All published articles of this journal are available on ScienceDirect.

Kuwait Adults Physical Activity Levels during the COVID Lockdown
Authors Info & Affiliations
Abstract
Introduction
The Coronavirus 2019 disease (COVID) pandemic has led to unprecedented global restrictions, prompting concerns regarding physical inactivity.
Methods
This study investigated physical activity (PA) levels among adults in Kuwait during the COVID pandemic using the International PA Questionnaire Short Form (IPAQ-SF) distributed via an online survey through social media between June and July 2020.
Results
A total of 679 adults completed the IPAQ-SF. Results showed that 28.9% were in the high PA category, 35.8% in the moderate PA category, and 35.3% in the low PA category. While no significant differences between genders were detected (P=0.460), PA levels were significantly associated with age (P=0.022) among adults in Kuwait.
Discussions
This study emphasized the necessity for a targeted public health initiative to encourage PA during pandemics in Kuwait.
Conclusion
During viral pandemics, national health awareness programs to encourage PA should focus on adults over 45 years.
1. INTRODUCTION
The COVID pandemic caused a global health crisis and unprecedented restrictions. As of March 2023, there were over 600 million confirmed cases and 6.8 million deaths reported [1]. To relieve stress on health services and mitigate transmission, countries introduced several measures, including lockdowns, causing changes in daily life. These changes limited movement and social interactions, which led to reduced PA levels and an increase in the incidence of sedentary behavior [2, 3]. Physical inactivity and sedentary behavior are linked to a range of negative health outcomes, including cardiovascular disease, obesity, mental health problems, and type 2 diabetes [4-14].
In Kuwait, over 630,000 confirmed cases and 2,555 deaths were recorded [15]. To contain the spread of the virus, Kuwait implemented several measures, including full and partial lockdowns and restrictions on public gatherings. These measures may have contributed to changes in PA levels in the Kuwaiti population. Understanding these changes is crucial for public health purposes, given PA health benefits including increasing immunity and reducing the risk of viral respiratory infections [16-19]. The fundamental factors behind these health benefits may be attributed to enhanced immunity by increases in white blood cells following regular exercise [20-22]. Therefore, public awareness of the benefits of PA during a viral pandemic is important.
During viral epidemics, the recommendation is to perform moderate PA at home using personal equipment, as well as brisk walking outdoors while avoiding crowded gyms and sports with close physical contact [23-25]. While some countries were weighing the risks and benefits of continuing major competitions such as the 2020 Olympics, the advice for competitive athletes during viral outbreaks was to follow strict isolation procedures or postpone events [26-28]. Both public health and individual well-being benefit from following expert guidance on maintaining regular PA during viral outbreaks in Kuwait.
To date, one study investigated the effects of the COVID lockdown on PA in Kuwait [29]. In this study 33% of the participants reported performing less than 30 minutes of PA per week during June and July of 2020. Of the sample, 33% did not meet the WHO’s recommended guideline of at least 150 minutes of PA per week [30]. However, PA levels were not categorized according to the specific PA categories (low, moderate, and high), and the effects by gender or age were not examined. Therefore, to address these limitations, the IPAQ-SF (International Physical Activity Questionnaire Short Form) was used to assess PA levels among a sample of Kuwaiti adults during the pandemic [31]. This study aimed to investigate the levels of PA during the COVID pandemic in Kuwait and factors that are related to performing PA. The findings of the study are aimed at generating public health interventions to promote PA during pandemics.
2. MATERIALS AND METHODS
2.1. Study Design and Sample Demographic Information
This cross-sectional study used an online survey that was distributed using social media platforms such as X, formerly known as Twitter, and WhatsApp during June and July 2020. Participants were provided with a link to the survey with an electronic consent page preceding the survey to obtain their consent. Participation was voluntary, and no incentives were offered to complete the survey. Participants self-reported demographic information including age, height, weight, gender, governorate, marital status, number of children, employment, education level, whether they are smoking, exercising, and if they have any chronic illnesses such as diabetes or hypertension.
