All published articles of this journal are available on ScienceDirect.

Sociodemographic Factors and Parenting Patterns Related to Stunting in Children Under Five Years in Pekanbaru, Indonesia: A Structural Equation Modeling Analysis
Authors Info & Affiliations
Abstract
Background
Stunting is a critical nutritional issue that affects children under five, significantly impacting their health and development. Pekanbaru has been identified as a priority area for stunting intervention, with the Lima Puluh Health Center reporting the highest prevalence of stunting in 2021. This study aimed to analyze the associations among sociodemographic factors, parenting patterns, and stunting in children under five in Pekanbaru, Indonesia.
Methods
A case-control study was conducted with 108 children (54 cases of stunting and 54 controls). All children with stunting who met the criteria were considered case samples. Control samples were randomly selected from the same Integrated Health Posts as the cases. Data were collected via validated questionnaires and analyzed using structural equation modeling.
Results
Sociodemographic factors, including maternal knowledge, attitudes, and family income, were indirectly associated with stunting through their influence on parenting patterns (β = 1.33; p < .001). Parenting patterns, encompassing feeding practices, hygiene practices, environmental sanitation, and health service use, directly impacted stunting (β = 0.09; p = .049). Notably, the structural equation model exhibited good fit indexes (goodness-of-fit index = 0.922; root mean square error of approximation = 0.073), confirming its validity.
Conclusion
Parenting patterns were found to mediate the relationship between sociodemographic factors and stunting. Holistic interventions that address sociodemographic factors while supporting parental education and improved parenting practices are essential for reducing the prevalence of stunting.
1. INTRODUCTION
Stunting refers to impaired growth and development resulting from inadequate nutrition, recurrent infectious diseases, and/or suboptimal parenting practices [1]. It has become a major global health issue due to its profound impact on physical growth, cognitive development, and long-term productivity [2]. Worldwide, approximately 22% of children under the age of five (149.2 million) had stunting in 2020, with the highest prevalence occurring in Asia and Sub-Saharan Africa. In Asia, South Asia had the most significant prevalence, accounting for more than 50% of stunting among children worldwide [3]. In Indonesia, the prevalence of stunting is still relatively high despite a decrease in the stunting rate from 27.67% in 2019 to 24.4% in 2021 and 21.6% in 2022 [4]. Stunting remains a significant challenge, contributing to reduced quality of life and economic consequences, including lower productivity, poverty, and inequality [1, 5, 6].
In the 2020–2024 National Medium-Term Development Plan (RPJMN), a key objective was to reduce the prevalence of stunting by 14% by 2024 [7]. To accomplish this target, the government emphasized addressing stunting as a priority project within the health sector [7]. According to the 2021 Indonesian Nutrition Status Survey report, Riau Province had a stunting prevalence of 22.4%, while Pekanbaru had a prevalence of 11.4% [8]. Given this data, the Pekanbaru government aimed to reduce stunting by 6.34% by 2024. Consequently, Pekanbaru was identified as a designated focal location for stunting reduction efforts in 2021. Among the focal locations was the health center in Lima Puluh, which has the highest prevalence of stunting among the health centers in Pekanbaru [9].
Numerous studies have identified various risk factors for stunting [10, 11], finding that stunting results from a combination of direct, indirect, and underlying factors. Direct causes include inadequate nutritional intake and the frequent occurrence of infections, particularly diarrhea and acute respiratory infections, which impair nutrient absorption and overall growth [12-14]. Iron deficiency anemia is also significantly associated with stunting among children in developing countries [15]. Indirectly, parenting practices play a critical role in stunting. Poor feeding practices, a lack of hygiene, insufficient sanitation, and the underuse of healthcare services contribute significantly to stunting [16, 17]. For instance, inappropriate feeding can result in nutrient deficiencies, while poor hygiene and sanitation increase exposure to pathogens that cause infections, exacerbating growth issues [18]. Sociodemographic factors underlie these issues. Limited maternal education and knowledge about nutrition and health can hinder effective caregiving [19, 20]. Additionally, low levels of maternal nutritional literacy and knowledge can increase the risk of stunting in children [21]. Low family income also restricts access to diverse and nutritious foods, proper healthcare, and sanitation facilities, creating an environment that perpetuates stunting [22]. These interconnected factors emphasize the complexity of stunting and the need for multifaceted stunting interventions.
