All published articles of this journal are available on ScienceDirect.

The Oral Health Team in the Family Health Strategy: Trajectories and Challenges
Authors Info & Affiliations
Abstract
Objectives:
The objective of this study was to review literature focused on the introduction of Brazilian oral healthcare service models, incorporation of Oral Health Teams (OHTs) within the Family Health Strategy (FHS), changes occurring in the work process of the professionals that make up OHTs, difficulties for successful implementation of this new healthcare model and impacts on indicators of oral health.
Methods:
A review of the literature was conducted through an electronic consultation of the Pubmed and Virtual Health Library (VHL) databases published between 2001 and 2016, using a combination of descriptors. We selected 44 studies for review.
Results:
Oral healthcare in Brazil evolved from exclusionary and curative models to those aimed at prevention and promotion of health. The increase in government resources dedicated to oral healthcare in Brazil represented an improvement in access to dental treatment, however, some studies demonstrated that OHTs within the FHS still operate by the traditional curative models.
Conclusion:
Lack of proper planning for hiring OHTs and precariousness of their work contracts were also reported. The need for better managerial planning for implementation of OHTs within the scope of the FHS was demonstrated.
1. INTRODUCTION
In 1994, the Ministry of Health of Brazil (MoH) proposed the implementation of the Family Health Program (FHP), intending to strengthen the Unified Health System (UHS), which aimed at restructuring primary health care in the public health system, prioritizing actions of prevention, promotion and recovery of the health of the population from a surrounding area [1]. Subsequently, the program was consolidated as a Family Health Strategy (FHS), aiming at the reorganization of the Brazilian Primary Health Care (PHC), with no defined duration [2].
Initially, the family health team consisted of a physician, a nurse, a nursing assistant and community health agents [1]. Nevertheless, the population continued to lack access to dental services, and the 1998 National Household Sampling Survey (PNAD in Portuguese) showed that, until then, almost 30 million Brazilians had never visited the dental surgeon [3].
The official insertion of dentistry in the FHS occurred on December 28, 2000, through Ministerial Order No. 1,444, which established a financial incentive for the reorganization of Oral Health (OH) provided by municipalities [4]. Months later, ordinance 267, dated March 6, 2001, regulated this insertion [5]. The purpose of this incorporation was to reorganize the dental care model, expand the population's access to oral health services, and increase preventive actions [4].
With this, the dental surgeon's work process incorporated new assignments, including actions that prioritized the promotion of individuals and families in a comprehensive, interdisciplinary way, and performed not only in the Basic Health Units (BHU) but also in community spaces and households [6].
The financial incentive provided by the MoH and the possibility of reorganizing the oral health actions were pointed out as stimulators of the incorporation of the Oral Health Teams (OHT) in the FHS [7]. However, it has been questioned whether the OHT has fully contemplated all UHS guidelines, pointing to challenges related to, for example, the lack of professional qualification, the lack of integration of the OHT with the rest of the family health team, and the existence of a suppressed demand, left by years of excluding assistance models [6, 8].
In spite of these questions, oral health has been assuming a prominent position in the last years, providing the widening of the population access to dental care and enabling an improvement of this aspect in the epidemiological framework of the Brazilian population [9]. By 2015, 24,467 OHT had been implanted throughout Brazil [10], and the number of first consultations had already reached approximately 30 million [11]. Few studies, however, address the impact of OHT on epidemiological indicators and dental services [12], and there is little scientific evidence of the beneficial impact produced by the OHT [13], since “the issue is not just the coverage amount, it is logical and of care organizational quality” [14].
Based on these considerations, the present study aims to analyze, through a literature review, (i) the evolution of oral health care models, (ii) the insertion of OHT into the FHS, (iii) changes in the work process of the professionals from the team, (iv) the difficulties for the success of this new care model, and (v) the impacts on oral health indicators.
2. METHODS
A review of the literature was conducted through an electronic consultation of the Pubmed and Virtual Health Library (VHL) databases, searching for articles published between January 2001 (year of the OHT implantation into the FHS) and July 2016. Combinations of the following descriptors were used: (1) Family health, (2) primary health care, (3) dentistry, and (4) oral health, in Portuguese and English. Articles in English, Portuguese and Spanish were selected (Table 1).
