All published articles of this journal are available on ScienceDirect.

Prevalence and Factors Associated with Chronic Energy Deficiency among Adolescent Girls and Young Mothers in Sub-Saharan Africa
Authors Info & Affiliations
Abstract
Background
Adolescent girls and young mothers (AGYM) have high nutritional needs, which puts them at risk of malnutrition. In particular, little is known about the prevalence and determinants of chronic energy deficiency (CED) of AGYM, which received less attention among researchers in sub-Saharan Africa.
Objective
The aim of the study was to examine the prevalence and associated factors of CED among AGYM in sub-Saharan Africa.
Methods
Data from the latest demographic and health surveys in four countries were used for this study: Gabon, Kenya, Malawi and Nigeria. Chronic energy deficiency, the outcome variable referred to as Body Mass Index (BMI), is classified as underweight for AGYM, whose BMI is less than 18.5kg/m2 according to the global standards established by the United Nations Children’s Fund (UNICEF) . Data analysis was done in three stages: descriptive, bivariate, and multivariable.
Results
The prevalence of chronic energy deficiency among AGYM was 7.2% in Malawi, 13.4% in Gabon, 14.9% in Kenya and 15.4% in Nigeria. The extent of chronic energy deficiency was particularly high among adolescent girls aged 15-19 in Gabon, AGYMs with no education in Nigeria and Kenya, and AGYMs from poor households in Nigeria, suggesting the necessity to provide systematic food rations to AGYMs of these specific groups. Finally, multivariable analysis shows that there are reduced odds of suffering from chronic energy deficiency among AGYM aged 20-24 years in Gabon and Kenya, compared with 15-19-year-olds. It is also revealed that education was negatively associated with chronic energy deficiency of AGYM in Nigeria and Kenya.
Conclusion
Mothers, particularly girls and young mothers, need more economic programmes to safeguard their reproductive rights through the promotion of nutritional information. This information is key for their nutritional protection, particularly for teenage girls (aged 15-19), the uneducated, and those living in poor households.
1. INTRODUCTION
Adolescence is a period of rapid growth and development by which up to 45% of skeletal growth takes place, and 15 to 25% of adult height is achieved [1]. Since it is a period of rapid growth, adequate nutrition is crucial for achieving full growth potential, and failure to achieve optimal nutrition may lead to delayed and stunted linear growth [2]. In some poorer populations, adolescent growth may be delayed and its duration extended at a young age (20-24) [3]. Nutritional challenges are even greater for adolescent mothers, given the additional energy they need to breastfeed [4]. When there is a lack of consistent nutritional intake, the breastfeeding mother will draw on her reserves to produce high-quality milk, which will affect her nutritional status [5]. Furthermore, a good nutritional status of lactating mothers is beneficial for their children's nutritional status [6].
Furthermore, poor nutritional status increases the risk of maternal deaths, which happens regularly among adolescent girls and young mothers (AGYM) in developing countries [7]. Although the mother's diet has no serious impact on the quality of her breast milk [8], it does affect the quantity of milk, which means that the children of malnourished mothers will be more exposed to malnutrition. So, nutritional challenges are particularly of great concern for adolescent girls and young mothers [9]. However, the nutritional status of AGYM is poorly documented in developing countries. Few studies analyzed the determinants of malnutrition in AGYM, especially in developing countries [7, 8]. Additionally, a study conducted in Bangladesh showed that young mothers from rural areas with low levels of education or whose husbands are not in work are significantly more at risk of suffering from malnutrition [10]. In Eastern African countries, a study found that access to information, measured by their education level and mass media use, was directly and positively associated with BMI-for-age of adolescent married girls [11].
The burden of protein energy is particularly high among African adolescents but is still little studied [12]. Few previous studies conducted in Africa showed that female adolescents are more likely to suffer from undernutrition compared to their male counterparts [13, 14]. With motherhood (pregnancy and breastfeeding), the challenges could be even greater for AGYM. To the best of our knowledge, more studies are needed to examine the nutritional status of AGYM in sub-Saharan Africa. However, a study has looked at the nutritional status of adolescents or young women in general [9] without assessing the factors specific to those who are mothers and hence more vulnerable.
Literature has shown that the prevalence of CED is high among adolescent girls and young mothers in sub-Saharan Africa, necessitating the need for this research [1, 4, 9]. Given the higher nutritional requirements of adolescent mothers as a result of breastfeeding, the prevalence of malnutrition could be even higher in this age group, especially as breastfeeding is widely practised in Africa. However, to the best of our knowledge, no study has estimated the extent of CED or investigated its determinants among adolescent girls and young mothers in sub-Saharan Africa. Thus, the focus of this research is to assess the extent of CED and, secondly, to identify the determinants of CED among AGYMs in sub-Saharan Africa in order to encourage decision-making for better nutritional protection.
