All published articles of this journal are available on ScienceDirect.

Navigating the 2022 Physician Workforce Dynamics in Saudi Arabia: A Study of Regional Distribution
Abstract
Introduction
Saudi Arabia’s Vision 2030 aims for comprehensive healthcare coverage and the nationalization of its workforce. However, physician distribution and composition disparities threaten these goals, negatively impacting access to and quality of healthcare services.
This study examines physician-to-population ratios and workforce composition across 20 Saudi Arabian health regions, guided by the research question: What are the disparities in physician distribution and workforce composition across regions, and how might these affect healthcare service equity and Saudization efforts?
Methods
A secondary analysis utilized the Ministry of Health’s 2022 Statistical Yearbook. Physician distribution and composition were explored using descriptive statistics, the Gini Coefficient, and a Lorenz curve.
Results
Findings reveal significant imbalances. While Riyadh, the capital region, hosts the largest number of physicians (20,385 physicians), its large population yields a lower physician-to-population ratio (2.5 per 1,000 persons), reflecting significant challenges in service provision. Al-Jouf and Northern regions exhibit higher ratios (4.5 and 4.2 per 1,000, respectively), indicating a better balance. Non-Saudi physicians remain prominent, especially in Bishah and Najran (92.5% in Bishah and 88.6% in Najran), suggesting a need for stronger Saudization policies. While there are no exact figures on the countries from which these physicians originate, estimates indicate that they mainly come from countries such as Egypt, Sudan, India, and Pakistan, reflecting long-standing recruitment patterns within the Gulf region.
Discussion
Significant regional disparities exist in the distribution of the physician workforce across Saudi Arabia, with a notable reliance on foreign physicians. Addressing these inequalities through Saudization and targeted policies is crucial for improving healthcare access, ensuring equitable resource allocation, and achieving sustainable workforce development nationwide.
Conclusion
These findings highlight significant disparities in the distribution of Saudi Arabia’s healthcare workforce, which can hinder the achievement of Vision 2030 goals. To address these imbalances, the study recommends specific measures, including expanding regional healthcare clusters, implementing targeted workforce incentives, increasing training capacity for Saudi physicians, and prioritizing underserved regions in national workforce planning. These actions are critical to reducing reliance on foreign physicians, promoting equitable access to care, and aligning service demand with a sustainable supply of qualified professionals across all regions.
1. INTRODUCTION
Saudi Arabia's healthcare sector is undergoing a significant transformation, driven by Vision 2030's goal of achieving comprehensive healthcare coverage and nationalizing the workforce [1-3]. The distribution and composition of the healthcare workforce are central to this transformation, as they significantly impact access, quality, and sustainability [4]. This paper examines the distribution of physicians across 20 Saudi Arabian health regions, highlighting disparities in physician-to-population ratios, workforce composition, and geographical imbalances [5]. The findings contribute to Vision 2030 by informing strategies to expand healthcare access, recruit and retain Saudi physicians, and address geographical disparities through educational reforms, strategic interventions, and workforce development programs [6]. Despite previous reports identifying healthcare workforce shortages in Saudi Arabia [7–10], few studies have examined regional physician distribution using national-level population-adjusted ratios or explored nationalization trends by region. This study addresses that gap by providing a comparative analysis of the distribution of Saudi and non-Saudi physicians across all 20 health regions.
This introduction focuses on four key areas: workforce enhancement under Vision 2030, reliance on foreign physicians, geographical disparities in physician distribution, and regional imbalances in the distribution of physicians in Saudi Arabia.
1.1. KSA Vision 2030 and Enhancing the Physicians’ Workforce
Saudi Arabia’s Vision 2030 aims to transform the kingdom into a diversified, knowledge-based economy with high-quality services and an empowered citizenry [3,11,12]. The health sector transformation is a central pillar of this plan, focusing on preventive care, improved access, efficient service delivery, and nationalization of the workforce. These objectives are supported by various health initiatives, including institutional restructuring and human capital development, to ensure the sustainability of the healthcare system.
