All published articles of this journal are available on ScienceDirect.

Effect of Drinking Water Quality on Birth Outcomes: A Systematic Review
Abstract
Objective
This review aimed to analyze the effects of drinking water contaminants during pregnancy on birth outcomes, focusing on chemical contaminants, including heavy metals, nitrates, and disinfection byproducts.
Methods
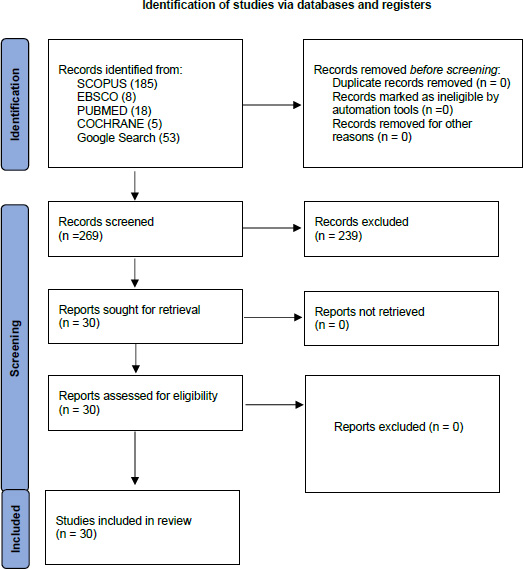
A literature search was conducted using SCOPUS, EBSCO, PubMed, Cochrane, and Google Scholar databases. The review included English-language prospective cohort studies and clinical trials published between 2007-2022 that focused on healthy pregnant women and measured birth outcomes. From 269 articles identified, 30 met the inclusion criteria.
Results
Analysis of 30 studies encompassing over 4 million births demonstrated significant associations between water contaminants and adverse birth outcomes. Arsenic exposure below 10 μg/L was associated with an increased risk of very low birth weight (AOR 1.14) and preterm birth (AOR 1.10). Nitrate concentrations of 5-10 mg/L were linked to higher rates of spontaneous preterm birth. Combined exposure to multiple contaminants demonstrated stronger effects than individual exposures, particularly during the second trimester.
Conclusion
Evidence demonstrates that exposure to water pollutants during pregnancy, even at levels below current regulatory guidelines, has a significant impact on birth outcomes. Recommendations include increased monitoring during pregnancy, particularly for private well users, reviewing regulatory standards, and implementing tailored treatments for vulnerable populations.
1. INTRODUCTION
The health and well-being of expectant mothers and their developing fetuses during pregnancy represent a critical public health concern, with numerous environ- mental factors influencing outcomes. Among these factors, drinking water quality has emerged as a significant focus in maternal-fetal health research. Drinking water quality, defined as the chemical, physical, and biological characteristics of water in relation to established standards for safety and public health [1], plays a fundamental role in determining health outcomes worldwide. Birth outcomes, encompassing measures such as birth weight, gestational age at delivery, congenital anomalies, and fetal growth parameters, are sensitive indicators of environmental influences during pregnancy.
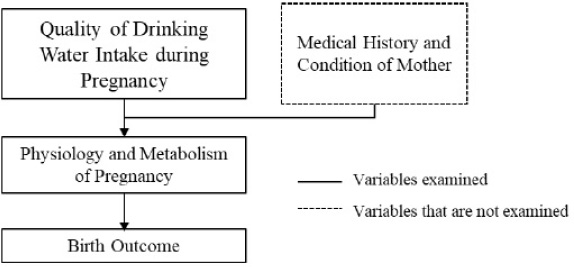
Conceptual framework.
Recent epidemiological studies have demonstrated an alarming increase in adverse birth outcomes potentially linked to environmental exposures. The World Health Organization estimates that approximately 2 billion people globally consume drinking water contaminated with chemical or biological agents that exceed safety thresholds [2]. This exposure risk is particularly concerning for pregnant women, as demonstrated by comprehensive biomonitoring studies. A landmark collaborative investigation between the Harvard School of Public Health and the Centers for Disease Control examined 87 distinct chemicals in mother-fetus pairs, revealing that nearly all these substances could traverse the placental barrier [3]. This finding fundamentally challenged previous assumptions about fetal protection and highlighted the urgent need to address water quality issues, especially for pregnant women.
The scope of water contamination concerns has expanded significantly in recent years. While traditional focus centered on microbial contamination, emerging research has identified various chemical contaminants as potential threats to fetal development. These include heavy metals (e.g., arsenic, lead), agricultural chemicals (e.g., nitrates, pesticides), and disinfection byproducts [4, 5]. A meta-analysis by Smith et al. [6] found that exposure to these contaminants during pregnancy was associated with a 20-40% increased risk of adverse birth outcomes.
Despite growing evidence linking water quality to birth outcomes, several critical research gaps persist such as limited understanding of the combined effects of multiple contaminants, as most studies focus on single agents [7], insufficient data on exposure timing and critical windows of vulnerability during pregnancy [8], inadequate assessment of how different water sources (municipal, private wells, bottled water) may influence exposure risks [9], and limited research on the effectiveness of current water quality standards in protecting fetal health [10].
Furthermore, existing reviews have typically focused on specific contaminants or particular birth outcomes, leaving a need for a comprehensive analysis of the broader relationship between water quality and birth outcomes. Maternal exposure to contaminated drinking water has been linked to various adverse outcomes, including low birth weight, preterm birth, and congenital anomalies [11, 12]. However, the strength and consistency of these associations vary across studies, highlighting the need for an evaluation of the evidence.
