All published articles of this journal are available on ScienceDirect.

The Utilization of Complementary and Alternative Medicine among Adults in Al Qassim Region, Saudi Arabia: A Cross-Sectional Study
Authors Info & Affiliations
Abstract
Introduction
Complementary and alternative medicine (CAM) is commonly used by healthy individuals for several reasons. This study estimated the prevalence, pattern, perceptions, and factors associated with CAM practices.
Methods
A cross-sectional survey was conducted using a self-administered questionnaire among the adult residents of the Al Qassim region, Saudi Arabia. Descriptive statistics and Multivariable logistic regression analysis were computed to determine the factors that predict CAM use.
Results
Out of 861 adults interviewed, 86.4% reported using CAM. The most common CAM modalities were Quran recitation (57%), prayer (53%), honey and bee products (53%), myrrh (50%), medicinal herbs mix (43%), and Zamzam water (42%). Age (40-59 years) was significantly associated with higher CAM use (p<0.05). However, the use of conventional medicines within the last 12 months and the monthly income of 5.000-10.000 SR were significantly associated with a decrease in the rate of CAM use. Females who are married, not currently employed, with monthly income (>10,000 SR) were reported to experience greater satisfaction with their CAM therapies (p<0.001).
Discussion
There is a high prevalence of CAM use in the Al Qassim region, with age identified as the most significant predictor of CAM utilization. Although males reported higher usage of CAM, females showed greater satisfaction with CAM therapies. The highest rate of spiritual CAM therapies was not surprising due to the strong religious beliefs and culture of the Saudi population.
Conclusion
More research is needed to understand the underlying mechanisms of CAM and to identify the most effective therapies for different health conditions, enabling more informed decision-making.
1. INTRODUCTION
Complementary and alternative medicine (CAM) could be defined as “a group of diverse medical and health care systems, practices, and products that are not presently considered to be part of conventional Western medicine” [1]. CAM has recently become more popular and accepted worldwide [2]. The use of CAM has increased markedly, both in developing and developed countries. It has been estimated that the prevalence of CAM or traditional medicine practice ranges from 31% in Belgium to 92% in Ethiopia [3].
The prevalence of CAM use in Saudi Arabia has not been population-based, where it ranged from very low (21.6%) to very high (93.5%), according to different regional studies [4-9]. In a recent study in the Riyadh region, 86% of the participants had used CAM at some point in their lives, mostly adults between 36–45 years [5]. Nevertheless, according to a study conducted in Qassim province, the prevalence of CAM usage was about 59.8% in the general population, predominantly among older females (average 44.5 years) with lower education levels [10].
The pattern of CAM use differs according to socioeconomic status, geography, and various religious and spiritual backgrounds [11]. The practices of CAM in Saudi Arabia are usually related to the religious beliefs of the consumers. Accordingly, the most popular CAM practices were honey, Zamzam water, Quran, and wet cupping, as it is a part of prophetic medicine [5, 7, 12-15]. Herbal and home therapies were also commonly used [8]. Modern practices were also introduced lately in the Saudi community through well-established clinics employing acupuncture, which is mostly practiced in the private sector with a prevalence between 1.6% and 42.8% [6, 7, 10, 16].
Most people all over the world use CAM for the management of medical conditions that are costly to society, such as diabetes mellitus, hypertension, asthma, chronic pain, heart diseases, arthritis, gastrointestinal disorders, and cancers [7, 17-19]. Recently, it has been reported that CAM use in Qassim province was significantly associated with the treatment and prevention of chronic diseases, such as diabetes mellitus (51.06%), hypertension (36.17%) [8], and chronic kidney diseases (35.3%) [20]. There are multiple reasons for CAM utilization. According to a worldwide systematic review of 51 populations, the top three reasons are the perceived possible beneficial effects (84%), the dissatisfaction with conventional medicine (37%), and the perceived safety of CAM (37%) [2].
Studies on the use of CAM in Al Qassim region are very limited [8, 10, 20, 21]. Also, these studies represent a sample of patients or outpatients and cannot be representative of the general population. Besides, none of the above studies were able to look at predicting factors associated with CAM use. Accordingly, the aim of this study was to investigate the prevalence, pattern, and predicted factors associated with the use of complementary and alternative medicine (CAM) in the community.