Vision 2030 focuses on enhancing its workforce and improving healthcare services [12, 13]. One key aim is to increase life expectancy from 75 years in 2016 to 80 years by 2030, necessitating a substantial expansion of healthcare services [3, 14]. Saudi Arabia's growing and aging population, along with the need for improved health outcomes, underscores the importance of strategic workforce planning [15]. The current disparity between the supply and demand of healthcare professionals underscores the need for reforms to increase the number of trained professionals. Efforts in recent decades have increased the number of physicians; however, a shortage persists, particularly among Saudi nationals [16]. Further measures are needed to address current and projected shortages, with projections indicating an urgent need for reforms to human resource planning and education [17].
To achieve Vision 2030's goals, Saudi Arabia needs to strategically develop its healthcare workforce, both regionally and nationally. This involves expanding healthcare facilities and services to meet the rising demand [18]. The anticipated increase in the Saudi population and the evolving health profile require an equitable distribution of physicians across the kingdom. Therefore, Vision 2030 emphasizes the expansion of healthcare facilities, necessitating an increase in the number of healthcare professionals across all regions. This expansion must also address disparities to ensure comprehensive healthcare services [19]. The growing healthcare demand and the existing workforce shortage necessitate a multifaceted approach to workforce development, including educational initiatives, strategic resource deployment, and recruiting Saudi physicians to fill the gaps and create a balanced regional healthcare system.
1.2. Saudi Dependence on Foreign Physicians and the Retention of Saudi Nationals
Saudi Arabia has historically relied heavily on foreign physicians to staff its healthcare system, with Saudi nationals making up only a minority of the physician workforce [20]. As of 2014, Saudi physicians constituted just 37.89% of the total physician workforce, highlighting a significant reliance on expatriate medical professionals [21]. This dependency has led to challenges, particularly in maintaining a uniform standard of care and ensuring accessible service across the kingdom. Vision 2030 addresses this imbalance by prioritizing strategic human resource development initiatives focusing on training, employing, and retaining Saudi nationals in the healthcare sector [22].
The Saudi government has implemented various policies to increase the recruitment and retention of Saudi physicians, including the Saudization policy, a national workforce localization initiative aimed at improving the proportion of Saudi nationals employed in key sectors, including healthcare, which seeks to increase the proportion of Saudi healthcare professionals from one-third to two-thirds by 2030 [6]. These efforts are part of a broader strategy to reduce reliance on foreign workers and improve the sustainability of the healthcare workforce. However, challenges still need to be addressed, including a mismatch between the healthcare demands of the growing Saudi population and the number of trained Saudi professionals available to meet these needs. To address these issues, there is a need for comprehensive strategies to support the nationalization of the healthcare workforce, including educational reforms, career development opportunities, and incentives to retain Saudi nationals in the healthcare sector [4, 23].
1.3. Geographical Disparities in Physicians’ Distribution
Saudi Arabia's healthcare system has made significant strides in expanding healthcare services, but geographical disparities in the distribution of physicians persist. These disparities are particularly evident between urban and rural areas, with urban centres such as Riyadh and Jeddah attracting more healthcare professionals due to better resources and infrastructure [4]. Rural and underserved regions, on the other hand, face a shortage of medical professionals, leading to limited healthcare services and accessibility issues. This uneven distribution not only affects access to healthcare but also impacts the quality of care, with urban areas generally benefiting from more comprehensive services and modern medical technologies. At the same time, rural regions may struggle with outdated facilities and limited medical services [4, 24]. As shown in Table 1, the 2021 physician-to-population ratio of 2.8 per 1,000 people in Saudi Arabia is notably lower than that of other high-income countries such as Sweden (7.1), the European Union (4.3), and the OECD (Organisation for Economic Cooperation and Development) average (3.4), underscoring the need for a balanced distribution [25].
1.4. Data Reflects the Most Recent Available Year, with the World Average as of 2019 being 1.7
To address these disparities, Vision 2030 and the Health Sector Transformation Plan emphasize strategic interventions to redistribute healthcare services and ensure equitable access across all regions [13]. This includes expanding regional health clusters to enhance the capacity and distribution of healthcare services, as well as aligning healthcare resources with the needs of each region's population [13]. Additionally, international collaboration and effective policy strategies are necessary to address the mismatch between the supply and demand for healthcare workers, ensuring equitable distribution and comprehensive healthcare coverage throughout Saudi Arabia [26].