The primary objective of this review was to consolidate and analyze existing research on the relationship between various parameters of drinking water quality and adverse birth outcomes. Through meticulous examination and synthesis of findings from diverse studies, this review aims to provide a comprehensive understanding of these relationships. These insights are vital for informing public health policies, guiding targeted interventions, and identifying areas requiring further research. The knowledge gained will be instrumental in promoting access to safe drinking water for pregnant individuals, with the ultimate goal of reducing the incidence of adverse birth outcomes.
2. METHODS
This review examined the relationship between drinking water quality during pregnancy and birth outcomes, focusing on summarizing and synthesizing current evidence from the literature. The review methodology employed a narrative approach to analyze and interpret findings from diverse studies (Fig. 1).
2.1. Literature Search Strategy
A comprehensive literature search was conducted using five electronic databases: SCOPUS, EBSCO, PubMed, Cochrane, and Google Scholar. The search strategy combined MeSH terms and free-text words using Boolean operators. The primary search string was: (“water quality”[MeSH Terms]) OR ((“pregnant”[All Fields] AND “birth outcome”[All Fields])). Additional search terms included: “drinking water quality” OR “water quality” OR “contamination” AND “pregnancy” OR “birth” OR “fetal”
| Databases | Search Strategies | Found | Used |
|---|---|---|---|
| SCOPUS | “water quality” [MeSH Terms] OR (“pregnant”[All Fields] AND “birth outcome” [All Fields]) | 185 | 29 |
| EBSCO | “water quality” [MeSH Terms] OR (“pregnant”[All Fields] AND “birth outcome” [All Fields]) | 8 | 0 |
| PUBMED | “water quality” [MeSH Terms] OR (“pregnant”[All Fields] AND “birth outcome” [All Fields]) | 18 | 0 |
| COCHRANE | “water quality” [MeSH Terms] OR (“pregnant”[All Fields] AND “birth outcome” [All Fields]) | 5 | 0 |
| Google search | “water quality” [MeSH Terms] OR (“pregnant”[All Fields] AND “birth outcome” [All Fields]) | 53 | 1 |
AND “outcome” OR “birth outcome” OR “birth weight.” The search was restricted to English-language publications from January 2007 to December 2022. The complete search results by database are presented in Table 1.
2.2. Study Selection
2.2.1. Inclusion Criteria
Studies were selected based on the following criteria i.e., original research published in English, published between 2007-2022, peer-reviewed journal articles, and full text available. The population criteria were pregnant women without pre-existing medical conditions (defined as the absence of chronic diseases such as diabetes, hypertension, or autoimmune disorders documented at the first prenatal visit), singleton pregnancies, and women aged 18-45 years. The study design criteria were clinical trials or prospective cohort studies, clear documentation of exposure assessment methods, birth weight as a primary or secondary outcome measure, and sample size ≥50 participants.
Studies were excluded if they focused on animals or in vitro studies, included only women with pre-existing conditions, were case reports or series, or lacked quantitative exposure assessment.
2.2.2. Types of Contaminants Considered
The review examined studies investigating both inorganic and organic contaminants in drinking water. Inorganic contaminants included heavy metals (arsenic, lead, mercury) and nitrates, while organic contaminants encompassed pesticides and disinfection byproducts. Only studies with clearly defined exposure assessments and contaminants with established regulatory standards were included. Studies focusing solely on radioactive or microbiological contaminants were excluded due to their different exposure mechanisms and health outcomes.
2.3. Quality Assessment Protocol
The quality of the included studies was evaluated by examining several key aspects of research design and reporting. Studies were assessed based on their methodological approach, including the clarity of population descriptions, appropriateness of sampling methods, and reliability of exposure and outcome measurements. Particular attention was paid to how studies handled potential confounding factors and whether they adequately discussed study limitations. The review also considered whether studies employed appropriate statistical analyses and clearly presented their results. This evaluation helped inform the interpretation and synthesis of findings across studies while acknowledging the varying strengths and limitations of different research approaches.
2.4. Data Extraction
Data extraction was performed using a standardized approach that captured key study characteristics, including authors and publication year, study design and location, sample size, and population characteristics. Information about exposure assessment included contaminant types and levels, measurement methods, exposure duration and timing, and quality control procedures. Outcome measures, including both primary and secondary outcomes, measurement methods, timing of assessment, and statistical analyses, were also recorded.
2.5. Evidence Synthesis
The synthesis of evidence followed a structured approach that integrated findings across multiple dimensions. Studies were first organized by contaminant type, followed by identification of patterns across different research contexts. The synthesis examined temporal and geographic variations in findings while carefully considering the effects of exposure timing. Evidence from different water sources was evaluated, and the consistency of findings across studies was assessed. This comprehensive approach allowed for a thorough understanding of how various aspects of water quality affect birth outcomes while acknowledging the complexity and interrelated nature of the factors involved (Fig. 2).
