All published articles of this journal are available on ScienceDirect.

Developing and Validating a Knowledge, Attitude, and Practice (KAP) Questionnaire for Pain Management
Authors Info & Affiliations
Abstract
Introduction
Nurses' knowledge, attitudes, and practices toward pain management are crucial for effective healthcare. This study aims to develop a KAP model questionnaire to assess these factors among Jordanian nurses, filling a research gap and informing targeted interventions.
Methods
A cross-sectional study validated a KAP questionnaire for assessing Jordanian nurses' pain management knowledge, attitudes, and practices. One hundred nurses completed a questionnaire adapted from existing scales, which was then reviewed by experts and analyzed statistically to ensure reliability and validity.
Results
Jordanian nurses showed moderate knowledge, attitudes, and practices toward pain management. Most were female with bachelor's degrees and short experience. Despite pain experience, few had training. A validated KAP questionnaire was developed, with reliability and validity confirmed. The study found positive relationships between attitudes, knowledge, and practices, highlighting their importance for effective pain management.
Discussion
This research confirms the effectiveness of a KAP survey in evaluating how Jordanian nurses handle pain management tasks effectively and shows that knowledge and attitudes play a role in shaping their practices; nurses who exhibit positive attitudes and possess adequate knowledge are more inclined to carry out efficient pain management procedures. The approved survey serves as an instrument for researchers and healthcare professionals to evaluate and enhance pain management techniques.
Conclusion
A validated KAP questionnaire assessed Jordanian nurses' pain management practices. The findings of the questionnaire were helpful in targeted interventions. Future research should explore generalizability and causal relationships.
1. INTRODUCTION
Pain is experienced by every individual. It has aspects related to our senses, emotions, and thoughts [1, 2]. It is a sensation that can arise from injuries, illnesses, or diseases. Pain is one of the primary reasons people seek medical help, and it greatly affects not only their physical well-being but also their emotions and social interactions [3, 4]. The complex and multifaceted nature of pain, which encompasses sensory, emotional, and cognitive components, has long been the focus of both medical and psychological research worldwide. Managing pain is crucial in healthcare because, if left untreated, it can lead to significant issues such as sleep disturbances, limited mobility, social isolation, and even psychological distress [5]. It has been indicated that the effect of untreated pain depends on the culture, while some societies have more stigma associated with pain or different norms regarding pain control [6, 7].
In the past, pain management mostly involved the administration of drugs to manage pain. However, the current developments in the field of international pain management reveal that the management of pain requires a systemic approach that encompasses both pharmacological and non-pharmacological strategies [8]. These include approaches like counseling, Cognitive Behavioral Therapy (CBT), mindfulness and other ways of complementary and alternative medicine. The following are some of the non-medication interventions that can be useful for those with chronic pain since they help to deal with the psychological and social aspects of pain that are usually not targeted in mere medication-based management [9]. For instance, research conducted in different countries, including the United States and Australia, has evidenced that CBT is effective in the management of chronic pain symptoms [10, 11], while culturally specific techniques, including acupuncture, have been effective in the Asian countries [12].
The success of pain control, therefore, depends on the skills and perception of the healthcare practitioners, especially the nurses. Nurses are in a prime position to identify the pain scores of the patients and teach the patients how to manage their pain [13]. However, the efficacy of pain control measures tends to differ in different countries, and this is determined by the healthcare systems, cultural beliefs and the availability of resources. For example, nurses in low-income countries are likely to have difficulties in offering adequate pain management as compared to their counterparts in high-income countries [14, 15].
The Knowledge, Attitudes and Practices (KAP) model, along with other theoretical models, can help to structure the analysis of how healthcare providers are responding to pain management problems. The KAP model is a conceptual framework that can help to identify an individual’s knowledge, appreciation and behavior with respect to a certain matter [3]. This model has been applied frequently in the field of public health and medicine to analyze the level of knowledge and behavior of healthcare providers and its effect on patients. The use of the KAP model has helped international studies on pain management to assess the variation in practice among healthcare providers based on cultural perception and variation in education systems [16-22].