1.5. Geographical Disparities in Saudi Physicians’ Distribution
The distribution of Saudi physicians across the kingdom remains uneven, with a significant concentration in urban areas such as Riyadh and Jeddah [4]. This imbalance is attributed to various factors, including better career opportunities, access to resources, and improved infrastructure in urban centres. In contrast, rural and underserved regions face challenges in attracting and retaining Saudi healthcare professionals, resulting in disparities in healthcare service availability and quality. This imbalance is compounded by the region-wide physician-to-population ratio of 1.5 per 1,000 in the Middle East and North Africa, emphasizing the need for comprehensive distribution policies [25]. These geographical disparities impact healthcare access and the uniformity of services provided to different communities [27].
To address these disparities, Vision 2030 emphasizes strategic interventions to redistribute healthcare resources and improve service availability nationwide [13, 14]. This includes policy measures to incentivize Saudi physicians to work in rural and underserved regions, as well as improving infrastructure and providing training and career development opportunities [17]. These efforts aim to increase the representation of Saudi physicians in the healthcare workforce and ensure an equitable distribution, aligning with Saudi Arabia's broader goals of nationalizing the workforce and meeting the healthcare needs of its population.
This paper examines the geographical distribution of physicians across Saudi Arabia, focusing on both the overall distribution and the specific distribution of Saudi nationals within the healthcare workforce. The paper examines the disparities between urban and rural regions, the impact of physician distribution on healthcare quality and access, and the challenges associated with retaining and attracting Saudi nationals in the healthcare sector.
By analysing 2022 data, this paper offers a unique contribution, as no previous studies have examined the geographical distribution of Saudi and non-Saudi physicians. It identifies the reliance on foreign physicians, geographical disparities in physician distribution, and the existing challenges in nationalizing the healthcare workforce. The paper offers insights into healthcare service inequalities and proposes strategic interventions to address these disparities. Ultimately, it aims to contribute to achieving Vision 2030 goals by providing policy recommendations to enhance the distribution and retention of physicians, both nationally and regionally, ensuring equitable healthcare access across Saudi Arabia.
| Country | Physicians-to-1,000-person | Most Recent Year |
|---|---|---|
| Sweden | 7.1 | 2020 |
| European Union | 4.3 | 2019 |
| USA | 3.6 | 2020 |
| High Income | 3.6 | 2019 |
| OECD | 3.4 | 2019 |
| UK | 3.2 | 2021 |
| Saudi Arabia | 2.8 | 2021 |
| China | 2.4 | 2020 |
| Middle East and North Africa | 1.5 | 2019 |
| Middle-income countries | 1.4 | 2019 |
| Low income | 0.4 | 2019 |
2. METHODS
This study conducts a secondary analysis of physician workforce data in Saudi Arabia, utilizing data from the Ministry of Health (MOH) 2022 Statistical Yearbook, corresponding to the Islamic year 1442 AH [5]. The inclusion criteria for the study were all licensed physicians registered under the Ministry of Health in Saudi Arabia in 2022 with an assigned region in the official workforce dataset. Physician-to-population ratios were calculated for each health region by dividing the number of physicians by the population size and multiplying by 1,000 to obtain a standardized ratio of physicians per 1,000 residents. The 2022 Yearbook reported a total physician workforce of 105,332 across MOH hospitals, private hospitals, primary care centres, MOH headquarters, and other governmental hospitals. After excluding records of physicians without defined regions of employment (MOH headquarters and other governmental hospitals), the final sample used in the regional analysis consisted of 85,240 physicians, representing approximately 81% of the original workforce reported by the MOH. This exclusion was necessary to ensure valid regional comparisons. Still, it may introduce bias by omitting physicians who potentially serve multiple regions or hold administrative and tertiary roles at the national level. The data analysis involved descriptive statistics, including the Gini Coefficient and the Lorenz curve, which are widely used tools to assess inequality in resource distribution. These methods were chosen because they provide a robust quantitative and visual assessment of inequality across multiple regions, allowing us to capture both the magnitude and structure of disparities in physician allocation. The Gini coefficient provides a standardized metric for measuring inequality, while the Lorenz curve visually illustrates the cumulative distribution of physicians relative to the population. This inequality is captured by the Gini coefficient, where a value closer to 0 reflects a more equal distribution, and a value closer to 1 indicates greater inequality. Lastly, a comprehensive analysis was conducted to compare the geographical distribution of physicians between Saudi and non-Saudi nationals. Because the data represent a complete national census rather than a sample, inferential statistics (e.g., p-values, confidence intervals) were not computed; the results instead rely on population-level descriptive metrics.