2.2. Inclusion and Exclusion Criteria
To take part in the study, participants had to be 21 years or older and living in Kuwait. The exclusion criteria involve participants younger than 21 years and living outside of Kuwait.
2.3. Data Collection Methods
2.3.1. IPAQ-SF Analysis
The IPAQ-SF was used to assess PA levels among study participants. The IPAQ-SF-short form is a well-established self-administered questionnaire that assesses PA spent in vigorous, moderate, and walking activities during the previous seven days [32, 33]. It is the most widely used tool to monitor PA levels worldwide [33] and it has demonstrated significant uses in policy change and decision-making in Europe [34]. The questionnaire comprises 7 items assessing frequency (number of days) and duration (minutes) spent in each PA category in the previous 7 days to avoid recall bias, in addition to an item related to the time spent sitting over the last 7 days. According to the IPAQ-SF, moderate PA is any PA that causes a moderate increase in heart rate and breathing rate, and is represented by 3-6 metabolic equivalents (METs) or the amount of oxygen consumed during rest [35]. Physical activities that are considered vigorous are those that result in rapid increases in breathing and heart rate and represent a value greater than 6 METs.
2.4. Ethics
The study protocol was approved by the Medical and Health Ethics Committee of the Ministry of Health in Kuwait (2020/1501) and was conducted under the declaration of Helsinki.
2.5. Data Analysis
The data were inspected, cleaned, and analyzed according to IPAQ-SF guidelines [31]. Missing data or incomplete responses were removed. To begin data analysis, the duration was converted from hours to minutes. The total amount of time, expressed in minutes, was then calculated for each category: walking, moderate, and engaging in vigorous PA. METs were calculated as follows: minutes from each category were then multiplied by the number of days and the METs value to determine the METs-minutes per week for each category using the typically assigned METs values of 3.3 for walking, 4.0 for moderate PA, and 8.0 for vigorous PA. To calculate the total METs-minutes per week, all categories are added together (Total METs= walking (METs) + moderate (METs) + vigorous (METs)). Based on whether respondents met the required standards for total METs-minutes per week and days per week of PA, respondents were then classified into a low, moderate, or high PA level category. Low PA refers to those who report some PA but do not meet moderate or high PA criteria. Moderate PA is considered as the following: three or more days of vigorous PA (>20 minutes each), five or more days of moderate PA, walking more than 30 minutes, or any combination of walking, moderate or vigorous intensity of more than 600 METS-minutes. The high PA category was defined as performing three or more days of vigorous PA with at least 1500 METs-minutes per week, or performing any PA (walking, moderate, or vigorous) for 7 or more days with a minimum of 3000 METs-minutes per week.
2.6. Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics version 28 (IBM Corp., Armonk, NY, USA). Numerical Data are presented as mean and standard deviation or as median and interquartile range and were analysed using one-way ANOVA. Categorical data were presented as frequencies and percentages and analysed using the Chi-square test or Fisher’s exact test, as appropriate. Ordinal logistic regression analysis was performed to assess factors associated with PA level. Significance was reached if P-value <0.05.
3. RESULTS
Table 1 represents the socio-demographic characteristics of the respondents. The study consisted of 679 participants, of which 45.2% were males and 54.8% were females, with an average body mass index was 27.8 ± 7.44 kg/m2. Most of the sample lived in Kuwait City (24.2%), Hawally (23.7%), and Mubarak Alkabeer (21.1%), while fewer participants participated from Farwaniya (13%), Alahmadi (10.6%), and Aljahra (7.5%). Most of the participants are married (54.2%), while 41.1% are single, and 4.7% either divorced or widowed. Of the sample, 47.4% had no children, 20.3% had 3 or 4 children, 19.3% had 1 or 2 children, and 13% had more than 4 children. Concerning employment status, 69.7% are employees, 17.7% are students, 6.5% are retired, and 6.2% are other. Participants who held an undergraduate degree were 62.7%, followed by doctoral and postgraduate degrees (19.1%), diploma (11.8%), and high school or less (6.3%). Furthermore, 21.8% of the sample were smokers, 13.5% had chronic illnesses, and 62.9% reported that they exercise. Fig. (1 and Table 2) represent PA levels among respondents; 35.8% were in the moderate PA group, 35.3% were in the low PA group, and 28.9% were in the high PA group.
