All published articles of this journal are available on ScienceDirect.

The Epidemiology and Pattern of Orthopaedic Injuries Caused by Delivery Motorbike Accidents (DMBA) at a South African Tertiary Hospital
Abstract
Background
The orthopaedic department at Steve Biko Academic Hospital (SBAH) has observed an increasing number of patients presenting with serious orthopaedic injuries due to Delivery Motorbike Accidents (DMBA). These patients sustain severe injuries that require major surgical procedures.
Objective
The aim of this study was to determine the pattern and severity of orthopaedic injuries due to delivery motorbike accidents (DMBA).
Methods
This was a retrospective qualitative observational study between 1st January, 2020, and 31st December, 2022. The details of patients involved in motorbike accidents (MBA) were collected from patient registers at the emergency department and used to obtain clinical data from medical and radiological records in the form of patient files and patient archiving and communication system (PACS), respectively.
Results
A total of 227 patients presented to the emergency department with orthopaedic injuries following a motorbike accident over a period of 3 years. Ninety-seven (97) files could not be retrieved from the patient records department. Sixty-seven (67) patients had their occupation recorded as unknown or unemployed. Sixty (60) patients had their occupation indicated in the file by the clinicians or administration clerks. Twenty-nine patients (48%) had their occupation indicated as delivery men or employees of a delivery company. All patients were males, presented after hours, and sustained multiple injuries that required surgical management. Four patients had their helmet usage status recorded in the file.
Conclusion
The study addresses a significant and underexplored issue in public health and occupational safety, providing preliminary insights into the patterns and severity of orthopaedic injuries caused by delivery motorbike accidents at Steve Biko Academic Hospital. Future research should adopt a prospective design to ensure more comprehensive data collection and explore the broader social and policy implications of delivery motorbike accidents.
1. INTRODUCTION
South African tertiary hospitals are overwhelmed by the high number of orthopaedic trauma patients observed in the accident and emergency departments, and Steve Biko Academic Hospital (SBAH) is no exception. The hospital is a teaching medical institution located in the capital city of South Africa, (Pretoria). The Department of Orthopaedic Surgery has evidenced a significant increase in patients who present with orthopaedic injuries due to delivery motorbike accidents. Some of these patients sustain severe injuries requiring major surgery to save their limbs and/or function. The Department of Orthopaedic Surgery at Steve Biko Academic Hospital (SBAH) is overwhelmed by injuries caused by already known and well-documented sources of severe orthopaedic injuries. A delivery motorbike is considered to be a significant contributor to accidents resulting in severe orthopaedic injuries. There has been a significant growth in the delivery motorbike business, with companies, such as Uber Eats, Take A lot, Mr. D delivery, and Checkers Sixty, commonly involved. The delivery sector boomed even before the COVID-19 pandemic in South Africa, and the pandemic has further accelerated its growth. It is, however, noteworthy that the drivers are expected to have licences after undergoing proper training, including motorbike riding training. The drivers are also expected to comply with all the road rules and regulations. The delivery activity usually takes place within a short radius, inside the city and residential areas. The speed limit in these areas is usually low, less than 60km/hour. The delivery motorbikes are generally easy to recognise by branded attire or reflective clothing. The increasing number of accidents involving delivery motorbikes reflects a failure on part of the society, the employee, or the employer. The aftermath of these accidents can be devastating to the livelihood of the employees. These patients are usually breadwinners who, due to the accidents, have to stay at home for a few weeks or even months without an income. They may even remain out of work for extended periods. In addition, some of these individuals are not registered by their employers and, as a result, cannot claim compensatory financial support. This highlights the need for a study to establish the patterns of orthopaedic injuries caused by delivery motorbike accidents (DMBA). This paper, thus, provides a focused examination of the increasing prevalence of orthopaedic injuries caused by delivery motorbike accidents (DMBA) at Steve Biko Academic Hospital (SBAH). It identifies a critical healthcare issue, highlighting the significant burden these accidents place on emergency and orthopaedic services. By analysing injury patterns, severity, and the occupation of affected individuals, the study aimed to bring attention to the rise of delivery motorbike services. The topic is both relevant and significant, addressing occupational risks in a burgeoning sector and offering a foundation for future research and policy recommendations. The manuscript addresses a pressing issue involving the rapid growth of the delivery motorbike industry, particularly in urban centers. It highlights the occupational hazards faced by delivery motorbike drivers, which is critical for public health and occupational safety discourse. The study lays the groundwork for more comprehensive research into the occupational risks of delivery motorbikes.