In the context of pain management, knowledge means the understanding that an individual has about the factors that lead to pain, the signs of pain, and the measures that can be taken to prevent or treat pain [23]. Attitude is an individual's overall evaluation of something, which includes his or her opinion and feelings toward the need to treat pain, as well as his or her perception of his or her capacity to deal with pain [24]. Practices, however, are the measures that are taken by healthcare professionals in order to prevent or relieve pain for example, pain assessment, medication administration, patient teaching, and the integration of pharmacological and non-pharmacological interventions when needed [25]. However, the practices of pain management are not equally well developed in all countries; sometimes, pain management is well developed and is a significant part of clinical care, while at other times, pain management is not given the due attention that it deserves due to other medical conditions [26, 27].
It is imperative to evaluate KAP in relation to pain management in order to determine which aspects of knowledge, attitude and practice need to be enhanced, modified, or developed, particularly among the nurses who are the main providers of care. This is particularly crucial in the case of persistent or chronic pain, which needs complex and consistent management approaches. As the cultural and health care system variates around the world it is important to know how KAP factors affect pain management practices in order to develop effective interventions. Despite the increasing focus on KAP in enhancing pain management, there is still a shortage of tools that can help to measure the KAP model regarding nurses. This gap in the current research hinders the advancement of targeted interventions and makes it difficult to assess and enhance the behavior of healthcare providers in managing pain.
In order to fill this gap, the present study means to create and validate a questionnaire based on the KAP model for evaluating the nurses’ knowledge, attitudes and practices in managing patients’ pain. The development process will entail a critical analysis of previous research, feedback from the experts in the field, and testing of the instrument for reliability and validity. This tool will be employed to determine the KAP levels of nurses and to determine the areas that require enhancement with regard to pain management, together with comparing how these practices may differ in different cultural and health care contexts.
2. METHODOLOGY
In this research, a cross-sectional approach was employed to evaluate the accuracy and consistency of a questionnaire based on the KAP model for pain management among nurses in Jordan. There are 6056 registered nurses working in the Ministry of Health. Using the Krejcie and Morgan table, the appropriate sample size was determined to be 382. A random sampling technique was used to select these nurses and invite them to participate in the study. However, only 100 nurses working at hospitals in Jordan agreed to participate. While the number of participants (100 nurses) is lower than initially calculated, this reflects practical constraints in recruiting participants within a specific geographical context. Several factors, such as work schedules, availability, and limited outreach efforts, may have contributed to this lower response rate. Nevertheless, the sample of 100 participants is still considered sufficient for an initial analysis, particularly given the context of the study and its exploratory nature.
Ethical approval for this study was obtained from the Ministry of Health’s Ethics Committee, allowing data collection across all government hospitals operating under the Jordanian Ministry of Health. Informed consent was obtained from each participant, ensuring they understood the purpose of the study, the voluntary nature of their participation, and their right to withdraw at any time without any consequences. Confidentiality and anonymity were maintained throughout the study to protect participants’ identities and ensure the privacy of their responses. All data collected were used solely for the research.
The questionnaire used in the study consisted of a total of 67 questions and were divided into three sections: nurses' attitudes towards pain management (22 questions), nurses knowledge about pain management (9 questions) and nurses practices in pain management (36 questions). Respondents were asked to rate each question on a 7-point Likert scale, where 1 represented “strongly disagree” and 7 represented “strongly agree.”
To create this questionnaire, we modified existing scales from various theses and articles [28-32]. The selection of items for each section was based on previous research and expert opinion to ensure they accurately captured the knowledge, attitudes, and practices regarding pain management. For example, we changed question number 1 in the section about pain management practices from “Did you use observation to determine patients' pain?” to “Did I use observation to determine patients' pain?” This change was made to ensure respondents had an understanding of the question, making it more applicable to individual practice. Each section of the questionnaire focuses on measuring a variable. You can find details about the number of items and sources for each variable in Table 1.
| Variable name | Number of items | Original scale source | Direct source | Scale |
|---|---|---|---|---|
| Nurses’ knowledge of pain management | 9 items | [28] | [28] | Strongly disagree--strongly agree 1-7 |
| Nurses’ attitude towards pain management | 22 items | [29] | [30] | Strongly disagree--strongly agree 1-7 |
| Nurses’ practices in pain management | 36 items | [31] | [32] | Never--constantly 1-7 |
The section on attitude evaluated how nurses perceive and feel about pain management, including its importance and their confidence in managing pain. The knowledge section assessed nurses’ comprehension of pain management principles and practices. The practices section examined nurses’ actual behaviors related to pain management, such as their use of pain assessment tools and the administration of pain medications.