| Item | N | % |
|---|---|---|
| Age (years) | ||
| 21 – 35 | 395 | 58.2 |
| 36 – 45 | 102 | 15.0 |
| >45 | 182 | 26.8 |
| BMI (kg/m2) | ||
| Mean ± SD | 27.8 ± 7.44 | |
| Gender | ||
| Male | 307 | 45.2 |
| Female | 372 | 54.8 |
| Governate | ||
| Kuwait City | 164 | 24.2 |
| Alahmadi | 72 | 10.6 |
| Farwaniya | 88 | 13.0 |
| Aljahra | 51 | 7.5 |
| Hawaly | 161 | 23.7 |
| Mubarak Alkabeer | 143 | 21.1 |
| Marital status | ||
| Married | 368 | 54.2 |
| Single | 279 | 41.1 |
| Other | 32 | 4.7 |
| Number of children | ||
| No children | 322 | 47.4 |
| 1 or 2 | 131 | 19.3 |
| 3 or 4 | 138 | 20.3 |
| More than 4 | 88 | 13.0 |
| Employment | ||
| Student | 120 | 17.7 |
| Employee | 473 | 69.7 |
| Retired | 44 | 6.5 |
| Other | 42 | 6.2 |
| Educational level | ||
| High school education or less | 43 | 6.3 |
| Diploma | 80 | 11.8 |
| Undergraduate | 426 | 62.7 |
| Doctoral and post-doctoral degree | 130 | 19.1 |
| Smoking | 148 | 21.8 |
| Chronic illness | 92 | 13.5 |
| Exercise | 427 | 62.9 |
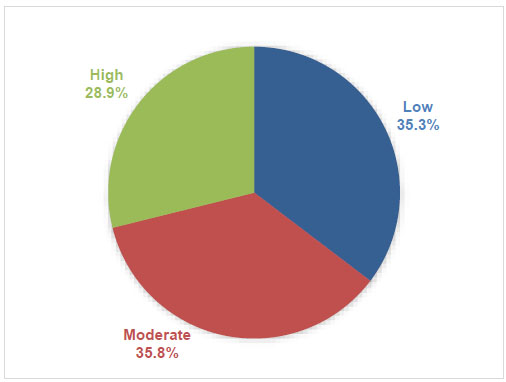
Distribution of respondents according to PA levels.
| Item | N | % | 95%CI |
|---|---|---|---|
| Physical Activity level | |||
| Low | 240 | 35.3 | 31.02 to 40.11 |
| Moderate | 243 | 35.8 | 31.43 to 40.58 |
| High | 196 | 28.9 | 24.97 to 33.2 |
| METs | |||
| Median (IQR) | 1308 (495, 2542.5) | ||
Our investigation revealed a statistically significant relationship between the age of respondents and their PA level (P=0.022), as respondents in the high PA category were significantly younger than those in the moderate PA category, with 65.3% of the first vs. 55.6% of the latter being in the 21–35 year range, 10.2% vs. 19.8% in the 36–45 range and 24.5% vs 24.7% over the age of 45 years. BMI significantly differed among groups (P=0.031), being significantly lower among participants with high PA levels than among those with low PA (26.9 ± 4.67 vs 28.75 ± 10.5 kg/m2). Additionally, exercise prevalence was 36.7% in the group with low PA levels, 64.2% in those with moderate PA, and 93.4% in those with high PA, showing a statistically significant difference among the three groups (P<0.001). Notably, 42.5% of the low PA group, 45.3% of the moderate PA group, and 48.5% of the high PA group were males, and these percentages were comparable among the groups (Table 3 and Figs. 2–4).
