All published articles of this journal are available on ScienceDirect.

Knowledge, Attitudes and Practices Regarding Dengue, Chikungunya, and Zika and their Vector Aedes Aegypti in Villavicencio, Colombia
Abstract
Background:
Aedes aegypti transmits dengue, chikungunya and zika, and high infestation rates of this mosquito are responsible for maintaining these arbovirus outbreaks in endemic areas
Objective:
To estimate the knowledge, attitudes, and practices regarding dengue, chikungunya, and zika and their vector Aedes aegypti in Villavicencio, Colombia.
Methods:
A descriptive, cross-sectional study was conducted. Verbal informed consent was obtained from adults and then interviewed using a structured questionnaire. Houses were randomly selected; in the event that no one was home, the next house was selected. Entomological data were recorded to calculate the larval indexes at homes.
Results:
Seventy-six houses (309 people) were evaluated. 70% of subjects were aware that dengue, chikungunya or zika are viral diseases. Fever was considered the most important symptom and could be related to the experience of having these diseases at home. 79.45% knew that a mosquito transmits these diseases but did not know the scientific name or that only the female bites. 81.36% did not know the life cycle of the mosquito but were aware that the elimination of breeding sites and destruction of containers with water could aid in transmission prevention. 88.46% recognized that the community should be responsible for these control actions at home, but the recommendations are not implemented due to the lack of interest or apathy. The average house index was 40.3%, and Breteau index was 47.66%. Low tanks represented the most common breeding site.
Conclusion:
It is necessary to review campaigns, communication, and education promoted in the municipality because they do not reflect the knowledge of the people.
INTRODUCTION
Worldwide, approximately 1500 arboviruses (arthropod-borne viruses) are known to be transmitted by one or several of approximately 100 vector mosquito species [1], which are the main vectors for most known arboviruses [2, 3]. Aedes aegypti is one of the most important vectors of viruses, transmitting diseases such as dengue, chikungunya, zika, yellow fever, and more recently, mayaro virus. High infestation rates of this mosquito are responsible for maintaining these arbovirus outbreaks in endemic areas, such as Colombia [4].
In Colombia, 106,763 chikungunya cases were reported in 2014, and 359,728 cases were reported during 2015; of these, 21,290 were reported in Meta (fatality rate of 0.015%). Till the 43rd epidemiological week in the country, 19,215 cases of chikungunya had been reported in 2016. For dengue, 94,916 cases were reported during 2015, and 95,711 cases had been reported up until the 43rd epidemiological week of 2016; of these, 2,426 belong to Meta county [5, 6]. Since the confirmation of zika circulation in Colombia during the 40th epidemiological week of 2015, 11,712 cases were reported during 2015, and till the 43rd epidemiological week of 2016, 10,5085 zika cases have been reported in Colombia [5, 6].
In Colombia, living conditions, urbanization and disorderly growth of endemic cities, risk behaviors and practices, intense commercial exchange and increased frequency of travel favor the emergence and re-emergence of these diseases. Also, climatic and ecological conditions are optimal for mosquito breeding and therefore the circulation and transmission of these arboviruses; particularly because Aedes aegypti is present in almost the entire country. Although mosquitoes live below 1,500 meters above sea level (m.a.s.l), in Colombia, their presence has been reported under 2,200 m.a.s.l [7]. The main determinant that has enabled mosquito introduction is the displacement of travelers and carriers of viruses from areas with active transmission to other areas. The dynamics of virus transmission depends on the interactions between the atmosphere, agent, and the host population vector, and its ability to coexist in a specific habitat is determined by environmental factors and the socioeconomic, political, and biological characteristics of the virus, vector, and the person affected [8].
Some of the risks factors identified in Colombia for endemic transmission of these arboviruses are that 85% of the 1,123 municipalities are located less than 2,200 m.a.s.l, making them susceptible to the presence of Aedes spp. (Ae. aegypti and Ae. albopictus) and high levels of infestation. Dengue is also considered to be endemic in different intensities in municipalities located between 0 and 2,200 m.a.s.l.
The persistence of breeding sites, risk behaviors, and practices of social and institutional factors, as well as the proliferation of other potential problems (such as solid waste collection), increases the likelihood of dengue, chikungunya, zika, and other febrile syndromes, making clinical diagnosis difficult. Limited accessibility to a diagnostic laboratory, which has caused delays in diagnosis, and a lack of trained health personnel in some endemic areas, has resulted in a reduced opportunity to detect cases and report them correctly [8].
