All published articles of this journal are available on ScienceDirect.

Strategies for Implementing Birth Companion Support During Labour: A Scoping Review
Authors Info & Affiliations
Abstract
Background
Birth companion support has been globally recognised as an essential component of childbirth care for decades. The benefits of birth companion support care include providing the pregnant woman with continuous emotional and physical support, thereby promoting positive childbirth experiences. Despite the numerous benefits of birth companion support care and the availability of policies to support this intervention, its implementation remains challenging.
Objectives
This study aimed to “map the evidence” and “identify gaps” in implementation strategies for birth companion support.
Methods
This scoping review adhered to the framework developed by Arksey and O'Malley, which comprised (i) developing the research question, (ii) identifying applicable studies, (iii) choosing studies, (iv) charting data, and (v) compiling, summarizing, and reporting findings. The databases utilized were PubMed, ProQuest, Scopus, and Web of Science. The findings of the review were analysed using thematic analysis.
Results
This scoping review encompassed 14 studies, and the results were divided into two main sections. Section A included identified implementation strategies covering the following themes: Models for implementing birth companion support, Development of programs for implementing birth companion support, and Task shifting. Section B entailed factors affecting the implementation of birth companion support, which are facilitators and barriers to the implementation of birth companion support.
Discussion
Continuous in-service training and workshops given to the target groups of health care professionals on the benefits of birth companion care and the roles of the companions will raise awareness and guarantee the implementation of birth companion support care during labour and childbirth. The significance of this practice lies in its ability to enhance a positive childbirth experience, which is essential for high-quality care.
Conclusion
The evaluated studies were conducted in nations with high, moderate, and low incomes. There was less evidence of a birth companion care implementation study conducted in South Africa. The findings of this study will assist in creating awareness and readiness for implementing birth companion support care in clinical practice.
1. INTRODUCTION
Policies on birth companion support are available, and the World Health Organization (WHO) [1] has recommended the worldwide practice of birth companion support for all nations. The Maternal Perinatal and Neonatal policy (NDOH, 2021) and maternity case record were developed in South Africa, incorporating the WHO Intrapartum Care Guidelines. These policies emphasise the use of birth companion care during labour. They are to be translated into practice to promote a positive childbirth experience, reducing anxiety related to negative childbirth experiences, increasing facility-based deliveries, which ultimately reduce maternal and neonatal mortality rates. Ideally, in practice, all pregnant women are supposed to select the birth companion of their choice. The maternity case record should indicate the person's name and contact information to call when necessary.
Evidence indicated that birth companion support is an effective strategy for avoiding abuse during childbirth and improving a positive childbirth experience [2]. In addition, birth companion support is one of the most critical aspects of Respectful Maternity Care (RMC) [3]. The benefits of birth companion support are a reduction in caesarean section, reduced hospitalization, reduced incidents of low birth weight, and serve as a non-pharmacological pain relief strategy, enabling the woman to cope with pain during labour [4]. However, although there is increasing evidence that birth companions improve the quality of care and create a more positive childbirth experience, implementing this practice remains a challenge [2, 5].
Implementing birth companion support also promotes end-user satisfaction, leading to achieving Sustainable Development Goal (SDG 3.1), ensuring good health and well-being by focusing on reducing the maternal mortality rate. The initiation of birth companion support involves providing the pregnant woman with continuous emotional and physical support, thereby promoting positive childbirth experiences. In a study conducted by Scholten [6], the level of positive childbirth experience was based on the position chosen by women during labour, where the importance of self-determination is obvious. Simultaneously, self-determination is frequently denied, which is linked to lower levels of birth satisfaction. The scope of birth companions will include facilitating the position adopted during labour.
Different names have been given to the intervention, including labour companion, doula support, emotional support person, or birth-partner during labour, which may refer to any person the woman chooses to support during labour and delivery, including friends, relatives, spouses, or partners [7].
Currently, the US is aggressively pursuing the implementation of birth companion support services through legislation, Medicaid expansion, and measures to incorporate doulas into maternity care. The standardizing and scaling of these services still present a hurdle. Globally, several countries cover doula services under their medical aid programs [8]. Despite the benefits of birth companion support care, its implementation in Sub-Saharan Africa faces systemic and cultural challenges. The barriers identified for the implementation of labour are a lack of awareness, a lack of physical and mental support, poor communication from healthcare personnel, infrastructural issues/privacy, and instances of disrespectful treatment, such as verbal abuse and neglect. These are some of the things that make it difficult for women to cope during labour [9].