2. MATERIALS AND METHODS
2.1. Study Design, Location and Duration
A descriptive, quantitative, and cross-sectional study was conducted in the Al Qassim region of Saudi Arabia. The data collection was performed over a period of 3 months, from 10th November 2022 to 16th February 2023.
2.2. Study Tool
To collect data, we used a well-structured self-administered questionnaire in the English language adopted from previous studies about CAM use among the Saudi population [5, 10, 22] after getting official permission from the authors. It consists of 28 items subdivided into four sections. The first section captured the demographics (age, sex, marital status, educational level, occupation, monthly income, and use of conventional medicine). The second section revolves around the details of CAM use, such as the types, frequency, and sources of information. The third section addresses CAM-related practices, including reasons for use, medical conditions treated, and reported side effects. The fourth section focuses on perceptions of and satisfaction with CAM use. Since Arabic is the official language among the general population of Saudi Arabia, the questionnaire was translated into Arabic language using a forward-backward translation technique [23]. The forward translation was done by three native Arabic speakers. The translated draft was revised by five academicians in the pharmacy practice specialty, social workers, and a few adults from the general population. This step was followed by backward translation, which involved translating the Arabic version of the questionnaire back into English by a bilingual academician who was not aware of the original questionnaire. Finally, the backward-translated version was carefully compared with the original English version to establish content validity.
2.3. Sample Size and Data Collection
According to the population characteristics survey in 2017, the study targeted the total adult population of 1,215,858 in the Qassim region (General Authority for Statistics, 2017). The Cochran equation [24: Eq.1] was applied to estimate the target sample size for the representation of this study population, which was 363.
 |
(1) |
Where:
N is the sample size,
Z is the standard error associated with the selected level of confidence,
P is the anticipated prevalence of CAM, and d is the error of estimation (precision).
The level of confidence used in this study is 95%.
The Zα value associated with 95% of confidence is 1.96.
The anticipated prevalence of CAM (P) is 67%.
The error of estimation is 5%.
Since the population of the Qassim region is more than one million, we added 7% (approximately 24 persons) to the calculated sample size to account for incomplete responses. Therefore, the sample size for this study should be no less than 363 persons.
2.4. Data Analysis
All statistical analyses were conducted using Microsoft Excel and R software. First, the data was entered into an Excel sheet, coded, and then exported to R software for descriptive and comparative analyses. Categorical data were presented as a frequency and percentage. Chi-square or Fisher's exact test, as appropriate, was applied for comparative analysis. Logistic regression was used to identify the predicted factors that may affect CAM use. The odds ratio and 95% confidence interval are used to quantify the association between predicted factors and CAM use in the Al Qassim population. p<0.05 was considered statistically significant.
2.5. Ethical Approval
This research was conducted on humans according to the guidelines of the Declaration of Helsinki after obtaining the Ethics Committee’s permission (2018-11-29) from the Qassim Bioethics Research Committee. Patients’ completion of the questionnaire implied their consent to participate in the study.
2.6. Study Participants and Eligibility Criteria
This study targeted all mentally stable adults in the Al Qassim region who are able to read and write and provide verbal consent to participate. Residents from outside the Al Qassim region, those under the age of 18, and those with intellectual disability and cognitive impairment were excluded from this study.
3. RESULTS
The demographic characteristics of the subjects are shown in Table 1. Out of 861 samples, 526 (61%) participants were males, and the majority of respondents were Saudi citizens 786 (91.3%). The highest number of participants was aged between 18 and 29 years (30.3%). The majority of participants were married 546 (63.4%). Regarding educational level, most of the participants, 537 (62.4%) had university degrees. The family's monthly income was evenly distributed. Some had an income of less than 5,000 SR (37%), and others had an income of more than 10,000 SR (37.4%). Regarding health status, the majority of participants, 571 (66%) reported the use of conventional medicine within the past 12 months.