For the above reasons, it is necessary to take extra efforts in the identification, registration, and correct notification of these arboviruses for the Colombian public health surveillance system (SIVIGILA). Additionally, it is important to conduct research to improve the quality of life for the population at risk, and it is essential to evaluate the communities and their actions to combat these diseases. The main goal of this study was to estimate the knowledge, attitudes, and practices of people in Villavicencio, Colombia about dengue, chikungunya and zika viruses and their vector, Aedes aegypti.
MATERIALS AND METHODS
Target Population and Sample
The study was carried out in the city of Villavicencio, the capital of Meta county and its largest city with 728,891 inhabitants; located in the foothills of the eastern mountain range, northwest of Meta on the left bank of the Guatiquia river, the city has a warm climate with temperatures ranging from 20°C up to 39°C. The temperature is related to precipitation; thus, the hottest months are those with less rainfall, especially February and March. In general, the rainy season lasts from April until November.
Two neighborhoods were selected for the project: Nueva Colombia and La Reliquia. The selection of the sample was based on 700,000 estimated people living in the urban area of the municipality, with a confidence level of 95%, an error rate of 5% and an expected frequency of 7%. This resulted in a sample size calculation of 100 people for the study.
Method
A descriptive cross-sectional study was conducted in April 2016. A structured questionnaire about Knowledge, Attitudes and Practices (KAP), designed by Ministry of Public Health and Social Welfare (2013) [9] and Castañeda et al. (2011) [10] was used with some modifications. The survey included: general data, knowledge, attitudes, practices and mass media use (Table 1). The inclusion criteria to be interviewed were: adults that lived in the house visited and verbal informed consent obtained from the respondent. Confidentiality was ensured throughout the study.
| Group of variables | Themes included | Description |
|---|---|---|
| General data | Age, sex, education, marital status, job, who live in the house, property characteristics | General data for a socioeconomic description of the population |
| Knowledge | What is, how the disease does gets, how to prevent, symptoms, who had dengue chikv or zika at home. Name of the vector, time of biting, breeding sites and life cycle | Information about knowledge of dengue, chikv and zika. |
| Attitudes | How to protect yourself from mosquito bites, Why people do not implement the recommendations | Information about individual attitudes to avoid, control and cure this diseases |
| Practices | What practices to prevent these diseases and how often | Information about individual practices to avoid the transmition of these diseases |
| Media use | Which media and how often do you use them to be informed | Described the individual access to mass media |
The houses were randomly selected; in the event that no one was home, the next house was selected. Medical students of the Universidad Cooperativa de Colombia and the Health Department of Meta were recruited during an educational activity about zika within the communities.
In addition to the survey, entomological data were recorded to calculate the larval indexes at homes. House index, container index, and Breteau index were also calculated [11].
RESULTS
Seventy-six houses were visited in the two neighborhoods during April 2016. Both neighborhoods represent low and very low socioeconomic levels. Adults from 18 to 80 years old were surveyed with an average age of 41.81 years (SD ±14.96). In total, 309 people lived in the 76 houses studied; most (53.07%) of the inhabitants were adults (CI 44.95-61.2%), and 36.57% were children (CI 29.83-43.31%) (Table 2). On average, 2.25 adults (SD ±1.04) and 1.98 children (SD ±1.25) lived in each house, with a minimum of 1 to a maximum of 10 people per house. In total, 73.33% of the sample was female, and most of the females were housewives (46.48%; CI 34.55-58.71%). Most of those surveyed have a basic education, and only 5.54% possess undergraduate studies (technical and university). Almost all persons surveyed had an affiliation to the health system, but 4.48% (CI 0.93-12.53%) of those surveyed did not have any affiliation. Basic services such as electricity, sewage and drinking water are nearly provided for the entire population; nevertheless, 96% of the homes had water storage tanks. The most common reasons to store water were “to wash”, “just in case” and “for the toilet” (Table 2).