While many studies have explored the determinants of stunting, few have investigated how direct and indirect factors influence the incidence of stunting. To fully understand these factors and their complex relationships, this study employs structural equation modeling (SEM), a robust analytical approach that aligns with the study’s conceptual framework, to examine the relationship between sociodemographic and parenting factors with stunting in children under five. SEM allows for comprehensively analyzing how sociodemographic factors and parenting patterns interconnect and contribute to stunting. This methodological approach is a novel aspect of the study, providing deeper insights into these multifaceted dynamics. Understanding these relationships is crucial for designing targeted and effective interventions to reduce stunting. By identifying key sociodemographic and parenting factors, this study can inform policymakers and healthcare providers on how to address the underlying causes of stunting, improve caregiving practices, and optimize resource allocation.
2. MATERIALS AND METHODS
2.1. Study Design and Type
This research followed a case-control design. The stunting cases were children under five who were classified as stunted based on the height-for-age index, with a Z-score of less than -2 standard deviations (SDs). Contrastingly, the control cases were children under five who were not stunted, as indicated by a height-for-age Z-score greater than -2 SDs. The research was conducted at the Lima Puluh Community Health Service in Pekanbaru, Riau Province, Indonesia, over a six-month period from October 2021 to April 2022.
2.2. Population and Sampling
The study population comprised all children aged 12–59 months in the Lima Puluh Health Centre Working Area, Pekanbaru, Riau Province, Indonesia. The case population included short and very short children under five, with a height-for-age Z-score of less than -2 SDs, totaling 58 children. The control population comprised children under five with a height-for-age Z-score of -2 SDs or higher who visited the integrated health posts (IHPs), totaling 612 children.
Respondents were the mothers of the children. The sample size was calculated using the sample size formula for case-control hypothesis testing, with an alpha of 5% and a beta of 80%. P1 = OR * P2 = 2.0 * 0.23; P2 = Proportion of mothers with little knowledge about children under five who are not stunted = 0.23 [23]. The formula (1) used was as follows:
 |
(1) |
A minimum sample size of 54 children under five was obtained. The case-to-control ratio was 1:1, resulting in 54 children under five as stunting cases and 54 as control cases. A total of 108 cases were obtained. Cases were selected from all children under five who were identified as having stunting, and these cases were recorded in the electronic application for recording and reporting community-based nutrition (e-PPGBM) in 2021 from each IHP. Controls were chosen through stratified random sampling and were matched to the case population of each IHP. The inclusion criteria for this study required that children be under five and living with both parents in the same household. Exclusion criteria were that children were born prematurely or had disabilities.
2.3. Exogenous and Endogenous Variables
The exogenous variables included sociodemographic factors and parenting patterns. Sociodemographic factors consisted of seven indicators: maternal knowledge, maternal age, maternal education, family structure, maternal employment status, family income, and maternal attitude. Maternal knowledge referred to a mother’s collective understanding of stunting, including its causes and effects, and her monitoring of the growth and development of children under five. Maternal knowledge was assessed based on the mother’s total score on the questionnaire. If the mother answered a question correctly, she received a score of 1; if she answered incorrectly, she received a score of 0. Maternal attitude referred to the mother’s response and approach to meeting the nutritional needs of her children. Maternal attitude was measured using a Likert scale.
Parenting patterns comprised seven indicators: feeding practices, psychological stimulation, hygiene practices, environmental sanitation, the use of health services, growth and development stimulation, and the availability of educational game tools. These seven indicators were measured using a Likert scale. Feeding practices referred to the specific patterns and practices that mothers employed to fulfill their child’s nutritional needs, considering factors such as age-appropriate foods, food types, portion sizes, and feeding schedules. Psychosocial stimulation involved the actions and behaviors that mothers, fathers, grandparents, or other caregivers demonstrated to provide emotional and verbal stimuli and skin-to-skin contact to children, such as cuddling, hugging, and interactive engagement. Hygiene practices encompassed the measures mothers took to maintain their child’s cleanliness, including their personal hygiene, the cleanliness of their clothes and diapers, the cleanliness of toys, and the hygiene of the food provided to them. Environmental sanitation pertained to the overall cleanliness and hygiene of the child’s living environment, including the cleanliness of their bedroom and playroom, the availability of waste disposal facilities, and access to a clean water source within the household. The use of health services referred to the mother’s behavior and practices in accessing health services for her child, such as regular visits to the community health center or other healthcare facilities to monitor the child’s growth and development. Growth and development stimulation involved the provision of physical and motor exercises, as well as early childhood stimulation activities. The availability of educational game tools referred to the presence of educational toys and tools within the home environment.