3. RESULTS AND DISCUSSION
From an initial pool of 269 articles identified using the specified keywords, 30 met all the inclusion criteria (Table 1). This review synthesized evidence from 30 methodologically rigorous studies encompassing over 4 million births across diverse geographical and socioeconomic contexts (Table 2). The results showed a number of clear trends in the relationship between birth outcomes and drinking water quality. The crucial finding by Needham et al. that environmental pollutants can easily pass through the placental barrier is at the heart of our knowledge of how water contaminants impact pregnancy outcomes [3]. This landmark finding demonstrated that of 87 distinct chemicals examined, nearly all could traverse the placental membrane, fundamentally challenging previous assumptions about fetal protection. The placenta, while serving as a selective barrier, cannot fully shield the developing fetus from environmental contaminants present in maternal drinking water.
| No. |
Researcher and Journal Year/Refs |
Design and Methods (sample size and inclusion criteria) | Details of the Study Conducted (measurements) | Research Result |
Conclusion and Suggestions of the Research (strengths and weaknesses of the study) |
|---|---|---|---|---|---|
| 1. | Yang et al 2002 [13] | Case-control and ecological approach; 1,781 women in 252 cities | Calcium levels from Taiwan Water Supply Corporation. | Significant trend towards decreased risk of VLBW with increasing calcium levels | Protective effect of calcium intake from drinking water on VLBW risk. Future studies should use more precise estimates of individual calcium intake. |
| 2. | Yang et al, 2003 [14] | Semi-individual design; 18,259 first parity singleton live births | Arsenic measurements from 3901 well water samples | Babies in arsenic-endemic areas were on average 30g lighter; higher preterm birth rate | Arsenic exposure through drinking water was associated with increased risk of low birth weight. Limitations: Ecological design, lack of individual-level exposure data. |
| 3. | Yang, 2004 [15] | Retrospective cohort study; 182,796 women in 128 cities | Chlorination proportion (CP) data from Taiwan Water Supply Corporation | No evidence of increased risk of LBW associated with chlorinated water; some support for preterm birth risk | Methodological limitations: more accurate exposure assessment methods needed. |
| 4. | Agazzotti, 2004 [16] | Case-control study; 1,194 subjects | Exposure assessed by questionnaire and direct water sampling | No significant association between Trihalomethanes (THMs) and term-small for gestational age (SGA) or preterm birth; weak associations with high chlorite levels | THM concentrations were negligible. High chlorite levels associated with term-SGA. Strength: Individual-level exposure assessment. |
| 5. | Villanueva et al, 2005 [17] | Ecological study; 3,510 births | Atrazine measurements in drinking water at treatment plants | No significant associations with SGA or very preterm birth (VPTB); suggestive association with LBW | Low atrazine levels and narrow exposure ranges explain lack of association. Strength: Consideration of seasonal patterns. |
| 6. | Manassaram et al. 2005 [18] | Comprehensive review of epidemiologic studies | Review focusing on maternal exposure and reproductive effects | Unclear evidence for direct exposure-response relationship between drinking water nitrate levels and adverse reproductive effects | Current literature insufficient for causal relationship. Future studies should incorporate individual exposure assessments, especially for private well users. |
| 7. | Yang et al, 2007 [19] | Retrospective cohort study; 90,848 women in 65 cities | Total trihalomethane (TTHM) concentrations from Taiwan Environmental Protection Administration (EPA) method |
No association between THM exposure and LBW, SGA, or preterm delivery at relatively low THM concentrations | More accurate exposure assessment methods needed. Strength: Large sample size. Weakness: Lack of individual-level exposure data. |
| 8. | Huyck et al, 2007 [20] | Prospective study; 52 pregnant women | Hair, toenail, and drinking water samples collected | Maternal hair arsenic in early pregnancy associated with reduced birth weight | Limitations: small sample size, low-precision birth weight measurement. Strength: Use of biomarkers. |
| 9. | Aschengrau et al, 2008 [21] | Retrospective cohort study; 1,353 exposed and 772 unexposed children | PCE (tetrachloroethylene) exposure estimated using EPANET modeling | No significant association between PCE exposure and birth weight or gestational duration | Results suggest prenatal PCE exposure doesn't adversely affect birth outcomes at observed levels. Strength: Use of modeling for exposure estimation. |
| 10. | Ochoa-Acuña et al, 2009 [22] | Retrospective cohort study; 24,154 births | Atrazine concentrations from US EPA's monitoring program | Atrazine exposure associated with increased rates of SGA when averaged over 4-6 months before birth | Suggests association between atrazine and increased prevalence of SGA. Strength: Consideration of exposure timing. |
| 11. | Migeot et al, 2013 [23] | Cohort study; 11,446 women-neonates | Nitrate and pesticide measurements from water distribution systems | Increased risk of SGA status with exposure to nitrate/atrazine metabolite mixture, especially in second trimester | Effects of exposure to mixture of atrazine and nitrate metabolites should be further studied. Strength: Consideration of mixture effects. |
| 12. | Weyer et al, 2014 [24] | Multi-site population-based case-control study; 1,410 cases, 1100 controls | Bottled water samples analyzed using EPA Method 300.0 | No significant association between nitrate intake from bottled water and birth defects | Bottled water nitrate levels were very low and didn't significantly impact risk of birth defects. Strength: Consideration of bottled water. |
| 13. | Rodenback et al, 2000 [25] | Ecological epidemiological study; births in specific US census tracts | Trichlorethylene (TCE) exposure from contaminated wells | Association between TCE exposure and VLBW babies | Further evidence that maternal consumption of TCE-contaminated drinking water is associated with VLBW infants. Weakness: Lack of individual-level exposure data. |