In univariate regression analysis, BMI, marital status, having chronic illnesses, and exercising were significantly associated with PA level according to the IPAQ-SF as follows: Each 1 unit increase in BMI resulted in a decrease in the odds of moderate or high PA levels by 3% (OR=0.97, 95%CI: 0.95 to 0.99, P=0.011). Single participants showed significantly higher odds of having moderate or high PA levels than married participants (OR=1.52, 95%CI: 1.14 to 2.02, P=0.005). As for chronic illnesses, participants suffering from them showed significantly lower odds of engaging in moderate or high PA than others (OR=0.6, 95%CI: 0.4 to 0.91, P=0.016). Further, participants who exercised showed significantly higher odds of having moderate or high PA levels than those who did not exercise (OR=7.13, 95%CI: 5.15 to 9.87, P<0.001).
After adjusting for the included factors, BMI, nationality, marital status, and number of children, and exercise were significantly associated with PA level as follows:
| Item | Physical Activity level | P-value | ||
|---|---|---|---|---|
|
Low (n=240) |
Moderate (n=243) |
High (n=196) |
||
| Age (years) | ||||
| 21 – 35 | 132 (55%) ab | 135 (55.6%) a | 128 (65.3%) b | 0.022 |
| 36 – 45 | 34 (14.2%) | 48 (19.8%) | 20 (10.2%) | |
| >45 | 74 (30.8%) | 60 (24.7%) | 48 (24.5%) | |
| BMI (kg/m2) | 28.75 ± 10.5 a | 27.6 ± 5.18 ab | 26.9 ± 4.67 b | 0.031 |
| Gender | ||||
| Male | 102 (42.5%) | 110 (45.3%) | 95 (48.5%) | 0.460 |
| Female | 138 (57.5%) | 133 (54.7%) | 101 (51.5%) | |
| Marital status | ||||
| Married | 146 (60.8%) | 129 (53.1%) | 93 (47.4%) | 0.076 |
| Single | 84 (35%) | 101 (41.6%) | 94 (48%) | |
| Other | 10 (4.2%) | 13 (5.3%) | 9 (4.6%) | |
| Number of children | ||||
| No children | 107 (44.6%) | 113 (46.5%) | 102 (52%) | 0.056 |
| 1 or 2 | 41 (17.1%) | 56 (23%) | 34 (17.3%) | |
| 3 or 4 | 57 (23.8%) | 38 (15.6%) | 43 (21.9%) | |
| More than 4 | 35 (14.6%) | 36 (14.8%) | 17 (8.7%) | |
| Employment | ||||
| Student | 45 (18.8%) | 38 (15.6%) | 37 (18.9%) | 0.342 |
| Employee | 168 (70%) | 166 (68.3%) | 139 (70.9%) | |
| Retired | 17 (7.1%) | 19 (7.8%) | 8 (4.1%) | |
| Other | 10 (4.2%) | 20 (8.2%) | 12 (6.1%) | |
| Educational level | ||||
| High school education or less | 17 (7.1%) | 16 (6.6%) | 10 (5.1%) | 0.360 |
| Diploma | 21 (8.8%) | 30 (12.3%) | 29 (14.8%) | |
| Undergraduate | 160 (66.7%) | 152 (62.6%) | 114 (58.2%) | |
| Doctoral and post-doctoral degree | 42 (17.5%) | 45 (18.5%) | 43 (21.9%) | |
| Smoking | 53 (22.1%) | 53 (21.8%) | 42 (21.4%) | 0.987 |
| Chronic illness | 42 (17.5%) | 31 (12.8%) | 19 (9.7%) | 0.055 |
| Exercise | 88 (36.7%) a | 156 (64.2%) b | 183 (93.4%) c | <0.001 |
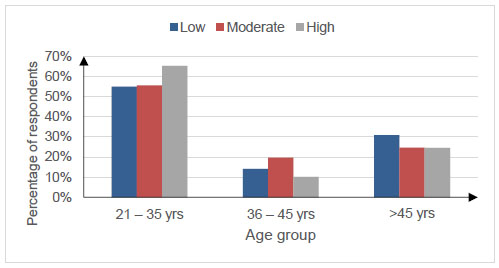
Comparison of age among the three Physical Activity groups.