The endogenous variable in this study was stunting, which was assessed using two indicators: the height-for-age Z-score and the child’s development status. The Developmental Pre-Screening Questionnaire was used to measure developmental progress in children younger than five.
2.4. Data Collection
Primary data for the research were obtained through interviews with participants using a validated and reliable questionnaire. Height data were collected via re-measuring based on the e-PPGBM report from the Pekanbaru Health Office. The data underwent various processing steps, including editing, coding, processing, and cleaning, based on the characteristics and categories of the data. Subsequently, the data were entered into a computer using the IBM SPSS AMOS 24 program.
2.5. Data Analysis
Univariate data analysis was performed to describe each variable studied. Multivariate analysis was conducted using SEM in several stages. First, a model was developed based on theoretical foundations. Second, a path diagram was constructed to represent the relationships among the variables in the model visually. Third, the path diagram was converted into a set of structural equations that mathematically depicted the proposed relationships. The fourth step involved selecting appropriate data and estimation techniques for the model. Model identification was then conducted to ensure that the model was identifiable and estimable. The model was evaluated by assessing assumptions and examining its fit using various goodness-of-fit criteria. These criteria included the p-value of the chi-squared test (> .05), the goodness-of-fit index (GFI; ≥ 0.9), the adjusted goodness-of-fit index (AGFI; ≥ 0.9), the normed fit index (NFI; ≥ 0.9), the Tucker–Lewis index (TLI; ≥ 0.9), and the root mean square error of approximation (RMSEA; < 0.08) [24, 25].
3. RESULTS
3.1. Sample Recruitment
This study conducted a sample recruitment process using the stratified random sampling of control. All children with stunting under five were cases sampled. From the total target population of 967 children under five, 612 children were included in the study population after excluding 355 children who did not visit the IHP. Subsequently, 54 children under five with stunting were selected as the case sample and 54 children under five without stunting were selected as the control sample. Ineligible children were excluded from the study, including one child who did not live with her parents, one child who was born prematurely, and two children who refused to participate (Fig. 1).
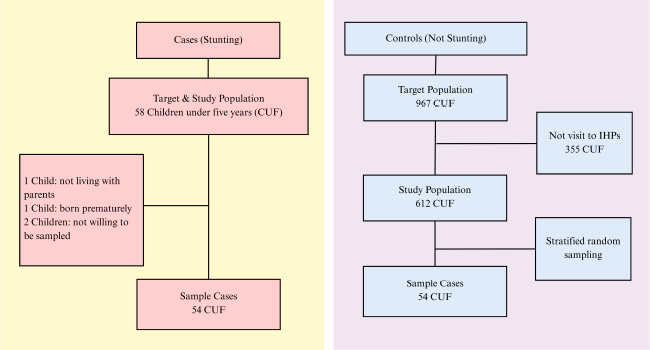
Sample recruitment.
