All published articles of this journal are available on ScienceDirect.

Impact of Kangaroo Care on Premature Infants’ Vital Signs: A Retrospective Cohort Study
Authors Info & Affiliations
Abstract
Introduction
The Kangaroo Mother Care (KMC) approach is the most effective method for ensuring that a newborn's skin maintains direct contact with the mother's skin. This practice is particularly beneficial for all newborns, especially those who are premature or have low birth weight. The current study aims to evaluate the effects of the Kangaroo Mother Care (KMC) method on the vital signs and arterial oxygen saturation of newborns compared to a control group not receiving KMC.
Methods
This study was conducted as a retrospective cohort study on 188 premature infants (defined as those with a gestational age of less than 37 weeks) admitted to the hospital. The vital signs, which include temperature, respiratory rate, heart rate per minute, and arterial oxygen saturation, were assessed and documented prior to, during, and following the care process in both groups. These measurements were subsequently compared and analyzed.
Results
The results of repeated measures variance analysis showed that the mean body temperature in the KMC group was statistically different from that of the control group, increasing from 35.68 on the first day to 36.68 on the 14th day (p < 0.05). The mean systolic and diastolic blood pressures exhibited statistically significant differences across all assessment stages over the 14-day period, with the KMC group demonstrating lower levels (p < 0.05). The means of the heart rate and respiratory rate of the newborns on each of the 14 days evaluated in the two groups did not show a statistically significant difference (p >0.05).
Discussion
It has been established that Kangaroo Mother Care (KMC) has a significant impact on physiological parameters such as body temperature and blood pressure. The findings of our study were consistent with the results of other studies.
Conclusion
We concluded that Kangaroo Mother Care (KMC), which entails skin-to-skin contact between an infant and caregiver, has been shown to significantly influence physiological parameters, including body temperature and blood pressure. On the other hand, no significant differences were found in the mean heart rate and respiratory rate. Additional research with enhanced methodological rigor is required to validate these findings. It was concluded that by promoting direct contact, KMC helps with thermoregulation, allowing neonates to maintain a stable body temperature through the warmth of the caregiver's skin, which is vital in preventing hypothermia.
1. INTRODUCTION
In the neonatal intensive care unit (NICU), premature infants face various stressors, including invasive medical procedures, bright lighting, and the noise generated by medical devices [1]. These essential interventions can trigger both physiological and behavioral responses in these vulnerable infants. Furthermore, the separation from their mothers, along with the NICU environment, restricts visual, tactile, and auditory interactions, which can hinder maternal bonding [2, 3]. The World Health Organization characterizes Kangaroo Mother Care (KMC) as the practice of early, continuous, and extended skin-to-skin contact between mother and infant, which may also involve fathers as caregivers, along with frequent and exclusive breastfeeding [3]. KMC was initially developed in Bogotá, Colombia, in 1978 to address the issue of incubator shortages in hospitals caring for premature babies [4].
This approach is founded on three fundamental principles: skin-to-skin contact, exclusive breastfeeding, and safeguarding the mother-infant relationship. Facilitating skin-to-skin contact between an infant and the mother is a critical practice that fosters attachment, supports breastfeeding success, and promotes physiological stability in newborns. In this process, the infant is positioned directly against the mother's chest, ensuring optimal warmth and sensory interaction. This positioning not only helps regulate the baby's heart rate and temperature but also stimulates breastfeeding instincts, as the infant can use innate reflexes to seek and latch onto the breast when ready. This practice can commence at birth or at any time throughout the day or night, with even brief and intermittent sessions proving beneficial [5]. Intermittent kangaroo care is typically administered for short durations, occurring once or multiple times daily. This method offers tactile stimulation through the mother's initial skin contact with the infant, visual engagement from direct contact, olfactory cues from breastfeeding, and motor stimulation from sucking at the nipple. When an infant is placed directly against a caregiver’s bare chest, there is significant regulation of body temperature, heart rate, and respiratory rate due to the warm environment provided by the caregiver’s body heat. Additionally, this close contact promotes breastfeeding success through improved latch-on and suckling reflexes, further ensuring optimal nutrition. The tactile stimulation from skin-to-skin interaction also stimulates neurological development by encouraging sensory learning while decreasing stress for both the infant and caregiver. This multifaceted approach reinforces the fundamental psychosocial connections necessary for healthy growth and development during critical early life stages [6, 7]. Kangaroo Mother Care also fosters interaction, bonding, and attachment between the mother and baby, which are crucial for emotional and social growth. Nevertheless, the ideal duration for kangaroo care has yet to be established [6, 7].