| Socio-demographic variables | Frequency | % | 95% CI |
|---|---|---|---|
| Gender | |||
| Male | 20 | 26.67 | 17.11-38.14 |
| Female | 55 | 73.33 | 61.86-82.89 |
| Occupation | |||
| Housewife | 33 | 46.48 | 34.55-58.71 |
| Merchant | 4 | 5.63 | 1.56-13.8 |
| Unemployed | 3 | 4.23 | 0.88-11.86 |
| Employed in private enterprise | 3 | 4.23 | 0.88-11.86 |
| Student | 3 | 4.23 | 0.88-11.86 |
| Construction worker | 4 | 5.63 | 1.56-13.8 |
| Independent worker | 18 | 25.35 | 15.77-37.08 |
| Other | 3 | 4.23 | 0.88-11.86 |
| Marital status | |||
| Married | 16 | 21.33 | 12.71-32.32 |
| Separated/divorced | 3 | 4.00 | 0.83-11.25 |
| Single | 18 | 24.00 | 14.89-35.25 |
| Living common law | 35 | 46.67 | 35.05-58.55 |
| Widowed | 3 | 4.00 | 0.83-11.25 |
| Level of education | |||
| Primary | 36 | 50.70 | 38.56-62.78 |
| High School | 31 | 43.66 | 31.91-55.95 |
| Technical studies | 2 | 2.82 | 0.34-9.81 |
| University | 2 | 2.82 | 0.34-9.81 |
| Household information (people living at home) | |||
| Children | 113 | 36.57 | 29.83-43.31 |
| Teenager | 21 | 6.79 | 3.88-9.70 |
| Adults | 164 | 53.07 | 44.95-61.20 |
| Seniors | 11 | 3.56 | 1.45-5.66 |
| Health system affiliation | |||
| Contributive | 29 | 43.28 | 31.22-55.96 |
| Special | 2 | 2.99 | 0.36-10.37 |
| Without affiliation | 3 | 4.48 | 0.93-12.53 |
| Subsidiated | 33 | 49.25 | 36.82-61.76 |
| Electricity | |||
| Yes | 75 | 100.00 | - |
| No | 0 | 0 | |
| Drinking water | |||
| Yes | 63 | 14.86 | 74.96-92.34 |
| No | 11 | 85.14 | 7.66-25.04 |
| Sewerage | |||
| Yes | 72 | 97.30 | 90.58-99.67 |
| No | 2 | 2.70 | 0.33-9.42 |
| Garbage collection | |||
| 2-3 times per week | 76 | 100.00 | - |
| Water storage tanks at home | |||
| Yes | 72 | 96.00 | 88.75-99.17 |
| No | 3 | 4.00 | 0.83-11.25 |
| Use for stored water at home | |||
| Reserve water | 20 | 28.95 | 16.28-41.69 |
| To wash | 33 | 47.82 | 31.51-64.14 |
| For toilet | 4 | 5.79 | 0.11-11.47 |
| Other | 12 | 17.39 | 7.55-27.23 |
The survey was constructed to determine the knowledge about three vector borne diseases (dengue, chikungunya, and zika) transmitted by Aedes spp. To the question “What do you think dengue, chikungunya and zika are”, between 40 and 45% of the people considered it just a disease, and between 20 and 25% thought it was a virus. There is still a percentage of people who do not know about the existence of these diseases (10-17%) Fig. (1).

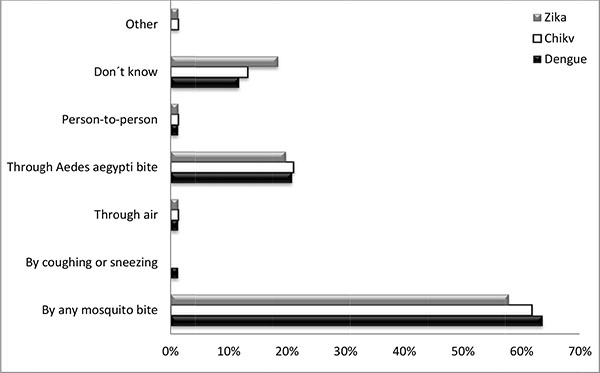
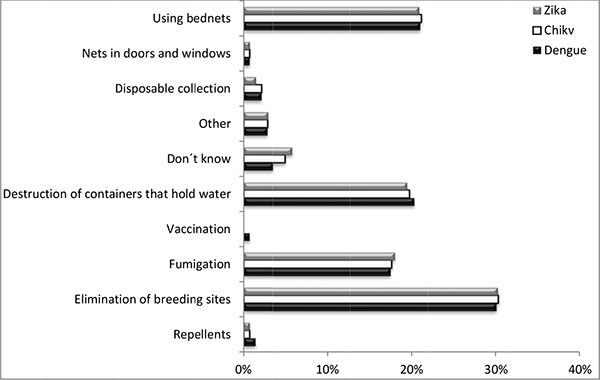
In general, people know that a mosquito could transmit these diseases, although they did not know the scientific name of the mosquito (79% of those surveyed did not know the scientific name, and 68% did not know that only females bite). Between 11 and 19% did not know how these diseases spread Fig. (2). These communities know that the elimination of breeding sites and the destruction of containers that could hold water are important to prevent the disease. The use of repellents was not considered important for prevention Fig. (3).