1.1. Literature Review
Orthopaedic injuries occurring due to delivery motorbike accidents in South Africa are not documented in the literature yet. There has been a rise in motorbike accidents since 1983, as noted by Dall. There is a lack of evidence on the epidemiology and pattern of orthopaedic injuries, specifically those caused by motorbike accidents. Studies confirm that there has been an increase in the use of motorbikes for different purposes in recent decades, possibly due to increasing fuel costs, intense traffic, and low purchase prices for motorcycles [1, 2]. Motorcycle accidents are one of the major causes of road death and injuries all over the world [2]. There is a paucity of literature on accidents caused by motorbikes used for delivery purposes. There is minimal data on injury costs, length of hospital stays, radiological imaging, surgical outcomes, work absence, or other long-term impacts. Motorcycles are increasingly being used for commercial transportation of parcels and goods [2]; however, accidents have been reported to contribute to more than 50% of the total number of traffic deaths in some countries. The motorcyclists must rely on helmets and specialised clothing for protection [1]. The factors related to injuries sustained include the rider’s driving skills, road environment, helmet usage, alcohol and drug use, the rider’s age and gender, inexperience, lack of driver training, riding speed, and risk-taking behaviours or violations [3-16]. Moreover, commercial motorbike riders have to drive long hours and work on a tight schedule for a better salary. Publications on the impact of motorbike accidents in terms of injuries, outcomes, and financial implications, have reported that these accidents result in significant musculoskeletal morbidity, with about 71.5% of these patients requiring orthopaedic intervention [4].
Several studies focus on orthopaedic injuries sustained during motorbike accidents, mostly delivery and non-delivery motorbike accidents. One retrospective study found almost 44% of all patients who presented to the emergency department to be admitted due to trauma and orthopaedic injuries and half of these patients were found to be involved in motorbike accidents. Motorbike accidents have been reported to be the most common cause of orthopaedic injuries requiring admission to the hospital in a study [5]. Many patients have been reported to be between 20 to 50 years of age and 92% of the patients have been reported to be male. The results have shown the most common fracture sustained to be a tibia fracture with or without a fibula fracture. Some injuries have been isolated tibia (with or without a fibula) fractures and others associated with other fractures (multiple injuries). The majority of fractures have been close at 83.2% as compared to open fractures at 16.8%. The fractures of the tibia and fibula were the most common open fractures in motorcycle injuries in the study [5]. Sixty-one percent of road traffic accidents, secondary to motorbike accidents, sustained lower extremity injuries. Forty-four percent (44%) of these patients sustained isolated lower long bone fractures, half of which were tibia fractures, followed by femur fractures. 68% of isolated tibia fractures were open fractures, and 42% of these were Gustilo III A and above. The same study found that some patients sustained severe injuries, like open femur fractures, pelvic fractures and spine fractures, as well as dislocation, resulting in complete spinal cord injury.
Non-orthopaedic severe injuries sustained included head injuries, and chest and blunt abdominal trauma. The outcomes of patients involved in motorbike accidents were poor as some patients had amputations for different indications and six patients died [5]. A descriptive cross-sectional retrospective study found many patients to sustain isolated musculoskeletal injuries at 66.9%, and 33.1% had associated head injuries. The fractures were mainly sustained in the lower limbs, followed by the upper limb [2]. These results were similar to those of another study in terms of injuries sustained during motorbike crashes. The tibia and fibula were the most commonly affected bone, accounting for 43.4% of all injuries to the lower limb. The majority of the fractures were close at 83.2%, and the rest of the fractures were open. The majority of patients required definitive surgical management before they were discharged (87.6%). In another study assessing the pattern of orthopaedic injuries in motorbike accidents, males between the ages of 16 and 30 years were more affected and sustained more than one injury [6]. Lower limb injuries and fractures were more common, accounting for 56.8% of all injuries, while upper limbs and other body regions constituted a small number of occurrences at 27.2%.
The outcomes of patients involved in motorbike accidents vary. Butts et al. conducted a study on these patients’ outcomes and found surgical procedures to be performed in more than half of the patients, accounting for 54.2%. Many patients (36.7%) were found to require emergency procedures. Other outcomes included an ICU stay for 2 days, a blood transfusion rate of 21%, a mortality rate of 4.7%, a hospital stay for 9.5 days, and a 30-day readmission rate of 7.2% [1]. One study found the duration of hospital stay to be between 1 day and 61 days with a mean of 9.1 days [2]. In another study, the mean length of hospital stay was 23.65 days, ranging from 1 to 176 days [7]. The length of stay in the hospital was reported to be a crucial method to assess the morbidity of trauma patients [2]. A prolonged duration of hospitalization leads to increased consumption of hospital resources, decreased productivity of the affected patient due to time spent in recovery, and disability of trauma victims [2]. Some patients lose their lives after an accident due to the resulting injuries and complications. Those who die constituted 4.71% and 31.5% of the total cases in two different studies. Often, motorbike accident patients are young males who are also breadwinners of their families; these injuries result in a loss of income for them, leading to a societal problem, as shared by several other studies [2, 9].