3. RESULTS
The study examines the distribution of physicians across Saudi Arabia's 20 health regions, revealing disparities in physician-to-population ratios, regional distribution, and workforce composition. This comprehensive analysis offers valuable insights into the alignment between healthcare resources and population needs, revealing significant disparities across the kingdom. The following sections provide a detailed examination of these findings, exploring variations in physician-to-population ratios, regional inequality, and the distribution of Saudi and non-Saudi physicians.
3.1. Physician-to-Population Ratios Across Saudi Arabia
This study presents the distribution of physicians across Saudi Arabia's 20 health regions, focusing on the total number of physicians, population sizes, and the physician-to-population ratio of 1,000 persons. These ratios provide insight into regional disparities in healthcare access and the availability of medical services. The data in Table 2 highlights significant variations in physician distribution, revealing key areas where strategic workforce planning is needed to ensure equitable healthcare coverage across the kingdom.
3.2. Regions Ranked by the Physicians-to-1,000-person Value
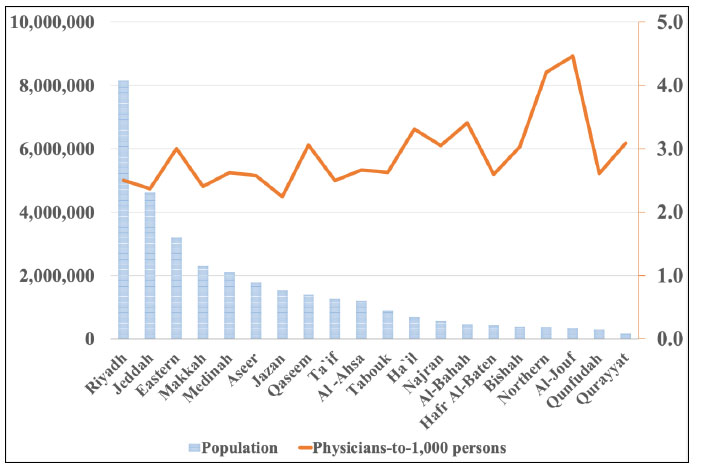
The number of physicians varies significantly across regions, ranging from 512 in Qurayyat to 20,385 in Riyadh. Riyadh, Jeddah, and the Eastern region have the highest numbers of physicians, each exceeding 9,000, reflecting the concentration of healthcare services in urban centres. In contrast, rural regions such as Qurayyat, Al-Bahah, and Hafr Al-Baten each have fewer than 1,600 physicians, demonstrating significant imbalances in healthcare staffing.
Population sizes also show substantial variation. Riyadh is the most populous region, with over 8 million residents, followed by Jeddah and the Eastern region, which have 4.6 million and 3.2 million residents, respectively. Smaller regions, such as Qurayyat, Al-Jouf, and Northern, have populations below 500,000, indicating a significant demographic gap between urban and rural areas. These findings highlight structural imbalances between service demand and workforce availability, particularly in high-density urban centers like Riyadh, where service provision may be overstretched despite the presence of a large number of physicians.
By dividing the number of physicians by the population size and multiplying by 1,000, the physician-to-1,000-person ratio provides a standardized measure of physician distribution. Al-Jouf leads with a ratio of 4.5, followed by Northern at 4.2 and Al-Bahah at 3.4, demonstrating a higher physician density in these regions. Conversely, Jazan has the lowest ratio at 2.2, while Riyadh, Ta'if, Jeddah, and Makkah also have ratios below the national average of 2.9, suggesting potential disparities in healthcare availability.