| Variables | N (%) |
|---|---|
| Gender | |
| Females | 335 (39.0%) |
| Males | 526 (61.0%) |
| Age (years) | |
| 18-29 | 261 (30.3%) |
| 30-39 | 185 (21.5%) |
| 40-49 | 195 (22.7%) |
| 50-59 | 157 (18.2%) |
| ≥60 | 63 (7.3%) |
| Marital status | |
| Single | 258 (30.0%) |
| Married | 546 (63.4%) |
| Divorced/Widow/Widower | 57 (6.6%) |
| Nationality | |
| Saudi | 786 (91.3%) |
| Non-Saudi | 75 (8.7%) |
| Education | |
| Postgraduate degree | 89 (10.3%) |
| University degree | 537 (62.4%) |
| Diploma | 86 (10.0%) |
| Secondary /preparatory | 121 (14.1%) |
| Primary/ illiterate | 28 (3.3%) |
| Occupation | |
| Unemployed /Retired/ Housewife | 371 (43.1%) |
| Non-Healthcare professional | 384 (44.6%) |
| Healthcare professional | 106 (12.3%) |
| Monthly income in SAR | |
| <5.000 | 319 (37.0%) |
| 5.000- 10.000 | 220 (25.6%) |
| >10.000 | 322 (37.4%) |
| Use of conventional medicine in the last 12 months? | |
| Yes | 571 (66.0%) |
| No | 290 (34.0%) |
A total of 744 (86.4%) participants had used CAM over the preceding 12 months (Table 2). There was a significant difference in CAM use between males (59%) and women (41%) (p=0.003). The participants aged more than 60 years tended to use CAM less frequently than their younger counterparts (p<0.0001). CAM was more frequently used among the married participants (66%) compared to single (27%) and widowed/divorced (7%) participants, and among high-income (>10,000 SR) participants (41%) compared to intermediate (24%) and low income (35%) (p<0.0001).
| Characteristic |
CAM users, N = 7441 N (%) |
Non-CAM users, N = 891 N (%) |
p-value2 |
|---|---|---|---|
| Gender | 0.003* | ||
| Females | 304 (41.0%) | 22 (25.0%) | |
| Males | 440 (59.0%) | 67 (75.0%) | |
| Age (years) | <0.001* | ||
| 18-29 | 201 (27.0%) | 50 (56.0%) | |
| 30-39 | 160 (22.0%) | 16 (18.0%) | |
| 40-49 | 179 (24.0%) | 12 (13.0%) | |
| 50-59 | 146 (20.0%) | 8 (9.0%) | |
| ≥60 | 58 (7.8%) | 3 (3.4%) | |
| Marital status | <0.001* | ||
| Single | 202 (27.0%) | 46 (52.0%) | |
| Married | 490 (66.0%) | 38 (43.0%) | |
| Divorced/Widow/Widower | 52 (7.0%) | 5 (5.6%) | |
| Nationality | 0.8 | ||
| Saudi | 681 (92.0%) | 82 (92.1%) | |
| Non-Saudi | 63 (8.0%) | 7 (7.9%) | |
| Education | 0.5 | ||
| Postgraduate degree | 80 (94.1%) | 5 (5.9%) | |
| University degree | 462 (89.0%) | 57 (11.0%) | |
| Diploma | 75 (88.2%) | 10 (11.8%) | |
| Secondary /preparatory | 102 (87.9%) | 14 (12.1%) | |
| Primary/ illiterate | 25 (89.3%) | 3 (11.7%) | |
| Occupation | 0.076 | ||
| Unemployed/Retired/Housewife | 90 (12.0%) | 15 (17.0%) | |
| Non-Healthcare professional | 342 (46.0%) | 30 (34.0%) | |
| Healthcare professional | 312 (42.0%) | 44 (49.0%) | |
| Monthly income in riyal | <0.001* | ||
| <5000 | 262 (35.0%) | 41 (46.0%) | |
| 5000- 10000 | 180 (24.0%) | 34 (38.0%) | |
| >10000 | 302 (41.0%) | 14 (16.0%) |
| Characteristic | OR1 | 95% CI1 | p-value |
|---|---|---|---|
| Gender (Ref=Male) | |||
| Female | 0.58 | 0.33, 1.01 | 0.061 |
| Age (years) (Ref =18-29) | |||
| 30-39 | 2.21 | 1.00, 4.99 | 0.052 |
| 40-49 | 2.67 | 1.05, 6.95 | 0.041* |
| 50-59 | 3.54 | 1.28, 10.4 | 0.017* |
