|---|---|---|
| N | N (%) | N(%) | |||
| 7 | Who recommends you the treatment | ||||
| MD, pharmacist | 327 (89) | 266 (72) | 61 (17) | - | |
| Social media | 42 (11) | 25 (7) | 17 (4) | 0.005 * | |
| 81 | Reasons why the survey population could lead to taking medication | ||||
| Never will take medication without a prescription | 177 (49) | 161 (48) | 16 (45) | - | |
| Prevention | 82 (23) | 40 (12) | 7 (20) | - | |
| Afraid of COVID-19 | 47 (12) | 11 (3) | 3 (8) | - | |
| Family adviced | 14 (4) | 30 (9) | 5 (22) | - | |
| Read online, social media | 35 (10) | 9 (2) | 0 | - | |
| I did not have time for medical advice | 9 (2) | 78 (24) | 4 (11) | 0.4811 | |
| 9 | Where did you buy the drugs | ||||
| Pharmacy | 306 (84) | 277 (84) | 29 (82) | - | |
| Supermarkets | 36 (10) | 32 (10) | 4 (11) | 0.7813 | |
| Family and Friends | 15 (4) | 13 (4) | 2 (6) | ||
| Social media | 7 (2) | 7 (2) | 0 | ||
| 13 | How did you know the treatment doses? | ||||
| Asking an MD | 222 (61) | 198 (60) | 24 (68) | 0.4026 | |
| Asking a pharmacist | 48 (13) | 43 (13) | 5 (14) | ||
| Reading the drug instructions | 52 (14) | 47 (14) | 5 (14) | ||
| Asking friends/ family/ social media | 42(11) | 41 (12) | 1 (3) | ||
| 16 | Which moment did you stop taking the treatment? | ||||
| According to health professional recommendations | 202 (55) | 183 (55) | 19 (54) | - | |
| Not according to health professional recommendations | 162 (45) | 146 (45) | 16 (46) | 0.8797 | |
| 17 | Treatment duration | ||||
| 1-3 days | 159 (44) | 146 (44) | 13 (37) | - | |
| 3-5 days | 74 (20) | 59 (17) | 15 (42) | - | |
| 5-10 days | 78 (21) | 75 (23) | 3 (9) | - | |
| >10 days | 53 (15) | 49 (15) | 4 (11) | 0.004043* | |
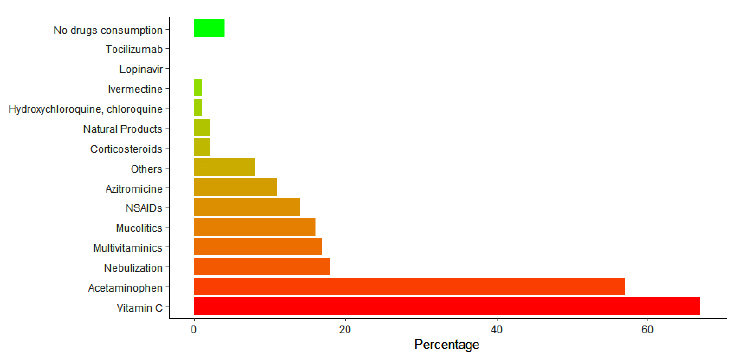
Percentage of drug consumption of the survey population during SARS-CoV-2 confinement.
Regarding drug utilization patterns, our results revealed that Vitamin C and Paracetamol were the most frequently consumed, with 57% and 67% rates, respectively (Fig. 2). Furthermore, 44% of the population used pharmacological treatments for only 1-3 days or a single dose, underlining impaired self-medication behavior (p=0.004).