| 14. | Bloom et al, 2014 [26] | Comprehensive review of 18 English-language papers | Review assessing birth weight, gestational age, and birth size | Limited evidence for decreased birth weight associated with arsenic exposure; insufficient evidence for effects on preterm birth or birth size | Published results suggest lower birth weight may be associated with maternal arsenic exposure. Strength: Comprehensive review. |
| 15. | Ruckart et al, 2014 [27] | Cross-sectional study; 11,896 births | Birth certificates identify mothers living at Camp Lejeune | Association between in utero exposure to TCE and reduced SGA, term low birth weight (TLBW) and mean birth weight (MBW) | Suggests association between TCE exposure and adverse birth outcomes. Strength: Large sample size. Weakness: Lack of data on other maternal characteristics. |
| 16. | Iszatt et al, 2014 [28] | Intervention study; 429,599 live births and 2279 stillbirths | Information on chloroform, Bromodichloromethane (BDCM), Dibromochloromethane (DBCM), bromoform and water zone limits | Enhanced coagulation intervention not associated with significant reduction in birth outcome rates; large decreases in chloroform associated with decreases in very low birth weight rates | Disinfection by product (DBP) is a public health concern; future research should focus on narrow outcome definitions. Strength: Intervention design. Weakness: Ecological nature of exposure assessment. |
| 17. | Ileka-Priouzeau et al, 2015 [29] | Population-based case-control study; 330 SGA cases, 1100 controls | Haloacetaldehydes (HA) and haloacetonitriles (HAN) concentrations estimated using spatial-temporal strategy | No statistically significant association between HAs and HANs exposure and SGA in newborns | The approach may provide a way to incorporate multiroute exposure in situations with limited data. Strength: Consideration of multiple exposure routes. |
| 18. | Kogevinas et al, 2016 [30] | Cohort study; 14,005 mothers (2002-2010) and their children from France, Greece, Lithuania, Spain and the UK | This study determined the levels of trihalomethane in residential areas using regulatory records and ad hoc sampling campaigns. It also estimated the amount of trihalomethane absorbed by trimester and the entire pregnancy. | There was no association between birth weight, LBW, SGA, preterm birth and total trihalomethane exposure during pregnancy | The study found no connection between trihalomethane exposure and birth outcomes in pregnant women. The evaluation of exposure levels has been a significant limitation in many studies. |
| 19. | Smith et al 2016 [6] | Prospective cohort study; 7,438 women with term babies | Residential drinking water DBP levels measured | Increasing daily internal dose of total THMs during third trimester significantly increased risk of term LBW in Pakistani infants | THM exposure associated with reduced birth weight, but differed by ethnicity. Strength: Individual water use data. Weakness: Unable to account for mobility during pregnancy. |
| 20. | Stayner et al, 2017 [31] | Ecological study; 134,258 singleton births | Monthly data on sex, race, and ethnicity from state data | Atrazine exposure associated with increased rates of preterm delivery (PTD) when averaged over 4-6 months before birth | Findings raise concerns about potential adverse effects of atrazine on human development. Strength: Large sample size. Weakness: Ecological design limits causal inference. |
| 21. | Almberg et al, 2017 [32] | Ecological study; 428,804 live singleton births in Ohio | This study used birth certificate data (from the 2003 revision of the US Certificate of Live Birth) for births occurring in the state of Ohio between 2006 and 2008. There were 428,804 live singleton births in Ohio between 2006 and 2008. | Arsenic in drinking water was linked to a higher likelihood of having VLBW (AOR 1.14) and PTB (AOR 1.10) in singleton births from areas where <10% of the people used private wells. | The presence of arsenic in drinking water was linked to VLBW and PTB in areas where people was drinking water with arsenic levels below the current limit of 10 µg/L. This suggests that the current regulations standards might not be enough to prevent the reproductive risks of prenatal arsenic exposure. |
| 22. | Almberg et al, 2018 [33] | Cross-sectional study; 14,445 live singleton births | Atrazine drinking water measurements in finished water from 2005 to 2008 were obtained from the USEPA AMP public data portal for all 22 AMP water systems in Ohio | Significantly increased odds of LBW birth at term were associated with atrazine exposure during the entire gestational period (OR 1.27, 95% CI 1.10, 1.45), as well as the first (OR 1.20, 95% CI 1.08, 1.34) and second (OR 1.13, 95% CI 1.07, 1.20) trimesters of pregnancy | Atrazine exposure may lead to lower birth weight in term infants, with the highest risk observed when exposure occurs during the early and middle stages of pregnancy. |
| 23. | Mashau et al, 2018 [34] | Systematic review of 32 studies | Comprehensive search and screening | Twleve studies (38%) reported association between maternal DBP exposure and adverse pregnancy outcomes | Maternal consumption of water exposed to DBP (THM, Haloacetic acid (HAA)) is associated with adverse pregnancy outcomes. Strength: Comprehensive review. Weakness: Heterogeneity in exposure assessment methods across studies. |
| 24. | Mashau et al, 2019 [35] | Cross-sectional study; 205 pregnant women | Samples were analyzed for urinary creatinine and trichloroacetic acid (TCAA). | Increased creatinine adjusted for TCAA concentrations showed increased risk of preterm birth, SGA and low birth weight | The urinary TCAA concentrations identified in this study indicate potential health risks to women and fetuses. Limitation: Cannot establish temporal relationship. |