| ≥60 | 4.02 | 0.98, 23.7 | 0.079 |
| Marital status (Ref=single) | |||
| Married | 1.18 | 0.57, 2.47 | 0.7 |
| Divorced/Widow/Widower | 1.01 | 0.32, 3.64 | >0.9 |
| Occupation (Ref= Health care professional) | |||
| Non-Health care professional | 1.34 | 0.63, 2.73 | 0.4 |
| Unemployed, housewife, and retired | 1.32 | 0.61, 2.76 | 0.5 |
| Education (Ref = Postgraduate degree) | |||
| Diploma | 0.72 | 0.41, 1.28 | 0.3 |
| Illiterate | 0.65 | 0.08, 14.2 | 0.7 |
| Monthly Income (Ref=<5000) | |||
| 5000- 10000 | 0.42 | 0.22, 0.82 | 0.011* |
| >10000 | 1.17 | 0.48, 2.91 | 0.7 |
| Do you use any conventional medicine in the last 12 months (Ref =NO) | 0.55 | 0.34, 0.88 | 0.014* |
Table 3 shows the multivariable logistic regression model of the factors predicting the use of CAM by Saudis in the Al Qassim region. The following factors were statistically significantly associated with the use of CAM: age categories of 40-49 and 50-59, income ranging from 5000-10000, and use of conventional medicines within the last 12 months. Indeed, the participants aged 40-49 years and 50-59 years were 2.67 and 3.5 times more likely to use CAM therapies compared to younger participants aged 18-29 years (OR = 2.67, 95% CI = 1.05-6.95, p=0.041) and (OR=3.54, 95% CI=1.28-10.4, p=0.017), respectively. Nevertheless, the participants with incomes ranging from 5,000 to 10.000 SR were less likely to use CAM products compared to those with incomes less than 5,000 SR (OR=0.42, 95% CI=0.22-0.82, p=0.01, although incomes greater than 10,000 SR did not affect the odds of CAM use (OR = 1.17, p = 0.7). Furthermore, the use of conventional medicines within the last 12 months was significantly associated with a decrease in the rate of CAM use (OR = 0.55, 95% CI = 0.34-0.88, p = 0.014). Gender, educational level, occupation, and marital status did not have a significant effect on the use of CAM therapies.
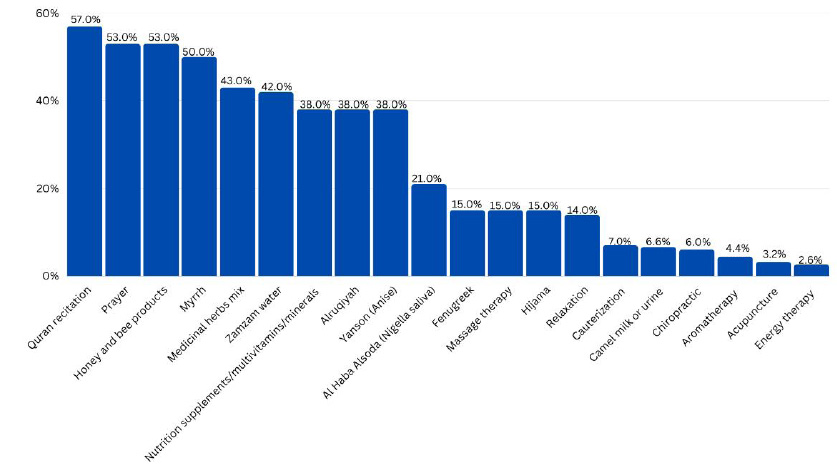
Twenty different kinds of CAM were used by the participants in this study (Fig. 1). The most common CAM types were Quran recitation (57%), Honey and bee products (53%), Prayer (53%), Myrrh (50%), Medicinal Herbs mix (43%), and Zamzam water (42%). In contrast, the use of acupuncture (3.2%) and energy therapy (2.6%) was very uncommon. These groups were not mutually exclusive because subjects may have used more than one CAM type.
Recommendations by relatives and/or friends were the most common reasons given by the study participants (35%) for using CAM, followed by the perceived safety and effectiveness of CAM (24.3%) and the absence of side effects for CAM therapies (17.9%) as shown in Table 4.
| Characteristics | N (%) |
|---|---|
| What is the main reason for using CAM? | |
| High cost of conventional medicine | 27 (3.6%) |
| CAM is inexpensive and available | 84 (11.3%) |
| CAM is safe and effective | 181 (24.3%) |
| They have no side effects | 111 (14.9%) |
| Specialized CAM centers and clinics / provided CAM services | 17 (2.3%) |
| Fear of using chemical treatments | 58 (7.8%) |
| Recommended by relatives/friends | 266 (35.8%) |
Types of CAM therapies used by the CAM users.