Kangaroo Mother Care (KMC) serves as a cost-effective substitute for incubator-based neonatal care. Research indicates that KMC has been associated with a 40% decrease in mortality rates among hospitalized infants with low birth weight (under 2,000 grams) [8]. This method enhances various health parameters in premature infants, including temperature regulation, respiratory function, and oxygen saturation, and reduces occurrences of apnea and bradycardia while also promoting weight gain. Even brief training in KMC, lasting as little as four hours daily, has been associated with improved outcomes for infants, such as reduced pain, lower rates of hypothermia, and enhanced growth. Additionally, KMC positively impacts maternal health by facilitating breastfeeding, alleviating anxiety, and boosting self-confidence [9, 10].
Globally, kangaroo care has become the established standard for the treatment of infants with low birth weight (LBW) once they have reached a stable condition. Research indicates that the implementation of Kangaroo Mother Care (KMC) can lead to a 40% reduction in infant mortality, as the majority of deaths in incubator settings occur during the initial days before the infant stabilizes [11, 12]. The anticipated advantages of kangaroo care encompass a stable heart rate, enhanced oxygen saturation and respiratory rate, improved feeding practices, and increased maternal milk production. Additionally, it is frequently regarded as a method to alleviate stress for infants in neonatal intensive care units. Furthermore, kangaroo care positively influences neurological, cognitive, emotional, behavioral, and social development, both in the short and long term [13].
The findings of randomized clinical trials in healthy infants show that kangaroo care is associated with improved breastfeeding and beneficial results in mother-infant primary care, infant crying, and cardio-respiratory system stability [14]. Considering the importance of the kangaroo care method in the special care of newborns and the developmental course of premature babies, and the lack of a similar study in Qazvin province, we decided to conduct a study to investigate the relationship between KMC and the amount of respiratory support in premature babies hospitalized from 2022 to 2023.
2. METHODS
The present investigation is a retrospective cohort study focusing on premature infants who were hospitalized at Qazvin University of Medical Sciences from 2022 to 2023. The study population consisted of premature infants (defined as those with a gestational age of less than 37 weeks) admitted to the Neonatal Intensive Care Unit (NICU) due to respiratory failure. An accessible sampling method was employed, utilizing the medical records of newborns maintained by the nursing staff, which were subsequently provided to the research team. The necessary samples were randomly selected from the list of premature infants admitted to the hospital during the specified period, ensuring a simple random sampling approach. To ascertain the statistical power of the study at 80%, the required sample size was determined using equation (1), establishing a minimum sample size of 94 individuals in each group. The parameters necessary for this calculation were derived from the research conducted by Dhyey Pandya et al. [15].

Patients were observed based on the established entry and exit criteria, and those who fulfilled the required conditions were incorporated into the study. The inclusion criteria specified premature infants (gestational age of less than 37 weeks) who required respiratory assistance (i.e., those placed in an oxygen hood following weaning from mechanical ventilation). The exit criteria included infants born to mothers with substance abuse issues and infants and mothers who were non-nationals.
The exposure group comprised premature infants (born at less than 37 weeks of gestation) who were removed from the ventilator and placed under an oxygen hood. Kangaroo Mother Care (KMC) was initiated for a minimum of thirty minutes each day, and feeding for the infants commenced. Mothers received essential training and were followed over 14 days. On the other hand, the control group comprised infants who did not receive KMC due to various factors, including maternal underlying health conditions, maternal hospitalization, family distance, and challenges in daily hospital visits. Similar to the exposure group, the infants in the control group were also monitored for 14 days.
Patient data were gathered utilizing a checklist that encompassed demographic details such as age, sex, weight, time of birth, initiation of Kangaroo Mother Care (KMC), and weight at discharge. Additional information included the duration of KMC, length of hospitalization, time taken to achieve full feeding, presence of concomitant heart disease in the newborn, as well as respiratory distress syndrome (RDS) and sepsis (indicated by a positive blood culture and/or CRP levels exceeding 7). Vital signs comprised blood oxygen saturation, blood pressure, heart rate, respiratory rate, and body temperature, along with laboratory tests including blood culture and CRP levels. There were no systematic errors, including selection bias or information bias, in this study. The researchers strictly followed all ethical principles and guidelines set forth by the Helsinki Declaration when conducting this research. The legal guardians of the participants provided informed verbal consent prior to study enrollment.