The review included original studies, case reports, bibliographical reviews and theoretical reflections fully available, which included information on Brazilian oral health policies, the process of the OHT insertion into the FHS, the work process of oral health teams, the impacts on oral health indicators and the comparison of these indicators between areas covered and not covered by the OHT. To include studies of comparable quality, only data published in peer-reviewed journals were considered. Studies on dental programs in other countries, comparative studies of OHT from the same municipality, users’ evaluations of a single OHT, studies evaluating the profile of dental surgeons in a municipality (whether or not members of the OHT), studies that analyzed evaluation programs or instruments, studies carried out exclusively on dentistry graduate courses, and on the profile of the OHT users were excluded.
| Search Strategies | Databases | |||
|---|---|---|---|---|
| Before the duplicity exclusion | After the duplicity exclusion | |||
| BVS | Pubmed | BVS | Pubmed | |
| Family Health + Dentistry | 611 | 192 | 611 | 145 |
| Family Health + Oral Health | 390 | 46 | 390 | 19 |
| Primary Health Care + Dentistry | 415 | 1119 | 415 | 941 |
| Primary Health Care + Oral Health | 132 | 70 | 132 | 56 |
| Total | 1548 | 1427 | 1548 | 1161 |
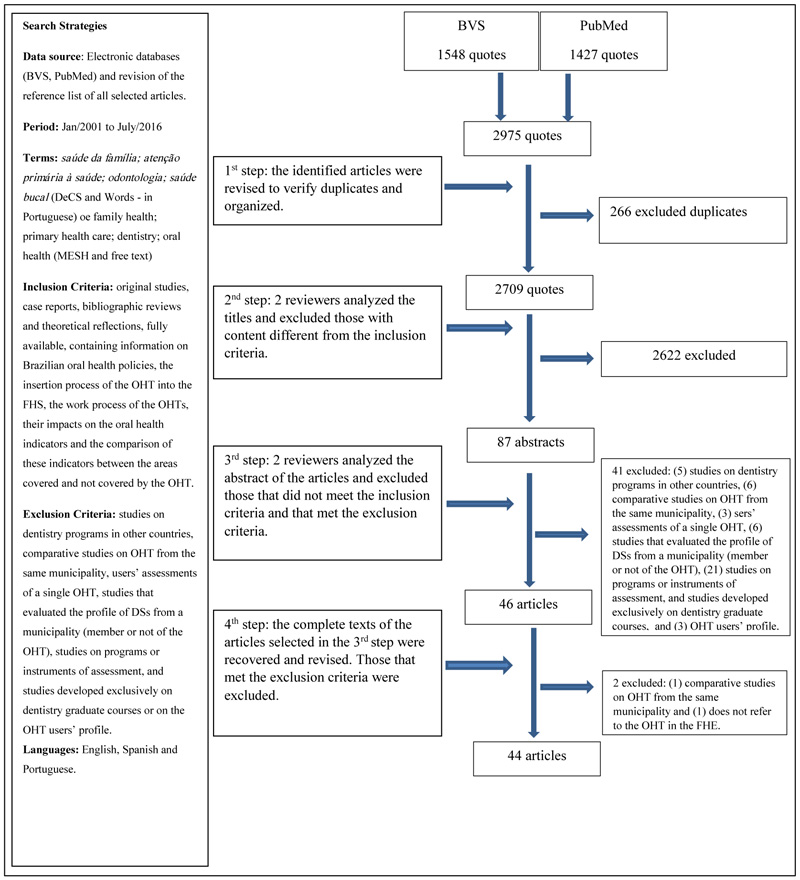
Two reviewers independently conducted the research and selection of the studies. The divergences in all steps of the study selection were resolved by consensus. Fig. (1) describes the selection steps of the studies and the number of articles included in each of them. After the selection, the articles were read and the main results were recorded on a form. Articles that did not present all the information had the author contacted, at least twice, for the due questions.
The articles were read and the results were divided into four categories: historical development of Brazilian oral health policies and their financing; Working process of Oral Health Teams; Oral health indicators after OHT implantation into the FHS and comparison between areas with and without OHT; and Challenges of the OHT in the FHS.
The study included, for discussion, some Ministerial Ordinances referring to the OHT in the FHS, as well as the guidelines of the National Oral Health Policy (PNSB) and the National Curricular Guidelines of the Dentistry Graduate Course.
3. RESULTS AND DISCUSSION
Fig. (1) describes the number of articles included in each of the study selection steps. 2709 papers were screened, of which 2622 were excluded from the reading of the titles. After the initial evaluations, 87 abstracts were reviewed and, from them, 46 complete articles were analyzed, of which 44 articles were included in this systematic review.