| Indicators | Cases | Controls | Total | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Maternal Knowledge | ||||||
| Low | 26 | 48.1 | 28 | 51.9 | 54 | 50.0 |
| Medium | 5 | 9.3 | 11 | 20.4 | 16 | 14.8 |
| High | 11 | 20.4 | 5 | 9.3 | 16 | 14.8 |
| Very High | 12 | 22.2 | 10 | 18.5 | 22 | 20.4 |
| Mother’s Age | ||||||
| < 20 years | 0 | 0.0 | 1 | 1.9 | 1 | 0.9 |
| 20-34 Years | 33 | 61.1 | 39 | 72.2 | 72 | 66.7 |
| >34 Years | 21 | 38.9 | 14 | 25.9 | 35 | 32.4 |
| Education | ||||||
| Elementary school and below | 7 | 13.0 | 1 | 1.9 | 8 | 7.4 |
| Junior High School | 13 | 24.1 | 11 | 20.4 | 24 | 22.2 |
| Senior High School | 26 | 48.1 | 34 | 63.0 | 64 | 55.6 |
| Colleges | 8 | 14.8 | 8 | 14.8 | 16 | 14.8 |
| Maternal Employment Status | ||||||
| Employed | 11 | 20.4 | 9 | 16.7 | 20 | 18.5 |
| Unemployed | 43 | 79.6 | 45 | 83.3 | 88 | 81.5 |
| Family structure | ||||||
| 1 child | 5 | 9.3 | 11 | 20.4 | 16 | 14.8 |
| 2 children | 22 | 40.7 | 24 | 44.4 | 46 | 42.6 |
| 3 children | 18 | 33.3 | 14 | 25.9 | 32 | 29.6 |
| >4 children | 9 | 16.7 | 5 | 9.3 | 14 | 13.0 |
| Family Income | ||||||
| Quartile 1 | 23 | 42.6 | 12 | 22.2 | 35 | 32.4 |
| Quartile 2 | 10 | 18.5 | 13 | 24.1 | 23 | 21.3 |
| Quartile 3 | 15 | 27.8 | 17 | 31.5 | 32 | 29.6 |
| Quartile 4 | 6 | 11.1 | 12 | 22.2 | 18 | 16.7 |
| Maternal Attitude | ||||||
| Strongly disagree | 10 | 18.5 | 3 | 5.6 | 13 | 12.0 |
| Disagree | 14 | 25.9 | 12 | 22.2 | 26 | 24.1 |
| Agree | 13 | 24.1 | 19 | 35.2 | 32 | 29.6 |
| Strongly Agree | 17 | 31.5 | 20 | 37.0 | 37 | 34.3 |
3.2. Sociodemographic Factors
Table 1 provides an overview of the sociodemographic characteristics of the study participants. Half of the mothers (50%) had inadequate knowledge about stunting. Most mothers (66.7%) were between 20 and 34 years old. Regarding education, most mothers (55.6%) had completed high school, suggesting moderate educational attainment. Employment data revealed that most mothers (81.5%) were housewives. Regarding family structure, 42.6% of mothers had two children, the most common family structure. Income distribution showed that 32.4% of families were in the lowest income quartile. Notably, more than half of the mothers (63.9%) displayed positive attitudes toward stunting prevention. More mothers among the stunting cases had high (20.4%) or very high (22.2%) levels of maternal knowledge, were > 34 years old (38.9%), had attended elementary school or below (13%), had attended junior high school (24.1%), were employed mothers (20.4%), had a family structure with three children (33.3%) or more (16.7%), had a family income in quintile 1 (42.6%), and had a maternal attitude of strongly disagreeing (18.5%) or disagreeing (25.9%).
3.3. Parenting Patterns
Table 2 displays the parenting practices among the stunting and control case groups. Among the mothers, 25% exhibited very inappropriate feeding behaviors. Contrastingly, psychological stimulation was appropriate, with 87.7% of mothers engaging in suitable practices. Hygiene practices were satisfactory for most participants, as 77.8% maintained proper hygiene standards. However, environmental sanitation was suboptimal, with 38.9% of mothers displaying inappropriate practices. Health service use showed that 45.4% of mothers made excellent use of healthcare services for their children. Additionally, 83.3% of mothers provided suitable stimulation for growth and development, while 75% ensured the availability of educational play tools at home. There were more mothers among the stunting cases than the control cases who displayed very unsuitable feeding practices (31.5%) or unsuitable psychological stimulation (7.5%), hygiene practices (16.7%), environmental sanitation (42.6%), the use of health services (24.1%), growth and development stimulation (11.1%), and availability of educational game tools (11.1%).