2. METHODS
2.1. Data Source
This study is based on a secondary analysis of data extracted from the Demographic and Health Surveys (DHS) conducted across four countries in Sub-Saharan Africa (SSA), namely Nigeria, Gabon, Kenya and Malawi. We selected Nigeria, Gabon, Kenya, and Malawi for this study because each of these countries had recent Demographic and Health Survey (DHS) data from 2018 or later, ensuring that the analysis would reflect current trends and conditions. Additionally, based on the DHS program, these countries report a high prevalence of low BMI among adolescents and young women in their respective regions within sub-Saharan Africa, making them critical for examining trends in chronic energy deficiency. The respective countries’ DHS was conducted between 2015 and 2022. For inclusion in the study, the country must have had conducted at least one DHS survey within the study period and had available data on the Integrated Public Use Microdata Series (IPUMS) platform or DHS program website. Furthermore, one country with a high prevalence of chronic energy deficiency among women from each sub-region was identified for inclusion in the study. DHS data are nationally representative and collected using a 2-stage stratified cluster design. The standard methodology for the DHS surveys is described in the guide to DHS statistics [15]. The women's datasets were retrieved from the DHS platform. The age range of adolescent girls and young mothers included in this study is 15 to 24 years. We retained only AGYM, who had at least 1 recent child whose age was less than 24 months. For this analysis, country-level weighted samples were 1236 for Nigeria, 417 for Gabon, 1133 for Kenya and 982 for Malawi. AGYM aged 15–24 years who had complete information on the outcome variable of interest, Body Mass Index (BMI), were included in the analysis from all four countries. The selection criteria for the analytical sample size are described in Fig. (1).
2.2. Study Design
This study is a quantitative investigation which uses recent data from the four selected countries to examine the factors associated with chronic energy deficiency among adolescent girls and young mothers based on country data collected between 2015 and 2022.
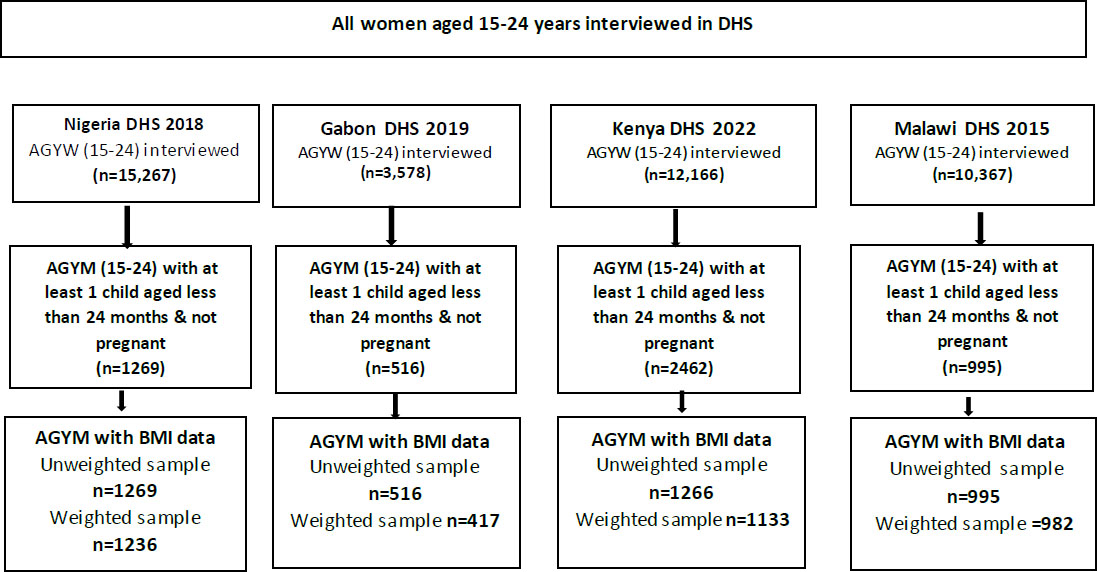
Sample derivation and inclusion criteria for the study.
2.3. Study Variables
2.3.1. Outcome Variable
The outcome variable for this study is chronic energy deficiencies referred to as Body Mass Index (BMI), classified as underweight for AGYM whose BMI is less than 18.5kg/m2, normal for those whose BMI was between (18.5-24.9kg/m2) and overweight/obese for those whose BMI was greater than (25.0kg/m2). The UNICEF global standard for the calculation of BMI was used to compute chronic energy deficiencies. The variable is given the value 1 (Chronic energy deficiency) if an individual had (<18.5kg/m2 and a value of 0 for (No Chronic energy deficiency) otherwise. BMI was used as the sole indicator of chronic energy deficiency in this study because it provides a straightforward, widely accepted measure for assessing body fat and nutritional status in relation to height and weight among adults. Additionally, BMI is an accessible and cost-effective metric that has been validated in numerous studies as a reliable indicator of energy deficiency, especially in population-level surveys such as DHS.