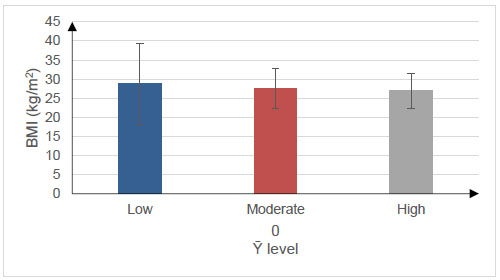
Comparison of BMI among the three Physical Activity groups.
Each 1 unit increase in BMI resulted in a decrease in the odds of having moderate or high PA levels by 0.97 (95%CI: 0.95 to 1, P=0.046). Single participants showed significantly higher odds of having moderate or high PA levels than married participants (OR=2.33, 95%CI: 1.19 to 4.58, P=0.014). Participants with one or two children elicited significantly higher odds of having moderate or high PA than those with no children (OR=2.07, 95%CI: 1.04 to 4.09, P=0.037). Furthermore, participants who exercised showed significantly higher odds of moderate or high PA levels than those who did not exercise (OR=7.18, 95%CI: 5.1 to 10.09, P<0.001) Table 4.
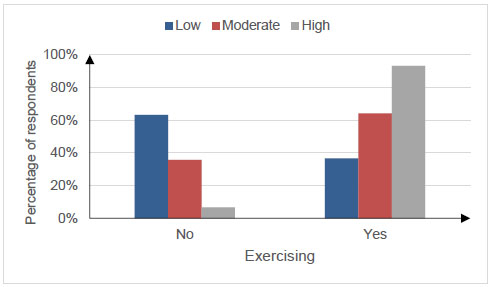
Comparison of exercising rate among the three Physical Activity groups.
| Item | Univariate analysis | Multivariable analysis | ||||
|---|---|---|---|---|---|---|
| Unadjusted OR | 95%CI | P-value | Adjusted OR | 95%CI | P-value | |
| Age (years) | ||||||
| 21 – 35 | Ref. | Ref. | ||||
| 36 – 45 | 0.76 | 0.52 to 1.13 | 0.177 | 0.88 | 0.55 to 1.39 | 0.574 |
| >45 | 0.73 | 0.53 to 1.01 | 0.061 | 1.17 | 0.71 to 1.91 | 0.538 |
| BMI (kg/m2) | 0.97 | 0.95 to 0.99 | 0.011 | 0.97 | 0.95 to 1 | 0.046 |
| Gender | ||||||
| Male | Ref. | Ref. | ||||
| Female | 0.84 | 0.63 to 1.11 | 0.214 | 0.85 | 0.59 to 1.21 | 0.363 |
| Marital status | ||||||
| Married | Ref. | Ref. | ||||
| Single | 1.52 | 1.14 to 2.02 | 0.005 | 2.33 | 1.19 to 4.58 | 0.014 |
| Other | 1.3 | 0.68 to 2.51 | 0.428 | 1.18 | 0.57 to 2.46 | 0.654 |
| Number of children | ||||||
| No children | Ref. | Ref. | ||||
| 1 or 2 | 0.92 | 0.64 to 1.33 | 0.665 | 2.07 | 1.04 to 4.09 | 0.037 |
| 3 or 4 | 0.81 | 0.55 to 1.18 | 0.267 | 1.72 | 0.82 to 3.59 | 0.151 |
| More than 4 | 0.66 | 0.43 to 1.01 | 0.057 | 1.42 | 0.63 to 3.19 | 0.400 |
| Employment | ||||||
| Student | Ref. | Ref. | ||||
| Employee | 1.02 | 0.7 to 1.48 | 0.931 | 1.11 | 0.69 to 1.8 | 0.656 |
| Retired | 0.75 | 0.4 to 1.41 | 0.369 | 1.05 | 0.45 to 2.43 | 0.913 |
| Other | 1.3 | 0.69 to 2.43 | 0.420 | 1.71 | 0.86 to 3.42 | 0.127 |
| Educational level | ||||||
| High school education or less | Ref. | Ref. | ||||
| Diploma | 1.82 | 0.92 to 3.6 | 0.084 | 0.85 | 0.4 to 1.78 | 0.662 |
| Undergraduate | 1.13 | 0.64 to 2.01 | 0.678 | 0.54 | 0.28 to 1.04 | 0.064 |