In South Africa, a national policy exists, but birth companion support care is poorly implemented during labour. Midwives view birth companions as a distraction and discourage the presence of a birth companion in support care [10]. Furthermore, challenges identified in implementing continuous support include a lack of human resources, insufficient awareness of the benefits of birth companion support care, negative attitudes among nurses, and the architectural layout of the ward [11].
The strategies for implementing birth companion care are outlined under the following headings: healthcare systems can successfully implement birth companion support care interventions by establishing clear policies and infrastructure, and by ensuring resources that support a birth companion’s presence, privacy, and space [12].
Furthermore, they can teach and train healthcare professionals, preparing birth companions on the benefits of birth companion care and their responsibilities. The training will involve community participation, including informing pregnant mothers and collaborating with community leaders and influencers to disseminate information about the intervention. This will be achieved by setting up a tracking system to ensure ongoing implementation and addressing cultural concerns. This will improve outcomes and positive experiences for both mothers and newborns [9].
Based on the study conducted by the lead author, Khan [13], collaboration among government institutions, healthcare providers, and community organizations is crucial for women to fully benefit from birth companion support. This review aims to identify strategies for implementing birth companion support care during labour, increasing hospital-based deliveries, and reducing maternal and neonatal mortality rates.
2. METHODS
The review question was addressed through a scoping review, which examines a research topic that has not been thoroughly discussed before, as described by Arksey and O'Malley1. This was essential for implementing birth companion supportive care during labour and birth. The following process served as a guide for the review: 1) determining the review question, 2) locating applicable research, 3) choosing a study, 4) mapping the data, and 5) compiling, analysing, and presenting the findings. In this review, these five phases served as a framework and guidance.
2.1. Databases and Search Strategy
The following are Boolean terms used to identify studies on birth companion support interventions:
(Strategies OR Methods OR Approaches OR Frameworks OR Techniques) AND (Enhance OR Improve OR Augment OR Develop OR Implement) AND (“birth companion* support” OR “birth supportive care” OR “birth companion care” OR “Labor support” OR “Maternity support” OR “Labor companionship”).
2.2. Determining the Review Question
This review considered the data related to the strategies for implementing birth companion supportive care during labour by reviewing available literature. This scoping review was guided by the question: “What are the present strategies to implement birth companion supportive care?” The review question was determined through a literature review that concentrated on implementing techniques to enhance supportive birth companion care during labour and childbirth. The Joanna Briggs Institute's Population, Concept, Context (PCC) framework was applied in this study (Table 1).
| PCC element | Determinant |
|---|---|
| Population | HCPs (health care providers), women, and birth companions |
| Concept | Strategies to enhance birth companion supportive care |
| Context | Worldwide |
2.3. Finding Applicable Literature
Under PCC's guidance, the datasets used for this review were obtained from Scopus, ProQuest, PubMed, and Web of Science. These databases were chosen because they could locate many relevant studies on strategies for implementing birth companion supportive care during labour and childbirth, which assisted in addressing the review question. For this scoping review, the literature search period covered articles published between 2016 to 2025. The Boolean search operators “And” and “OR ” were employed because the reviewer did not want to restrict the search. The operator “NOT” was not used, and the setting on fields was set to include all fields. The following phrase combination was used in the search: (“Strategies” OR “Interventions”) AND (“Birth doula” OR “Doula” OR “Labour companion” OR “Companion support” OR “Birth companion” OR “Birth coach” OR “Companionship”) AND (“Labour” OR “Labor” OR “Childbirth” OR “Birth” OR “Delivery”).
2.4. Selection of Studies
The criteria for inclusion and exclusion served as a guide for the search. The articles were included if they were written in English. Articles published from 2016 to 2025 reporting on strategies, methods, approaches, techniques, frameworks, and implementation of labour companion or companion support, birth companion, or companionship were included in the review. There was sufficient literature available, and reviewers agreed not to include grey literature to prevent potential bias. The reviewers were involved in the data screening and data extraction process. In this stage, the disagreements were resolved by reviewing one article each reviewer, discussing, and reaching a consensus. The reviewers independently selected one study to ensure uniformity, guided by MMAT (2018). The selected study was used to address the research question, and consensus was reached.