The common medical conditions for using CAM among saudi adults (N=744).
| Characteristic | N=744 (%) |
|---|---|
| Do you use CAM alone or with prescribed drugs or OTC drugs (over the counter)? | |
| Alone | 556 (74.7%) |
| With prescribed drugs | 188 (25.3%) |
| Did you experience an improvement in your health situation while using CAM? | |
| Yes | 646 (86.8%) |
| No | 18 (2.4%) |
| I don't know/Not sure | 80 (10.8%) |
| Did you experience a worsening of your health situation while using CAM? | |
| Yes | 33 (8.6%) |
| No | 647 (87.0%) |
| I don't know/Not sure | 64 (8.6%) |
| Did you experience any adverse effects while using CAM? | |
| Yes | 55 (7.4%) |
| No | 596 (80.1%) |
| I don't know/Not sure | 93 (12.5%) |
| If yes, please specify (Please tick more than one option, if desired). | |
| Constipation | 11 (20.0%) |
| Diarrhea | 2 (3.6%) |
| Nausea | 10 (18.1%) |
| Vomiting | 5 (9.0%) |
| Flatulence | 10 (18.1%) |
| Heartburn | 6 (10.9%) |
| Allergy | 7 (12.7%) |
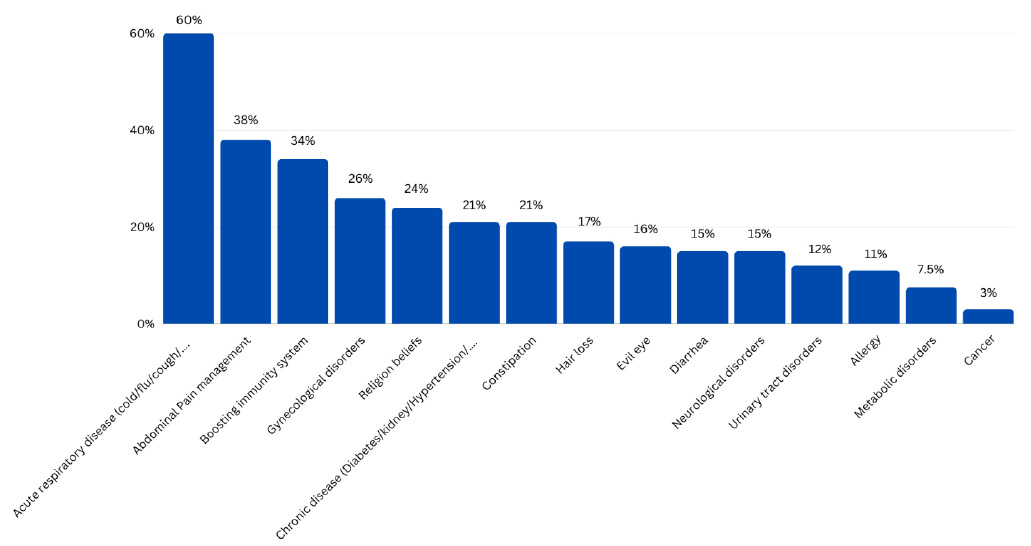
The most common medical conditions reported among CAM users were acute respiratory disorders such as cold, flu, and cough (60%), followed by abdominal pain (38%), boosting the immune system (34%), and gynecological disorders (26%). On the other hand, the least common reason to seek CAM was cancer (3%) (Fig. 2).
It is worth noting that 556 (74.7%) CAM users had used CAM therapies exclusively, without extra prescribed drugs or over-the-counter medications. The majority of the CAM users, 646 (86.8%) reported a clinical improvement, while only 33 (8.6%) reported a worsening in their health. Only 55 out of 744 CAM users (7.4%) reported some adverse effects while using CAM, in which constipation (20%), nausea (18.1%), and flatulence (18.1%) were the most common. The details about CAM-related practices are shown in Table 5.