| Doctoral and post-doctoral degree | 1.48 | 0.78 to 2.79 | 0.229 | 0.7 | 0.34 to 1.44 | 0.335 |
| Smoking | 0.97 | 0.7 to 1.36 | 0.870 | 0.95 | 0.62 to 1.44 | 0.800 |
| Having a chronic illness | 0.6 | 0.4 to 0.91 | 0.016 | 0.95 | 0.6 to 1.5 | 0.813 |
| Exercising | 7.13 | 5.15 to 9.87 | <0.001 | 7.18 | 5.1 to 10.09 | <0.001 |
4. DISCUSSION
We sought to determine PA levels among adults during the COVID pandemic by using the IPAQ-SF. This is the first attempt to both quantify and categorize PA levels using the IPAQ-SF in Kuwait during the pandemic. The main findings of this study were twofold. First, there were no gender differences in PA levels during the pandemic in Kuwait. Secondly, age and BMI were contributing factors to PA levels. These findings indicate that promotion of PA levels in Kuwait is necessary for specific age groups during the pandemic, and multidimensional strategies should be pursued at the national level to increase levels of PA.
During the pandemic, unprecedented measures such as social distancing caused interruptions to the ‘normal’ daily activities. This was a global attempt to contain the virus and to limit its transmission. However, one of the strict social distancing measures, such as ‘lockdowns’ and quarantines, came at a huge cost [5]. People’s daily living, travel, education, and leisure were impacted and had an enormous effect on their daily PA levels [5]. Indeed, a recent systematic review found that PA levels were reduced during the pandemic, especially in countries with lockdowns [38]. This is important because PA can promote health and well-being, and Exercise can be prescribed as a therapy for various chronic diseases, highlighting its role as a subcategory of PA [39-41]. It is well established that weekly moderate-to-vigorous PA can reduce all-cause mortality [42-45]. Increased PA levels have been shown to provide immunity against viruses such as COVID-19 [16, 17, 24]. Frequent moderate-intensity PA reduces the incidence of respiratory tract infection by a value of 40-50% as reported elsewhere [19]. Moreover, individuals with chronic conditions such as diabetes and hypertension can benefit from exercising due to its positive immune effects, a conclusion supported by several studies [17, 46, 47]. Therefore, given the evidence on the benefits of PA levels, monitoring them at a national level is crucial for implementing policies to promote PA.