2. METHODS
2.1. Research Design
This was a retrospective qualitative observational study carried out from 1st January, 2020, to 31st December, 2022, at Steve Biko Academic Hospital.
2.2. Inclusion Criteria
All patients who presented to the emergency department following a delivery motorbike accident and sustained orthopaedic injuries were included in the study. Pedestrian-motorbike accidents and private motorbike accidents were excluded from the study.
2.3. Sample
The details of all patients involved in motorbike accidents were collected from the emergency clerk office.
2.4. Data Collection
The motor vehicle accident (MVA) administration office at SBAH in the emergency department was approached to obtain patients’ registers between 1st January, 2020, and 31st December, 2022. The details of patients classified as having motorbike accidents (MBA) were collected and used to obtain clinical data from medical and radiological records in the form of patient files and PACS, respectively.
3. RESULTS
A total of 227 patients were involved in motorbike accidents between 1st January, 2020, and 31st December, 2022. A total of 97 files could not be found in the records. 70 patients had their occupation unspecified in the file. The remainder of the 60 patients had their occupation or use of the motorbike clearly indicated in the file. This was indicated in the patient registration form, doctors’ notes (casualty, speciality doctors), and occupational therapists’ and physiotherapists’ notes. Of the patients who had their occupation indicated in the file (n=60), 29 (48.3%) patients were delivery motorbike riders (Fig. 1). These were included in the study.
3.1. Patient Demographics
All patients (n=29) were males aged 20-44 years with an average age of 29 years. The majority of the patients were between 20 and 35 years old, accounting for 75% (20) of the population (Figs. 2-5). 8 (25%) patients were above 35 years of age. No patient was under 18 years of age.
3.2. Time of Arrival
The time of arrival was found in the patients’ files and the radiological record of the PACS system. We determined whether the patient arrived during or after hours, further classifying after hours into evening and night. Daytime was defined as between 08:00 and 16:00, evening from 16:00 to 22:00, and night between 22:00 and 08:00. Sixty percent of the patients (i.e., 17 out of 29) arrived at the emergency department at after hours (16:00). A higher burden of orthopaedic trauma patients due to delivery motorbike accidents was dealt with at after hours.
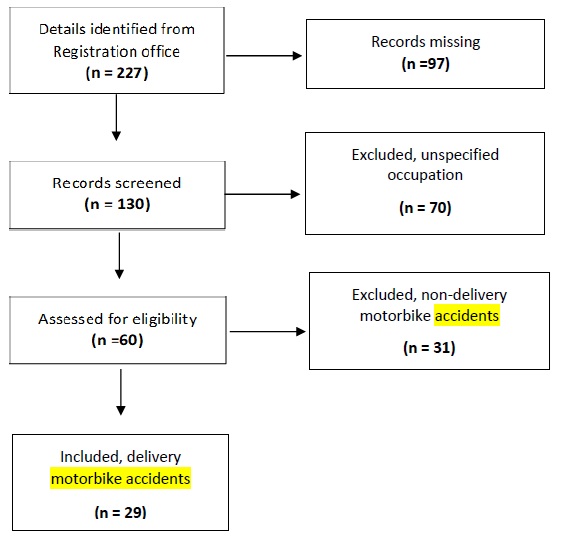
Flow diagram showing patient population [11].
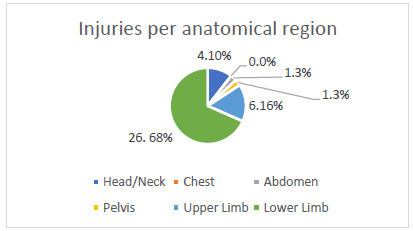
Pie chart showing injuries per anatomical region.
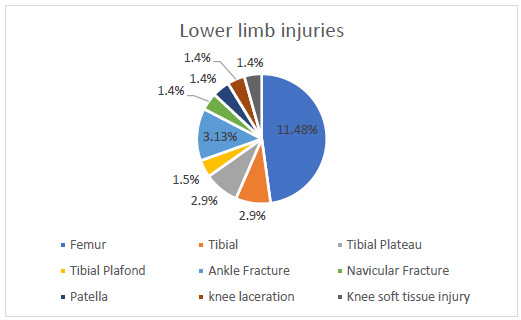
Pie chart showing lower limb injuries.