3.2. Drug Risk and Severity used Analysis by Hazard Risk Assessment Score
The result of possible risks associated with drugs used by Ecuadorians during the COVID-19 lockdown in Ecuador recorded the highest Hazard Rate (H.R.) score of 25 points (question 8), underscoring the urgency of taking immediate steps to mitigate the risk of impending self-medication (55% of the population). Moreover, 35% of the surveyed population preferred therapeutic recommen- dations from the media over those provided by healthcare professionals. These findings underscore the gravity and frequency of self-medication consumption events. About 39% of the participants discontinued their treatment before seeking medical guidance, registering a Hazzard risk score of 12. Furthermore, three questions within the questionnaire attained an H.R. score of 14 points— questions 7b, 13, and 18—which applied to 74% of the population. It was determined that there is a high risk of self-medication with a score of 12 in the orange zone, which indicates that it is necessary to act within six months in these participants. In the same way, some participants presented a low risk in HRAS in the yellow zone, which means that the actions to be taken can be postponed for up to a year (Fig. 3).
3.3. Drug-related Risk of the Study Population
Despite over 80% of the surveyed population not reporting any additional symptoms or occurrences related to medications, 12% encountered discomfort after medication intake, which included symptoms, such as tachycardia at 2%, dizziness at 4%, nausea at 4%, vomiting at 2%, stomach pain at 3%, diarrhea at 3%, skin rash at 1%, pruritus at 2%, and exacerbation of dyspnea at 3%. Additionally, they were asked about the actions that they would take after presenting symptoms. These last participants were also asked about their actions after experiencing symptoms. The responses ranged from consulting a healthcare professional at 9% to self-administering another medication without supervision at 1% and seeking care at the emergency room at 2% (Table 3).
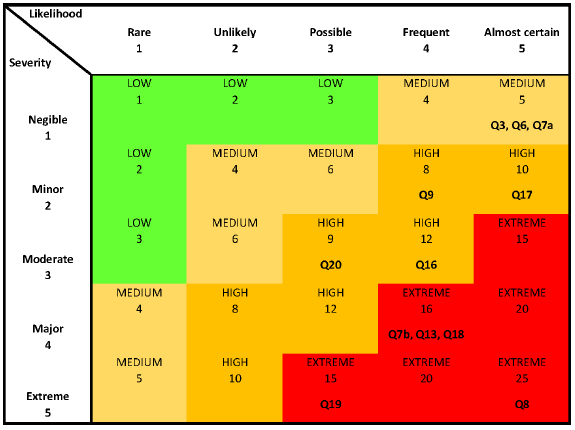
Self-medication frequency score staging by severity (according to HRAS criteria).
| Questions | N (%) |
|---|---|
| Question 18: After taking the drug or medication, did you feel any discomfort related to the drug? (Adverse drug reaction) | |
| No | 322 (88%) |
| Yes | 42 (12%) |
| Question 19: What type of adverse reaction did you present related to taking medications? | |
| Tachycardia | |
| Not answer | 343 (94%) |
| Non-existent | 12 (3%) |
| Mild | 4 (1%) |
| Moderate | 5 (1%) |
| Severe/intense | 0 (0%) |
| Dizziness | - |
| Not answer | 344 (95%) |
| Non-existent | 9 (2%) |
| Mild | 6 (2%) |
| Moderate | 3 (1%) |
| Severe/intense | 2 (1%) |
| Vomito | |
| Not answer | 341 (94%) |
| Non-existent | 12 (3%) |
| Mild | 6 (2%) |
| Moderate | 4 (1%) |
| Severe/intense | 1 (0%) |
| Nauseous | |
| Not answer | 339 (93%) |
| Non-existent | 9 (2%) |
| Mild | 7 (2%) |
| Moderate | 8 (2%) |
| Severe/intense | 1 (0%) |
| Skin rash | |
| Not answer | 347 (95%) |
| Non-existent | 14 (4%) |
| Mild | 1 (0%) |
| Moderate | 2 (1%) |
| Severe/intense | 0 (0%) |
| Skin itch | |
| Not answer | 344 (95%) |
| Non-existent | 12 (3%) |
| Mild | 4 (1%) |
| Moderate | 4 (1%) |
| Severe/intense | 0 (0%) |
| Yellowing of the skin (Jaundice) | |
| Not answer | 349 (96%) |
| Non-existent | 15 (4%) |
| Mild | 0 (0%) |
| Moderate | 0 (0%) |
| Severe / intense | 0 (0%) |
| Worsening breathlessness or choking | |
| Not answer | 344 (2%) |
| Non-existent | 10 (2%) |
| Mild | 6 (2%) |
| Moderate | 4 (2%) |
| Severe/intense | 0 (2%) |
| Question 20: What did you do or what would you do after developing any of these symptoms? | |
| Not answer | 325 (89%) |