2.5. Data Extraction
Three reviewers (MM, MY, MM, and VN) independently extracted data. They gathered to discuss the extractions, reviewed one article to ensure uniformity, and resolved their disagreements until they reached a consensus.
2.6. Analysis of Data
Four databases were included in the first search, and 290 studies were identified. Covidence identified 74 duplicates. Out of 216 studies screened, 25 were assessed for eligibility, and fourteen articles fulfilled the requirements for inclusion. (Fig. 1) below provides the article selection process.
The thematic analysis technique was used to analyse data. After reading the articles, the reviewers familiarized themselves with the sources and created codes by marking significant and unique themes. The themes were constructed to identify parallels and overlaps while considering the study question, goals, and objectives. The process was completed by reviewing, defining, and naming the themes after they had been identified. The development and piloting of the data charting form were conducted through consensus discussions with reviewers. Each reviewer piloted one article. A summary of the articles included in the review is presented in Table 2.
Table 2: Overview of the studies that were part of the review according to the study title and authors, study type, purpose, context and population, method of data collecting, data analysis, and study results.
3. RESULTS
This scoping literature review identified what is known from existing literature about strategies for implementing birth companion support care. The screening process included fourteen studies. The study's findings will be presented in two sections. Section A identifies implementation strategies, which are models of care, training, and task shifting. Section B outlines the factors that affect the implementation: facilitators and barriers to birth companion support.
Table 2.
| Authors and study title | Type of study | Purpose | Population and context | Data collection method | Data analysis method | Study results |
|---|---|---|---|---|---|---|
| 1. Evans, K., Moya, H., Lambert, M. and Spiby, H., 2022. Developing a training programme for midwives and maternity support workers, facilitating a novel intervention to support women with anxiety in pregnancy. |
Randomised control trial (quantitative design) | To develop a training program to prepare midwives and maternity support workers to facilitate the intervention. | Midwives -facilitators, midwifery support workers as co-facilitators. United Kingdom health care |
Post-training questionnaire | Descriptive analysis | Findings revealed a training program to prepare maternity support workers and midwives to lead the intervention. Facilitators are midwives, while co-facilitators are support staff in midwifery. The UK healthcare post-training survey analysis is descriptive. A training program was created that considered the requirement to deliver instruction within midwives' scope of practice and with the least amount of extra resources. The training schedule consisted of two workshop sessions and a training handbook. *Key implementation strategy: Training |
| 2. Mirzania, M., Shakibazadeh, E., Hantoushzadeh, S., Panahi, Z., Bohren, M.A., and Khajavi, A., 2024. An investigation into the acceptability, adoption, appropriateness, feasibility, and fidelity of implementation strategies for birth companionship in Tehran: A qualitative inquiry on mitigating mistreatment of women during childbirth. |
Qualitative inquiry | To investigate the acceptability, adoption, appropriateness, feasibility, and fidelity of implementation strategies for birth companions (BCs). | Women, BC, Maternal health care providers (MHCP). Tehran. Northern part of Iran |
Face-to-face -in-depth interview | Thematic analysis | Birth companions (BCs) must be trained before entering the maternity ward. Educating women about BC's significance. Designating a committed midwife to offer instruction and designing implementation strategies of birth companion care. *Key implementation strategy: Training |
| 3. Wanyenze, E.W., Nalwadda, G.K., Byamugisha, J.K., Muwanguzi, P.A., and Tumwesigye, N.M., 2023. Effect of midwife-provided orientation of birth companions on maternal anxiety and coping during labour: A stepped wedge cluster randomized control trial in eastern Uganda. |