3.3. Helmet Use
The use of a helmet in motorbike accidents was not routinely indicated in the emergency doctors’ files. We sought to determine whether the patients did not wear it or if it came out during the accident, or if the doctors did not note its use altogether. Only 4 patients out of 29 (14%) were indicated to be wearing a helmet during motorbike accidents. This information was obtained from the patients' files when they arrived at the emergency department. It could not be deduced whether the motorbike riders were not wearing it during the accident or the doctors did not document it as they were focusing on attending to the patients’ injuries. Helmet use may unlikely affect the results of extremity injuries, but it may prevent head and neck injuries. Many of our patients had extremity injuries.
3.4. Injuries Sustained
The results showed that a total of 29 patients sustained 39 injuries from the motorbike accidents. 25 patients (85%) sustained fractures and soft tissue injuries were found in the remaining 15% of the patient population. Of 39 injuries, only 9 (23%) were soft tissue injuries. These injuries occurred in 5 patients. Fractures occurred in 30 injuries (n=39) sustained in 25 patients. Long bone fractures contributed to 60% of all fractures. Femur fractures constituted 61% of long bone fractures and 37.9% of all injuries sustained. Tibial fractures and humerus fractures were found in 17.35 and 11.7% of long bone fractures, respectively. Open fractures occurred in 20% (n=6 out of 30) of all fractures. The majority of injuries sustained were bony injuries, accounting for 77% (i.e., 30 out of 39).
The region most affected was the lower limb, with 79% of injuries involving the lower extremity. These injuries primarily consisted of long bone fractures, with femur fractures accounting for 52% and tibial fractures making up 9% of lower limb injuries. Other injuries included Pilon, tibial plateau, and metatarsal fractures, accounting for 4% of lower limb injuries. Seven injuries of the upper extremity included humerus fractures, distal radius fracture, scaphoid fracture dislocation, radial head fracture, and AC joint injury.
3.5. Severity
We used the pattern of injuries as a measure of the severity of the injuries sustained. We observed multiple injuries to be open fractures or those requiring surgical treatment. Multiple injuries occurred in 8 patients (n=29), accounting for 32%. Open injuries were found in 25% of all injuries, amounting to 7 of 39. There were 6 open fractures and one soft tissue injury. There were two open tibial fractures, metatarsal fractures, and distal femur fractures. In terms of injury severity score (ISS), many patients had an ISS of less than 9 and two patients (6%) had an ISS of more than 9, being 27. These were the patients who were admitted to the high care unit and ICU, respectively. Only one patient with mild traumatic brain injury had an abnormal Glasgow coma scale (GCS) score of 13-15. All other patients had normal GCS score.
3.6. Surgical Procedures
Surgical procedures were performed for 89% of the injuries (i.e., in 35 out of 39). With respect to patients, 86% of the patients were managed surgically (i.e., 25 out of 29). Surgical intervention was performed more than once in two patients. The most commonly performed orthopaedic procedures were intramedullary nailing of the femur, open reduction and internal fixation of the ankle, and tibial nailing. Other procedures included femur plating, external fixation of the Pilon fracture, navicular ORIF and K-wire fixation of the foot fractures.
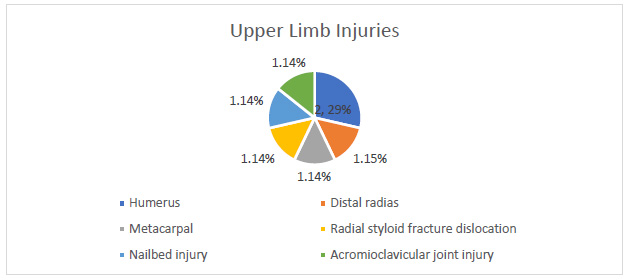
Pie chart showing upper limb injuries.
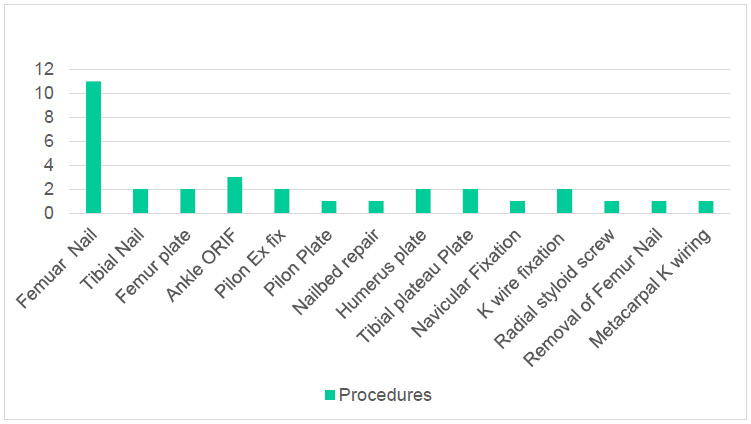
Bar graph showing the surgical procedures performed.