WHO suggested PA guidelines for the general population. The recommendation is that the minimum PA needed to have the benefits is engaging in a minimum of 150 minutes of moderate or 75 minutes of vigorous PA weekly [30]. Due to the pandemic restrictions and the ‘stay at home’ message that was disseminated during this period, vigorous activities such as running or playing soccer, which are very common in Kuwait, are not possible. However, other vigorous intensity physical activities can be performed at home, such as stair climbing or moving heavy loads, which can be considered as a vigorous PA at home [48]. In the present study, most participants engaged in regular physical activities. The results showed that 35.8% and 28.9% of the sample were in the moderate or high PA category, respectively, during the pandemic. These results are consistent with those of other studies that have assessed PA levels using the IPAQ-SF during the pandemic. Antunes, Frontini [49] and Maugeri, Castrogiovanni [50] found that the majority of participants recruited from Portugal and Italy belonged to the high and moderate categories of the IPAQ-SF. Maugeri, Castrogiovanni [50] investigated the impact of COVID on PA levels and whether it had psychological effects [50]. They found that most participants were in either the moderate (50%) or high (19%) PA category. They also reported that ~40% of their participants were in the low PA category. In the present study, 35% of the participants were in the low PA category, which is higher than the figure reported by Antunes, et al. [49] (32%), but lower than that reported by Maugeri, Castrogiovanni [50] (40%). Antunes, Frontini [49] explored PA levels during the pandemic. They also found that most participants had either moderate (30%) or vigorous PA (31%). Discrepancies in the results may be attributed to the level of restrictions that occurred during these different settings of the studies compared to Kuwait or other social and cultural factors. However, ~30-40% physical inactivity levels among studies can reveal that work needs to be done to curb the burden of inactivity.
The finding of low PA in our sample (35.3%) is consistent with concerns across the Gulf Cooperation Council (GCC) region regarding insufficient PA levels before the pandemic. A systematic review conducted before the pandemic revealed low levels of PA, particularly among women [51]. Furthermore, our findings during the COVID lockdown are also comparable to those of neighboring countries. A recent scoping review concluded that PA was reduced consistently across all ages and in both genders during the COVID lockdown period in Saudi Arabia [52]. Kuwait's response to the pandemic during June and July of 2020 included a 12-hour curfew (6 am-6 pm) and closure of non-essential business, where gyms and public outdoor areas were closed off, limiting PA engagement. In addition to extreme heat (>45°C daytime) during June and July making prolonged PA dangerous, especially for older adults, due to heat-related immunosuppression effects [53]. Nevertheless, the proportion of individuals maintaining moderate to high activity levels (64.7%) during the pandemic may indicate adoption of home exercise, a shift reinforced by a worldwide increase in digital fitness platforms and applications during the pandemic [54].
In the present study, no significant gender differences were found between males and females in Kuwait. This finding is interesting as it contrasts with studies conducted before the pandemic in Kuwait and the surrounding region. For example, a study on Kuwaiti adolescents found that males were significantly more physically active than females [55]. This is consistent with studies conducted in the region across the Arabian Peninsula, where a systematic review reported that males were significantly more active than females [51]. Several factors may have contributed to this finding. Pandemic restrictions limit access to sports venues such as soccer fields, where males were more often accessed before the pandemic. Traditionally, men are more likely to exercise in gyms, and societal norms make females more likely to engage in PA at home [56]. In addition, restrictions might have restricted females’ PA to segregated venues that they often accessed before the pandemic. Limited access to male sports outdoor venues may have reduced PA of males, and possibly females, increased activity levels at home, which might lead to convergence in overall PA levels. However, these explanations require further investigation.
Our study also showed that age was a contributing factor in PA levels in Kuwait during the pandemic. As expected, PA decreased as age increased in all participants. It is well known that as age increases, PA levels decrease [57, 58]. In an older study conducted in Saudi Arabia [59], a region close to Kuwait, PA levels decreased as age increased from 15-29 years old to 60-78 years old. The 15-29 years old group was 15% more active than the older group in the study 60-78-year-old group. Similarly, the largest age group with physical inactivity was the older group with 41%, compared to over 50% in the other study [59]. Therefore, as aging can play a role in PA levels, it is necessary to focus on these aging groups towards PA level participation and surveillance.