A quantitative design | To assess the effects of midwife-provided orientation of birth companions on maternal anxiety and coping during labour. | Women Eastern Uganda |
Observation | Descriptive data analysis (STRATA 14) | Midwife-provided orientation of birth companions on labour support lowers maternal anxiety and improves coping during labour. *Key implementation strategy: Training |
| 4. Najafi, T.F., Roudsari, R.L. and Ebrahimipour, H., 2017. Validation of a logic model program to support Iranian females during labour: A Delphi method. | A qualitative study | Verify a program using a logic model to assist mothers during labour and delivery. | Experts of different specialties were selected for the study. Iran |
E-Delphi | Frequency counting-consensus | The findings showed that a comprehensive program to assist mothers during labour could be divided into six categories: preparation, equipment and facilities, education, process and intervention, and evaluation. *Key implementation strategy: Training |
| 5. Shakartzi, H., Wenren, L., Fernandes, S., Marino, R., Meade, M., Pierre-Joseph, N., Rodrigues, D., St. Omer Roy, N., Valle, E., and Abbott, J.F., 2018. DREAM: Empowering preclinical medical students with labour support. | Quantitative design | This program aims to provide labour support to preclinical medical students. | Medical students were trained by doulas/midwives on labour support. United States of America |
Survey | Descriptive data analysis | Students demonstrated increased knowledge and communication, advocacy, and support for women in labour. Both students’ and patients’ reflections show that the program was mutually beneficial. *Key implementation strategy: Task shifting |
| 6. Yaya Bocoum, F., Kabore, C.P., Barro, S., Zerbo, R., Tiendrebeogo, S., Hanson, C., Dumont, A., Betran, A.P., and Bohren, M.A., 2023. Women’s and health providers’ perceptions of companionship during labour and childbirth: A formative study for implementing the WHO companionship model in Burkina Faso. | Qualitative study | To identify barriers and facilitating factors to the implementation of labour companionship. | Women, potential companions, and health workers. Burkina Faso |
In-depth interviews | Thematic data analysis | All participants acknowledged the existence of the traditional companionship model. Participants were not familiar with companionship during labour and childbirth. Training potential companions is recommended. *Key implementation strategy: Models of care |
| 7. Dilruwan, P., Goonewardene, M. and Furukan, R., 2022. Medical and administrative barriers to the implementation and sustenance of a labour companionship program: A cross-sectional study in a teaching hospital in Sri Lanka. | Cross-sectional study (quantitative) |
To describe how medical and administrative barriers in implementing a labour companionship program were addressed. | Specialists, obstetricians, gynaecologists, house officers, staff nurses, midwives. Sri Lanka |
Questionnaire | Descriptive data analysis | Midwives must be educated regarding the beneficial effects of a labour companion. Doctors and nurses must be motivated to increase the counselling of women and their partners regarding the beneficial effects of a labour companion to sustain the program. *Key implementation strategy: Training |
| 8. Kabakian‐Khasholian, T., Bashour, H., El‐Nemer, A., Kharouf, M., Elsheikh, O., Labour Companionship Study Group, Sheikha, S., Saleh, S., Jaffa, M., Barazi, R., and El Lakany, N., 2018. Implementation of a labour companionship model in three public hospitals in Arab middle‐income countries. | Implementation research using mixed methods | To evaluate the integrated personalized labour companionship model's viability, acceptability, efficacy, and cost. | Women, health care providers, and management. Arab |
A pilot-tested questionnaire and semi-structured interviews with women, labour companions, and health care providers. | Thematic analysis | The model was determined to be workable, acceptable, efficient, and economical. Implementation included a steering committee, seminars for healthcare providers, IEC materials, and adjustments in labour rooms. *Key implementation strategy: Model of care |