3.7. Secondary Objectives
These objectives included orthopaedic procedures performed on patients on arrival at the emergency department. The procedures were performed in 96% of the patients (i.e., 27 out of 29). These procedures were all non-invasive and included backslaps and skin tractions. One patient had suturing done on her. Some patients underwent non-orthopaedic procedures in the emergency department, for e.g., intercostal drain insertion. Some procedures required assistance and the use of consumables. Six patients (i.e., 6 out of 29) were subjected to special radiological investigations, including computerized tomography (CT) scan and CT angiography (CTA). These investigations estimated the severity of the injuries, showing to be associated with high costs.
Blood transfusion was performed in 14% of the patients (i.e., 4 out of 29). This is significant in the cases involving a shortage of blood. Admission to the intensive care unit (ICU) and high care unit (HCU) indicates that the patient has sustained severe injury. Any stay in these units incurs significant costs for the hospital in terms of human resources and consumables. There was one admission to the ICU and one to the HCU, respectively. Both patients were polytraumatized, with the patient in the ICU having the longest stay for 66 days.
3.8. Length of Stay
The length of stay was classified into three categories: less than 48 hours, 48-96 hours, and more than 96 hours. More than 50% of the patients stayed for more than 96 hours (5 days). Those who stayed for less than 48 hours and 48 to 96 hours constituted 25% of the population.
3.9. Readmissions
There were three readmissions due to another MBA. The first patient was a polytrauma patient who had not sustained any fractures, and he was admitted for more than 14 days. The patient presented 9 months later, within a year from discharge, with open tibial and humerus fractures, and he was managed surgically. The second patient sustained a medial malleolar fracture that was treated surgically and the patient stayed for 5 days. The patient sustained a more severe tibia plateau fracture Schatzker 6 a year after the initial accident. The third patient had a subtrochanteric femur fracture and an open metatarsal fracture, and was taken to the operation theatre for intramedullary nailing and k-wire fixation of the metatarsal fracture. This patient stayed for more than 5 days; he was further involved in another delivery MBA after 8 months and was admitted for plating of the distal femur fracture and proximal tibial plateau fracture. He sustained a floating knee injury, Frazer 2C, which was a more severe injury than the initial presentation. Ten percent of the patients suffered repeat motorbike accidents that resulted in more severe injuries.
3.10. Data Analysis
In this study, descriptive analyses were performed using frequencies, percentages, and graphical representations. These analytical methods proved to be adequate for most results of the variables and a conclusion could be made without ambiguity. These analyses were performed for patients who sustained multiple injuries and open fractures, arrived at the emergency department, had longer lengths of stay, and underwent readmissions. Multiple injuries occurred in 9 patients and 4 patients out of 9 presented to the emergency department in the evening. Three arrived during the day and 2 at night. Five (out of 9) of these patients were younger than 35 years. All the patients were taken to the operation theatre for some surgical procedures. Open fractures were sustained by 6 patients in this study, and 50% of these patients arrived during the day. Half of these patients were older than 35 years and they were all operated on during their hospitalization. In terms of readmissions, the number of patients was too small to analyse and arrive at any significant conclusion. Of the three patients in the study who were readmitted following another delivery motorbike accident, two were younger than 35 years, and one of them presented during the day, while the other in the evening, and one at night. No association between readmission with age and time of arrival was found. Descriptive analysis was also performed on prolonged length of stay, defined as more than 96 hours (5 days) in this study. 15 patients (50%) in the study were hospitalized for more than 5 days. 66.6% of these patients were between 18 and 35 years of age, and the remainder were older than 35 years. 8 out of 15 patients presented in the evening, 5 during the day, and only 2 patients presented at night. 9 out of 15 patients who stayed more than 5 days sustained multiple injuries. All these patients were taken to the operation theatre for a surgical procedure.