| Ask a doctor | 29 (8%) |
| Ask a pharmacist | 2 (1%) |
| Go to the emergency room | 2 (1%) |
| Ask a family member or friend | 1 (0%) |
| Search for the response on social media | 1 (0%) |
| Take another medicine | 3 (1%) |
| Various other | 1 (0%) |
| Questions | N (%) |
|---|---|
| Question 21: Did you know that the pharmaceutical professional can assist you with your questions regarding drugs in this PANDEMIC? | |
| Yes | 195 (54%) |
| Not sure | 121 (33%) |
| No, I do not trust them | 48 (13%) |
| Question 22: Do you trust the role of the pharmacist as a health professional? | |
| Yes | - |
| No, I will never trust them | 239 (66%) |
| I do not know any pharmacist | 60 (16%) |
| - | 65 (18%) |
| Question 23: Do you prefer to find the same pharmacist for the delivery of your medications? | |
| Yes | 185 (51%) |
| No | 179 (49%) |
We also evaluated the influence of pharmacists as healthcare professionals in Ecuador. In 46% of the population, pharmacists were required to comprehend their role within the medical team better, particularly their ability to guide prescription medications. Additionally, 34% of the interviewees indicated a lack of trust and familiarity with pharmacists' role as healthcare professionals, and 49% of the population remained unaware that they could seek a consulting pharmacist for medicine delivery and dispensing (Table 4).
4. DISCUSSION
Our study has found that 67% of the population suffered any symptom of COVID-19 related or discomfort, and 74% took any medication to treat the condition. Overall, 51% of Ecuadorians practiced self-medication independently of their education level. Even though some participants previously responded that health pro- fessionals recommended the treatment, 25% of the study population determined the drug dose by asking relatives or friends or reviewing the medicine leaflet, our leading indicator of self-medication. Similarly, a recent study by Miñan-Tapia and colleagues showed that around 51.5% of the Peruvian population also practiced self-medication [19]. Another study on self-medication patterns in Ecuador found a rate of 53.5% during the first wave. Ecuadorians practice this pattern, which is more evident in women [20].
When considering the methods of medicine acquisition, 26% of the population preferred to obtain information on social media or phone group chats rather than in the pharmacy. A concerning data rely on the frequent consumption (44% of our study population) of a single dose of medications usually prescribed for a period, such as vitamins, azithromycin, and mucolytics. Single-dose consumption without professional supervision or indications is also considered self-medication [21]. Unfortunately, this single-dose consumption of antibiotics, such as azithromycin, promotes drug–resistance, a significant public health problem worldwide [22, 23]. Even though Vitamin C endovenous administration as a single dose is used for COVID-19 treatment at the hospital level [24, 25], consumption of Vitamin C at an ambulatory level with oral administration still needs reliable information about its safety and effectiveness before suggesting recommendations. Our study corroborates the literature that indicates that 56% of the population from other regions of Ecuador acquired medicines and obtained information about their use on social media, mainly during the first COVID-19 wave [9].
The lockdown experienced in many countries due to the COVID-19 pandemic has magnified facing outbreaks, which are responsible for O.T.C. medication. These lead to adverse reactions, such as hydroxychloroquine, azithro- mycin, and acetaminophen. The most used drugs for COVID-19 treatment were hydroxychloroquine [26]and azithromycin [27].