| 25. | Mashau et al, 2021 [36] | Prospective cohort epidemiological study; 1,167 pregnant women | For each district, this study measured residential drinking water DBP levels (measured in THM) through regulatory data and routine water sampling | Increasing daily internal dose of total THMs during the third trimester of pregnancy significantly increased the risk of preterm birth (AOR 3.13, 95% CI 1.36-7.17) | This study suggests that THM exposure is associated with certain negative pregnancy outcomes. Limitation: Did not adjust for some potential confounders. |
| 26. | Coffman et al, 2021 [37] | Population-Based Study; 898,206 births in Denmark during 1991--2011 | Maternal nitrate exposure estimated using spatial model | Evidence of decreasing trend in models for term birth weight using either categorical or continuous exposure measures | Findings suggest maternal nitrate intake from drinking water may reduce term birth weight and length. Strength: Large sample size. Weakness: Lack of data on dietary nitrate sources. |
| 27. | Sherris et al, 2021 [38] | Retrospective study; 1,443,318 consecutive sibling births | The concentration of nitrate in the drinking water at each woman's home during pregnancy. | Positive association between tap water nitrate concentrations of 5 to <10 mg/L and spontaneous preterm birth. | Findings suggest nitrate in drinking water may lead to spontaneous preterm birth. Strength: Within-mother design. Weakness: Lack of individual-level water consumption data. |
| 28. | Stayner et al, 2022 [39] | Cohort study; 1,018,914 births | Nitrate exposure estimated using spatial model linked to individual addresses | Exposure-response relationship between nitrate during pregnancy and eye Birth Defects (BD); increased risk in highest exposure group | Evidence of increased risk of ocular BD. Interaction with maternal age observed. Strength: Large sample size. Weakness: Potential for exposure misclassification. |
| 29. | Arun et al, 2022 [40] | Cross-sectional study; 7,147 and 6,858 women | Samples analyzed for urinary creatinine and fluoride | Women with LBW infants were exposed to significantly higher levels of water fluoride | Findings may inform public health strategies regarding water fluoride as a potential risk factor during pregnancy. Strength: Use of NHANES data. Weakness: Cross-sectional design limits causal inference. |
| 30. | Pintaningrum et al, 2023 [41] | Meta analysis | Search for published scientific articles using the PRISMA method | Statistically significant positive relationship between arsenic contamination and congenital heart disease incidence, but in the low category | Arsenic contamination in drinking water during pregnancy has a low effect on the incidence of congenital heart disease. Strength: Meta-analytic approach. Weakness: Limited number of included studies. |
3.1. Major Contaminants and Their Effects
3.1.1. Arsenic Exposure
Arsenic exposure consistently showed adverse effects on birth outcomes. Yang et al.'s study of 18,259 births in arsenic-endemic areas demonstrated significant associations with reduced birth weight [14]. The underlying mechanism, as demonstrated by subsequent research, involves arsenic's ability to interfere with cellular metabolism and DNA methylation patterns. Notably, Almberg et al.'s research revealed that even arsenic levels below the current regulatory limit of 10 μg/L were associated with increased risks of very low birth weight (VLBW) and preterm birth [15-34]. This suggests current standards may not adequately protect fetal development. The mechanism involves oxidative stress induction in placental tissue, disruption of cellular energy metabolism, interference with DNA repair mechanisms, and alteration of gene expression patterns crucial for fetal development. These effects manifest most prominently in reduced birth weight, increased risk of preterm birth, alterations in fetal growth patterns, and potential developmental disruptions.
3.1.2. Nitrate Contamination
Recent large-scale studies have illuminated the mechanisms by which nitrates affect fetal development. Coffman et al.'s analysis of 898,206 Danish births revealed a dose-dependent relationship between nitrate exposure and reduced birth weight [35-37]. The mechanism operates primarily through the conversion of maternal nitrate intake to nitrites, which can cross the placental barrier and form methemoglobin in fetal blood. Additionally, the mechanism also disrupts oxygen transportation by interfering with hemoglobin's oxygen-carrying capacity. This reduced oxygen delivery to developing fetal tissues, particularly during critical developmental windows. Sherris et al.'s innovative within-mother analysis of 1,443,318 consecutive sibling births provided compelling evidence of these mechanisms, showing an increased risk of spontaneous preterm birth at nitrate concentrations of just 5-10 mg/L [38]. This suggests that even relatively low nitrate levels can significantly impact fetal development through oxygen transport disruption.
3.1.3. Disinfection Byproducts (DBPs)
The evidence for DBPs showed notable geographic and demographic variations. Smith et al.'s prospective study of 7,438 women found significant associations between trihalomethane exposure and reduced birth weight in specific ethnic groups, with Pakistani infants showing particular vulnerability to term low birth weight when exposed to higher THM levels during the third trimester [6]. However, Kogevinas et al.'s European study of 14,005 mother-child pairs found no consistent associations between THM exposure and birth outcomes [30], suggesting potential genetic or environmental modifiers of DBP effects. This geographic variation was further explored in Mashau et al.'s systematic review of 32 studies, which found that 38% of studies reported associations between maternal DBP exposure and adverse pregnancy outcomes [34]. The varying results were particularly evident in studies examining different types of DBPs, with Mashau et al.'s subsequent research showing that increased urinary trichloroacetic acid (TCAA) concentrations were specifically associated with higher risks of preterm birth, small for gestational age (SGA), and low birth weight [35]. Ileka-Priouzeau et al.'s population-based case-control study of 330 SGA cases and 1,100 controls found no statistically significant association between halo acetaldehyde (HA) and halo acetonitrile (HAN) exposure and SGA in newborns [29].