A Likert scale offered a variety of responses to choose from, rather than just a binary yes or no option [33]. Moreover, a 7-point scale enabled the detection of responses that might suggest understanding or experience in pain management.
In order to evaluate the validity of the KAP model questionnaire on pain management among nurses, a number of approaches were employed. First of all, the content validity of the questionnaire was ensured as it was pilot-tested by a group of pain management experts. They evaluated whether the items of the questionnaire are able to capture properly the constructs of knowledge, attitudes and practices that are related to pain management so that all the important aspects of pain management are covered. This particular process helped in establishing the comprehensiveness of the questionnaire as well as the understanding of its items to a great extent [34, 35].
Furthermore, the validity of the questionnaire was also established by involving a group of nurses who completed the questionnaire and commented on the clarity and comprehensiveness of the items. The contribution of the working nurses was crucial in identifying which parts of the instrument could be improved in order to make each item relevant and easy to understand while at the same time making sure that each item captured the right aspect of the information that was being measured. In addition, to test the model’s structure and content more effectively, the data collected through the KAP model questionnaire was tested against an existing pain management measure using Smart PLS, a software application that employs equation modeling procedures for establishing linkages between various entities. This approach allowed for the evaluation of how well the items in the KAP model survey are aligned with the notion of pain management and for the items to capture the right construct as intended.
In addition, to ensure the reliability of the KAP model survey, we calculated Cronbach’s alpha coefficient using SmartPLS to test the internal consistency of the survey. This statistical tool is useful in determining how well the questions in a study measure the specific concept in question. SmartPLS was used in computing Cronbach's alpha in order to determine the reliability of the survey and the stability of the outcomes with regard to the knowledge, attitudes and practices [36].
The researchers administered the KAP model questionnaire to nurses themselves and the participants were asked to complete the questionnaire at their respective workplaces. The participants were requested to answer the questions to the extent of their knowledge and understanding. They applied SmartPLs software to analyze the questionnaire and for the presentation of the data, they used statistics. They also used exploratory factor analysis to reduce the items of the KAP model questionnaire to its constituent parts. They computed Cronbach’s alpha using SmartPLs to determine the reliability and the internal consistency of the questionnaire.
In the analysis stage of our study, we conducted a correlation examination to explore the connection between nurses' attitudes, knowledge and practices in pain management. Our goal was to gain insight into the dynamics that impact pain management among Jordanian nurses. By examining these correlations, we were able to confirm the framework of the KAP model for pain management, thus strengthening its validity and practicality. Additionally, these correlations uncovered patterns and trends in how these three variables interact with each other, providing information for future research and the development of interventions.
3. RESULTS
3.1. Descriptive Statistics for Participants' Profile
Most of the individuals who took part in the study were women, accounting for 57% of the participants. A significant majority (82%) held a bachelor’s degree. Around 40% reported having 1-5 years of experience. Almost all of them (89%) had encountered pain at some point, with a number (76%) not having received any training in pain management. The average age of the participants was 30 years old, with a deviation of 4.773 years. The summarized findings can be found in Table 2.
| - | Frequency | Percentage | |
|---|---|---|---|
| Gender | |||
| Male | 42 | 42 | |
| Female | 57 | 57 | |
| Education | |||
| Bachelor degree | 82 | 82 | |
| Master degree | 10 | 10 | |
| Experience | |||
| From 1-5 years | 40 | 40 | |
| From 6-10 years | 33 | 33 | |
| From 11-15 years | 16 | 16 | |
| From 16-20 years | 4 | 4 | |
| Pain experience | |||
| Yes | 89 | 89 | |
| No | 11 | 11 | |
| Training | |||
| Yes | 24 | 24 | |
| No | 76 | 76 | |
| Age | Mean | Std. deviation | |
| 30 | 4.773 | ||
3.2. Descriptive Statistics for Questionnaire Constructs
The information presented in Table 3 contains data related to three questionnaire categories. Using a scale of 1, to 7 the average scores for knowledge of pain management, attitude towards pain management and pain management practices were found to be 4.5222, 4.5345 and 5.1406. Higher scores reflect more positive responses from the participants. The standard deviations for these three categories were determined as 0.94102, 0.83921 and 1.11055 respectively.