| 9. Steward, R.P., 2021. Feasibility of implementing a hospital-associated doula program in a metropolitan hospital (doctoral dissertation, University of Kansas). | Quantitative design | To assess the readiness and necessary steps for a mid-sized metropolitan hospital to implement a hospital-associated doula program. | Health care provider, management, obstetrician. United States of America |
Survey | Descriptive data analysis | The most commonly reported strength was an open and experienced staff. The most frequently reported weakness was the concern of provider support for the doula program. *Key implementation strategy: Training |
| 10. Kivlighan, K.T., Gardner, T., Murphy, C., Reiss, P., Griffin, C., and Migliaccio, L., 2022. Grounded in community: Development of a birth justice‐focused volunteer birth companion program. | Qualitative | To increase access to continuous labour support by bringing the community into the hospital. | Community volunteers. Mexico |
Interviewed before training | Thematic analysis | Co-values to guide the development of the program were radical presence, radical respect, non-judgmental, and self-care. *Key implementation strategy: Training |
| 11. Leap, N. and Hunter, B., 2022. Supporting women for labour and birth: A thoughtful guide. Routledge. | Qualitative | To support women in labour and birth. | Women, doulas, and maternal health care providers, including midwives, doulas, childbirth educators, and students. London |
Narrative | Thematic analysis | Encouraged readers to consider how this could be integrated into their work by evaluating their own experiences and analyzing the research data, as well as the experiences of women and practitioners. *Key factors enabling the implementation strategy |
| 12. Boire, 2022. Birth companions: Teaching students to become doulas. |
Quantitative | To provide nursing students with the opportunity to develop knowledge and skills to provide continuous labour support to women. | Women and birth companions. America |
Survey | Descriptive data analysis | Educating nursing students to become doulas through programs, such as “Birth Companions,” is one way to help fill the gap. Such programs also benefit students by providing them with opportunities for interprofessional collaboration, developing leadership skills, and fostering involvement in local communities. *Key implementation strategy: Task shifting |
| 13. Wanyenze, 2023. A qualitative exploratory interview study on birth companion support actions for women during childbirth. |
Qualitative study | To investigate ways that birth companions can assist mothers during delivery. | Ten women who were admitted in early labour for NVD and had a full-time birth companion. Eastern Uganda |
In-depth interviews and non-participant observations | Thematic analysis | Support activities that contributed to a positive experience included body massage for pain treatment, emotional presence, motivation, feeding, and messenger activities. Companion apprehensive behavior and disrespectful care were examples of support behaviors that made it difficult to cope with labour. The women anticipated that BC would be considerate, trustworthy, and attentive to their needs. *Key factors enabling the implementation strategy |
| 14. Najafi, 2020. Developing a supportive care plan for women during labour based on the logic model |
A qualitative study | To develop a supportive care plan for labour using the logic model. | 25 mothers and eight health care professionals. Iran |
Semi-structured interviews | The stages of supportive program development included identifying problems, defining inputs, activities, and outputs, and determining program outcomes. | The created care plan identified five areas under the input category: infrastructure, equipment, facilities, training, and processes. Under the activities category: creating interventions, carrying them out, and adhering to moral principles. Under output: statements related to assessment. Under outcomes: short-term and long-term plans. *Key implementation strategy: Model of care. |
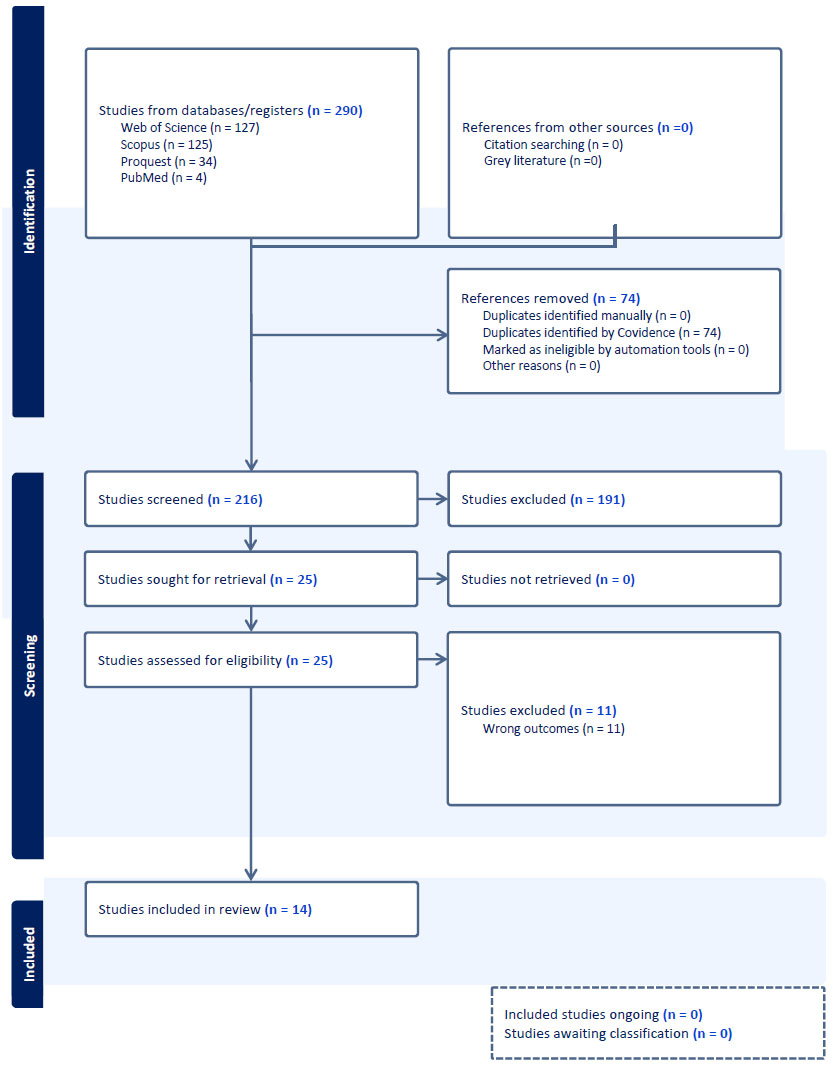
PRISMA diagram of the article selection process (Covidence).