2.4. Independent Variables
We considered a few explanatory variables, such as age, place of residence, educational level, wealth index, sex of head of household, employment status, marital status, access to media, number of under 5 children in a household and visited health facility in last 12 months and breastfeeding status. Age was categorised as 15-19 and 20-24 years. The DHS programme employed principal component analysis to calculate factor scores for household possession of certain items as a proxy for wealth status. The factor scores were ranked and divided into tercile (poor, average and rich) to represent the household wealth index. The place of residence was categorized as either rural or urban. Education level was categorized as none, primary and secondary schools, respectively. The sex of household head is also categorized as either male or female-headed. The choice of explanatory variables was based on their conceptual relevance to the indicators accessed. The five explanatory variables (employment status, marital status, access to media, number of under 5 children in a household, and visited a health facility in the last 12 months) are all indicators of socioeconomic characteristics of individuals in SSA. Employment status and wealth index is a direct measure of socio-economic empowerment, which affects the ability of individuals to cope with chronic energy deficiency. This is also related to visiting health facilities and the number of under 5 children in the household (which can suggest whether there is enough money or capacity should the need arise). As the production of milk for breastfeeding is an important source of energy expenditure, we have also taken it into account as an independent variable.
2.5. Statistical Analysis
Data analysis was done in three stages: descriptive, bivariate, and multivariable. All analyses were performed using Stata version 17 software, with a 5% level of significance. At a descriptive stage, frequencies and percent distributions of selected background characteristics of AGYM were presented for each country. At the bivariate level, cross-tabulations with chi-square tests were used to analyse the association between chronic energy deficiency and the selected independent variables. To assess the effects of several individual-level factors on chronic energy deficiency in each country, a multivariable binary logistic regression model was applied to each country’s DHS data. Adjusted odds ratios (AOR) with corresponding 95% confidence intervals (CI) were reported. All covariates from the bivariate analyses with a significance of 0.2 were included in the multivariable logistic regression analysis.
Socioeconomic variables such as education, household wealth status, employment status, and access to media are expected to have a significant effect on chronic energy deficiency among adolescent girls and young women. For example, higher education levels often correlate with better knowledge of nutrition and health practices, potentially reducing the risk of chronic energy deficiency. Household wealth status directly influences access to nutritious food and healthcare, as individuals in wealthier households are more likely to afford a balanced diet and healthcare services. Employment status can affect nutritional status by improving financial independence and access to resources to support nutritious food access. Lastly, access to media can play a key role in shaping health awareness and behaviours, as media exposure increases access to information on nutrition, healthy lifestyles, and health-related resources, which may help mitigate chronic energy deficiency among AGYMs.
2.6. Ethical Approval
The data analysed in this study is available in the public domain at (https://dhsprogram.com/). Permission to the data was obtained from the IPUMS and DHS programs. None of the data used contain any identifying information. The original DHS Biomarker and survey protocols for each respective country were approved by each country’s Ethical Review Body and that of the Research Ethics Review Board of the Centers for Disease Control and Prevention (CDC) Atlanta. Thus, all data collection methods were carried out in accordance with relevant ethical guidelines and regulations. The DHS protocols ensured that all participants older than 18 years who were enrolled in the DHS gave their informed consent during enumeration. Additionally, parents or guardians of all participants aged 15 to 17 gave informed consent before the legal minors were asked for their permission.
3. RESULTS
Table 1 provides the distribution of the study samples across the four countries included in the study. This table on the distribution of study samples is crucial to the manuscript’s overall findings, as it provides a detailed overview of participant demographics and socioeconomic characteristics, allowing for a clearer understanding of how these factors may relate to chronic energy deficiency outcomes in the study. The table indicates that the AGYM aged 20-24 years constituted the highest proportion of respondents across the four countries. In Kenya (76.0%), Nigeria (74.8%), Malawi (69.9%) and 68.8% in Gabon of the AGYM were aged 20-24 years. For education level, secondary/higher education constituted 79.6% of respondents in Gabon, 62.4% in Kenya, Nigeria and Malawi had 43.8% and 24.5%, respectively, while adolescents with primary education in Malawi constituted the highest 69.7%, Nigeria had the biggest proportion among AGYM with no formal education at 42.1%. Furthermore, Malawi (56.2%) and Nigeria (54.1%) have the highest proportion of AGYM working. Those based in rural areas were 86.2% in Malawi, 68.5% in Kenya, 66.3% in Nigeria and 11.1% in Gabon. In the four countries, the majority of the AGYM were from households whose heads were males: 87.5% (Nigeria), 72.7% (Malawi), 69.2% (Kenya) and 63.9%) in Gabon. Nigeria (12.5%) has the least adolescents from households whose heads are females. There are more adolescents in the poor wealth index compared to other categories in all the countries. A higher percentage of married AGYM were from Nigeria (91.3%), while Gabon (44.2%) has the least married AGYM across the four countries sampled.