| Latent Constructs | Number of Items | Mean | Std. Deviation |
|---|---|---|---|
| Knowledge | 22 | 4.5222 | .94102 |
| Attitude | 9 | 4.5345 | .83921 |
| Pain management practices | 36 | 5.1406 | 1.11055 |
These findings suggest that the individuals involved in the study displayed a comprehension of pain management and held attitudes towards it. Additionally, they reported participating in pain management practices.
3.3. Validity Findings
In this study the researcher sought feedback on the measurement scales by sending the questionnaire to five pain management experts. These experts consisted of three lecturers, from universities College of Nursing all holding degrees and two individuals specialized in pain management. Their task was to evaluate the appropriateness and suitability of the questionnaire items. Feedback mainly focused on identifying spelling errors and grammatical mistakes, which were then addressed by making edits based on their recommendations.
Furthermore, as part of this study the researcher gauged the face validity of the measurement scales by distributing the questionnaire to ten registered nurses working in hospitals. Their role was to assess aspects such as structure, clarity, and content of the questionnaire. This phase is also aimed at gaining experience in conducting studies while evaluating research feasibility and determining time requirements for completing the questionnaire. The nurses provided feedback indicating that they found the questionnaire items clear.
To evaluate construct validity using SmartPLS methodology two measures were considered: convergent validity and discriminant validity [37]. Convergent validity refers to how different items measure a variable [38]. In this study convergent validity was assessed by calculating variance extracted (AVE) with a recommended threshold of 0.5 or higher, for each variable to ensure convergence [39]. To enhance the AVE value, we followed the following process. We removed the items with the lowest loadings from the dataset. Consequently 18 items were excluded, leaving us with 49 retained items.
As depicted in Table 4 all variables exhibited AVE values ranging from 0.502, to 0.578 which fell within the recommended range. Hence, we can conclude that all latent variables met the threshold value [AVE ≥ 0.5] and demonstrated convergent validity according to recommendations.
The concept of Discriminant validity refers to the extent to which each variable in a study's distinct from the other variables. To test for Discriminant validity, we used Fornell Larckers criterion as recommended by research [40]. According to this criterion the square roots of the variance extracted (AVE) for each variable should be greater than the correlations among all variables [39]. In line with this criterion, we found that the AVE square root values for each study variable were higher than the correlations among variables except for the attitude variable. As a result, we removed two attitude items with the loadings, from our dataset. Retained only 47 items.
| Latent Constructs | Average Variance Extracted (AVE) |
|---|---|
| Knowledge of pain management | 0.502 |
| Attitude towards pain management | 0.578 |
| Pain management practices | 0.556 |
After removing these elements, it was observed that the square root of the variances extracted (AVE) for each variable, in the study was higher than the correlations between variables. This suggests that there is validity. In Table 5 you can find the square roots of the variance extracted (AVE) highlighted in bold and the correlations between variables shown in regular font.
| Latent Variables | 1 | 2 | 3 | |
|---|---|---|---|---|
| 1 | Attitude towards pain management | 0.761 | - | - |
| 2 | Knowledge of pain management | 0.620 | 0.708 | - |
| 3 | Pain management practices | 0.738 | 0.689 | 0.746 |
Based on the construct validity assessment, it can be concluded that the KAP model questionnaire is a tool to evaluate the knowledge, attitudes and practices of nurses, in Jordan regarding pain management.