Of the 44 studies included, 31 were characterized as original articles, 12 were critical and documentary reviews and 1 case study. The results and discussion are presented below.
3.1. Historical Development of Brazilian Oral Health Policies and their Financing
Dental care in the Brazilian public network was characterized, for years, by assistance models that prioritized restricted population groups [15, 16], leaving for the rest of the population merely curative and mutilating services [16]. An important example of this type of model was the Incremental System, implemented in Brazil in the 1950s by the Foundation for Public Health Special Services (SESP), which represented a milestone in Brazilian free dental care, however, restricted its preventive actions to fluoridation of public water supply and prioritized the restorative treatment of schoolchildren [17]. Subsequently, this model was replaced by the Integral System (or Modified Incremental), which, in practice, did not present substantive changes in relation to the previous one.
Due to the criticism of these models, the Attention Reversal Program (or Universal System) emerged in the late 1980s. This new model decentralized the classic curative attention and sought to control the disease before beginning the definitive restorative treatment. However, despite having been implanted in several municipalities with the intention of “covering the flaws” of the curative Incremental System, it did not take into account the real epidemiological needs of the population [17].
With the creation of the UHS in 1988 - which had as its principles the attention universality, integrality and equity - it was no longer possible to admit the exclusion of clienteles. The UHS sought to “reduce the remaining distances between social rights guaranteed by law and the effective capacity to offer public health services” and had the challenge of obtaining the financial resources to keep the system functioning [16].
PNAD, conducted by the Brazilian Institute of Geography and Statistics (IBGE) in 1998, pointed out that, at that time, about 30 million Brazilians had never gone to the dentist [4]. These data “revealed to Brazilian society information that, from the ethical point of view, confronted the role of the State as provider of actions and health services” [18]. In this context, the MoH proposed, as a strategy to reorganize the PHC, the inclusion of the OHT into the FHP, intending to: institute a new work process focused on the family [16], expand the population's access to promotion, prevention and recovery, and improve the epidemiological indicators of the population [14, 19].
In this sense, the Moh created the Ordinance GM/MS No. 1,444, on December 28, 2000, which officially included oral health in the FHP, providing financial resources to encourage municipalities to adhere to the new model [4]. The rules and guidelines for this inclusion were regulated on March 6, 2001, through Ordinance GM/MS No. 267 [5]. Thus, in the first quarter of 2001, the first OHT [20] begin to be implanted, which could be inserted into two different modalities of habilitation: Mode I, which consisted of one dentist and one oral health assistant (OHA); and Mode II, which consisted of one dentist, one OHA and one oral health technician (OHTe). Initially, ordinance 1,444/2000 established the implementation of one OHT for each two FHP teams (an average of 6,900 patients to be attended by each OHT). Subsequently, Ordinance GM/MS 673, dated June 3, 2003, established that as many OHTs as the FHP teams in operation in the municipalities could be deployed [21, 22].
The financial incentive to implement the OHT and to assist in the monthly costing of these teams was transferred to the municipalities through the variable Basic Attention Floor (BAF) [2], and they had a gradual and considerable increase over the years (Table 2).
| Year | Ordinance | Costing | Incentive* |
|---|---|---|---|
| 2000 | Ordinance GM/MS No. 1.444 | Modality I –R$ 13,000.00 | R$ 5,000.00 |
| Modality II –R$ 16,000.00 | |||
| 2003 | Ordinance GM/MS No. 673 | Modality I –R$ 15,600.00 | R$ 5,000.00 |
| Modality II – R$ 19,200.00 | |||
| 2004 | Ordinance GM/MS No. 74 | Modality I –R$ 20,400.00 | R$ 6,000.00 + R$ 1,000.00 ** |
| Modality II – R$ 26,400.00 | |||
| 2006 | Ordinance GM/MS No. 650 | Modality I –R$ 20,400.00 | R$ 7,000.00 |
| Modality II – R$ 26,400.00 | |||
| 2008 | Ordinance GM/MS No. 2.489 | Modality I –R$ 22,800.00 | R$ 7,000.00 |
| Modality II – R$ 29,400.00 | |||
| Ordinance GM/MS No. 3.066 | Modality I –R$ 24,000.00 | R$ 7,000.00 | |
| Modality II – R$ 31,200.00 | |||
| 2011 | Ordinance GM/MS No. 1.599 | Modality I –R$ 25,400.00 | R$ 7,000.00 |
| Modality II – R$ 33,600.00 | |||
| 2012 | Ordinance GM/MS No. 978 | Modality I –R$ 26,760.00 | R$ 7,000.00 |
| Modality II – R$ 35,760.00 |
Source: Own elaboration from the Ordinances GM/MS No. 1,444 [4], GM/MS No. 673 [22], GM/MS No. 74 [23], GM/MS No. 650 [24], GM/MS No. 2,489 [25], GM/MS No. 3,066 [26], GM/MS No. 1,599 [27] and GM/MS No. 978 [28].