| Indicators | Cases | Controls | Total | ||||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Feeding Practice | |||||||
| Very unsuitable | 17 | 31.5 | 10 | 18.5 | 27 | 25.0 | |
| Unsuitable | 9 | 16.7 | 10 | 18.5 | 19 | 17.6 | |
| Suitable | 16 | 29.6 | 12 | 22.2 | 28 | 25.9 | |
| Very suitable | 12 | 22.2 | 22 | 40.7 | 34 | 31.5 | |
| Psychosocial Stimulation | |||||||
| Unsuitable | 4 | 7.5 | 1 | 1.9 | 5 | 4.7 | |
| Suitable | 47 | 88.7 | 46 | 86.8 | 93 | 87.7 | |
| Very suitable | 2 | 3.8 | 6 | 11.3 | 8 | 7.5 | |
| Hygienic Implementation | |||||||
| Very unsuitable | 1 | 1.9 | 0 | 0.0 | 1 | 0.9 | |
| Unsuitable | 9 | 16.7 | 3 | 5.6 | 12 | 11.1 | |
| Suitable | 41 | 75.9 | 43 | 79.6 | 84 | 77.8 | |
| Very suitable | 3 | 5.6 | 8 | 14.8 | 11 | 10.2 | |
| Environmental sanitation | |||||||
| Very unsuitable | 4 | 7.4 | 2 | 3.7 | 6 | 5.6 | |
| Unsuitable | 23 | 42.6 | 19 | 35.2 | 42 | 38.9 | |
| Suitable | 19 | 35.2 | 19 | 35.2 | 38 | 35.2 | |
| Very suitable | 8 | 14.8 | 14 | 25.9 | 22 | 20.4 | |
| Use of Health Services | |||||||
| Very unsuitable | 2 | 3.7 | 0 | 0.0 | 2 | 1.9 | |
| Unsuitable | 13 | 24.1 | 9 | 16.7 | 22 | 20.4 | |
| Suitable | 18 | 33.3 | 17 | 31.5 | 35 | 32.4 | |
| Very suitable | 21 | 38.9 | 28 | 51.9 | 49 | 45.4 | |
| Growth and Development Stimulation | |||||||
| Very unsuitable | 2 | 3.7 | 1 | 1.9 | 3 | 2.8 | |
| Unsuitable | 6 | 11.1 | 5 | 9.3 | 11 | 10.2 | |
| Suitable | 44 | 81.5 | 46 | 85.2 | 90 | 83.3 | |
| Very suitable | 2 | 3.7 | 2 | 3.7 | 4 | 3.7 | |
| Availability of Educational Game Tools | |||||||
| Very unsuitable | 1 | 1.9 | 1 | 1.9 | 2 | 1.9 | |
| Unsuitable | 6 | 11.1 | 5 | 9.3 | 11 | 10.2 | |
| Suitable | 40 | 74.1 | 41 | 75.9 | 81 | 75.0 | |
| Very suitable | 7 | 13.0 | 7 | 13.0 | 14 | 13.0 | |
| Estimate (β) | S.E | C.R | p-value | Conclusion | |||
|---|---|---|---|---|---|---|---|
|
Validity Parenting Stunting |
<-- <-- |
socio-demographic Parenting |
1.33 0.09 |
0.26 0.05 |
5.03 1.96 |
<0.001 0.049 |
Valid Valid |
| Maternal Attitude | <-- | socio-demographic | 1.00 | ||||
| Family Income | <-- | socio-demographic | 0.72 | 0.20 | 3.64 | <0.001 | Valid |
| Maternal Knowledge | <-- | socio-demographic | -0.90 | 0.20 | -4.40 | <0.001 | Valid |
| Feeding Practices | <-- | Parenting | 1.00 | ||||
| Hygienic Application | <-- | Parenting | 0.49 | 0.09 | 5.22 | <0.001 | Valid |
| Environmental Sanitation | <-- | Parenting | 0.79 | 0.12 | 6.55 | <0.001 | Valid |
| Use of Health Services | <-- | Parenting | 1.56 | 0.24 | 6.58 | <0.001 | Valid |
| Reliability | Estimate | 1-estimate | Construct Reliability | ||||
| Socio-demographic | |||||||
| Maternal Attitude | 0.68 | 0.54 | 0.6 | Reliable | |||
| Family Income | 0.46 | 0.79 | |||||
| Maternal Knowledge | 0.52 | 0.73 | |||||
| Parenting Patterns | |||||||
| Feeding Practices | 0.91 | 0.7 | 0.77 | Reliable | |||
| Hygienic Application | 0.59 | 0.73 | |||||
| Environmental Sanitation | 0.65 | 0.58 | |||||
| Utilization of Health Services | 0.6 | 0.64 | |||||
3.4. Structural Model of the Relationship Between Sociodemographics and Parenting Patterns with Stunting
After examining the value of the regression coefficient (r), it was found that from the sociodemographic factors, there were three indicators with a value of r > 0.5, namely maternal knowledge, maternal attitudes, and family income, while from parenting, there were four indicators with a value of r > 0.5, namely feeding practices, hygiene practices, environmental sanitation, and the use of health services. Subsequently, these indicators were included in the SEM analysis.