| Background Characteristics | Nigeria DHS 2018 (N=1236) | Gabon DHS 2019 (N=417) | Malawi DHS 2015 (N=982) |
Kenya DHS 2022 (N= 1133) |
|---|---|---|---|---|
| Age | ||||
| 15-19 | 311 (25.2) | 130 (31.2) | 295 (30.1) | 272 (24.0) |
| 20-24 | 925 (74.8) | 287 (68.8) | 687 (69.9) | 862 (76.0) |
| Residence | ||||
| Urban | 417 (33.7) | 371 (88.9) | 136 (13.8) | 357 (31.5) |
| Rural | 819 (66.3) | 46 (11.1) | 846 (86.2) | 776 (68.5) |
| Education level | ||||
| None | 520 (42.1) | 18 (4.4) | 57 (5.8) | 61 (5.4) |
| Primary | 174 (14.1) | 67 (16) | 684 (69.7) | 365 (32.2) |
| Secondary/higher | 541 (43.8) | 332 (79.6) | 241 (24.5) | 708 (62.4) |
| Wealth status | ||||
| Poor | 623 (50.4) | 215 (51.5) | 497 (50.6) | 526 (46.4) |
| Middle | 249 (20.1) | 104 (24.9) | 197 (20.0) | 205 (18.1) |
| Rich | 365 (29.5) | 99 (23.6) | 288 (29.4) | 402 (35.5) |
| Sex of Household Head | ||||
| Male | 1081 (87.5) | 267 (63.9) | 714 (72.7) | 784 (69.2) |
| Female | 155 (12.5) | 150 (36.1) | 268 (27.3) | 349 (30.8) |
| Employment status | ||||
| Not working | 567 (45.9) | 323 (77.4) | 430 (43.8) | 775 (68.4) |
| Working | 669 (54.1) | 94 (22.6) | 552 (56.2) | 358 (31.6) |
| Marital status | ||||
| Not married | 107 (8.7) | 233 (55.8) | 193 (19.6) | 362 (32.0) |
| Married | 1129 (91.3) | 184 (44.2) | 789 (80.4) | 771 (68.0) |
| Access to media | ||||
| No | 500 (40.4) | 42 (10.0) | 469 (47.8) | 164 (14.5) |
| Yes | 736 (59.6) | 375 (90.0) | 513 (52.2) | 969 (85.5) |
| Number of under 5 children in the household | ||||
| Zero-One | 533 (43.1) | 152 (36.6) | 541 (55.1) | 656 (57.9) |
| Two or more | 703 (56.9) | 265 (63.4) | 441 (44.9) | 477 (42.1) |
| Visited health facility in last 12 months | ||||
| No | 537 (43.5) | 122 (29.3) | 266 (27.1) | 301 (26.6) |
| Yes | 699 (56.5) | 295 (70.7) | 716 (72.9) | 832 (73.5) |
| Currently breastfeeding | ||||
| No | 158 (12.8) | 186 (44.5) | 103 (10.5) | 135 (11.9) |
| Yes | 1078 (87.2) | 231 (55.5) | 879 (89.5) | 998 (88.1) |
Table 2 shows the prevalence of variables significantly associated with chronic energy deficiency among adolescent girls and young mothers in the study countries. The table on chronic energy deficiency prevalence among adolescent girls and young mothers across the four countries is essential as it highlights the scope and variation of energy deficiency across key demographics, supporting a deeper analysis of risk factors within this population. Overall, age, residence, education level, wealth status, marital status, access to media, number of under 5 children, visiting health facilities in the last 12 months and current breastfeeding status are associated with chronic energy deficiency in at least one of the selected countries. For instance, age is associated with chronic energy deficiency in Nigeria, Gabon and Malawi with the highest proportion among AGYM aged 15-19 years, respectively 19.1%, 24% and 10.6%. Place of residence is associated with chronic energy deficiency in Nigeria. In the other countries (Kenya, Malawi and Gabon), no significant association was observed between chronic energy experience and place of residence. A higher proportion of AGYM with no education experienced chronic energy deficiency in Kenya (36.5%) and Nigeria (23.4%) has a significant association with chronic energy deficiency. Access to media is also associated with chronic energy deficiency among AGYM in Nigeria and Kenya, while the number of children under 5 was also associated with chronic energy deficiency in Nigeria among AGYMs. Current breastfeeding status had a significant association with chronic energy deficiency only in Malawi. Sex of the head of household, marital status and visiting health facility in the last 12 months had no significant association with chronic energy deficiency in any country.