As demonstrated in Fig. (1), it visually compares the population sizes and physician-to-1,000-person ratios across the 20 health regions of Saudi Arabia. It reveals wide disparities between regions, with some urban centres having larger populations and lower physician-to-population ratios, despite having higher overall numbers of physicians. This visual representation highlights the imbalance between healthcare resources and population needs, underscoring the necessity for strategic interventions to ensure an adequate supply of physicians and an equitable distribution, particularly in underserved regions.
| Region | Physicians | Population | Physicians-to-1,000-person |
|---|---|---|---|
| Al-Jouf | 1,486 | 333,189 | 4.5 |
| Northern | 1,509 | 358,989 | 4.2 |
| Al-Bahah | 1,588 | 465,779 | 3.4 |
| Ha`il | 2,269 | 685,571 | 3.3 |
| Qurayyat | 512 | 165,804 | 3.1 |
| Qaseem | 4,275 | 1,397,187 | 3.1 |
| Najran | 1,740 | 570,698 | 3 |
| Bishah | 1,154 | 380,622 | 3 |
| Eastern | 9,627 | 3,202,857 | 3 |
| Al-Ahsa | 3,197 | 1,199,375 | 2.7 |
| Tabouk | 2,340 | 889,914 | 2.6 |
| Medinah | 5,527 | 2,105,376 | 2.6 |
| Qunfudah | 789 | 302,597 | 2.6 |
| Hafr Al-Baten | 1,136 | 437,822 | 2.6 |
| Aseer | 4,591 | 1,782,856 | 2.6 |
| Riyadh | 20,385 | 8,153,488 | 2.5 |
| Ta`if | 3,184 | 1,275,200 | 2.5 |
| Makkah | 5,551 | 2,308,801 | 2.4 |
| Jeddah | 10,940 | 4,623,940 | 2.4 |
| Jazan | 3,440 | 1,535,152 | 2.2 |
| Total | 85,240 | 32,175,220 | - |
| Mean | 4,262 | 1,608,761 | 2.9 |
Population sizes and physician-to-1,000-person ratios across Saudi Arabia's health regions.
Source: Authors’ analysis based on data from the Saudi Ministry of Health Statistical Yearbook 2022
3.3. Gini Coefficient and Lorenz Curve
The Gini Coefficient provides a quantitative measure of the inequality in the distribution of physicians across Saudi Arabia's health regions. A Gini coefficient of 0.491 indicates a moderate disparity across the total physician workforce, with greater inequality in the distribution of Saudi physicians, as evidenced by a value of 0.612 concentrated in specific regions. These values suggest that despite national policies, physician access remains inequitable, particularly for populations in the underserved areas, potentially resulting in longer wait times, overburdened providers, and unequal health outcomes.
A lower coefficient of 0.434 implies a more balanced distribution among non-Saudi physicians. These coefficients reflect significant disparities in physician distribution across the kingdom. The higher Gini coefficient for Saudi physicians suggests substantial inequality in their distribution, indicating a need for targeted strategic interventions to address these imbalances. The lower Gini coefficient for non-Saudi physicians suggests a more balanced distribution, while the overall Gini coefficient of 0.491 represents moderate inequality across the entire physician workforce.
An acceptable level of inequality in physician distribution is generally considered to be associated with a Gini coefficient below 0.5, as lower Gini values are linked to improved access to healthcare. To ensure equitable physician coverage across all regions of Saudi Arabia, policymakers should prioritize strategies that address and reduce the disparity between Saudi and non-Saudi physicians.
The Lorenz Curve, shown in Fig. (2), further visualizes these disparities, illustrating the cumulative share of physicians relative to the cumulative share of regions. This highlights the need for policies to address regional disparities and ensure equitable access to healthcare across Saudi Arabia.
3.4. Saudi and Non-Saudi Physician Distribution Across Saudi Arabia
This section presents the distribution of Saudi and non-Saudi physicians across Saudi Arabia's 20 regions, revealing significant disparities in nationalization within the healthcare sector. Table 3 highlights the total number of Saudi and non-Saudi physicians, the percentage of non-Saudi physicians, and the proportion of Saudi physicians in each region.