In 2004, the guidelines of the National Oral Health Policy (PNSB) [29] were launched, which sought, among other things, to guide the reorganization of the oral health care model, and to guarantee the integral care of specialized actions through the creation of Dental Specialties Centers (DSC) and Regional Dental Prosthesis Laboratories (RDPL) [30]. The PNSB represented a significant increase in the federal government's investment in oral health, from R$ 58 million in 2002 to R$ 1.3 billion in 2006 [31].
In 2006, the document “The Pact for Health” changed the way in which the SUS funding occurring, linking them into five large blocks. The resources for PNSB were contemplated in three of these blocks: APS (resources destined to oral health care in the FHS, within the variable BFA); UHS Management (costing of actions that increase access to the service, such as the implementation of DSCs); and Medium- and High-Care Complexities (a resource designed to provide a permanent incentive for the maintenance of DSCs and the payment of prosthetics performed by the RDPL). The health pact also redefined the responsibilities of each manager according to the health needs of the population, in the pursuit of social equity [2].
In 2009, MoH, through Ordinance No. 2,372, stipulated the provision of new dental equipment for OHTs, considering encouraging the reorganization of oral health care, expanding the population's access to OH promotion, prevention and recovery actions, and improving the epidemiological indices [32]. For Pucca-Junior et al. [33], this determination also aimed at improving the working conditions of dentist and making oral health actions more efficient.
Importantly, the federal financial incentive does not, and did not, intend to be sufficient to maintain the costs related to OH [31], with states and municipalities being responsible for the financial supplementation for the additional expenses related to the maintenance of equipment, the purchase of instruments, inputs and specific consumables [34, 35], and the payment of professionals.
The inclusion of OHT in the FHS was an opportunity to replace the exclusive models of attention to OH [33] and improve the quality of life of the population [36]. It's actions aimed at the expansion and optimization of dental services, through the knowledge of the needs of the community where each OHT was inserted [37].
3.2. Working Process of Oral Health Teams
The dentist, “in order to work in the FHS, needs to develop skills beyond its 'knowledge core', leaving the isolation of practice restricted to the dental office and equipment, assuming a new role in the team and actions to promote health” [38].
The increase in the contribution of OH investment in Brazil in recent years has represented an expansion of coverage of dental services and equity of access to these services [39]. However, analyzing if there are changes in the work process of the dentist [40, 41] is necessary, in order to contemplate the UHS principles. In this sense, some studies have shown that the OHT inserted in the FHS still maintains the predominance of the characteristics of the traditional care models [15, 20, 37, 40, 42-45], which indicates that all the financial incentive seems not to be enough to lead to the necessary changes in professional practice.
The maintenance of the work process is contrary to the operational characteristic of reorganization of OH's actions [5]. The guidelines of the PNSB propose an adaptation of the work process to the new care model, and require, among other things, that the OHT not only works in the dental-technical field, but that it can interact with professionals from other areas, in order to expand their knowledge and allow the approach of the individual as a whole [29].
In interdisciplinarity, the sharing of knowledge and the complementarity of knowledge is essential to address health problems and risk factors of the population [9, 18], produce more effective care for the patient [14], and approach the patient integrally [3]. Thus, acting in the UHS requires the professional to be able to “think no more about a subject-individual, but about a collective-subject” [46].
However, some results have shown a challenge regarding the performance of OHT in an interdisciplinary way with the rest of the team [3, 6-9, 15, 46-49], which may be justified by the fact that dentistry was later incorporated into the FHS [3, 19, 50] and/or by the characteristics of vocational training [3]. For the dentist that works in the FHS, as important as the technical skill is the knowledge in the collective oral health area and the development of the citizen conscience [18], both still poorly contemplated in the dentistry graduate courses, which in large part still form a professional focused on the biomedical paradigm and with a predominantly procedure-centered approach [14, 51].