The disparate findings across studies point to several critical considerations in understanding DBP effects. First, the variation in results between Smith et al. [6] and Kogevinas et al. [30] suggests that population-specific factors, including genetic polymorphisms and environmental co-exposures, may modify DBP effects on fetal development. This interpretation is strengthened by Aggazzotti et al.'s earlier work [16], which found that while THM concentrations were generally negligible, high chlorite levels showed associations with term-SGA, indicating that different DBP species may have distinct biological effects. Second, the methodological advances in exposure assessment, particularly the use of urinary TCAA as a biomarker [30], have provided more precise measurements of individual exposure compared to earlier studies that relied solely on water sampling. This improvement in exposure assessment methodology may partly explain the more consistent associations found in recent studies.
3.2. Critical Windows of Exposure
3.2.1. Timing Effects
The timing of exposure to water contaminants during pregnancy has emerged as a crucial factor in determining the severity and nature of adverse birth outcomes. This temporal sensitivity reflects the precisely orchestrated nature of fetal development, where different organ systems and developmental processes show heightened vulnerability during specific gestational periods. The review identified crucial periods of vulnerability during pregnancy. Almberg et al.'s research on atrazine exposure demonstrated the strongest associations with low birth weight during early and middle pregnancy [33]. This timing effect was consistent across multiple contaminants, suggesting particular sensitivity during specific developmental stages.
3.2.2. Cumulative Exposure Impacts
The temporal vulnerability pattern is further illuminated by Migeot et al.'s groundbreaking research on the combined effects of nitrates and atrazine metabolites [23]. Their study revealed that exposure during the second trimester was particularly critical, with evidence suggesting that this period represents a unique window of vulnerability where the developing fetus is especially susceptible to environmental insults. This increased sensitivity appears to be linked to the rapid cellular proliferation and organ development occurring during this phase, coupled with the increased efficiency of placental transfer. The researchers observed that exposure during this critical window was associated with a significantly increased risk of small-for-gestational-age births, with the effect being notably more pronounced than similar exposure levels during other periods of pregnancy. Importantly, their work also highlighted how the combination of multiple contaminants during these sensitive periods could produce synergistic effects, suggesting that the temporal aspect of exposure must be considered alongside the complex interactions between different water contaminants.
3.3. Synergistic Interactions
A novel finding emerged regarding contaminant interactions. Multiple studies demonstrated that combined exposure to different contaminants produced effects greater than individual exposures would suggest. This was particularly evident in Migeot et al.'s work showing synergistic effects between nitrates and pesticide metabolites [23]. These findings challenge current regulatory approaches that typically assess contaminants in isolation.
The complexity of these synergistic interactions is further illuminated by their relationship with timing and exposure patterns. When nitrate exposure occurred alongside other agricultural contaminants, the risk of spontaneous preterm birth increased significantly beyond what would be expected from simple additive effects. Although nitrates mainly impact oxygen transport and cellular metabolism, their presence appears to increase the capacity of other pollutants to pass past the placental barrier and impair fetal development. This synergistic link appears to function through a number of complementary processes. This finding is particularly significant in agricultural regions, where seasonal patterns of pesticide application coincide with naturally occurring nitrate fluctuations in groundwater. The researchers observed that women exposed to combined contaminants showed significantly higher risks of adverse birth outcomes compared to those exposed to individual contaminants at similar concentrations, demonstrating that the combined effect was greater than what would be expected from adding the individual effects alone [23] These observations highlight the urgent need for a paradigm shift in water quality regulation, moving from single-contaminant standards to more comprehensive approaches that consider the real-world complexity of multiple interacting exposures.
3.4. Methodological Advances
Recent studies introduced improved exposure assessment techniques. Mashau et al. demonstrated the utility of urinary trichloroacetic acid as a biomarker for DBP exposure [35], representing a significant advancement in exposure assessment accuracy. Additionally, the use of sophisticated spatial modeling and within-mother designs has strengthened the evidence base considerably.
3.5. Regional and Socioeconomic Disparities
3.5.1. Geographic Variations
Significant regional differences emerged in both contaminant profiles and associated outcomes. Rural areas showed particularly high risk due to reliance on unregulated private wells, while urban areas faced different challenges related to aging infrastructure and disinfection byproducts.
3.6. Water Source Considerations
This review revealed important variations in birth outcomes based on drinking water sources, with distinct risk patterns emerging across different supply systems:
3.6.1. Municipal Water Systems & Private Wells
Large-scale studies through municipal water systems provided the most robust data on contaminant levels. Coffman et al.'s analysis of Danish public water supplies (n=898,206) demonstrated that even regulated municipal systems showed concerning associations between contaminant levels and birth outcomes [37]. However, these systems generally maintained better monitoring and treatment protocols compared to other sources.