| Variable | Delivery n (%) | Non-delivery n (%) |
|---|---|---|
| Total | 29 | 31 |
| Age (years): <18 | 0 | 1(3) |
| 18-35 | 21 (72.4) | 17 (54.8) |
| >35 | 8 (27.5) | 13 (41.9) |
| Gender: Male (%) | 29 (100) | 26 (83.8) |
| Female (%) | 0 (0) | 5 (16.1) |
| Helmet use (%) | 4 (14) | 1 (3.2) |
| Time of arrival | ||
| Day (08:00-16:00) | 11 (37.9) | 12 (38.7) |
| Evening (16:00-22:00) | 11 (37.9) | 6 (19.3) |
| Night (22:00-08:00) | 5 (17.2) | 6 (19.3) |
| Unknown | 1 (3.4) | 7 (22.5) |
| Total injuries | 39 | 41 |
| Bony | 30 (76.9) | 35 (85.3) |
| Soft tissue | 9 (23) | 6 (14.6) |
| Open injuries | ||
| Upper extremity (%) | 8 (20.5) | 16 (39.0) |
| Clavicle | 0 | 5 |
| Shoulder/ACJ | 1 | 1 |
| Proximal humerus | 0 | 1 |
| Shaft humerus | 2 | 0 |
| Radial neck fracture | 1 | 0 |
| Shaft radius/Ulna | 0 | 1 |
| Distal radius/Ulna | 1 | 1 |
| Metacarpal | 1 | 4 |
| Nailbed injury | 1 | 0 |
| Scaphoid fracture dislocation | 1 | 1 |
| Lower extremity (%) | 28 (71.7) | 18 (43.9) |
| Femur fracture | 0 | 2 |
| Intertrochanteric | 2 | 1 |
| Subtrochanteric | 8 | 3 |
| Shaft femur | 2 | 1 |
| Knee soft tissue injury | 2 | 0 |
| Distal femur | 0 | 0 |
| Segmental | 1 | 1 |
| Patella | 2 | 1 |
| Tibia plateau | 2 | 1 |
| Shaft tibia/fibular | ||
| Distal tibia/fibular | 2 | 1 |
| Ankle | 4 | 1 |
| Metatarsal | 1 | 0 |
| Lisfranc injury | 1 | 0 |
| Navicular | 1 | 0 |
| Head/Neck | 4 (10.2) | 2 |
| Chest | 0 | 2 |
| Abdomen | 1 (2.56) | 0 |
| Pelvis | 1 (2.56) | 1 |
| Spine | 0 | 2 |
| Surgical procedures | ||
| Performed | 34 (87.9) | 14 |
| Not performed | 5 (12.8) | 2 |
| Unknown | 0 | 15 |
| Readmissions | 3 | Unknown |
| ICU admission | 1 | 2 |
| HCU admission | 1 | 0 |
| Blood transfusion | 4 | Unknown |
| Injury severity score | ||
| <9 | 27 | 28 |
| 27-Sep | 2 | 3 |
| >27 | 0 | 0 |
| Glascow coma scale | ||
| 13-15 | 27 | 28 |
| 13-Aug | 2 | 3 |
| <8 | 0 | 0 |
3.11. Non-delivery Motorbike Accidents
The results showed a total of 31 patients to be involved in non-delivery motorbike accidents and to sustain 41 injuries. There were five (16%) females; one patient was less than 18 years of age, 17 (54.8%) patients were between 18 and 35 years, and 13 patients (41.9%) were older than 35 years. Only one patient (3%) was documented to have been wearing a helmet. Many patients (12 out of 31) arrived between 08:00 and 16:00, and 6 patients (19%) between 16:00 and 22:00 and 22:00- 08:00, respectively. The time of presentation was not established in 7 patients’ files. There were two patients admitted to the ICU. Twenty-two percent of patients (7 out of 31) stayed less than 24 hours in the hospital, 5 stayed for 24 to 96 hours, and 7 patients were admitted for more than 96 hours. The length of stay was not indicated in 12 patient folders. Thirty-one patients sustained 41 injuries and multiple injuries occurred in 7 patients (22.5%). The highest number of injuries (18 out of 41) occurred in the lower limb at 43.9%, followed by the upper extremity at 39%. Two injuries affected the head/neck, chest, and spine regions, respectively. One injury occurred in the pelvis and no abdominal injury was recorded. Soft tissue injuries constituted 14.6% and the rest of the injuries were fractures. Surgical procedures were performed in 15 patients (48.3%). Three patients were treated conservatively and the mode of treatment could not be established in 14 patients (45.1%) (Table 1).
4. DISCUSSION
This is one of the first three studies on delivery motorbike accidents in the whole country of South Africa presented at the South African Orthopaedic Congress in 2023. There are countries where motorbikes are used mostly for business purposes, like Vietnam in Southeast Asia [10]. This is the first paper to explore the epidemiology, pattern of injuries, and treatment of orthopaedic injuries caused by delivery motorbike accidents. Orthopaedic injuries require special attention because they include fractures that take approximately 6 weeks to heal and several weeks of rehabilitation program. The patients require a multidisciplinary team of healthcare workers, including physiotherapists and/or occupational therapists, to assist them in returning to their normal duties and activities of daily living. The anecdotal is that patients involved are mostly immigrants from other countries who work for delivery companies in South Africa.