Table 3 shows the results of the multivariable regression of factors influencing whether an adolescent girl or young mother is associated with chronic energy deficiency. This table is important as it identifies and quantifies the factors significantly associated with chronic energy deficiency among adolescent girls and young mothers, providing a data-driven basis for targeted interventions and policy recommendations. For AGYM with chronic energy deficiency, the odds of age were statistically significant for the AGYM aged 20-24 years in Gabon (aOR=0.26, 95% CI=0.11-0.60), who were less likely to experience chronic energy deficiency. The same trend is observed in Kenya, where AGYM aged 20-24 years were less likely to experience chronic energy deficiency compared to those aged 15-19 years. The significant effect of education is observed in three selected countries (Nigeria, Gabon and Kenya). AGYM with secondary or higher education in Nigeria (aOR=0.38, 95% CI=0.23-0.65) and Kenya (aOR=0.44, 95% CI=0.25-0.77) had statistically significant lower odds of chronic energy deficiency compared to those with no education. For Gabon, AGYM with secondary or higher education (aOR=9.32, 95% CI=1.29-67.33) had statistically significant higher odds of chronic energy deficiency compared to those with no education.
Table 2.
| - | Chronic Energy Deficiency | |||
|---|---|---|---|---|
| Background Characteristics | Nigeria DHS 2018 (N=1236) | Gabon DHS 2019 (N=417) | Malawi DHS 2015 (N=982) |
Kenya DHS 2022 (N= 1133) |
| Freq (%) | Freq (%) | Freq (%) | Freq (%) | |
| Age | * | * | * | - |
| 15-19 | 19.1 (14.8,24.2) | 24 (13.9,38.2) | 10.6 (7.1,15.7) | 18.1 (13.9,23.3) |
| 20-24 | 14.1 (11.8,16.8) | 8.6 (4.7,15.4) | 5.7 (3.9,8.2) | 13.9 (11.1,17.3) |
| Residence | ** | - | - | - |
| Urban | 10.1 (7.3,13.9) | 14.2 (9.2,21.3) | 10.0 (4.7,19.8) | 13.0 (8.0,20,3) |
| Rural | 18.1 (15.2,21.3) | 7.2 (3.9,13.0) | 6.7 (5.0,8.9) | 15.8 (13.2,18.7) |
| Education level | *** | - | - | *** |
| None | 23.4 (19.5,27.7) | 2.7 (0.6,11.7) | 11.2 (5.1,22,9) | 36.5 (28,45.9) |
| Primary | 15.6 (10.3,22.8) | 11.2 (2.8,35.3) | 5.9 (4.2,8.2) | 11.8 (8.8,15.7) |
| Secondary | 7.6 (5.5,10.5) | 14.5 (9.2,22.0) | 9.9 (5.8,16.5) | 14.6 (11.3,18.7) |
| Wealth status | *** | - | - | - |
| Poor | 22.4 (18.7,26.7) | 11.7 (6.4,20.3) | 5.6 (3.8,8.2) | 17.4 (14.1,21.1) |
| Middle | 8.8 (6.0,12.7) | 17.4 (8.1,33.3) | 10.2 (6.1,16.5) | 14.7 (9.7,21.5) |
| Rich | 7.8 (5.3,11.5) | 13.1 (5.3,29.0) | 7.9 (4.6,13.1) | 11.8 (7.4,18.2) |
| Sex of head of household | - | - | - | - |
| Male | 15.8 (13.5,18.4) | 15.0 (8.9,24.2) | 7.5 (5.5,10.2) | 14.4 (11.4,18.0) |
| Female | 12.6 (7.5,20.2) | 10.7 (4.5,23.3) | 6.3 (3.7,10.5) | 16 (12.2,20.8) |
| Employment status | * | - | - | - |
| Not working | 17.8 (14.5,21.6) | 12.4 (7.5,19.8) | 6.8 (4.4,10.5) | 14.0 (11.3,17.1) |
| Working | 13.3 (10.7,16.5) | 16.9 (7.8,32.9) | 7.4 (5.3,10.3) | 16.9 (12.2,22.9) |
| Marital status | - | - | - | - |
| Not married | 10.2 (5.3,18.7) | 16.5 (9.9,26.2) | 7.3 (4.3,12.3) | 15.8 (12.2,20.3) |
| Married | 15.9 (13.6,18.5) | 9.6 (4.9,18.1) | 7. (5.2,9.6) | 14.5 (11.5,18.1) |
| Access to media | * | - | - | *** |
| No | 18.7 (15.2,22.9) | 22.2 (6.6,53.5) | 6.4 (4.4,9.2) | 26.4 (20.5,33.3) |
| Yes | 13.1 (10.6,16.1) | 12.5 (8.1,18.6) | 7.9 (5.4,11.3) | 13.0 (10.3,16.2) |
| Number of under 5 children in household | * | - | - | - |
| Zero-One | 14.7 (11.7,18.1) | 9.7 (4.9,18.4) | 8.6 (6.2,11.9) | 13.9 (10.9,17.5) |
| Two or more | 15.9 (13.2,19.1) | 15.6 (9.3,24.8) | 5.4 (3.4,8.3) | 16.3 (12.5,21.0) |
| Visited health facility in last 12 months | - | - | - | - |
| No | 15.6 (12.3,19.5) | 17.8 (7.3,37.2) | 6.9 (4.1, 11.3) | 17.9 (13.5,23.4) |
| Yes | 15.2 (12.5,18.5) | 11.6 (7.2,18.2) | 7.3 (5.5,9.6) | 13.8 (11,17.2) |
| Currently breastfeeding | - | - | * | - |
| No | 10.4 (6.5,16.4) | 13.1 (7.4,22.2) | 2.5 (0.8,7.2) | 19.2 (11.6,30.2) |
| Yes | 16.1 (13.8,18.7) | 13.7 (7.7,23.4) | 7.7 (5.8,10.1) | 14.3 (11.9,17.2) |
| Total | 15.4 (13.2, 17.8) | 13.4 (8.9, 19.7) | 7.2 (5.5, 9.4) | 14.9 (12.4, 17.8) |