| Region | Total Saudi Physicians | Total Non-Saudi Physicians | Total | % of Non-Saudi Physicians | % of Saudi Physicians |
|---|---|---|---|---|---|
| Bishah | 87 | 1,067 | 1,154 | 92.50% | 7.50% |
| Najran | 198 | 1,542 | 1,740 | 88.60% | 11.40% |
| Hafr Al-Baten | 132 | 1,004 | 1,136 | 88.40% | 11.60% |
| Qurayyat | 79 | 433 | 512 | 84.60% | 15.40% |
| Qunfudah | 125 | 664 | 789 | 84.20% | 15.80% |
| Ha'il | 380 | 1,889 | 2,269 | 83.30% | 16.70% |
| Tabouk | 420 | 1,920 | 2,340 | 82.10% | 17.90% |
| Al-Bahah | 312 | 1,276 | 1,588 | 80.40% | 19.60% |
| Northern | 297 | 1,212 | 1,509 | 80.30% | 19.70% |
| Al-Jouf | 326 | 1,160 | 1,486 | 78.10% | 21.90% |
| Qaseem | 1,032 | 3,243 | 4,275 | 75.90% | 24.10% |
| Jazan | 980 | 2,460 | 3,440 | 71.50% | 28.50% |
| Ta'if | 968 | 2,216 | 3,184 | 69.60% | 30.40% |
| Riyadh | 7,393 | 12,992 | 20,385 | 63.70% | 36.30% |
| Aseer | 1,668 | 2,923 | 4,591 | 63.70% | 36.30% |
| Medinah | 2,011 | 3,516 | 5,527 | 63.60% | 36.40% |
| Jeddah | 5,116 | 5,824 | 10,940 | 53.20% | 46.80% |
| Eastern | 4,655 | 4,972 | 9,627 | 51.60% | 48.40% |
| Al-Ahsa | 1,676 | 1,521 | 3,197 | 47.60% | 52.40% |
| Makkah | 3,111 | 2,440 | 5,551 | 44.00% | 56.00% |
| TOTAL/ AVG | 30,966 | 54,274 | 85,240 | 63.70% | 36.30% |
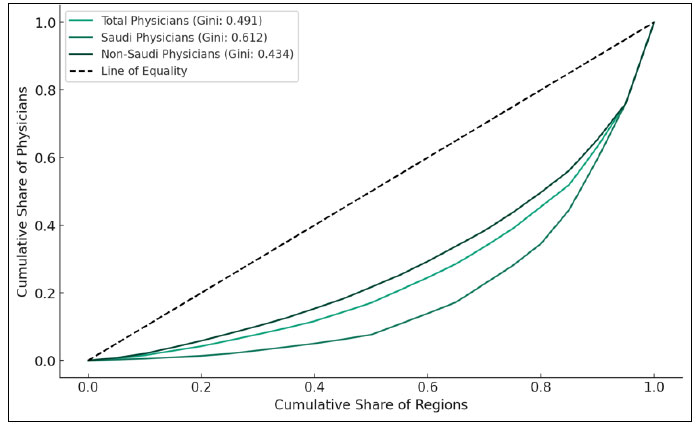
Lorenz curve for physicians-to-1,000-person ratio in Saudi Arabia.
Source: Authors’ analysis based on data from the Saudi Ministry of Health Statistical Yearbook 2022.
3.5. Regions Ranked by the Percentage of Saudi Physicians
The data in Table 3 reveal a diverse range of Saudi and non-Saudi physician distributions across the kingdom. Regions such as Bishah and Najran have high percentages of non-Saudi physicians, at 92.5% and 88.6%, respectively, indicating a significant reliance on foreign healthcare professionals in these areas. In contrast, Makkah and Al-Ahsa have higher percentages of Saudi physicians at 56% and 52.4%, respectively, suggesting a more balanced nationalization of the healthcare workforce in these regions.
While some regions, such as Riyadh, show a relatively balanced distribution between Saudi and non-Saudi physicians, others exhibit disparities. For instance, Bishah, Najran, and Hafr Al-Baten rely heavily on non-Saudi physicians, with less than 20% of their workforce being Saudi nationals. The concentration of non-Saudi physicians in several regions not only highlights the uneven progress of Saudization but also raises questions about the long-term sustainability and resilience of the workforce.