Although with several limitations, such as involving a small population and focusing on commercial motorcycles, this study found almost 50% of motorbike accidents to occur due to delivery purposes, being higher than 32.1% and 43% found in other studies; one study also involved a high number of unconfirmed commercial motorcyclists [17-19]. This study has confirmed injuries occurring due to delivery motorbike accidents to be common at Steve Biko Academic Hospital, being a significant contributor to the high burden of trauma experienced at the hospital. There have been found notable differences between the delivery and non-delivery groups. The non-delivery group has involved five female patients and a higher number of older patients, being more than 35 years of age. The commonly encountered injury has been found to be a fracture of the clavicle. The injury patterns between the upper and lower extremities have been less obvious as compared to the delivery group. Other findings have been found to be similar between the two groups. The study has found all the patients in the delivery group to be young males, presenting at after hours (16:00) with lower limb injuries requiring surgical treatment. This implies people to be possibly tired from work and ordering food instead of cooking. This is also the time when the delivery bikers receive many orders as people are on their way back from work. The findings emphasize the need for targeted interventions, such as improved safety measures for delivery drivers and enhanced trauma care protocols.
The increase in the use of delivery motorbikes in South Africa has been rather rapid, occurring within a few years. However, the increase in motorbike accidents in general was on the rise in 1983, as noted by Dall [20]. There is a paucity of literature on motorcycle accidents in South Africa both for private use and commercial purposes. An annual study conducted over four years on both delivery and non-delivery motorbike accidents found an increase in the delivery group with no increase noted in the non-delivery motorbike accidents [9]. The current study found that all patients were young males with the age ranging between 20 and 44 years. Seventy-five percent (75%) of patients were between less than 35 years. Similar findings were noted in other studies [8, 17, 19]. The current study did not involve any teenage patients. Other studies have found most workers to be single (65%), internal migrants (57%), and to not have any university degree (63%); working as a delivery rider was the only occupation for 61% of the respondents and 28% were students [10]. Our study did not explore patient demographics other than age and gender. Mustisto et al. found 87.5% of their patients to be male and six of them to be less than 15 years old [7]. The peak age group affected was the 21-30-year-olds, comprising 41.6% of the population. The current study shared similar peak age findings. The majority of the patients (68.4%) were informally employed as commercial motorcyclists or casual labourers and attained primary (41.3%) and secondary (39.5%) level education [7]. Other studies have found the patients to be younger in the delivery group than those in the non-delivery group [9]. They have also found the rule violation rate to be high in riders aged less than 30 years. We, however, did not explore the circumstances leading to the accidents, such as road sign violation, in the current study.
The most sustained injury was found to be lower limb fractures, with femur fractures being the most prevalent; 90% of them were treated surgically. This pattern of injuries has also been demonstrated by several publications [6, 9, 12, 15, 21]. The results showed that a total of 29 patients sustained 39 injuries from motorbike accidents; 25 of these patients (85%) sustained fractures, and soft tissue injuries were found in the remaining 15% of the patient population. The study also found less than a quarter of the injuries (i.e., 9 out of 39) to be soft tissue injuries. Fractures occurred in 30 injuries (n=39) sustained by 25 patients. The majority of injuries sustained in this study were bony injuries at 77% (i.e., 30 out of 39). Injuries to the head/neck, chest, and abdomen were low, as also reported by other authors [6, 9, 12, 15]. However, some studies have involved craniofacial injuries in the highest numbers, followed by upper limb, pelvic-abdominal, and lower extremity fractures as the least common injuries [12, 13, 22]. Upper limb injuries comprised 53% of the injuries in one study [14].
Contrary to the DINED study [8], the patients in the current study sustained major injuries, and lower extremity injuries were more prevalent than upper limb injuries. One study found a higher proportion of extremity injuries in the delivery group than in the non-delivery group [9]; the study reported lower extremity injuries to be most common at 46.4%, followed by head and face injuries at 34.4%, trunk injuries at 24.7%, and upper extremity injuries at 22.9%. A similar pattern has been displayed by several studies [8, 9, 12].