In Nigeria, AGYM with middle wealth status (aOR=0.43, 95% CI=0.26-0.71) or rich wealth status (aOR=0.44, 95% CI=0.26-0.75) had statistically significant lower odds of chronic energy deficiency compared to those with poor wealth status. In the other selected countries, there was no significant difference in chronic energy deficiency among AGYMs according to their wealth status. The effect of access to media has been shown in Kenya, where AGYM who have access to media (aOR=0.58, 95% CI=0.36-0.93) had statistically significantly lower odds of chronic energy deficiency compared to those who had no access to media.
These results could inform age-specific nutritional support programs targeting younger AGYM. Education also plays a key role; in Nigeria and Kenya, AGYMs with secondary or higher education have significantly lower odds of chronic energy deficiency, implying that improved education access could enhance health outcomes. Wealth status, being an important determinant of chronic energy deficiency, highlights a need for economic support and nutrition programs for lower-income households.
| - | Chronic Energy Deficiency | |||
|---|---|---|---|---|
| Background Characteristics | Nigeria DHS 2018 (N=1236) | Gabon DHS 2019 (N=417) | Malawi DHS 2015 (N=982) |
Kenya DHS 2022 (N= 1133) |
| AOR | AOR | AOR | AOR | |
| Age | - | - | - | - |
| 15-19 | 1 | 1 | 1 | 1 |
| 20-24 | 0.91 (0.61-1.35) | 0.26 (0.11-0.60)** | 0.52 (0.26-1.05) | 0.68 (0.46-0.99)* |
| Residence | - | - | - | - |
| Urban | 1 | 1 | 1 | 1 |
| Rural | 1.00 (0.61-1.65) | 0.49 (0.18-1.28) | 0.81 (0.34-1.96) | 0.85 (0.45-1.61) |
| Education level | - | - | - | - |
| None | 1 | 1 | 1 | 1 |
| Primary | 0.70 (0.41-1.21) | 5.97 (0.43-82.0) | 0.45 (0.17-1.19) | 0.29 (0.16-0.52)*** |
| Secondary/Higher | 0.38 (0.23-0.65)*** | 9.32 (1.29-67.33)* | 0.85 (0.28-2.58) | 0.44 (0.25-0.77)** |
| Wealth status | - | - | - | - |
| Poor | 1 | 1 | 1 | 1 |
| Middle | 0.43 (0.26-0.71)** | 2.17 (0.76-6.22) | 1.70 (0.84-3.42) | 0.97 (0.56-1.67) |
| Rich | 0.44 (0.26-0.75)** | 1.65 (0.56-4.87) | 1.16 (0.59-2.29) | 0.75 (0.41-1.37) |
| Sex of head of household | - | - | - | - |
| Male | 1 | 1 | 1 | 1 |
| Female | 0.95 (0.51-1.77) | 0.53 (0.18-1.52) | 0.78 (0.38-1.61) | 1.10 (0.73-1.66) |
| Employment status | - | - | - | - |
| Not working | 1 | 1 | 1 | 1 |
| Working | 0.85 (0.60-1.22) | 2.47 (0.92-6.64) | 1.10 (0.60-2.01) | 1.51 (0.95-2.39) |
| Marital status | - | - | - | - |
| Not married | 1 | 1 | 1 | 1 |
| Married | 1.13 (0.53-2.42) | 0.64 (0.29-1.41) | 1.14 (0.48-2.66) | 0.97 (0.64-1.48) |
| Access to media | - | - | - | - |
| No | 1 | 1 | 1 | 1 |
| Yes | 1.34 (0.90-1.98) | 0.34 (0.10-1.15) | 1.02 (0.58-1.81) | 0.58 (0.36-0.93)* |
|
Number of under 5 children in household |
- | - | - | - |
| Zero-One | 1 | 1 | 1 | 1 |
| Two or more | 0.93 (0.66-1.30) | 1.67 (0.50-5.62) | 0.76 (0.40-1.44) | 1.14 (0.73-1.77) |
|
Visited health facility in last 12 months |
- | - | - | - |
| No | 1 | 1 | 1 | 1 |
| Yes | 1.15 (0.79-1.67) | 0.61 (0.20-1.80) | 0.98 (0.53-1.80) | 0.84 (0.54-1.30) |
| Currently breastfeeding | - | - | - | - |
| No | 1 | 1 | 1 | 1 |
| Yes | 1.14 (0.65-1.99) | 1.26 (0.55-2.87) | 2.80 (0.86-9.13) | 0.69 (0.36-1.31) |
4. DISCUSSION
Our results show that the prevalence of chronic energy deficiency among AGYM is 7.2% (5.5, 9.4) in Malawi, 13.4% (8.9, 19.7) in Gabon, 14.9% (8.9, 19.7) in Kenya and 15.4% (13.2, 17.8) in Nigeria. In these countries, the prevalence of chronic energy deficiency among all adolescent girls and young women aged 15-24 was 9.1%, 15.3%, 15.7% and 19.8% in Malawi, Gabon, Kenya and Nigeria, respectively. For all women aged 15-49, the prevalence of chronic energy insufficiency was 7.2% in Malawi, 7.9% in Gabon, 9.5% in Kenya and 12.1% in Nigeria [16]. These results indicate that the extent of chronic energy deficiency among AGYM is almost identical to that of their 15–24-year-old counterparts overall. They also reveal that all adolescents and young people aged 15-24 constitute a high-risk group, given the particularly high level of chronic energy deficiency in this age group. This nutritional deficiency in teenage girls and mothers increases their risk of death, especially during pregnancy and in the post-partum period when the risk of death from anemia is particularly high. Programs to combat