5. RECOMMENDATIONS AND POLICY IMPLICATIONS
Based on the findings of this study, we propose several recommendations and policy implications. First, public health efforts should focus on getting older adults (45+ years old) more active, especially during viral pandemics. This study indicated that this age group was at risk of not being active during the viral pandemics. In addition, public health messaging should encourage a wide range of home-based physical activities, using little or no equipment. This would ensure that individuals are active even during periods of lockdown and restrictions. Furthermore, Kuwait's policy makers should monitor trends in PA and evaluate national health interventions. Integrating the IPAQ-SF as a validated evaluation tool is important for achieving this goal.
6. STUDY LIMITATIONS
This study has several limitations regarding PA assessment. Although the IPAQ-SF is a validated tool to assess PA levels, it is subject to self-reporting biases, including an over-reporting bias and potential recall bias regarding PA levels during the previous 7 days. Therefore, future studies could incorporate accelerometers or wearable fitness trackers to support these findings. Second, recruitment was through an online survey that could have introduced a selection bias and may have over-represented individuals with more digital literacy and under-represented older adults and others who have less access to digital online platforms. However, recruitment through social media remains an efficient strategy [60, 61], and during lockdowns commuting is restricted; therefore, it is difficult to assess PA levels in any other means such as accelerometers or wearable fitness trackers. Furthermore, the IPAQ-SF can provide an acceptable estimate of PA levels, and its validity has been demonstrated and confirmed [33, 62, 63]. Another limitation in this study is the lack of a comparative analysis, which limits the generalizability of the findings to Kuwait. Also, the cross-sectional design of the study may identify relationships between variables, but it does not allow for inference of the causes of these relationships. For example, we detected a relationship between age and PA; however, it’s difficult to conclude that age causes reductions in PA according to the design of this study. Future studies should consider longitudinal studies to study the causes of reductions in PA during the pandemic and use these limitations and investigate how the pandemic affected PA levels using objective measures such as accelerometers.
CONCLUSION
In conclusion, the findings of this study provided a valuable snapshot of PA levels among adults in Kuwait during the COVID lockdown. This study indicated that older adults and adults with higher BMI were associated with lower PA; therefore, during viral pandemics, PA promotion strategies should focus on older adult age groups and those with higher BMI. These strategies can be implemented at the community level by establishing a social environment where older adults can engage and perform low-impact activities in collaboration with healthcare providers, such as physical therapists. Future studies should consider longitudinal studies to study the causes of reductions in PA during the pandemic and investigate PA levels using objective measures such as accelerometers.
AUTHORS' CONTRIBUTIONS
The authors confirm contribution to the paper as follows: Study conception and design; S.A., A.A., M.M.:, Analysis and interpretation of results; S.A., A.A, M.M., A.A.A., A.H.A., M.A., and N.A.; and A.S.H.: Draft Manuscript; S.A., A.A., M.M., A.A.A., A.H.A., M.A., and N.A.; and A.S.H.:, Given final approval of the version to be published;. All authors reviewed the results and approved the final version of the manuscript S.A., A.A., M.M., A.A.A., A.H.A., M.A., and N.A.; and A.S.H.
LIST OF ABBREVIATIONS
| ANOVA | = Analysis of Variance |
| BMI | = Body Mass Index |
| CI | = Confidence Interval |
| COVID | = Coronavirus Disease |
| GCC | = Gulf Cooperation Council |
| IPAQ-SF | = International Physical Activity Questionnaire Short Form |
| METs | = Metabolic Equivalents |
| OR | = Odds Ratio |
| PA | = Physical Activity |
| WHO | = World Health Organization |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was approved by the Medical and Health Ethics Committee of the Ministry of Health in Kuwait (2020/1501).
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were under the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Electronic informed consent was obtained from all subjects involved in the study.
AVAILABILITY OF DATA AND MATERIALS
The data presented in this study are available on request from the corresponding author [S.A].
ACKNOWLEDGEMENTS
We extend our heartfelt thanks to all the participants whose invaluable contributions made this study possible.