Out of the 861 study participants 713 (82.8%) and 496 (57.6%) agreed that CAM products are effective and can treat certain health conditions that cannot be treated with conventional medicine, respectively. Moreover, 668 (77.6%) of the respondents stated that they would recommend CAM products to others. Lastly, out of the 744 CAM users, 516 (69.3%) were very satisfied with their CAM use. The respondents' answers to CAM-perception and satisfaction-related questions are shown in Table 6.
| Characteristic | N (%) |
|---|---|
| Do you think CAM is effective? (N=861) | |
| Agree | 713 (82.8%) |
| Neutral | 132 (15.3%) |
| Disagree | 16 (1.9%) |
| Do you think that CAM can treat a health condition that cannot be treated with conventional medicine? (N=861) | |
| Agree | 496 (57.6%) |
| Neutral | 222 (25.8%) |
| Disagree | 143 (16.6%) |
| Would you recommend CAM to someone? (N=861) | |
| Agree | 668 (77.6%) |
| Neutral | 161 (18.7%) |
| Disagree | 32 (3.7%) |
| If you CAM user, are you satisfied? (N=744) | |
| Very | 516 (69.3%) |
| Somewhat | 223 (30.0%) |
| Not at all | 5 (0.7%) |
| Characteristic |
Very satisfied N= 516 |
Somewhat satisfied N= 223 |
Not at all satisfied N=5 |
p-value2 |
|---|---|---|---|---|
| Gender | <0.001* | |||
| Females | 277 (54%) | 161 (72%) | 2 (40%) | |
| Males | 239 (46%) | 62 (28%) | 3 (60%) | |
| Age (years) | <0.001* | |||
| 18-29 | 115 (22%) | 82 (37%) | 4 (80%) | |
| 30-39 | 105 (20%) | 54 (24%) | 1 (20%) | |
| 40-49 | 131 (25%) | 48 (22%) | 0 (0%) | |
| 50-59 | 115 (22%) | 31 (14%) | 0 (0%) | |
| ≥60 | 50 (9.7%) | 8 (3.6%) | 0 (0%) | |
| Marital status | <0.001* | |||
| Single | 116 (22%) | 81 (36%) | 5 (100%) | |
| Married | 364 (71%) | 126 (57%) | 0 (0%) | |
| Divorced/Widow/Widower | 36 (7.0%) | 16 (7.2%) | 0 (0%) | |
| Nationality | 0.7 | |||
| Saudi | 474 (92%) | 202 (91%) | 5 (100%) | |
| Non-Saudi | 42 (8.1%) | 21 (9.4%) | 0 (0%) | |
| Education | 0.5 | |||
| Postgraduate degree | 56 (11%) | 24 (11%) | 0 (0%) | |
| University degree | 315 (61%) | 143 (64%) | 4 (80%) | |
| Diploma | 47 (9.1%) | 27 (12%) | 1 (20%) | |
| Secondary /preparatory | 76 (15%) | 26 (12%) | 0 (0%) | |
| Primary/ illiterate | 22 (4.3%) | 3 (1.3%) | 0 (0%) | |
| Occupation | 0.04* | |||
| Unemployed/Retired/Housewife | 371 (72%) | 167 (75%) | 4 (80%) | |
| Non-Healthcare professional | 129 (25%) | 56 (25%) | 1 (20%) | |
| Healthcare professional | 16 (3.1%) | 0 (0%) | 0 (0%) | |
| Monthly income in riyal | <0.001* | |||
| <5000 | 158(31%) | 99 (44%) | 5 (100%) | |
| 5000- 10000 | 116 (22%) | 64 (29%) | 0 (0%) | |
| >10000 | 242 (47%) | 60 (27%) | 0 (0%) |
Our results indicate that more than half of the study participants (69.3%) were satisfied with the CAM practices they received. Also, we found a significant association between satisfaction towards CAM use and gender (p<0.001), age (p<0.001), marital status (p<0.001), occupation (p=0.04), and monthly income (p<0.001) (Table 7).
Specifically, we found that a majority of participants who were very satisfied with their CAM use were females (54%), less than 60 years old (80.3%), married (71%), either unemployed, retired, or a housewife (73%), and living with high monthly income (>10,000 SR) (47%).