maternal mortality should also reinforce the nutritional education of AGYMs. Systematic food supplementation programs for pregnant and lactating adolescents and young women are particularly useful in sub-Saharan Africa. Also, participating in school-based physical activities and community-based sports and recreation programmes can improve the mood and overall mental well-being of AGYM. We also found that certain sub-groups, in particular adolescent girls aged 15-19 in Gabon (24 [13.9,38.2]), AGYM with no education in Nigeria (23.4 [19.5,27.7]) and Kenya (36.5 [28,45.9]) and AGYM from poor households (22.4 [18.7,26.7] in Nigeria) had prevalences almost two to three times higher than the average observed for all AGYM. These results suggest that food rations should be systematically given to AGYMs who are still adolescents aged 15-19, those who are uneducated and those from poor households.
The explanatory analysis showed that age, education, wealth status and access to the media were statistically associated with chronic energy deficiency after taking into account the confounding factors. In terms of age, it was found in Gabon and Kenya that 20–24-year-olds were less likely to suffer from chronic energy deficiency than 15–19-year-olds. In fact, young women aged 15-19 have particularly high energy requirements to complete their growth and to meet the specific needs associated with pregnancy and breastfeeding. These results demonstrate once again the need to adopt or implement adequate policies to delay the age of first pregnancy beyond adolescence (15-19 years).
In terms of education, our analyses showed that in Gabon, Malawi and Kenya, over 90% of AGYMs have at least a primary education level. In all four countries selected, the level of education of AGYM is relatively higher than that of all women of reproductive age (15-49). In addition, the extent of chronic energy deficiency among AGYM is similar or higher than among all women aged 15-49 [17]. In Gabon and Malawi, the extent of chronic energy insufficiency appears to be higher among young women with secondary education than that observed for all young women. Also, after taking into account possible confounding factors, a protective effect of education emerged in Nigeria and Kenya insofar as the risk of chronic energy deficiency is relatively lower among educated AGYM. In Gabon, the results seem to indicate a higher risk among educated AGYMs, but this may be due to the small number (18) of AGYMs in this country who were included in the analysis. A more in-depth analysis, with a larger sample size, is needed to better analyze the effects of education on the nutritional status of young adults in Gabon. A critical analysis of these results indicates that the effect of education on the nutritional status of AGYMs varies according to the country's overall level of education. In countries such as Nigeria, where the level of education of the population as a whole is relatively low [16], there is a clear and positive effect of education in the sense of a reduction in risk as the level of education rises. On the other hand, in countries such as Gabon or Malawi where the overall level of education is high, the effect of education on the individual risk of chronic energy deficiency tends to diminish [18]. Education enables them to gain access to nutritional knowledge and to increase their purchasing power so that they have greater access to food, which promotes good nutritional status [19, 20]. This is why it is commonly observed that educated populations have a better nutritional status than non-educated populations [11, 21]. However, in a context where the vast majority of the population is educated, this nutritional knowledge could spread throughout the community (neighborhood effect). In this case, educated and uneducated AGYM would have the same level of information, hence the absence of any significant effect of education. It is this diffusion effect that would explain the lack of effect of education in Gabon and Malawi. This result shows the need to reinforce nutrition education for AGYMs, especially in low-education contexts, to prevent a deterioration in their nutritional status.