3.1. CHARTING DATA
Fourteen studies were included in this review. Seven studies used qualitative research designs, one used mixed methods, and six studies were quantitative. All fourteen included articles were reviewed using the following organizational categories: author (s), study title, type of study, purpose, population and context, data collection method, data analysis method, and study results. The studies in this review are summarized in Table 2.
3.2. Compiling, Analysing, And Reporting The Findings
The thematic analysis of the studies included in this evaluation yielded five themes, as described below. A summary of the articles’ origins is presented in Table 3.
| Article Origin | Number |
|---|---|
| America | 03 |
| Arab | 01 |
| Burkina Faso | 01 |
| Eastern Uganda | 02 |
| Iran | 03 |
| London | 01 |
| Mexico | 01 |
| Sri Lanka | 01 |
| United Kingdom | 01 |
3.2.1. SECTION A: Identified Implementation Strategies
3.2.1.1. THEME 1: Models for Implementation of Companion Support Care During Labour.
The first theme identified from the findings of this review is models for implementing companion support care during labour. Two models were identified from the above theme: the labour companionship model and the logic model.
3.2.1.1.1. Labour Companionship Model [14]
Developing a model for labour companionship in different settings requires consultation with stakeholders, including women, health care providers, and management. Implementing the labour companionship model involves creating a steering committee and seminars, as well as using information, education, and communication materials.
According to Najafi [12], a logic model refers to formulating a program according to mothers' demands and desires during childbirth, which is the main aim of holistic care. The key elements of this model are preparation, equipment or facilities, education, process activities, interventions, and evaluation.
3.2.1.2. THEME 2: Development of Training Programmes
The second theme identified from the findings of this review is the development of training programmes. Three training programmes were identified from the above theme: Kern`s six steps for curriculum development, a birth justice-focused volunteer birth companion program, and training programmes for midwives and maternity workers.
3.2.1.2.1. Kern`s Six Steps for Curriculum Development [7]
Kern's six-step curriculum development technique was chosen because it is widely used in healthcare education. It helps organize, summarize, and assist with essential issues unique to developing clinical and professional skill curricula. This method was employed to determine the training requirements for maternity support workers and midwives to help pregnant women experiencing anxiety and to provide a supportive intervention.
3.2.1.2.2. Establishment of a Birth Justice-focused Volunteer Birth Companion Programme [15]
An evidence-based approach shown to improve birth outcomes is continuous labour support, especially when given by a qualified doula. Regretfully, not everyone supports ongoing labour help from a preferred companion. As a result, a person has few resources and cannot use a skilled doula's services. Volunteering in birth companion programs expands access to ongoing labour support by integrating the community into the hospital.
Multistakeholder collaboration involving community health workers, regional reproductive justice organizations, hospital-based clinicians, administrators, and staff directly responds to community needs. The WHO states that every woman has the right to a good delivery experience, which includes mobility during labour and a birth position of choice, clear communication from maternity care, respect and dignity, and a companion of her choice.
3.2.1.2.3. Developing a Training Programme for Midwives and Maternity Workers [7]
A training program was created that considered the requirement to deliver instruction within the midwife's scope of practice and with the minimal use of additional resources. The training schedule consisted of two workshop sessions and a training handbook.
3.2.1.3. THEME 3: Task Shifting
The third theme identified from the findings of this review is task shifting for the implementation of companion support care during labour. Three task-shifting initiatives were identified from the above theme: empowering medical students, training midwives/doulas, and community volunteers to provide birth companion support care during labour.
The Dream program [16] aims to empower medical students by training them to provide labour support through orientation and shadowing a midwife or doula, offering labour support, conducting their own client orientation, and providing training to the medical student. Student midwives are also trained to support women during labour [16], and community volunteers are trained to provide birth companion support care during labour.