The severity of injuries was assessed using associated variables, such as multiple injuries, surgical treatment of the patient, length of stay, emergency department procedures, special investigations, blood transfusion, and admission to ICU/HCU. Thirty-six percent of the patients sustained more than one injury during the accident. Emergency department procedures were performed in 96% of the patients (i.e., 27 out of 29). These were all non-invasive and included backslaps and skin tractions. Special radiological investigations in the form of computerized tomography (CT) scan and CT angiography (CTA) were performed for 6 out of 29 patients (20%). Blood transfusion was performed in 14% of patients (i.e., 4 out of 29). Although it accounted for a small number of patients, it is significant in cases generally having a shortage of blood. The admission to the intensive care unit (ICU) and high care unit indicates the patient to be severely injured. There was one admission to the ICU and HCU, respectively. One study had a similar number of ICU admissions, accounting for 6.9% of the patients [7]. More than 50% of our patients stayed for more than 96 hours in the hospital (5 days). Long hospital stay is associated with elevated hospital costs and is considered to be a crucial method for estimating the morbidity of trauma patients [2]. It also leads to increased consumption of hospital resources, disability, and decreased productivity of the affected patient [2].
Surgical procedures were performed for 89% (i.e., 35 out of 39) of the injuries and 86% (i.e., 25 out of 29) of patients, respectively. Surgical intervention was done more than once in two patients. The most commonly performed orthopaedic procedures were intramedullary nailing of the femur, open reduction and internal fixation of the ankle, and tibial nailing. The number of surgeries during the same admission was likely once; however, three patients (6.6%) underwent surgical procedures twice in the same admission period.
Secondary findings of this study included the time of arrival at the emergency department; 60% of patients arrived at after hours (16:00). The delivery group had a peak around noon with respect to the admissions that did not exist in the non-delivery group, while the greatest number of crashes occurred between 17:00 and 21:00 [9, 17, 19]. The delivery group had a higher proportion of individuals wearing a helmet (77.9%) than the non-delivery group (63.2%). Only 4 patients in the current study had their helmet use stated in their files. Other studies have found more injuries on Saturday and Sunday, and 60% of injuries to occur at night time. The current study found a similar trend in terms of time of presentation. Some studies have found 73.5% of courier crashes to occur in the daytime and 26.5% to occur at night (from 18:00 to 06:00) [9, 22]. The rule violation rate has been found to be high at night (12.4%) [3]. The peak time for accidents in our study was after 16:00. We did not explore the outcomes of the patients; these have been expected to be long stays in the hospital and prolonged rehabilitation periods at home before returning to work. Their families have been expected to be severely affected by these accidents.
5. LIMITATIONS
The occupation data in this study were limited, with 67 patients listed as “unknown or unemployed”. Exploring strategies to improve the accuracy of this data, such as direct patient interviews at admission, could enhance future research. A small population of patients were confirmed motorbike riders (i.e., 60 out of 130). Many patients who were involved in motorbike accidents had their occupation not indicated in the files and also other clinical data was not complete in many of the files. All the patients with incomplete data were excluded from the study. The data capturing system at SBAH should be improved to an electronic and/or digital system. This can ensure complete and accurate data capture from patients on presentation at the emergency department.
6. RECOMMENDATIONS
The authors recommend addressing the data gaps and improving the robustness of future research. This can assist in determining the profiles of the patients, their employers, and the financial burden caused by these injuries on the national health system, as well as patients’ outcomes. The traffic department is also recommended to monitor the licensing and training policies of the delivery motorbike riders. The Department of Employment should work together with the courier companies in South Africa to assist employees following an accident.
CONCLUSION
This study has addressed a significant and underexplored issue in public health and occupational safety, providing preliminary insights into the patterns and severity of orthopaedic injuries caused by delivery motorbike accidents at Steve Biko Academic Hospital. While the findings have highlighted important trends, the study’s limitations, particularly regarding data completeness and reporting on helmet usage, warrant a cautious interpretation of the results. Future research should adopt a prospective design to ensure more comprehensive data collection and explore the broader social and policy implications of delivery motorbike accidents. By addressing these gaps and contextualizing the findings within national and global frameworks, the study has the potential to contribute meaningfully to public health policy and injury prevention strategies.
AUTHORS’ CONTRIBUTION
It is hereby acknowledged that all authors have accepted responsibility for the manuscript's content and consented to its submission. They have meticulously reviewed all results and unanimously approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| SBAH | = Steve Biko Academic Hospital |
| DMBA | = Delivery motorbike accident |
| ED | = Emergency department |
| HC | = High care unit |
| ICU | = Intensive care unit |
| PACS | = Picture Archiving and Communication System |
| ORIF | = Open reduction and internal fixation |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was conducted following the obtainment of ethical approval by the Ethics Committee of the Faculty of Health Sciences, University of Pretoria, South Africa, (clearance certificate number: 436/2022).
HUMAN AND ANIMAL RIGHTS
All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
AVAILABILITY OF DATA AND MATERIALS
The data sets used and/or analysed during this study are available from the corresponding author [D.N] upon request.
ACKNOWLEDGEMENTS
Declared none.