4. DISCUSSION
In this study, results over an 8-month period showed that 86.4% of adults in the Al Qassim region, central Saudi Arabia, used one or more types of CAM. The prevalence of CAM use varies between studies and countries. The prevalence of CAM use in the current study was relatively high compared to other studies conducted in Saudi Arabia and around the world. Recently, Aljawadi and Coll. reported that 62.5% of the general population in Saudi Arabia had used CAM [25]. Other studies conducted in the Majmaah and Makkah regions in Saudi Arabia reported that 66.3% and 51.6% of Saudis had used CAM, respectively [7, 26]. In neighboring countries, the prevalence of CAM was about 70% and 88.3% in Jordan [27] and Palestine [28] populations, respectively. Such differences in the prevalence were expected because of the broad spectrum of the samples’ demographic, religious, and socioeconomic data, and the locality of herbs.
In the current study, gender was significantly associated with CAM use (p=0.003). Males reported the greatest rates of CAM use (59%). This finding was similar to the reports of a study carried out in Riyadh region, Saudi Arabia [29]. In addition, we found a significant association between CAM use and age, marital status, and monthly income (p<0.001). Similar to our findings, a previous study in the Al Qassim region [8] reported a significant association between CAM use and gender (p = 0.029) and marital status (p = 0.034). The higher income was associated with more prevalent CAM use in various studies among European [30], England [31], and Lebanon [32] populations.
Similar to our data, the predicted factors for CAM use were the age ranged between 45-54 and 55-64 years (p=<0.001) in England's population [31] and the ages between 45-49 and 55-59 years (p=<0.001) in Malaysian population [18]. Furthermore, our data showed a decline in the rate of CAM use among individuals with a monthly income of 5,000-10,000 SR (p = 0.014) and those who had used medical treatment in the last 12 months (p = 0.011), findings that have not been previously investigated.
The most commonly used CAM therapies in our study were spiritual, such as Quran recitation (57%), prayer (53%), and Zamzam water (42%), followed by honey products (53%), Myrrh (50%), and Medicinal herbs mix (43%). These results are similar to Khan's study among the Saudi residents in the center of Saudi Arabia, in which the highest reported form of CAM used was prayers/spirituality (83.6%) [13]. In addition, recently, a study carried out in Dammam and Al Khobar (Eastern of Saudi Arabia) showed that the majority of CAM users favor honey (24.6%) and Quran (20.5%) [22].
The highest rate of spiritual CAM therapies was not surprising due to the strong religious beliefs and culture of the Saudi population. These were recommended by the Prophet Mohammed, peace be upon him, and that is why people trust these methods of healing. Myrrh and traditional herbal medicine have long been commonly used in the Saudi population for their anti-inflammatory and antimicrobial properties to treat various acute and chronic diseases [8, 20, 33].
The main incentive reported in this study, for the use of complementary medicine as a form of healing was recommendation by family and friends (35.8%). This result is similar to a previously published study among the Saudi population, in which 56.1% of participants have used CAM based on relative's and friends' recommendations [22]. This is generally perceived as a common means in the Saudi population by which people are influenced to try new things. The second most common reason was the perceived safety and effectiveness of CAM practices (24.3%). Similarly, previous studies conducted in the Emirate [34], West Africa [35], and the USA [36] found that the reason for using CAM was its effectiveness and safety compared to conventional treatments, which are associated with troublesome side effects.
According to our data, the most common conditions for CAM use were acute respiratory diseases such as cold, flu, and cough (60%), followed by abdominal pain management (38%). This is in line with a study conducted in Riyadh in which abdominal pain (48.9%) and the common cold (48.9%) were the most common diseases for CAM use [37]. Also, another study conducted in Al-Khobar among adolescents showed that CAM was commonly used to treat health symptoms such as abdominal pain, cold, flu, and cough [38]. Also, recently, Alfadeel and Coll. reported the use of CAM for treating the common cold (66.50%) among the adult population [5].
Also, a notable percentage of participants (34%) in the current study had used CAM therapies to boost the immune system. This is likely due to the heightened awareness of the importance of maintaining a strong immune system to prevent illness, particularly after the COVID-19 pandemic. This finding is similar to a study conducted in Riyadh in which 66% of respondents agreed that using herbal medicines strengthens immunity [29]. This suggests that there is a high level of belief in the efficacy of CAM therapies among the Saudi population.