Table 3 presents the parameter estimation, validity, and reliability of the sociodemographic, parenting pattern, and stunting variables based on the SEM analysis. Sociodemographic factors were found to significantly influence both parenting patterns (β = 1.33, p < .001) and stunting outcomes (β = 0.26, p = .049). Among the sociodemographic indicators, family income had a positive association (β = 0.72, p < 0.001), while maternal knowledge had a negative association (β = -0.90, p < .001), suggesting that less maternal knowledge might increase the risk of stunting.
Parenting patterns were measured through four observed variables: feeding practices, hygiene practices, environmental sanitation, and the use of health services. All these variables were valid indicators of parenting patterns, with p-values < .001. The strongest influence was observed in the use of health services (β = 1.56), followed by environmental sanitation (β = 0.79) and hygiene practices (β = 0.49). The reliability assessment showed that most variables were consistent, with construct reliability values ranging from 0.6 to 0.77. Overall, the findings indicated that sociodemographic factors indirectly influenced stunting through parenting patterns.
The SEM confirmed the relationships among the sociodemographic factors, parenting patterns, and stunting. Fig. (2) illustrates the structural model, demonstrating a good fit with the data (GFI = 0.922, RMSEA = 0.073). The model showed that sociodemo graphic factors, including maternal knowledge, family income, and maternal attitudes, indirectly influence stunting through their effects on parenting patterns. Key parenting indicators, such as feeding practices (β = 1.00), hygiene practices (β = 0.49), environmental sanitation (β = 0.79), and health service use (β = 1.56), significantly contributed to reducing stunting risk. Stunting status was directly measured using height-for-age Z-scores and developmental indicators.
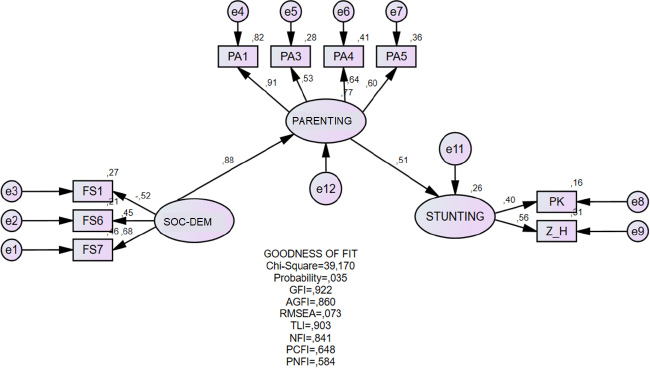
SEM of sociodemographic factors and parenting patterns with stunting. Height-for-Age Z-score (Z_H), development of children under five (PK), maternal knowledge (FS1), family income (FS6), and maternal attitude (FS7). Feeding practices (PA1), hygiene practices (PA3), environmental sanitation (PA4), and use of health services (PA5).
| Goodness of Fit | Model test Results | Cut off Value | Conclusions |
|---|---|---|---|
| Chi Square | 39.170 | < 48.602 | Good Fit |
| Probability | 0.035 | >0.05 | Not Fit |
| GFI | 0.922 | >0.90 | Good Fit |
| AGFI | 0.860 | >0.90 | Marginal Fit |
| RMSEA | 0.073 | <0.08 | Good Fit |
| TLI | 0.903 | >0.95 | Marginal Fit |
| NFI | 0.841 | >0.90 | Marginal Fit |
Table 4 presents the GFIs for the SEM. The chi-squared value (39.17) was within the acceptable range, and other indexes, including the GFI and RMSEA, indicated a well-fitting model. However, the AGFI (0.860) and NFI (0.841) were marginal, suggesting areas for potential refinement in future research models.
4. DISCUSSION
The study findings revealed a significant association between maternal knowledge, maternal attitudes, and family income as sociodemographic factors of maternal parenting. Maternal literacy and nutritional knowledge were also found to be strongly linked to the incidence of stunting [21]. Low maternal literacy levels and insufficient nutritional knowledge increase the risk of stunting in children, but they can be enhanced in areas such as infant and young child feeding, the selection and preparation of healthy and nutritious food products, and child growth and development [26]. Maternal knowledge plays a crucial role in managing and designing a healthy and nutritious diet for the mother and her family, thereby improving children’s nutrient intake. Research has indicated that maternal expertise impacts the prevalence of stunting among children under five from a nutritional perspective [27]. Specifically, mothers with a good understanding of menu preparation and food variety are more likely to take preventive measures against stunting [28]. Furthermore, higher maternal knowledge levels correlate with a more diverse diet and greater consumption of animal protein [29]. One practical approach to increasing maternal knowledge is health education and counseling being provided at IHPs or other healthcare facilities. Balanced nutrition counseling has been shown to significantly enhance mothers’ knowledge of malnutrition prevention in children under five [30]. By emphasizing the critical role of maternal knowledge in improving child health, this study reinforces prior findings while emphasizing the need for targeted educational interventions for mothers.