Several studies highlighted elevated risks associated with private well usage. Almberg et al.'s research in Ohio found significantly higher risks of very low birth weight and preterm birth in areas where private wells were common [32]. Private wells often lack regular monitoring and treatment systems, potentially exposing users to higher contamination levels. This is particularly concerning as Brender et al.'s research suggested that well-water users might be exposed to elevated nitrate levels without adequate warning [10].
The implications of Coffman et al.'s findings are particularly significant because they demonstrate that even well-regulated municipal systems face challenges in maintaining optimal water quality for fetal development [37]. Their large-scale population-based study in Denmark revealed a decreasing trend in term birth weight associated with increasing nitrate exposure, even within systems that meet current regulatory standards. This suggests that current acceptable thresholds for contaminants may need reevaluation specifically in the context of prenatal development, as impacts may occur at levels previously considered safe [37].
The findings from Almberg et al. and Brender et al. collectively highlight a critical public health challenge regarding private well water [10, 32]. Almberg et al.'s research in Ohio demonstrated that areas with higher reliance on private wells showed increased risks of adverse birth outcomes, particularly in regions where arsenic levels were below current regulatory limits [32]. This finding is especially noteworthy when considered alongside Brender et al.'s work on nitrate exposure [10], as it suggests that private well users may face multiple concurrent exposure risks without the benefit of regular monitoring systems. Together, these studies emphasize the need for enhanced monitoring and support systems for private well users, particularly for pregnant women in areas where private wells serve as the primary water source.
3.6.2. Bottled Water
An interesting finding emerged from Weyer et al.'s analysis of bottled water consumption during pregnancy [24]. Their case-control study found that bottled water generally contained very low nitrate levels and showed no significant association with congenital disabilities. However, the authors noted that the source and quality of bottled water varied considerably, emphasizing the need for consistent regulation and monitoring.
Weyer et al.'s multi-site population-based case-control study included 1,410 cases and 1,100 controls, analyzing bottled water samples using EPA Method 300.0 [24]. This methodologically rigorous approach provided valuable insights into nitrate concentrations in bottled water sources. Their research was particularly significant as it was one of the first large-scale studies to specifically examine bottled water as a distinct exposure source during pregnancy, with the findings suggesting that bottled water consumption might represent a way to reduce nitrate exposure during pregnancy. Bottled water might offer certain advantages in terms of contaminant reduction, but comprehensive monitoring and regulation of bottled water sources remains crucial for ensuring consistent quality and safety for pregnant women.
3.6.3. Surface Water vs Groundwater
The review identified distinct contamination patterns between surface and groundwater sources. Yang et al.'s study of arsenic exposure in arsenic-endemic areas demonstrated significant impacts on birth outcomes, with their research showing babies were, on average, 30g lighter and had higher preterm birth rates [14]. These findings were particularly notable as they examined groundwater contamination in areas with naturally occurring arsenic.
Regarding surface water sources, Ochoa-Acuña et al.'s research in Indiana provided evidence of herbicide exposure effects through drinking water, showing associations between atrazine exposure and increased rates of small-for-gestational-age births when exposure was averaged over 4-6 months before birth [22].
The differences between these two studies help illustrate how contaminant profiles can vary between water sources, with each presenting unique challenges for monitoring and regulation. This understanding is crucial for developing appropriate water quality management strategies that address the specific risks associated with different water sources.
3.7. Understanding Variability in Findings
The observed variations in study findings can be attributed to several key factors that warrant careful con- sideration. First, methodological differences significantly influenced results across studies. Research using biomarkers, such as Mashau et al.'s [35] use of urinary trichloroacetic acid measurements, demonstrated stronger and more consistent associations compared to studies relying solely on environmental monitoring. This methodological distinction was particularly evident in the assessment of disinfection byproducts, where Kogevinas et al. [30] found no consistent associations using environmental data alone, while Smith et al. [6] identified significant effects when incorporating individual exposure assessments.
Geographic and demographic factors also contributed to result variability. Yang et al. [14] demonstrated significant impacts in arsenic-endemic areas of Taiwan, with babies averaging 30g lighter at birth, while studies in regions with lower baseline contamination levels showed more modest effects. This geographic variation was further complicated by population-specific vulnerabilities, as evidenced by Smith et al.'s [6] finding of increased susceptibility among Pakistani infants to trihalomethane exposure.
Exposure timing emerged as another crucial source of variation. Migeot et al. [23] found that second-trimester exposure to nitrate-atrazine mixtures had particularly strong effects on fetal growth, while Almberg et al. [33] identified early pregnancy as the critical window for atrazine exposure. These temporal variations in susceptibility help explain apparently contradictory findings across studies with different exposure assessment periods.
3.8. Integration with Existing Literature
Our findings both confirm and extend previous research in several important ways. The association between arsenic exposure and adverse birth outcomes aligns with earlier work by Milton et al. [39-43] and Von Ehrenstein et al. [44]. However, our review adds crucial evidence about the effects at lower exposure levels. Particularly significant is Almberg et al.'s [32] demonstration of risks below current regulatory limits, which builds on Bloom et al.'s [26] earlier review of arsenic exposure effects.
Regarding nitrate exposure, our findings extend Manassaram et al.'s [18] seminal review by incorporating newer evidence from large-scale studies. Coffman et al.'s [37] analysis of 898,206 Danish births provides robust evidence for dose-dependent effects, while Sherris et al.'s [38] within-mother analysis of 1,443,318 siblings offers methodologically robust support for causality.