3.2.2. SECTION B: Factors Affecting The Implementation Strategy
3.2.2.1. THEME 4: Facilitators for Implementation Of Birth Companion Care During Labour
The fourth theme identified from the review findings is facilitators for implementing companion support care during labour. Three facilitators were identified from the above theme, namely: the need for training, midwives, and birth companions before entering the maternity hospital; addressing any physical infrastructure concerns; and an investigation into the acceptability, adoption, appropriateness, feasibility, and fidelity of implementation strategies for birth companionship [2, 17].
3.2.2.2. THEME 5: Barriers to the Implementation Of Birth Companion Support Care During Labour
According to Wanyenze [9], support actions that hinder coping with labour included fearful behaviors, such as some birth companions crying. This makes it difficult for the woman to cope with pain and anxiety. Furthermore, Minnie [11] stated that a lack of awareness of the benefits of birth companion support care, negative attitudes among nurses, and inadequate infrastructure are barriers to the implementation of birth companion support care.
4. DISCUSSION
There is a need to implement birth companion support in South Africa. Although the researchers acknowledge that the existing global strategies are evidence-based, they may not be automatically implemented in South Africa due to various factors, including overpopulation, the burden of disease, and culturally related elements. Therefore, for the success of this intervention, strategies will be adopted according to the South African context.
The implementation outcomes framework for successful implementation, as proposed by Proctor et al. (2011), was employed in this study, utilizing the following indicators: implementation outcomes, service outcomes, and client outcomes. Addressing the research-to-practice gap and scaling up evidence-based interventions are the key goals of implementation science.
The objective of this review was to determine what information is currently available for implementation strategies to enhance birth companion support during labour. The findings of this review revealed that midwives should provide orientation to a birth companion support person during the antenatal care clinic, intrapartum, and postnatal periods. This includes using an orientation book on the benefits of birth companion care, informing women about the role of birth companions, and assigning a dedicated midwife to provide training for maternal care providers. In this review, the emphasis is placed on the facilitators of birth companion care [18-20].
To maximize the facilitators of birth companion support care, models of maternity care must be intentionally designed to leverage enablers at every level, policy, system, facility, community, and individual. These approaches should be rights-based, relationship-centered, community-inclusive, staff-supported, and evidence-informed [7].
The review further revealed that models for implementing birth companion support care may assist in facilitating the process by establishing a steering committee to oversee and facilitate implementation, adjusting the process to the local context, assigning key personnel responsible for implementation, and proposing and approving channels of communication. Under the labour companion model, the steering committee and the research team are responsible for organizing seminars and workshops for target groups in the setting to create awareness about the benefits and roles of birth companion support care.
In addition, the use of information, education, and communication (IEC) materials like flipchart messages and posters can be used as a means of briefing the women and their companions upon arrival at the antenatal clinic and labour ward on benefits, roles of the birth companion, and the regulations in the labour room. Training is one of the most effective tools for optimizing facilitators for delivering birth companion support care. Effective training ensures that the workforce not only accepts birth companions but also actively supports them by aligning knowledge, attitudes, skills, and processes [2]. It is through the training of the target groups that the barriers to implementing a birth companion support can be overcome [18].
Before implementation, adjustments in the labour rooms are necessary to make the environment user-friendly and maintain the privacy and dignity of patients. This will also promote the implementation of the South African Department of Health's Integrated Maternal and Neonatal Guidelines among the target groups of maternal healthcare providers, women, and birth companions.
The findings also revealed that identifying the issues, outlining the inputs, actions, and outputs, as well as determining the program's goals, were all phases of the supportive development program. Five categories of infrastructure, equipment, facilities, training, and procedure were categorized in the care plan's outcomes. The tasks were divided into three categories: creating interventions, implementing interventions, and adhering to ethical guidelines. Assessment-related statements were proposed as output. The outcomes were defined as short-term and long-term related to the program`s intervention.
The review further revealed that task shifting may assist with implementing a birth companion strategy. The orientation of student doctors and nurses may help close the gap in areas where there is a shortage of midwives and the absence of a family member assigned to the woman during labour. The orientation includes a one-hour welcome meeting, shadowing a midwife with an assigned client. The support training may last 4-5 hours, including sessions with midwives and birth sisters, a prenatal meet and greet visit (home visit), labour and delivery labour support, and a postpartum follow-up visit.