The Lorenz curves shown in Fig. (2) and corresponding Gini coefficients comprehensively represent the distribution of physicians within Saudi Arabia, indicating notable disparities across regions. With a Gini coefficient of 0.612, the distribution of Saudi physicians displays significant inequality, underscoring the challenges of inequitable access to healthcare services among local populations. Conversely, non-Saudi physicians exhibit a lower level of inequality, with a Gini coefficient of 0.434, suggesting a more uniform distribution across regions. Positioned between these extremes, the total distribution of physicians registers a Gini coefficient of 0.491, indicating a moderate but discernible imbalance in the accessibility of healthcare professionals nationwide.
4. DISCUSSION
The discussion explores key findings regarding the distribution of physicians across Saudi Arabia's health regions, identifying disparities in workforce composition, physician-to-population ratios, and regional healthcare access. This comprehensive analysis reveals significant disparities in the alignment between healthcare resources and population needs, underscoring the reliance on foreign physicians and the necessity for Saudization policies to balance the workforce. The discussion explores specific aspects of these disparities, examining the challenges and strategies for achieving comprehensive healthcare coverage and sustainable workforce development across Saudi Arabia.
4.1. Disparities in Physician Distribution
The analysis reveals notable disparities in physician distribution across Saudi Arabia's regions. Despite hosting the highest number of physicians, Riyadh exhibits a lower physician-to-population ratio due to its large population, indicating challenges in healthcare service provision in densely populated areas [28]. In contrast, regions like Al-Jouf and Northern, with higher physician-to-population ratios, reflect a better balance between the healthcare workforce and population needs. Nevertheless, these findings highlight disparities among rural areas, underscoring the need for the development of strategic policies to ensure comprehensive healthcare coverage throughout the kingdom [9]. These disparities align with earlier assessments of workforce maldistribution in the kingdom [4], and reinforce projections that existing gaps may widen without targeted interventions [27,9].
Saudi Arabia's reliance on foreign physicians exacerbates these challenges, particularly in regions where non-Saudi physicians comprise a significant portion of the workforce. For instance, regions such as Bishah and Najran rely heavily on expatriate medical professionals, underscoring the need for robust nationalization strategies [21]. Strategic initiatives to increase the recruitment and retention of Saudi physicians are crucial to achieving a balanced workforce, reducing dependency on expatriate health workers, and ensuring equitable healthcare coverage [23, 29].
The Saudization policy seeks to increase the proportion of Saudi healthcare professionals, integrating them into the national workforce for economic and social purposes [23]. This policy, alongside other initiatives such as educational reforms and private sector cooperation, aims to create a balanced healthcare workforce, improving sustainability and reducing unemployment among Saudi nationals. However, dual practice trends, where physicians work in both the public and private sectors, complicate the distribution of healthcare services, exacerbating regional disparities [29]. Thus, a comprehensive approach is essential to address these challenges effectively, ensuring reforms support both immediate needs and long-term goals [19].
The regional distribution of educational institutions is a significant factor influencing the geographical distribution of physicians. This distribution influences the availability of medical education and training facilities, affecting where physicians can practice and reside [28]. Additionally, incentives to encourage Saudi nationals to work in underserved areas, improvements in infrastructure, and professional development opportunities are essential to mitigate disparities [30].
4.2. Policy Implications
Addressing disparities in Saudi Arabia's healthcare workforce requires a multifaceted approach, including strategic interventions to redistribute resources and ensure equitable access to healthcare services [3, 12, 13]. This approach must encompass expanding regional health clusters to enhance healthcare capacity and align resources with the needs of the regional population [13]. For example, expanding medical colleges and residency programs in underserved regions can lead to improved long-term retention of physicians. Regional clusters can also benefit from decentralized recruitment authority, enabling them to respond more effectively to local shortages. Additionally, robust nationalization strategies, comprehensive workforce development programs, and holistic policies are crucial for reducing reliance on expatriate physicians and ensuring sustainable, balanced healthcare coverage [13, 14, 31]. Saudization efforts should be guided by clear benchmarks and supported with incentives such as housing allowances, performance-based advancement, and scholarships tied to service in remote areas [17].
As part of Vision 2030, the Saudi government has launched initiatives such as the Health Sector Transformation Program, the expansion of medical education seats for Saudi students, and structured Saudization plans with defined workforce localization targets [3,12–14]. These efforts aim to reduce dependency on foreign professionals while ensuring regional coverage.