3.4. Reliability Findings
In the PLS path model, the suitable method for evaluating internal consistency reliability is through composite reliability [40, 41]. The composite reliability value, represented by Cronbach’s α, is expected to exceed 0.7 [42]. Table 6 displays details regarding the composite reliability of individual variables. The table reveals that the composite reliability values for each variable ranged from 0.800 to 0.978, surpassing the benchmark of 0.70. This outcome signifies the satisfactory internal consistency reliability of the measures employed in this study.
| Latent Constructs and Indicators | Composite Reliability |
|---|---|
| Knowledge of pain management | 0.800 |
| Attitude towards pain management | 0.905 |
| Pain Management Practices | 0.978 |
In summary, the outcomes of the validity and reliability evaluation affirm that the KAP model questionnaire serves as a valid and dependable tool for gauging the knowledge, attitudes, and practices of Jordanian nurses concerning pain management.
3.5. The Significant of Path Coefficient
The research focused on the importance of path coefficients by using 5000 bootstrapping samples to evaluate the KAP models path coefficients regarding pain management among nurses in Jordan with SmartPLs software tools. Both the information, in Fig. (1) and Table 7 show the examination of these paths aligning well with the models’ expectations.
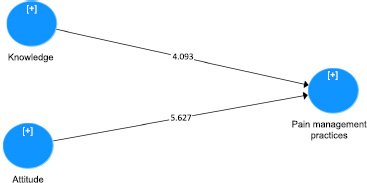
Analysis of study paths using Smart Pls Software.
| Hypotheses | Relation | Beta | SD | T-value | P-value | Findings |
|---|---|---|---|---|---|---|
| H1 | Attitude & Pain management practices | 0.505 | 0.091 | 5.627 | 0.000 | Supported*** |
| H2 | Knowledge & Pain management practices | 0.376 | 0.093 | 4.093 | 0.000 | Supported*** |
There was a strong positive relationship found between how Jordanian nurses manage pain and their beliefs and about pain management [β= 0·505; t= 5·627; p < 0·001]. This discovery indicates that nurses who have favorable attitudes towards pain management are more likely to implement pain management techniques.
A strong positive link was found between nurses’ understanding of pain management principles and their actual practices, in managing pain [β=0.376 t=4.093 p<0.001]. This suggests that nurses who possess knowledge are inclined to apply pain management techniques in their workplace.
The results strongly back up the KAP models validity and importance, in understanding the factors that affect how Jordanian nurses approach pain relief practices. They underscore the significance of integrating comprehensive education and training initiatives addressing both nurses' knowledge and attitudes toward pain management to enhance patient care and outcomes.
3.6. Evaluating the Level of R-Squared (R2) Value
Assessing the R-squared (R2) value is crucial in understanding the extent of variation in a dependent variable that can be explained by one or more predictor variables [43]. In partial least squares structural equation modeling (PLS-SEM), R-squared values of 0.26, 0.13, and 0.02 for the dependent variables can be classified as significant, moderate, and minimal, respectively [44]. In this study, an R2 value of 0.63 was recorded (Fig. 2), indicating substantial explanatory power. Specifically, the independent variables (knowledge, and attitude) accounted for 63% of the variation in the dependent variable (pain management practices).
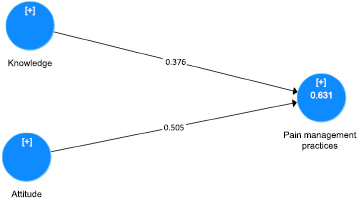
Assessment of R2 using Smart PLs Software.
Out of the 67 questions initially collected from previous literature, 47 items were found to be valid and reliable for assessing the KAP model in the field of pain management among Jordanian nurses. These 47 items were retained after rigorous validation processes, ensuring their relevance, clarity, and ability to accurately measure the targeted constructs of knowledge, attitudes, and practices. The complete and dependable questionnaire, for the KAP model elements (Knowledge, Attitudes and Practices) related to pain management can be found in Appendix A.
4. DISCUSSION
This research study investigates how Jordanian nurses approach pain management techniques in their work settings. The results support the creation and testing of the KAP model, which can be used to evaluate the knowledge levels of nurses and their attitudes and practices related to pain care procedures, thus offering a tool for this aspect of patient treatment. The data uncovered that Jordanian nurses generally have a certain level of knowledge about pain management and its implementation. However, there is still scope for enhancing their implementation of pain relief strategies while caring for patients in need.