The findings also indicated that family income is a sociodemographic factor that significantly impacts maternal parenting and the risk of stunting. A higher income enables families to meet their nutritional needs adequately, while a lower income reduces food purchasing power [31]. This decreased purchasing power is linked to limited food diversity within the family. Sekartaji et al. conducted a study revealing minimal dietary diversity among Indonesian children, and this was attributed to factors such as education, mass media exposure, and socioeconomic status [32]. Similarly, Yunitasari et al.’s study found that children from families with higher wealth indexes are more likely to meet the minimum dietary diversity, minimum acceptable diet, and minimum meal frequency requirements compared to children from families with lower wealth indexes [33]. This study reinforces existing evidence by linking socioeconomic disparities to parenting practices and stunting outcomes, offering a nuanced understanding of how income levels mediate child nutrition.
The study findings suggested that feeding practices, hygiene practices, environmental sanitation, and the use of health services are significantly associated with maternal parenting. Inadequate child-feeding practices have been identified as a factor contributing to stunting [34]. Implementing responsive feeding practices and increasing children’s intake of high-quality protein can help them meet their nutritional needs, thereby reducing the incidence of stunting caused by chronic malnutrition [35]. Maternal hygiene practices, household sanitation, and drinking water conditions were also found to be significant indicators of parenting factors that contribute to the risk of stunting in children under five. Proper maternal hygiene is recognized as a crucial strategy for empowering mothers and protecting the health of both mothers and children. The incidence of diarrhea can be significantly reduced by increasing mothers’ knowledge and awareness of the benefits of clean water, for instance. Enhancing mothers’ attitudes and understanding can lead to notable improvements in child health outcomes, particularly in children experiencing diarrhea [36]. Children under five who live in environments with unclean water sources face a higher risk of stunting [37]. This study adds to the existing literature by demonstrating that improving maternal parenting, hygiene, and sanitation practices can serve as transformative pathways for reducing stunting risks.
This study examined the application of hygiene practices, focusing on household hygiene, sanitation practices, and the quality of water consumed by children under five. It was found that poor environmental sanitation can indirectly affect children’s health and nutritional status in this age group. That is, when the physical environment and family sanitation are well-maintained, they positively impact the overall health of household members. Maintaining the cleanliness of wells and water sources is crucial for minimizing the risk of infectious diseases.
The use of health services refers to the extent to which healthcare services are accessed and used for monitoring the growth of children under five. Studies have shown that children who infrequently use health services have the highest prevalence of stunting [2, 12]. The proactive involvement of health workers and IHPs in visiting the homes of children under five who rarely access health facilities is essential since it can ensure proper growth and development monitoring.
Some previous studies have identified a relationship between sociodemographic factors and stunting without considering the mediating role of parenting. The model obtained in this study demonstrated that sociodemographic factors influence stunting indirectly through parenting. These findings clarified how sociodemographic factors impact both parenting and stunting. This aligns with ecological theory, which emphasizes the importance of micro and macro environmental factors in determining child health [38]. Sociodemographic factors operate at the macro level, while parenting functions at the micro level, with interactions between these levels influencing the risk of stunting. A study in Ethiopia found that maternal education improves feeding practices [39], while research in the United States showed that low income and high mobility influence maternal parenting behavior [40]. A study in Ghana revealed that socioeconomic conditions are linked to children’s dietary patterns and food diversity [41], while a randomized controlled trial in Haiti demonstrated that responsive parenting can prevent growth faltering under constrained economic conditions [42]. These findings confirm that interventions aimed at improving parenting practices can reduce stunting risk, even when macro-level factors like economic conditions have not yet improved. Therefore, a holistic approach combining macro-level environmental improvements (such as education and income) with improved micro-level parenting practices is an effective strategy for addressing stunting sustainably.