The National Curricular Guidelines of the Dentistry Graduate Course of 2002 include among its objectives: to train professionals who respect the ethical principles inherent to professional practice, who are committed to the human being, who exercise their profession in an articulated way to the social context, and who have the necessary knowledge to act at all levels of health care: promotion, prevention, maintenance, protection and recovery of health [52].
In order to repair possible failures in the dentist formation and to adapt it to the new care model, public policies that incorporate training programs are necessary to enable the dentist to act in accordance with the guidelines of the FHS [6, 38, 51, 53], since nothing can guarantee “that there will be changes in the current care model if the professionals do not change the way they produce care” [9].
Under the responsibility of the health departments of the municipalities and states [2, 5], the training facilitates the understanding of the professionals about the objectives of the program. Some municipalities performed this training [19, 22], however, most of the published studies report that dentist are being inserted into the FHS without training [3, 18, 38, 40, 48], which may be causing the reproduction of the traditional curative model.
In this change of the work process, preventive-educational actions are important, since it has low complexity and high population coverage [22]. They must be carried out in a rational and reasonable manner, with evaluations to verify their effectiveness [8]. Aquilante and Aciole [42] reported, in their study, the periodic practice of educational groups, organized by life cycles, which is in line with the guidelines of the PNSB, which states that these actions should be offered in a continuous way and to different priority groups [29]. Nevertheless, studies have reported that schools and day-care centers have been places of choice for these actions [3, 8, 40], which can be seen as a remnant of the practices of traditional models of oral health [42]. In addition, a recent study has shown that there is still a low number of OH teams who perform preventive dental procedures, such as dental sealant, topical application of fluoride, among others [54].
Knowing the reality of the area of operation is essential to plan a service in an equitable and ethical way. The realization, together with the other members of the team, of the territorialization and the planning of health actions, are also part of the attributions of the dentist [2]. Knowing the epidemiological profile and the socioeconomic characteristics of the community are essential, in order to develop priority promotion, protection and recovery actions [29], seeking to reorganize oral health care in PHC with a view to the UHS guidelines [47]. Although there is a study that reports this fact [37], attention has been drawn to the lack of accomplishment of the situational diagnosis of the area of performance [9, 20].
The realization of the agenda should be widely discussed with the community in local and municipal health councils [55] because the population's knowledge on their needs and the limitations of the System favors the development of policies appropriate to the epidemiological profile of the community [56]. A study carried out by Cruz et al. [18] on the work process of the OHT in the city of Curitiba identified an important participation of the dentist in the Local Health Councils. On the other hand, the study by Moraes et al. [6] showed little involvement of the oral health (OH) professionals with the living conditions of the community.
The work carried out by the dentist outside the health unit is essential to know the social reality of the population and for professionals to strengthen the bonds formed with the community [9]. The home visit (HV), in particular, increases OHT's bond with the family and is a way to bring access to oral health services to people with limited mobility [6]. Unfortunately, studies report the non-implementation of this practice by the OHT [6, 43]. Ordinance 267/2001 already had as a common attribution to all of the FHS the performance of the HV, according to the identified needs [5] and the PNSB/2004 guidelines reaffirmed the importance of this practice, mentioning it as an opportunity to identify oral lesions for the early detection of oral cancer [29]. However, a study with Brazilian dental surgeons identified the low adherence of these professionals to the actions related to oral cancer screening [57].
Another important point for the transformation of the OH care model, reported in some studies, is the qualification of the Community Health Agents (CHA) to be multipliers of oral health information [37, 58], and, in fact, ordinance 267 of 2001 brought as one of the specific duties of the dental surgeon the qualification of all the team on oral health [5].
Reis et al. [38] draw attention to the need for a combination of autonomy and responsibility in the working process of the dentist so that its actions are resolute. They consider that the presence of norms is essential; however, they also state that the singularity of the work practice of each professional in their reality is fundamental. They emphasize that freedom at work favors creativity, but it relates to the commitment and the affinity of the professional with its work [38].
Finally, Cruz et al. [18] reported in their study that “there seems to be a reasonable understanding about the focus of actions being directed to the family nucleus and not to the individual alone”, which corroborates one of the bases for the reorganization of oral health, which is the definition of the family as the central nucleus of approach [5].