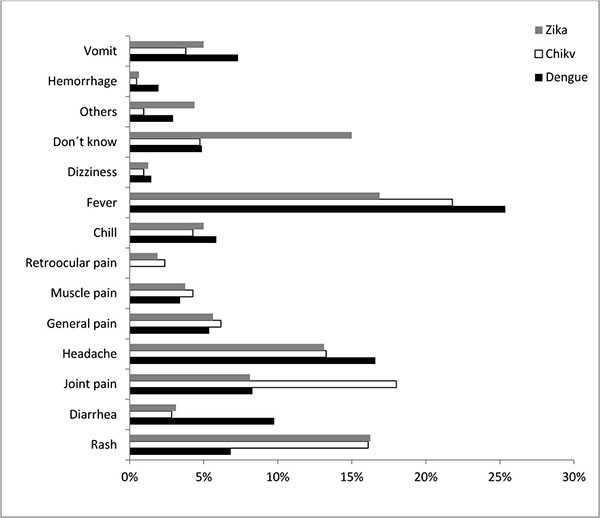
Regarding the knowledge of the symptoms of the three diseases, most of those surveyed considered fever as a symptom for the three viruses (dengue 25.37%, CI 19.56-31.90%; chikungunya 21.8%, CI 16.43-27.99%; zika 16.88%, CI 11.43-23.59%). For chikungunya, joint pain was commonly considered a symptom (18.01%, CI 13.07-23.87%); for zika, 15% (CI 9.85-21.49%) of the people surveyed did not know of any symptoms Fig. (4). This knowledge could be related to the individual’s experience of having one of these diseases; in total, 32% (CI 21.85-45.4%) of the people claimed that they have had or know that someone in their family has had dengue. For chikungunya, the percentage was higher at 67.12% (CI 55.13-77.67%), with zika at 23.81% (CI 13.98-36.21%). The percentage of sick people who were diagnosed by a medical doctor was 75% (CI 50.90-91.34%) for dengue, 62.2% (CI 46.54-76.23%) for chikungunya, and 23.81% (CI 13.98-36.21%) for zika. Although these percentages differed, there was no significant difference between dengue and chikungunya (p>0.05). Additionally, there was no association between the number of sick people at home and the presence of idle water tanks at home (p>0.05) for the three viruses.
Regarding the mosquito and its life cycle, 95% of the people said that mosquitoes breed in water (clean or dirty), 50.63% (CI 39.14-62.08%) said that they breed in dirty backwater, and the remaining 44.30% (CI 33.12-55.92%) said that mosquitoes breed in clean backwater. Some of the breeding sites listed by respondents included tires, bottles, plants, vases, sewer, tanks, and holes in the floor and walls. In response to the question, “How to remove breeding sites?”, 38.58% (CI 30.08-47.63%) said by removing accumulated water, and 26.77% (CI 19.31-35.35%) said by washing the laundry tank. Likewise, 88.46% (CI 73.19-90.82%) of the respondents said that each person and family must remove the breeding sites, and 8.98% said that the mayor’s office and Health Department were responsible for removing breeding sites. According to the answers in the survey, breeding site removal must be conducted more frequently each week (44%; CI 32.55-55.94%).
Regarding the knowledge of mosquito feeding time, 26.67% (CI 17.11-38.14%) did not know the mosquito feeding time. In total, 24.00% (CI 14.89-35.25%) said that mosquitoes feed during the morning and afternoon, and 18% (CI 10.6%-29.33%) said mosquitoes feed 24 hours a day. Despite these results, 81.36% (CI 69.09-90.31%) claim they do not know anything about the life cycle of the mosquito. The remaining 18.64% of the respondents provided answers such as the following: “eggs and larvae”, “eggs, larvae, and bug”, “in 30 days they laid 300 eggs”.
In response to the question “Why do mosquitoes bite?”, 42.64% think that they bite because they need to feed, and 10.29% think they bite because they are hungry. Other answers included “to contaminate people”, “because God permits that”, “because they like to bite us and our blood”.