Overall, the model demonstrated a good fit based on key indicators such as the chi-squared, GFI, and RMSEA values, although other indicators like probability, AGFI, TLI, and NFI fell into the marginal fit category. The model’s ability to explain the indirect effect of sociodemographic factors on stunting through parenting suggested that it was sufficiently representative in capturing these relationships. However, further improvements can be made to enhance the overall model fit, ensuring a more comprehensive understanding of the complex interplays among sociodemographic factors, parenting, and child health outcomes.
Holistic interventions are recommended to address stunting by providing education and support for parents, particularly in enhancing parenting practices while considering sociodemographic factors. This study bridges a critical gap in the literature by clarifying the mediating role of parenting in the relationship between sociodemographic factors and stunting, offering a more comprehensive model for addressing stunting at multiple levels.
4.1. Limitations
While helpful in identifying associations between risk factors and health outcomes, this case-control study had several limitations. Selection bias may have arisen if the cases and controls did not represent the general population adequately. This study used stratified random sampling to reduce selection bias, but relying on participants from IHPs may have caused children without regular healthcare access to be overlooked, affecting generalizability. Recall bias is another concern, as mothers’ self-reported data on parenting, feeding practices, and health service use may have been influenced by memory lapses or social desirability. Validated questionnaires were used to minimize this risk, though the risk could not be eliminated. Confounding factors may also have influenced the findings. Statistical adjustments with SEM were applied, but unmeasured variables such as dietary diversity, micronutrient deficiencies, and genetic predispositions could still have impacted the results. Future longitudinal studies should confirm the causal links between these factors and stunting.
CONCLUSION
This study explained how sociodemographic factors—including maternal knowledge, attitudes, and family income—shape parenting practices, influencing stunting in children under five. Key mediators included feeding habits, hygiene practices, sanitation, and health service use. Effective stunting reduction requires a holistic approach wherein socioeconomic gaps are addressed while parental education and caregiving support are improved. Health interventions should thus integrate nutrition education, economic empowerment, and community engagement factors to ensure that they have a sustainable impact. Policymakers must also prioritize multi-sectoral strategies, combining healthcare access, poverty alleviation, and behavioral change programs to break the cycle of malnutrition. Improving maternal knowledge and household resource use can also enhance child growth outcomes, while collaborative efforts among governments, NGOs, and local communities are essential to scale effective interventions and achieve long-term progress in child health.
AUTHORS’ CONTRIBUTIONS
The contributions of the authors to this study are as follows: M.M., H.I., H.M., and A.T. were responsible for the conceptualization of the research. Methodology and validation were carried out by M.M., R.M., and H.I., while M.M. and R.M. conducted the formal analysis. M.M., R.M., and H.I. prepared the original draft and curated the data. Review and editing of the manuscript were undertaken by R.W.B., M.M., and R.M. The investigation was conducted by M.M., H.I., H.M., E.D.A.S., and A.T. Funding for the project was acquired by M.M. and R.W.B., and project administration was managed by H.M., E.D.A.S., and A.T. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| SEM | = Structural Equation Modeling |
| SDs | = Standard Deviations |
| IHP | = Integrated Health Post |
| P1 | = Proportion of exposure in the case group |
| P2 | = Proportion of exposure in the control group |
| OR | = Odds Ratio |
| CUF | = Children Under Five Years |
| SE | = Standard Error |
| CR | = Critical Ratio |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was conducted in accordance with the Declaration of Helsinki and approved by Ethics Committee) of STIKes Hang Tuah Pekanbaru, Indonesia [Ethical approval code: 098/KEPK/STIKES-HTP/II/2022 on 17 February 2022].
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committees and with the 1975 Declaration of Helsinki, as revised in 2013.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article is available in the Zenodo Repository at https://zenodo.org/records/15392913, reference number: 10.5281/zenodo.15392912.
FUNDING
This study was funded by Universitas Hang Tuah Pekanbaru, Indonesia. Grant number: 12/STIKes-HTP/ XII/2021/0963.
ACKNOWLEDGEMENTS
Acknowledgments are extended to Universitas Hang Tuah Pekanbaru for providing funding support for this research. The researchers would like to express their gratitude to Pekanbaru City Health and Lima Puluh Community Health Centre for their cooperation and assistance throughout the study. We gratefully acknowledge the Varians Statistik Kesehatan for providing the boot camp and mentoring to improve manuscript writing.