This study’s findings highlight the links between knowledge, attitude and practices among nurses in pain management. Nurses, with a knowledge of pain management and positive attitudes are more likely to use strategies consistently. This discovery supports the core concepts of the KAP model highlighting the interconnected nature of these factors [45-47]. It emphasizes the importance of customized programs that address the behavioral aspects of pain management. Educational courses should not focus only on teaching pain evaluation and treatment techniques. They should also encourage positive views on handling pain and enable nurses to apply their knowledge effectively [48].
The KAP model survey shows that it is reliable and valid for assessing nurses understanding and attitudes towards pain management practices. This tool is useful for both researchers and healthcare providers. Researchers can employ the KAP model survey to study how pain management is carried out in nursing environments by pinpoint areas needing enhancement and measuring the impact of initiatives. Healthcare professionals can use these surveys to identify needs and customize programs to address knowledge gaps and attitude issues, among their nursing team.
Nurses' knowledge, attitudes, and practices are linked to pain management. While this study found associations between nurses' knowledge, attitudes, and practices, causality cannot be definitively established due to the cross-sectional design. Additionally, the sample size and geographical focus on Jordan may limit the generalizability of the findings. Only 100 nurses from Jordan participated in the study, which is a relatively small and geographically restricted sample. Despite limitations, the study provides valuable insights and a validated KAP questionnaire for future research. Future studies should consider longitudinal designs and explore wider applicability of the KAP model.
The study points out the relation between nurses’ knowledge, attitudes, and practices in pain management; however, it also shows the need for holistic approaches. First, it is crucial to note that the enhancement of nurses’ attitudes and the increase of their knowledge could be insufficient for the changes to be realized. Therefore, it is important that healthcare organizations create an environment that supports the implementation of the knowledge that is being provided. The training programs should not only focus on improving the knowledge of the participants but also on their attitude to manage pain effectively, thus improving the quality of patient care.
In addition, the study results offer important findings that can help to inform future research in pain management. Research on the effects of organizational factors, for instance the availability of pain relief resources on nursing practices may offer a better understanding of the role of contextual factors in pain management. Future research should also assess how the KAP model can be adapted and used in different healthcare settings and cultural backgrounds to enhance the effectiveness of pain management care.
CONCLUSION
The study has also succeeded in applying a survey model called the Knowledge Attitude Practice (or KAP) survey to explore how the nurses in Jordan perceive and deal with pain and pain management. The survey is divided into three sections and a total of 67 questions, and it was developed after reviewing the literature, getting input from the experts and being pilot-tested on a small group of participants.
The questionnaires’ validity was established through validity tests, including content validity, construct validity, and face validity. On the other hand, the questionnaires’ reliability was established since all the study variables were consistent, as the composite reliability values were greater than 0.70 for each of them.
In conclusion, the proposed KAP model survey is a useful tool that can help measure the knowledge, attitudes and practices of Jordanian nurses in the management of pain. This study reveals that increasing the level of knowledge and attitude of the nurses will, in turn, improve their performance and hence enhance patient outcomes and minimize pain severity. The results of this research support the need to design educational programs to help improve nurses’ pain management strategies and thus enhance patient results and minimize pain intensity. The KAP model can be used as a validated tool in future research, and it will act as a basis for designing interventions to change the knowledge and practices of nurses on pain control.
LIMITATIONS AND GENERALIZABILITY
The research is useful in providing the understanding and behavioral aspect of the Jordanian nurses regarding pain management; however, there are some limitations that can pose a limitation to the research and may affect the generality of the results. First, the current study was conducted using a cross-sectional survey, which enables the identification of correlations between variables but cannot establish cause-effect relationships. Although the study established a relationship between knowledge, attitude, and practices, it cannot be assumed that improvement in knowledge or attitude will lead to improvement in practices in pain management. Future research should, therefore, employ a longitudinal research design in which nurses are followed up at different points in time to see how knowledge, attitudes, and practices are interrelated with each other.