In all selected countries, the proportion of girls from poor households was relatively higher (almost 50%) than that of girls from middle-income or wealthy households. This result shows that in all the countries selected, insufficient economic resources (on the part of parents or girls) “force” adolescent girls and young women into early marriage or risky sexual behaviour. Economic empowerment programmes for girls and young women are needed to safeguard their reproductive health rights. Also, on multivariate analysis, wealth status is statistically associated with energy insufficiency among AGYMs in Nigeria, with a lower risk for AGYMs from middle-income or poor households. This result indicates that, due to a lack of resources, some AGYMs are unable to eat properly, which affects their nutritional status. It is essential to set up food assistance programmes for AGYM in order to preserve the nutritional status of those who do not have the means to access quality food.
In all the countries selected, multivariate analysis revealed at least one factor associated with chronic energy deficiency, with the exception of Malawi, where the prevalence was lowest (7.2%). In fact, when the scale of a problem is relatively small, it is advisable to study the problem in depth within the groups specifically at risk in order to identify the specific factors and address them. In the case of Malawi, a study specifically targeting uneducated AGYMs is indicated to further reduce the prevalence of energy insufficiency.
The main limitation of this study is the cross-sectional nature of the data, which makes it impossible to ascertain the anteriority of factors such as access to the media and employment status compared with the onset of chronic energy deficiency in AGYMs. It should also be noted that the nutritional status of the AGYMs could vary across the months of the year following food availability, intake, and disease pattern. Thus, a longitudinal data collection would have made it possible to control for the effect of the seasons and thus better identify the determinants of EWC. Similarly, the absence of data meant that it was not possible to take into account the nutritional knowledge of young people with diabetes, which could also be associated with chronic energy deficiency.
CONCLUSION
This study has shown that the prevalence of chronic energy among adolescent girls and young mothers is high across the four countries examined. It further indicates that poor educational knowledge was negatively associated with chronic energy deficiency of AGYM, particularly in Gabon. Indicating that in a country where the citizens are highly educated, chronic energy deficiency among AGYM tends to diminish or decrease. Thus, education provides individuals access to nutritional knowledge and increases their purchasing power so that they have access to food. It is important to promote and improve the nutritional status of the communities or neighbourhoods where AGYM lives. There is also a need to provide economic empowerment programmes for girls and young women to safeguard their reproductive rights. Therefore, this study further recommends that nutritional protections for AGYMs require nutritional support programmes from the government to be implemented, targeting girls (aged 15-19 years), and the uneducated and the poor.
AUTHORS’ CONTRIBUTIONS
P.M.S and H.N.U.: Conceptualization was provided; methodology was adopted by H.N.U., MP., P.M.S., and C.A: Software was developed; M.P.: Validated the study, formal analysis and data curation were contributed; H.N.U and P.M.S., and M.P., and C.A: writing—original draft preparation were provided were involved in writing-review and editing. All authors have read and agreed to the published version of the manuscript.”
LIST OF ABBREVIATIONS
| AGYM | = Adolescent Girls and Young Mothers |
| AOR | = Adjusted Odds Ratios |
| BMI | = Body Mass Index |
| CDC | = Centers for Disease Control and Prevention |
| CED | = Chronic Energy Deficiency |
| CI | = Confidence Interval |
| DHS | = Demographic and Health Survey |
| SSA | = Sub-Saharan Africa |
| UNICEF | = Integrated Public Use Microdata Series |
| IPUMS | = Integrated Public Use Microdata Series |
ETHICAL STATEMENT
The original DHS Biomarker and survey protocols for each respective country were approved by each country’s Ethical Review Body and that of the Research Ethics Review Board of the Centers for Disease Control and Prevention (CDC) Atlanta. Thus, all data collection methods were carried out in accordance with relevant ethical guidelines and regulations.
CONSENT FOR PUBLICATION
The DHS protocols ensured that all participants older than 18 years who were enrolled in the DHS gave their informed consent during enumeration. Additionally, parents or guardians of all participants aged 15 to 17 gave informed consent before the legal minors were asked for their permission.