Our data show that Vitamin C was the most consumed drug in a single dose by 67% of the survey population. The following was acetaminophen, which was consumed by 54% of the population. Even though acetaminophen is an O.T.C. medication, it has risks, such as hepatotoxic damage [8]. A study in The United States showed that 48.29% of people suffered acetaminophen poisoning [28, 29]. Of this population, 72.72% suffered from kidney failure and heart issues, indicating possible toxicity unawareness due to prolonged consumption or an increased daily dose [13, 30].
Nebulization, vitamin supplementation, and combined azithromycin with hydroxychloroquine were reported to be less than 15% [31]. These differences could be due to the analysis period, considering our study has focused on the COVID-19 lockdown. Even though there is a high risk of self-medication in Ecuador, medication consumption is more related to preventing COVID-19. Nevertheless, in our study, the consumption was mainly of a single dose, compared with other studies that reported a paired self-medication prevalence. Ivermectin, acetaminophen, and azithromycin are consumed by over 50% of the population [17]. Quizpe Cañaris and colleagues determined that the primary medication consumption among the population during the lockdown was acetaminophen, with a rate of 27% [15].
The risk of self-medication is a worldwide concern that demands the development of tools to evaluate and mitigate its effects [32]. The Hazard Risk Assessment Score (HRAS) tool assesses risk factors for a given 'problem' and stratifies them according to severity and frequency [33]. This study research is necessary to have a national range of studies and limited investigation that use the HRAS tool to identify risk factors, severity, and frequency of self-medication. About 55% of the population had a risk of imminent self-medication with HRS 25 points, and 35% preferred therapy recommendations from social media rather than health professionals. We determined 55% higher risk and 74% mild risk in actions that have been considered for decreasing the HRS of self-medication in our population. The documentary framework on the unsafe practice of consumption of these medicines describes advantages, such as promoting responsible self-medication, reducing the bill of public spending by transferring it to private spending, and saving time for health professionals and citizens by reducing the number of primary care for minor symptoms [17, 34-36]. However, the current public policy does not cover a security framework for consumerism [35]. This policy affects the main use drawbacks, such as correct information being received only through advertising offers, increased costs as greater medication consumption is derived inappro- priately, and adverse side effects due to misuse. It generates the opposite outcome: irresponsible self-medication with greater distrust of the vendor and the consumer [36-38].
Even though we reported a 12% lower rate of drug-related problems in the study population, which were acetaminophen and Vitamin C. Additionally, our study identified that 49% of the survey population did not know that pharmacists could assist them during drug-related issues. These results correlated with a study conducted in the U.S. about acetaminophen consumption in which 56% of the population did not know that the pharmacist could help with O.T.C. medication to avoid self-medication, and 72% presented effects of adverse [39]. These results show an urgency in Ecuador to regulate O.T.C. medication and pharmacovigilance, which is necessary to avoid serious consequences. In the quality management of pharma- ceutical care, relevant information with a safety profile on any drug must reach the consumer [35]. This action can reduce drug-related problems, besides educating the population about the proper use of medication and the importance of contacting a health professional.
According to the outcomes of this study, self-medication is the highest risk in Ecuador. Further studies must be conducted to determine the extent of the consequences and causes of self-medication, such as how self-medication practice could increase health spending. The development of automatic information systems might be safe to contribute to the search for this over-the-counter (O.T.C.) medication, as Han-Yu Sung and colleagues developed an improved drug consultation system, especially for self-medication users [40]. As we show in our results, the image of pharmacists as health professionals must be better received. Nevertheless, pharmaceutical professionals at this level need to be more present [41]. The question arises: Who oversees identifying the effects of self-medication and preventing or resolving such problems? This approach far exceeds the activities traditionally carried out by the person who currently collaborates in most hospitals nationwide, so the new processes must be adapted to this new paradigm” [42].
CONCLUSION
In conclusion, our results indicate that at least 55% of the population had a high or maximum risk of self-medication and the appearance of drug-related problems despite the high level of education of the surveyed population. Therefore, the indiscriminate use of drugs and self-medication in the Ecuadorian population can be controlled by the development of public health educational programs that communicate with the general population. We determined that working on the health education of the Ecuadorian population and the image of pharmacists as health professionals could mitigate this growing problem. There have been overselling drugs, azithromycin and paracetamol. It could lead to an increase in intoxication and even mortality. Further, hydroxy- chloroquine and tocilizumab are still being evaluated for their effectiveness in hospitalized patients.