Furthermore, the use of CAM has been associated with positive health outcomes among the participants, with 86.8% of them experiencing an improvement in their health condition after using CAM, and 82.8% agree that CAM is effective. Additionally, more than half of the study participants (57.6%) believe that CAM can treat health conditions that cannot be treated with conventional medicine. Similarly, it has been reported in a recent Iranian study that the most common reasons for adopting CAM among the general population are the perceived utility of CAM approaches and the perceived effectiveness compared to conventional therapies [39]. Additionally, a study conducted in the Riyadh region found that 71.7% of outpatients supported the idea that CAM helps conventional medicine and did not consider it a myth [37]. This indicates that there is a growing acceptance of CAM therapies as a complementary approach to conventional medicine.
Our results indicate that more than half of the study participants (69.3%) were satisfied with the CAM practices they received. Also, we found that the female participants (54%), those who are less than 60 years old (80.3%), married (71%), either unemployed, retired or a housewife (73%), and living with a high monthly income (>10,000 SR) (47%) were very satisfied with their CAM practices. This means that individuals who are in stable relationships, not currently employed, and living comfortably may be more likely to experience greater satisfaction with their use of CAM therapies.
Many factors have been investigated in the research of CAM. To the best of our knowledge, this study is one of the pioneer studies investigating the predicted factors that may affect CAM use in the general population with an appropriate sample size and a validated questionnaire. This study demonstrated the association between CAM use and different sociodemographic data. Also, the multivariable logistic regression, for predicting factors for CAM use showed a significant association for some demographic data, such as the age ranges between 40-49 and 50-59, the medium monthly income (5000-10000), and the use of conventional medicines. Furthermore, the participants in this study were drawn from the general population, suggesting that our findings are likely to be representative of a broader population rather than a specific subgroup.
However, this study has a few limitations that should be considered. Firstly, the findings are based on data collected from populations in only one province of Saudi Arabia. This geographical restriction limits the generalizability of the results to the entire kingdom, as other provinces may have differing cultural, social, and economic factors influencing the use of complementary and alternative medicine (CAM). Secondly, the study excluded certain groups, including individuals who are illiterate, those unable to provide verbal consent, and elderly patients with cognitive impairments. These exclusions may have introduced selection bias and potentially omitted key demographic groups that could have provided different perspectives on CAM usage. Despite these limitations, the study offers valuable insights into the prevalence and patterns of CAM use within the sampled population.
CONCLUSIONS
The use of CAM was highly prevalent among the participants of this study, 86.4% of whom had used CAM in the past 12 months. This widespread use of the various types of CAM reflects religious and cultural preferences, with many participants using spiritual, honey/bee products, and medicinal herbal therapies, suggesting strong preferences for natural and traditional remedies. Recommendations by relatives and friends were reported as the most common reason for using CAM in this sample, highlighting the role of social influences and cultural traditions in healthcare decision-making. CAM therapies are being used to treat a diverse range of conditions, ranging from non-serious minor health ailments such as respiratory diseases and abdominal pain to more generalized health improvement, including boosting the immune system and overall well-being. This suggests that CAM was not only sought for disease management but for preventive care and overall health maintenance. Demographic analysis revealed that, the participants aged between 40-59 years were more likely to use CAM than other participants. Finally, the participants who are in stable relationships, not currently employed, and living comfortably on their monthly income are likely to be more satisfied with CAM therapies than the other participants.
AUTHORS’ CONTRIBUTIONS
It is hereby acknowledged that all authors have accepted responsibility for the manuscript's content and consented to its submission. They have meticulously reviewed all results and unanimously approved the final version of the manuscript.
ABBREVIATION
| CAM | = Complementary and alternative medicine |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The ethical approval was obtained from the Committee of Research Ethics at Qassim Bioethics Research Committee (2018-11-29) , Saudi Arabia (reference number 9442/44/607).
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committees and with the 1975 Declaration of Helsinki, as revised in 2013.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article is available open request from the corresponding author [M.F] of this manuscript.
ACKNOWLEDGEMENTS
The researchers would like to thank the Deanship of Graduate Studies and Scientific Research at Qassim University for financial support (QU-APC-(2025). The authors would also like to express their gratitude to all participants in the study.