In spite of the knowledge of the communities regarding the disease and the vector, according to the survey, they do not implement the recommendations because they are not interested (39.51%, CI 28.81-50.99%), due to laziness (27.16%, CI 17.87-38.19%), or because they do not understand what they need to do (12.35%, CI 6.08-21.53%). However, 97.33% of the respondents think that it is important to receive visits from experts to monitor and teach them about these issues; highlighting the importance of environmental education to the communities.
People in these two neighborhoods protect themselves from mosquito bites by using bed nets (51.92%, CI 41.91-61.83%), insecticides (27.88%, CI 19.54-37.53%) and repellents (13.46%, CI 7.56-21.55%). To prevent the disease, they eliminate accumulated water (36.67%, CI 28.06-45.95%), eliminate breeding sites (29.17%, CI 21.23-38.16%), clean the house and throw out the garbage (16.67%, CI 10.49-24.56%). A total of 1.67% (CI 0.20-5.89%) of the survey respondents do not do anything to prevent mosquito bites. These results demonstrated the engagement level of the people with an individual and collective cause.
Most of those surveyed went to the doctor when they felt sick with symptoms related to dengue, chikungunya, or zika (48.1%, CI 36.71-59.64%). However, 37.97% (CI 27.28-49.59%) simply take medication without seeking medical services, 11.39% rest at home, and 2.53% drink many water.
During rapid sampling inside the houses visited, the larval indexes showed a house index of 39.22% and 41.38% for Nueva Colombia and La Reliquia, respectively. The container index was 10.76% for Nueva Colombia and 11.57% for La Reliquia. The Breteau index was 47.06% and 48.28% for Nueva Colombia and La Reliquia, respectively. The highest percentage of positive breeding sites was in low tanks in the two neighborhoods (62.5% and 57.14% in Nueva Colombia and La Reliquia, respectively). In Nueva Colombia, containers not in use had a breeding site percentage of 20.83%, while for La Reliquia the containers in use had a breeding site percentage of 28.57% (Table 3).
| % | |||
|---|---|---|---|
| Larval Index | Nueva Colombia | La Reliquia | Average ± SD |
| House | 39.22 | 41.38 | 40.30 ± 1.53 |
| Deposit | 10.76 | 11.57 | 11.17 ± 0.57 |
| Breteau | 47.06 | 48.28 | 47.67 ± 0.86 |
| Breeding sites | |||
| High tank | 0.00 | 0.00 | 0.00 ± 0.00 |
| Low tank | 62.50 | 57.14 | 59.82 ± 3.79 |
| Tires | 4.17 | 7.14 | 5.65 ± 2.10 |
| Plants | 4.17 | 0.00 | 2.08 ± 2.95 |
| Containers in use | 8.33 | 28.57 | 18.45 ± 14.31 |
| Containers in disuse | 20.83 | 7.14 | 13.99 ± 9.68 |
DISCUSSION
The neighborhoods studied represent a low social level in Villavicencio and were the consequence of land invasion years ago. Therefore, this led to a lack of proper planning in infrastructure for water supply and sewage. Currently, the city does not have a permanent water supply, forcing inhabitants to store water improperly. The houses have high tanks (in ceilings) and low tanks (in kitchens, backyards, and bathrooms), which are usually full of water and lack protection against mosquitoes. This unbridled urbanization makes these communities more receptive to epidemics caused by vector borne diseases [12].
Although the communities receive education about these diseases and the level of knowledge of disease transmission by Aedes spp. seems to be high, the learning is not being put into practice regularly. Similar results were obtained in Paraguay, where communities with a high level of knowledge, doesn´t participate in any control activities, leading to a failure in the vector control programs [13]. Knowledge about a subject does not always translate into behavior change, presumably because it is difficult to change a person’s behavior, as seen in Thailand and Peru [14, 15] similar results were obtained in Jamaica where the good knowledge about dengue did not translate to adoption of preventive measures [16]. It is quite common that although some people do take control measures correctly, they cannot control their neighbors, and people may feel unmotivated to do anything. The same situation is observed in other endemic cities in Peru [15]. Nevertheless, almost 95% of those surveyed are engaged in positive preventive practices against these diseases (elimination of water containers, cleaning, etc ). Results from a previous study made in Villavicencio in 2003, showed that people had good knowledge about the vector and dengue virus but the practices were not the best [17]; this proves that the situation has not changed in this city in more than 10 years, and the vector control programs have not had an impact on the population that lead to a change in empowerment towards vector control and surveillance of these diseases.