The analysis of the variables was conducted using SPSS version 20 software. Descriptive statistics were derived by computing the frequency, mean, and standard deviation according to the nature of the variables. The examination of the variables was performed using the independent t-test to explore the relationship between quantitative variables and two categorical variables, one-way ANOVA for assessing quantitative variables against three categorical variables, and chi-square tests to analyze the relationships among qualitative variables. A significance threshold of less than 0.05 was established.
3. RESULTS
In the recent evaluation, a total of 188 premature babies were evaluated and compared in two groups. The findings showed that in the KMC group, 54 infants (57.4%) were male and 40 (42.6%) were female, while in the control group, 49 (52.1%) were male and 45 (47.9%) were female, and the difference in observed proportions was not statistically significant (p > 0.05). The mean gestational age (GA) in the KMC group was 32.23 (1.62) and in the control group was 32.28 (1.56) weeks, which was not statistically significant (p >0.05) Tables 1 and 2.
| Variable | KMC group Freq. (%) |
Control group Freq. (%) |
p-value |
|---|---|---|---|
| Gender Male Female |
54 (4/57) 40 (6/42) |
49 (1/52) 45 (9/47) |
0.4 |
| Heart disease | 6 (6.4) | 5 (5.3) | 0.7 |
| RDS | 63 (67) | 54 (57.4) | 0.1 |
| BPD | 20 (21.3) | 18 (19.1) | 0.7 |
| Culture result (first) Positive Negative |
2 (2.1) 92 (97.9) |
2 (2.1) 92 (97.9) |
1.0 |
| Culture result (first) Positive Negative |
0 94 (100) |
0 94 (100) |
1.0 |
| Variable | KMC group Mean (SD) |
Control group Mean (SD) |
p-value |
|---|---|---|---|
| Pregnancy week | 32.23 (1.62) | 32.28 (1.56) | 0.8 |
| Birth weight | 1580.90 (259.93) | 1619.47 (238.64) | 0.2 |
| KMC base weight | 1548.19 (258.66) | 1584.89 (274.80) | 0.3 |
| Discharge weight of the baby | 1734.84 (152.76) | 1756.06 (146.59) | 0.3 |
| Length of hospitalization | 20.11 (9.80) | 21.81 (11.84) | 0.2 |
| Full feed time | 8.57 (4.01) | 8.05 (3.69) | 0.3 |
| CRP (first) | 12.32 (11.51) | 8.95 (9.18) | 0.03 |
| CRP (last) | 4.07 (1.86) | 3.87 (1.59) | 0.4 |
| Days under the hood oxygen | 2.60 (1.66) | 2.12 (1.65) | 0.049 |
| Days under the ambient oxygen | 12.20 (7.38) | 13.23 (6.46) | 0.3 |
The mean newborn weight at birth, KMC starting weight, and newborn weight at discharge, based on the independent t-test between the two groups, showed no statistically significant difference (p >0.05).
The means of the heart rate and respiratory rate of the newborns on each of the 14 days evaluated in the two groups did not show a statistically significant difference (p >0.05) (Figs. 1 and 2).
The findings from the repeated measures analysis of variance, utilizing the Greenhouse-Geisser correction, indicated that the mean heart rate in the KMC group decreased from 143.95 on the first day to 125.30 by the 14th day. Conversely, the average heart rate in the control group declined from 143.96 on the first day to 125.23 on the 14th day (F = 379.85, df = 9.01, p = 0.001). Additionally, the analysis revealed an interaction effect between the two groups under investigation, with no statistically significant difference over time (F = 380.85, df = 1, p = 0.9). On the other hand, the differences in the observed mean within each group over the specified follow-up periods were statistically significant (p < 0.05), and there was no statistically significant difference between the two study groups (p >0.05).
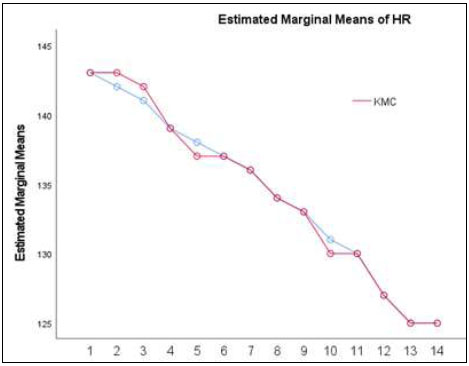
The mean of the heart rate of the newborns in each of the 14 days.