Health education regarding the administration, monitoring, and completion of medical treatment makes it imperative to improve the image of pharmacists as part of the multidisciplinary health team, monitor the prescription of the doctors, and reduce the side effects of the medications. Further cross-sectional studies with a larger population and extended timeline are being performed to confirm the self-medication risk and prevalence. Besides, longitudinal studies with PCR SARS-CoV-2 detection, drug consumption, and symptoms are being carried out to confirm the study.
6. STRENGTHS AND LIMITATIONS
The limitation of our study is the national sample size, which needs to be increased to improve the significance of the results. It is also important to note that self-reported data may be affected by recall bias or inaccuracies, potentially impacting result accuracy. Additionally, focusing solely on single-dose consumption of vitamins and antibiotics may limit the scope of the study by not considering chronic self-medication patterns. Further research is necessary to understand self-medication behavior using a longitudinal approach and the Hazard Risk Assessment Score, which evaluates the high risk of self-medication and drug-related problems in the population.
The study on self-medication practices among Ecuadorian adults during the COVID-19 pandemic has several strengths that enhance its academic rigor and relevance. We address a critical public health issue - self-medication - in the context of the COVID-19 pandemic. During this period, we encountered challenges in healthcare access and widespread misinformation, potentially exacerbating self-medication behaviors. The findings offer valuable insights into the response of the population to healthcare limitations during a global crisis. This detailed examination of specific self-medication behaviors, such as the single-dose consumption of vitamins and antibiotics, adds depth to the literature on risky medication practices. This focus highlights behaviors that may contribute to public health risks, such as antibiotic resistance. There is high relevance in public health, emphasizing the need for targeted public health interventions to educate the population on the risks associated with unsupervised medication use. This practical application of the findings makes the study highly valuable for public health policymakers and healthcare professionals. By focusing on the consumption of single doses of medications, particularly antibiotics like azithromycin and vitamins, the study sheds light on specific practices that may pose long-term health risks. This aspect of the research is particularly relevant for addressing issues, such as drug resistance and inappropriate medication use during the pandemic.
AUTHORS’ CONTRIBUTIONS
D. D. G., S. O.-M., A. O.-M.: Study concept or design; M. J. V.: Data analysis or interpretation; D. O., D. A.-M., L. C.-T., F. G.-F., K. A., L. D.-S.: Writing the paper; Y. S.: Data collection.
LIST OF ABBREVIATIONS
| HRAS | = Hazard-Risk-Assessment-Score |
| WHO | = World Health Organization |
| CDC | = Centers for Disease Control and Prevention |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
All experimental protocols were approved by the “Comité Nacional Expedito para Investigación sobre COVID-19” as part of the “autosalud” proposal project MSP-MSP-2020-1113-O and Expedited Ethics Committee of the Ecuadorian Health Ministry, Ecuador (Approval No. 024–2020).
HUMAN AND ANIMAL RIGHTS
All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
All participants were informed about the objectives and purpose of the study, and all participants provided electronic informed consent.
AVAILABILITY OF DATA AND MATERIALS
The data and supportive information are available within the article.
ACKNOWLEDGEMENTS
The authors wish to acknowledge the support of FCV-60-2020 and the Autosalud project for letting the study be part of the COVID-19 research. Additionally, the author dedicated this work to MD. Silvia Orellana-Manzano, may she rest in peace.
The content of this manuscript has been presented in part at the conference meeting “Experimental Biology 2021”,, Orellana-Manzano, A., Manzano, S. O., Sanchez, L. D., & Vizcaino, M. (2021). Self‐Medication Risk During SARS‐COV‐2 Confinement Pandemic. The FASEB Journal, 35(Suppl 1). https://doi.org/10.1096/fasebj.2021.35.S1.04814.