When used effectively, task shifting reduces bottlenecks, frees up time, and enables companions and staff to perform more productive and complementary roles. Particularly in environments with limited resources and barriers, task shifting, the reorganization of duties among health workforce teams, can significantly increase facilitators for delivering birth companion support services [16]
This review further revealed the assistance initiatives for women giving birth as facilitators for implementing birth companion support care [9].A psychologically secure setting with ongoing emotional support is essential for a satisfying delivery experience. In contrast, support actions, such as physically assisting women, providing nourishment, messenger activities, body massage for pain relief, assistance with walking, and offering tea or food, were the primary forms of care among all the birth companions [19]. Labour companions further walked with the woman during labour and encouraged her to walk, even if she did not feel like doing so.
Mobility and upright posture are advised to aid the baby`s descent and pain management during labour. Effective communication is essential to providing respectful maternity care. The women said they felt appreciated and comforted all the time. They felt more in control of the situation, and their confidence increased.
The review further revealed that key barriers to implementing companionship during labour and childbirth include limited space in labour and delivery wards, an open-floor-plan maternity ward, the absence of private rooms for women, hospital rules preventing companionship, and social norms that discourage the woman from choosing a companion [20].
Birth companion support is a cost-effective strategy that might be expanded to fulfill the objectives of the SDGs and Universal Health Coverage. WHO recommends it as a quality improvement strategy. Countries with institutionalized companion policies (e.g., Brazil, India, Tanzania) exhibit improved care satisfaction, reduced litigation, and a more positive public perception of maternity care [21].
The tensions that arise from allowing task shifting in implementing birth companion support care stem from organizational, professional, ethical, and systemic challenges. Task shifting, delegating tasks from highly specialized professionals (e.g., doctors, midwives) to less specialized health workers, support staff, or community members, can help facilitate companion support. Still, it also introduces conflicts and risks that must be carefully managed.
Midwives and nurses may feel that their autonomy, authority, or professional space is undermined when tasks are shared with or delegated to non-clinicians. Healthcare providers were concerned about the role of the companion and the possible interference with activities in the labour ward. Allocation of resources, organization of care, facility-related constraints, and cultural inclinations were identified as implementation barriers. Therefore, before introducing the companion of choice at birth, understanding providers’ attitudes and sensitizing them is essential.
Gap: Limited data are available on effective strategies to improve birth companion coverage and inform scale-up efforts [22]. Only a single clustered randomized control trial was conducted to assess the feasibility, acceptability, and impact of implementing the birth companion intervention package in Ethiopia, Kenya, and Nigeria. Although several birth companion models have been identified, no study directly compares the cost-effectiveness of the volunteer-based model with the hospital staff-based model.
CONCLUSION
In conclusion, more studies have been conducted in high-income countries and are not directly related to the South African context. Therefore, implementation strategies must be adopted that are appropriate for the context. Nevertheless, scant research has been done in South Africa on implementing birth companion care. Introducing birth companion support as a routine practice will require commitment from policymakers, healthcare providers, and communities to sustain this evidence-based intervention. Implementing a strategy to enhance birth companion care requires training all target audiences on the benefits and role of birth companions, including addressing barriers, such as cultural norms, institutional policies, staff attitudes, and space limitations.
RECOMMENDATIONS FOR FUTURE RESEARCH
There is growing evidence of efficacy, but less research is carried out on sustainably implementing companionship in diverse systems. Context-specific studies regarding localized implementation research are needed (e.g., facility design, cultural barriers, legal frameworks). Few standardized indicators exist to track the integration of birth companions.
LIMITATION OF THE STUDY
Studies in other languages that could have provided helpful information were not included since this review only covered English-language studies. The findings may not be generalizable to the rural setting, as the context may differ.
AUTHORS’ CONTRIBUTIONS
M.M.K., M.Y., M.R., and T.V.N. contributed to the conception and design of the study and assisted in data collection and analysis.
LIST OF ABBREVIATIONS
| PCC | = Population, Concept, Context |
| WHO | = World Health Organization |
| MHCP | = Maternal Health Care Providers |
| NDOH | = National Department of Health |
AVAILABILITY OF DATA AND MATERIALS
The data and supportive information are available within the article.
ACKNOWLEDGEMENTS
The first author would like to thank the supervisors and the librarian for their expert advice and support throughout the review.