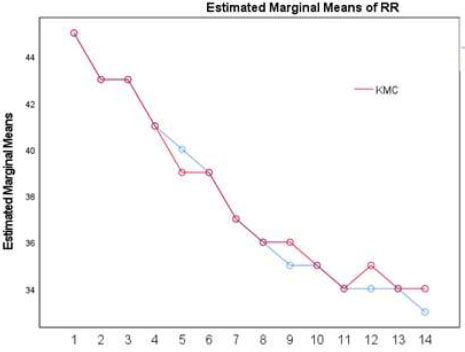
The mean of the respiratory rate of the newborns in each of the 14 days.
The mean systolic blood pressure exhibited statistically significant differences across all assessment stages over the 14 days, with the KMC group demonstrating lower levels (p<0.05).
The findings from the repeated measures analysis of variance indicated that the mean systolic blood pressure in the KMC group rose from 70.94 on the initial day to 81.43 by the 14th day. Similarly, the mean systolic blood pressure in the control group increased from 76.02 on the first day to 89.19 on the 14th day (F = 90.12, df = 4.74, p = 0.001). Additionally, the analysis revealed a significant interaction effect between the two groups over time (F = 17.242, df = 1, p = 0.001). This suggests that within each group, the differences in the observed averages across the study period were statistically significant (p < 0.05). It was found that the mean systolic blood pressure had a statistically significant difference only on the 14th day (p < 0.05), and at other follow-up times, the difference between the two groups was not significant (p > 0.05). Moreover, the mean diastolic blood pressure in the KMC group rose from 34.71 on the first day to 38.17 by the 14th day. Similarly, the mean diastolic blood pressure in the control group increased from 35.49 on the first day to 39.49 on the 14th day (F = 17.36, df = 8.88, p = 0.001). Additionally, an interaction effect was noted between the two groups over time (F = 2.129, df = 1, p = 0.1). This indicates that within each group, the differences in the observed averages over the study follow-up period were statistically significant (p < 0.05). Furthermore, a statistically significant difference was also identified between the two groups over time (p<0.05).
The mean body temperature of the premature infants on the first, second, and third days was statistically different in the two groups and was lower in the KMC group. On the fourth day, there was no statistically significant difference in body temperature between the two studied groups (p > 0.05). The results of repeated-measures analysis of variance showed that the mean body temperature in the KMC group increased from 35.68 on the first day to 36.68 on the 14th day. Similarly, the average body temperature in the control group increased from 35.99 on the first day to 36.59 on the 14th day (F = 37.21, df = 6.93, p = 0.001). Moreover, it was observed that within each of the studied groups, the difference between the observed means during the follow-up period was statistically significant (p < 0.05), but no statistically significant difference was observed between the two studied groups during the follow-up period (p> 0.05).
4. DISCUSSION
The results of repeated-measures analysis of variance showed that the mean body temperature in the KMC group was statistically different from that of the control group, increasing from 35.68 on the first day to 36.68 on the 14th day. The mean systolic and diastolic blood pressures exhibited statistically significant differences across all assessment stages over the 14-day period, with the KMC group demonstrating lower levels. The means of the heart rate and respiratory rate of the newborns over each of the 14 days evaluated in the two groups did not show a statistically significant difference. Kangaroo Mother Care (KMC) is characterized by early, ongoing, and extended skin-to-skin contact between a mother and her infant, which may also include the involvement of fathers as caregivers. This practice is complemented by frequent and exclusive breastfeeding [3]. For premature infants in the neonatal intensive care unit (NICU), the experience can be a fight for survival, involving invasive procedures, harsh lighting, and an environment stripped of the comforting presence of their mothers [1]. In the NICU, premature infants encounter various stressors, including invasive medical procedures, bright lighting, and noise generated by medical devices [1]. Interventions that are both beneficial and essential within the NICU can elicit physiological and behavioral reactions in preterm infants. Furthermore, the separation of these infants from their mothers, along with the NICU environment, restricts visual, tactile, and auditory interactions, thereby impacting maternal bonding. Consequently, the implementation of Kangaroo Mother Care (KMC) has the potential to enhance outcomes for premature infants [2, 3].