The results presented above are in accordance with the level of knowledge of the diseases but not with the larval indexes found at homes. Thus, it is likely people are not engaging in these preventative practices in a correct way; although they know the theory behind these practices, they are not applying it in the best way. If lower tanks were washed once per week and garbage was disposed of properly, this could ideally control more than 80% of the breeding sites in these neighborhoods. These results are similar to other studies performed in Colombia, where the knowledge of disease transmission and control is considerably good, but attitudes and practices are deficient and the larval index is high [18].
Other similar studies in Colombia, in large cities like Bucaramanga, Yopal and Cartagena, agree that the knowledge in these communities is sketchy, the attitudes are favorable but preventative practices are inadequate to control diseases like dengue, chikungunya or zika [19-21]. Therefore, whether the community has a high level of knowledge or not, the vector control programs have failed to make communities feel committed to improving their health and their environment.
In a city like Villavicencio, which is endemic for many tropical diseases, the exposure to infected mosquitoes occurs not only at home but also at other locations (e.g., job location, school location). This leads to community members becoming perpetually ill and living with chronic diseases. For these people, it is normal for two or three people at home to be sick at the same time. This is the reason that individuals living in endemic areas such as Villavicencio should be knowledgeable about the symptoms of dengue, chikungunya, and zika. According to Gyawali et al. (2016) [17], the greater understanding of the signs and symptoms of these endemic diseases in tropical locations may be based on their close observation of infections contracted by their family members and/or neighbors [22]. Unfortunately, when they feel sick, they do not always seek medical services, likely because one of the system barriers includes few resources since there is an overwhelming amount of patients and few medical doctors. This situation leads people to self-medicate, which can lead to complications of symptoms, especially in those that belong to high-risk groups such as children, elderly, and pregnant individuals. These problems in the health system make people tend to involve God in their response, for example, “God allows mosquitoes to bite us” or “God allows us to get sick.” This “divine” attribution to events related to health-disease processes is common in the Colombian population, giving responsibility for the causes and consequences of the disease to God. In some cases, religion can affect health processes in a negative way, leading to passive styles, in which people give the control of problems to a higher power [23]. Other problems derived from this situation are that most of the surveillance systems are based on passive detection of suspected cases (some without a correct diagnosis), cases without warning signs are generally sent back to their homes with just symptomatic medicinal treatment [24], and a lack of notification to the surveillance system. The case notification system is closely related to vector-control activities [4] and without an alert for a high number of cases, there is no vector-control intervention in the communities.
Aedes aegypti is known to bite mostly during the several hours after dawn and the several hours before dusk. In our study, we found that the majority of people did not know the biting time of the A. aegypti mosquito (55.7%), and they had a poor knowledge about the life cycle of the mosquito as well. All of these factors are essential in the design of programs aimed to educate the residents on personal protection against mosquitoes [16]. None of the residents used mosquito screening as an effective preventive method, but 52% used bed nets and 13% used repellents. Thus, contact between vectors and humans persists.
People are aware of the importance and the responsibility that they have to control mosquitoes at home (in our study, this number was more than 80%) and that the government complements these actions with education, fumigation, and the evaluation of the current strategies. Unfortunately, the majority of residents do not put the recommendations and the strategies into practice because they lack care or are apathetic about the matter.
CONCLUSION
In conclusion it is necessary to review information campaigns, communication, and educational programs promoted in the municipality, as they currently do not empower residents to take adequate preventive measures. These programs need to translate population knowledge about vector borne diseases into positive preventive practices that lead to a reduction in the transmission of dengue, chikungunya and zika in these communities. This will require more infrastructure and resources for long-term sustainability.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Authors had the approval of the medical school faculty (Villavicencio branch) and they had the oral consent of all respondants.
HUMAN AND ANIMAL RIGHTS
No Animals/Humans were used for studies that are base of this research.
CONSENT FOR PUBLICATION
Not applicable.
CONFLICT OF INTEREST
The authors don´t have conflict of interest with this article.
ACKNOWLEDGMENTS
The authors wish to thank Dr. Cesar Garcia Balaguera, students of the Medicine School from the Universidad Cooperativa de Colombia, Villavicencio and the technicians from the Health Secretary of Meta-Colombia.