Another limitation is the sample population, where only the Jordanian nurses working in the public hospitals were involved. The findings of this study have a limited transferability if the nurses are from other countries or other healthcare institutions. Future research can also apply this study in countries with different healthcare systems and cultural values to see the transferability of the results. Also, it may be crucial to modify the KAP model questionnaire to fit the specificities of various healthcare organizations, cultural contexts, and contexts. Applying the model in different contexts and on different groups of people would strengthen the findings of the study.
Also, the study failed to control other variables that can affect the relationship between knowledge, attitudes and practices. For example, there are characteristics that may affect pain management practices, including the type of healthcare center, the nursing specialty, and the availability of pain management resources. Therefore, future research should encompass such variables to offer a more specific perspective on the relationship between contextual factors and pain management practices. This way, researching institutional resources, training programs and nursing specialties with the knowledge and attitudes of nurses may help in identifying potential for enhancement and action.
Finally, the research failed to evaluate the effect of institutional policies or organizational culture on pain management practices among nurses. Future research should also look at the part played by policies, institutions and culture in healthcare organizations in determining the knowledge, perception and practices of nurses in pain management. Identifying the factors that affect nursing performance may help to identify ways of improving pain management in healthcare organizations.
In light of this, it can be stated that the findings of this research are significant in providing useful information regarding pain management practices among Jordanian nurses; however, the limitations discussed in this paper call for more research in order to extend this study to other healthcare settings, to cross-check the findings with a different group of participants, and to assess the effect of different variables on the pain management practices using the KAP model. Thus, mitigating these limitations will assist in the enhancement of the understanding of pain management as well as the development of better practices for its execution in healthcare environments.
IMPLICATIONS FOR FUTURE RESEARCH AND PRACTICE
This research has implications for upcoming studies and current approaches to handling pain effectively. The confirmation of the KAP model questionnaire offers a trustworthy instrument for researchers and healthcare providers. This tool can be utilized in environments to evaluate the understanding levels, beliefs and behaviors of nurses concerning pain management. By integrating the KAP model survey in investigations, institutions in healthcare can acquire useful perspectives on the positive aspects and drawbacks of their pain management initiatives as well as pinpoint areas that require enhancements.
The results of the research also provide insights for enhancing pain treatment procedures in healthcare settings. A positive relationship between knowledge, beliefs, and actions indicates that educational initiatives can play a role in improving pain control. Healthcare facilities can use the data gathered from the KAP model survey to create training schemes that target particular knowledge deficiencies and promote favorable attitudes towards pain relief among nursing staff. The research also emphasizes the advantages of cultivating a workplace environment that values pain relief and enables nurses to incorporate optimal methods into their everyday duties.
Instruction: Please circling your response according to the following scale (1) Strongly disagree ← ∙∙∙ → Strongly agree (7).
| Attitude Towards Pain Management | ||
|---|---|---|
| 1. | Continuous assessment of pain and medication effectiveness is necessary for good pain management. | 1 2 3 4 5 6 7 |
| 2. | Patients have a right to expect total pain relief as a goal of treatment. | 1 2 3 4 5 6 7 |
| 3. | Patients with chronic pain should receive pain medications at regular intervals. | 1 2 3 4 5 6 7 |
| 4. | Lack of pain expression does not necessarily mean lack of pain. | 1 2 3 4 5 6 7 |
| 5. | If a patient continues to have pain after receiving pain relieving medication[s], the nurse should contact the physician. | 1 2 3 4 5 6 7 |