The findings of this study showed that the implementation of Kangaroo Mother Care (KMC) did not influence the respiratory indices of newborns. The findings of our study were consistent with the results of other studies [16-18]. For example, in a study by Gable et al. (2023), a total of 32 infants were enrolled, and the results showed that no variations in work of breathing (WOB) or vital signs were observed. Adjusting for respiratory support or the randomization/initial location did not alter the outcomes [16]. Similarly, the study conducted by Bisanalli et al. (2019) indicated that there were no notable alterations in respiratory rate or saturation levels [17]. Similarly, Dehghani et al. (2017) found no significant differences in the breathing rate between the two groups studied [18]. The decrease in the frequency of breathing following Kangaroo Mother Care (KMC) may be attributed to the upright position of the newborn during the caregiving process. This positioning enhances both ventilation and perfusion, thereby improving respiratory function [19].
This study showed that the increase in body temperature was higher in the KMC group. The results align with the conclusions drawn from numerous studies on this matter [18, 20, 21]. Increasing temperatures, especially for low-birth-weight and premature infants who are prone to hypothermia, are highly beneficial and enhance treatment outcomes. Conversely, as heat loss occurs, there is an increase in metabolic rate and oxygen consumption, which can result in physiological and metabolic instability, challenges in homeostasis, exacerbation of apnea, and hindered weight gain [18]. On the other hand, there are studies that are inconsistent with the findings of our study. For example, the study conducted by Bisanalli et al. (2019) indicated that there were no notable alterations in temperature between the two study groups [17]. The findings of a systematic review indicated that stable preterm infants, regardless of whether they receive respiratory support, exhibit no significant differences in heart rate (HR), oxygen saturation (SpO2), and fractional time of oxygen exposure (FTOE) during kangaroo care (KC) when compared with standard incubator care. Additionally, regional cerebral oxygen saturation (rScO2) remains stable during KC, showing a slight upward trend. The researchers in this study concluded that further research with enhanced methodological rigor is required to validate these results [22].
In this study, the means of the heart rate and respiratory rate of the newborns on each of the 14 days evaluated in the two groups did not show a statistically significant difference. The results of a study indicated that infants who were provided with Kangaroo Mother Care (KMC) exhibited a higher average heart rate, oxygen saturation, and body temperature; however, these findings did not reach statistical significance [23]. The results of a study consistent with ours showed that the temperature of newborns decreased during Kangaroo Mother Care (KMC) compared with care provided in an incubator, despite the temperature readings remaining within the normal range [24]. In a study by Sontheimer et al., it was demonstrated that in newborns receiving Kangaroo Mother Care (KMC) as opposed to incubator care, the heart rate, respiratory rate, arterial oxygen saturation, and body temperature remained stable [5]. Placing the newborn in direct skin contact with the mother effectively reduces heat loss and can improve treatment outcomes [18, 25]. The results of this research are applicable to infants born in Qazvin city, and it is advisable to carry out similar studies in other cities and provinces.
CONCLUSION
It was determined that Kangaroo Mother Care (KMC), which entails skin-to-skin contact between an infant and caregiver, has been shown to significantly influence physiological parameters, including body temperature and blood pressure. Conversely, the means of the heart rate and respiratory rate did not show any significant differences. Further research with improved methodological rigor is necessary to confirm these results. It was concluded that by promoting direct contact, KMC helps with thermoregulation, allowing neonates to maintain a stable body temperature through the warmth of the caregiver's skin, which is vital in preventing hypothermia.
LIMITATION
One limitation of this study was its design, which did not utilize a prospective cohort approach, potentially leading to inaccuracies in the recording of case information. Future research should consider employing a prospective cohort design to mitigate these issues. Prospective cohort studies are suggested to provide a more robust level of evidence.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contribution to the paper as follows: S.N., M.R.M.: Conceptualization; S.H.M.: Data collection; A.R.M. Draft manuscript;. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| KMC | = Kangaroo Mother Care |
| NICU | = Neonatal Intensive Care Unit |
| RDS | = Respiratory Distress Syndrome |
| FTOE | = Fractional Time of Oxygen Exposure |
| HR | = Heart Rate |
| KC | = Kangaroo Care |
| rScO2 | = Regional Cerebral Oxygen Saturation |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study received ethical approval from the Research Ethics Committee in the Qazvin University of Medical Sciences, Iran, with Ethical code of IR.QUMS.REC.1402.456.
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Legal guardians of the participants provided informed verbal consent prior to study enrollment.
AVAILABILITY OF DATA AND MATERIAL
The data sets used and/or analysed during this study are available from the corresponding author [M.M] upon request.
ACKNOWLEDGEMENTS
The authors would like to thank the participating neonates and their parents, especially the mothers for being compliant with the study.