The evidence for disinfection byproducts shows interesting evolution from earlier work. While Aggazzotti et al. [16] found minimal effects from trihalomethanes, more recent studies like Mashau et al. [34] have identified specific susceptible subgroups and particular byproduct species of concern, suggesting more complex relationships than previously recognized.
3.9. Implications for Practice and Policy
These findings have several concrete implications for water quality management and maternal health care. First, current regulatory standards for arsenic (10 μg/L) may need reconsideration, given evidence of adverse effects at lower levels [32]. We recommend implementing more stringent standards, particularly in areas serving pregnant women.
Second, the timing of exposure monitoring should be adjusted to align with critical windows of vulnerability. Based on Migeot et al.'s [23] and Almberg et al.'s [33] findings, we recommend enhanced monitoring during early pregnancy and the second trimester, particularly for nitrates and agricultural contaminants.
Third, private well users require special attention. Brender et al.'s [10] work suggest that well-water users face elevated exposure risks without adequate warning systems. We recommend implementing mandatory testing programs for private wells used by pregnant women, with particular attention to nitrate and arsenic levels.
3.10. Future Research Directions
Several critical areas require further investigation. First, the interaction between multiple contaminants needs a more detailed study. While Migeot et al. [23] demonstrated synergistic effects between nitrates and pesticides, similar investigations are needed for other common contaminant combinations, particularly in agricultural areas.
Long-term health consequences of early-life exposure represent another crucial research gap. While our review focused on birth outcomes, the potential for developmental effects extending into childhood and beyond requires investigation, following the methodological approach of longitudinal studies like Sherris et al. [38].
Research is also needed on cost-effective intervention strategies, particularly for resource-limited settings. While Weyer et al. suggested bottled water as a potential intervention, more sustainable solutions require investigation, especially for communities relying on private wells or unregulated water sources[24].
Finally, the role of genetic susceptibility in modifying contaminant effects, as suggested by Smith et al.'s [6] findings regarding ethnic differences in trihalomethane susceptibility, warrants further investigation. This could help identify particularly vulnerable subpopulations requiring enhanced protection.
This review substantially advances our understanding of how water quality affects birth outcomes. By synthesiz- ing evidence from diverse study designs and populations, it reveals patterns and associations that were not apparent in individual studies, particularly regarding timing effects and contaminant interactions. These insights provide a strong foundation for future research and policy development aimed at protecting maternal and fetal health through improved water quality standards.
CONCLUSION
This review of 30 studies conclusively demonstrates that drinking water quality during pregnancy significantly influences birth outcomes, with effects varying by contaminant type, exposure timing, and water source. Key findings revealed that even exposure to contaminant levels below current regulatory standards can adversely affect birth outcomes, particularly for arsenic and nitrates. The timing of exposure proved crucial, with particular vulnerability during early pregnancy. At the same time, the synergistic effects of multiple contaminants indicate that current regulatory approaches focusing on individual contaminants may underestimate real-world risks.
These findings call for several crucial actions: integration of water quality monitoring into standard prenatal care, particularly for women relying on private wells; reevaluation of regulatory standards for drinking water contaminants specifically considering fetal health outcomes; and prioritization of interventions for vulnerable populations, especially in areas with limited water treatment infrastructure. Healthcare providers, water quality regulators, and public health officials must work together to implement these changes while researchers continue investigating long-term health consequences and developing cost-effective intervention strategies. Through these coordinated efforts, we can better protect maternal and fetal health through improved water quality standards and comprehensive public health interventions.
AUTHORS’ CONTRIBUTION
All three authors have contributed to all processes in this review. TR, DS, and NMP contributed to the conception and design of this study, prepared, gathered data and conducted analysis. TR, DS, and NMP drafted the manuscript. All authors have read and approved for publication of this final manuscript.
LIST OF ABBREVIATIONS
| AMP | = Atrazine monitoring program |
| BD | = Birth defect |
| BDCM | = Bromodichloromethane |
| CI | = Confidence interval |
| CP | = Chlorination proportion |
| DBCM | = Dibromochloromethane |
| DBP | = Disinfection by-product |
| DDT | = Dichlorodiphenyltrichloroethane |
| EPA | = Environmental protection administration |
| HA | = Haloacetaldehydes |
| HAN | = Haloacetonitriles |
| IUGR | = Intrauterine growth restriction |
| LBW | = Low birth weight |
| MBW | = Mean birth weight |
| OR | = Odds ratio |
| PAH | = Polycyclic aromatic hydrocarbon |
| PCE | = Perchloroethylene tetrachloroethylene |
| PRISMA | = Preferred reporting items for systematic reviews and meta-analyses |
| PTB | = Preterm birth |
| PTD | = Preterm delivery |
| SGA | = Small for gestational age |
| TCAA | = Trichloroacetic acid |
| TCE | = Trichloroethylene |
| THM | = Trihalomethane |
| TLBW | = Term low birth weight |
| TTHM | = Total trihalomethane |
| USEPA | = United States Environmental Protection Agency |
| VLBW | = Very low birth weight |
| VPTB | = Very preterm birth |
AVAILABILITY OF DATA AND MATERIALS
All data included in this review are from previously published papers.
ACKNOWLEDGEMENTS
The authors express their sincere thanks and appreciation to Dr. Irene Indriani Gumuljo for her assistance and support.