| 6. | diversion of patient’s attention [use of music, relaxation] can decrease the perception of pain | 1 2 3 4 5 6 7 |
| 7. | A constant level of analgesic should be maintained in the blood to control pain effectively. | 1 2 3 4 5 6 7 |
| Pain Management Knowledge | ||
|---|---|---|
| 1. | Pain can be effectively relieved. | 1 2 3 4 5 6 7 |
| 2. | It is important to give the lowest amount of medicine possible to save larger doses for later when the pain is worse. | 1 2 3 4 5 6 7 |
| 3. | Treatments other than medications [such as massage, heat, relaxation] can be effective for relieving pain. | 1 2 3 4 5 6 7 |
| 4. | Pain medicines can be dangerous and can often interfere with breathing. | 1 2 3 4 5 6 7 |
| Pain management practices | ||
| 1. | I used observation to determine patients’ pain | 1 2 3 4 5 6 7 |
| 2. | I asked my patients to determine patients’ pain | 1 2 3 4 5 6 7 |
| 3. | I asked my patients to describe the intensity of pain using a scale | 1 2 3 4 5 6 7 |
| 4. | I asked my patients to evaluate their pain | 1 2 3 4 5 6 7 |
| 5. | I asked my patients to locate the area of pain | 1 2 3 4 5 6 7 |
| 6. | I asked my patients about frequency of pain experience | 1 2 3 4 5 6 7 |
| 7. | I asked my patients to describe the pain by own words | 1 2 3 4 5 6 7 |
| 8. | I asked my patients about the most severe pain | 1 2 3 4 5 6 7 |
| 9. | I asked my patients about the least severe pain | 1 2 3 4 5 6 7 |
| 10. | I asked my patients about the average pain | 1 2 3 4 5 6 7 |
| 11. | I asked my patients about the presence of any other symptoms | 1 2 3 4 5 6 7 |
| 12. | I asked my patients about the intensity of pain before giving pain killers | 1 2 3 4 5 6 7 |
| 13. | I asked my patients about the intensity of pain after giving pain drug | 1 2 3 4 5 6 7 |
| 14. | I asked my patients about factors that increase the intensity of pain | 1 2 3 4 5 6 7 |
| 15. | I asked my patients about factors that reduce the intensity of pain | 1 2 3 4 5 6 7 |
| 16. | I asked my patients about the cause if their pain becomes worst | 1 2 3 4 5 6 7 |
| 17. | I asked my patients about non-pharmacological method to reduce pain |
1 2 3 4 5 6 7 |
| 18. | I asked my patients about the side effects of pain medication | 1 2 3 4 5 6 7 |
| 19. | I gave prescribed pain medication to my patients on a fixed schedule | 1 2 3 4 5 6 7 |
| 20. | I gave my patients a medication as necessary | 1 2 3 4 5 6 7 |
| 21. | I explained the pain experience for my patients | 1 2 3 4 5 6 7 |
| 22. | I taught my patients alternative methods to reduce pain | 1 2 3 4 5 6 7 |
| 23. | I explained for my patients the side effects of pain medication | 1 2 3 4 5 6 7 |
| 24. | I explained to my patients the drug addiction to reduce their fear | 1 2 3 4 5 6 7 |
| 25. | I taught my patients the importance of pain evaluation | 1 2 3 4 5 6 7 |
| 26. | I provided comfort after surgery to my patients | 1 2 3 4 5 6 7 |
| 27. | I helped my patients to position comfortably after surgery | 1 2 3 4 5 6 7 |
| 28. | I helped patients when they need help | 1 2 3 4 5 6 7 |
| 29. | I helped my patients to have enough sleep | 1 2 3 4 5 6 7 |
| 30. | I spent time with my patients to reduce their pain | 1 2 3 4 5 6 7 |
| 31. | I taught my patients to perform distracted activities | 1 2 3 4 5 6 7 |
| 32. | I helped my patients to ambulate such as sitting up | 1 2 3 4 5 6 7 |
| 33. | I taught my patients to support their surgical wound | 1 2 3 4 5 6 7 |
| 34. | I helped my patients to support pain area | 1 2 3 4 5 6 7 |
| 35. | I took care of patients’ wounds | 1 2 3 4 5 6 7 |
| 36. | I provided alternative activities to alleviate the patients pain | 1 2 3 4 5 6 7 |
AUTHORS’ CONTRIBUTIONS
Dr. Bashar: Study conception and design and data collection were performed; Dr. Bashar, Dr. Khalid and Dr. Hussam: analysis and interpretation of results and manuscript draft were provided by All authors reviewed and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| CBT | = Cognitive Behavioral Therapy |
| KAP | = Knowledge, Attitudes and Practices |
| PLS-SEM | = Partial Least Squares Structural Equation Modeling |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The Ethical Committee of Jordanian Ministry of Health has approved this particular study; (approval no. AB-15359).
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
AVAILABILITY OF DATA AND MATERIAL
All the data and supporting information are provided within the article.
ACKNOWLEDGEMENTS
Declared none.