The Saudi government has initiated strategic human resource development initiatives under Vision 2030, prioritizing the training, employment, and retention of Saudi nationals in the healthcare sector [6]. However, the study highlights the need for comprehensive reforms in healthcare workforce planning and to address the gap between demand and supply, principally as the population grows and ages [17, 19]. This mismatch necessitates immediate action, including expanding medical education programs, enhancing training facilities, and developing incentives to attract Saudi professionals into the healthcare sector.
To strengthen workforce development, comprehensive programs should include mentorship and career progression opportunities to retain Saudi physicians while expanding regional healthcare clusters and aligning resources with population needs [13]. This multifaceted approach aims to balance the growing demand for healthcare services with a sustainable supply of qualified professionals, thereby contributing to Saudi Arabia's broader goals of nationalizing its workforce and ensuring comprehensive access to healthcare. Additionally, promoting the equitable distribution of physicians across regions supports national priorities of balanced development and inclusive access to healthcare. These efforts strengthen social stability by ensuring that all citizens, regardless of location, can access essential medical services, in line with the values embedded in Vision 2030.
5. LIMITATIONS AND RECOMMENDATIONS
The study has potential limitations. First, the data used were derived from the Ministry of Health (MOH) based solely on 2022. Therefore, the findings represent a cross-sectional snapshot that may not capture temporal fluctuations or long-term workforce trends. Second, Physicians whose locations were not regionally defined and who work at the MOH headquarters or other governmental hospitals were excluded. As a result, the analysis may not fully represent the national distribution and characteristics of all physicians in the Kingdom of Saudi Arabia.
To enhance the comprehensiveness of future research, it is recommended that a unified national database be developed to encompass all physicians across all health sectors, including those working at the MOH headquarters and other governmental institutions. Establishing such an integrated system would enable more inclusive and representative analyses of the national healthcare workforce. Furthermore, adopting a longitudinal design to track physician movements, distribution, and retention patterns over time would provide valuable insights into workforce dynamics, supporting evidence-based planning and policy development. Furthermore, a more comprehensive analysis of regional factors, including the availability of healthcare facilities, socioeconomic status, and population health needs, should be conducted to gain a deeper understanding of the underlying determinants of physician distribution and healthcare accessibility across regions.
CONCLUSION
This study reveals marked disparities in physician distribution across Saudi Arabia’s regions, with urban centers, such as Riyadh, experiencing pressure despite having a high number of physicians. At the same time, underserved areas continue to face shortages. A persistent reliance on non-Saudi physicians further underscores the need for targeted Saudization policies and equitable allocation of resources. These conclusions should be viewed in light of limitations, including the use of a single-year dataset and the exclusion of physicians without defined regional assignments. To address these challenges, workforce planning must align with national goals by strengthening regional capacity, supporting Saudi recruitment, and tailoring interventions to local needs. Future research should investigate longitudinal trends in the workforce and examine factors influencing physicians’ regional preferences, particularly in underserved areas. Advancing evidence-based planning is crucial for promoting equity, maintaining access to healthcare, and achieving the objectives of Vision 2030.
AUTHORS’ CONTRIBUTIONS
The authors confirm contribution to the paper as follows: W.K.: Conceptualized the study, designed the methodology, analysed and interpreted the data, and wrote the original draft and revisions of the manuscript; A.A.: Provided feedback and oversight to enhance the manuscript and validated the accuracy and quality of the findings; All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| OECD | = Organisation for Economic Cooperation and Development |
| MOH | = Ministry of Health |
ETHICAL STATEMENT
Ethical approval and consent were not required for this study, as it was based on publicly available data.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article are available in the Saudi Ministry of Health Statistical Yearbook repository at https://www.moh.gov.sa/en/Minis try/Statistics/book/Pages/default.aspx, reference number MOH-2022-Statistical-Yearbook.
FUNDING
This study was funded by Deanship of Scientific Research (DSR) at King Abdulaziz University, Jeddah, Saudi Arabia (Awards/Grant number: IPP: 33-120-2025).
ACKNOWLEDGEMENTS
We extend our gratitude to the Ministry of Health in Saudi Arabia for their support and for making the data from 2022 and previous years publicly available on their website. This contribution was invaluable to this research.