3.3. Oral Health Indicators After the OHT Implementation in the FHS and Comparison between Areas with and Without the Implanted OHT
Since the official insertion of the OHT into the FHS, the number of teams incorporated into the OHT has been increasing, from 2,248 in 2001 to 24,467 teams in 2015, in both modalities. These teams were distributed in 1,288 municipalities in 2001, increasing to 5,014 municipalities (90% of Brazilian municipalities) in 2015 [10]. This increase in the number of OHT implanted facilitated the population's access to oral health services, leading the percentage of Brazilians who had never had access to dental consultations to decline from 18.7% in 1998 to 15.9% in 2003, and, later, to 11.7% in 2008 [59].
The increase in the number of dentists registered in the UHS led to an increase in the number of first dental consultations (indicator used to assess access to oral health services), which increased from approximately 21.5 million in 2001 to almost 30 million in 2015 [11]. Corrêa and Celeste [60] analyzed the association between OHT coverage in the FHS and increased outpatient production in Brazilian municipalities between 1999 and 2011, and reported that the average rate of procedures increased 49.5% in 2011 in relation to 1999, which shows that this incorporation is associated with greater chances of increasing rates of use of dental services, and associates this increase with meeting the repressed demand and the 40-hour weekly load of the OHT.
Analyzing data from the UHS Outpatient Information System on the use of oral health services in the period between 2001 and 2015, the rate of preventive procedures increased 35% (from 10.95/thousand in 2001 to 14.77/ thousand inhabitants in 2015); the rate of restorations increased 15.5% (from 16.17/thousand inhabitants in 2001 to 18.67/thousand inhabitants in 2015); and the rate of exodontias decreased 10.1% (from 9.20/thousand inhabitants in 2011 to 8.18/thousand inhabitants in 2015) [11]. Regarding the exodontia, a study carried out in the states of the Brazilian southern region, between 2000 and 2005, already showed a downward trend in the ratio between the number of permanent tooth exodontia and the number of individual dental procedures in the PHC. Rio Grande do Sul had the highest rate of decline in this indicator, from 14.06 in 2000 to 8.49 in 2005 [61].
Studies performed in some Brazilian municipalities to analyze the evolution of the indicators after the insertion of the OHT into the FHS showed that, with the increase in the average number of OHT over the years, the indicators of access [62-64], income, and the percentage of urgencies also increased, and the number of supervised brushings increased considerably [62]. The increase in population coverage by OHT was also related to the reduction of periodontal problems in the elderly [63]. However, there are studies that have identified inequalities in this access [65].
The study by Carvalho et al [66] also found a positive result, showing that adolescents living in areas with OHT coverage in FHS were less prone to more severe tooth pain when compared to those living in areas with traditional dental treatment, and suggesting that early diagnosis and treatment of minor injuries may have reduced dental pain.
Brunhauser et al. [41] reported in their study that access to dental consultation was considered easier by users of the FHS in relation to the users of traditional basic health units. However, with respect to satisfaction regarding the resolution of care, “users attended at the conventional BHU, proportionally, showed greater satisfaction with their reported masticatory capacity after receiving treatment”, compared to those attended at the FHS, which calls attention to the need to reflect if changes are actually occurring in the oral health care model.
Pereira et al. [67] conducted a study in Natal-RN, comparing areas with OHT in the FHS, areas covered by FHS units with a dentist without linking to the family health team, and areas covered by traditional or uncovered basic health units, and found that. The impact of oral health on FHS was only significant when compared to areas covered by traditional units or without any coverage, i.e., the access to dental service was not different, when compared to the FHS with OHT or with traditional oral health service. According to the author, this analysis would isolate the effect of the presence of the OHT in the FHS [67].
A study carried out in Brazil between the periods of 1998 and 2012 showed that municipalities with higher OHT coverage have, on average, a higher rate of dental extraction [68]. A study in the south of the country comparing oral health of adolescents living in areas covered or not covered by the OHT in the FHS found similar result, which showed that there were no significant differences in the comparison of almost all oral health outcomes between the two areas compared, with the exception of dental floss, which showed that young people from areas not covered by the OHT in the FHS had almost half of the dental loss compared to adolescents in the covered areas [13]. The author pondered that these outcomes may have been caused by maintaining the traditional transgender work process of the OHT and that the greater amount of tooth loss in areas with the OHT may be justified by the increased access to these traditional mutilating practices.
Research carried out in the Brazilian Northeast comparing the impact of oral health indicators in areas with implanted OHT, and areas with dental care of the traditional model or without care, demonstrated positive results in relation to access to collective preventive actions and the treatment of toothache; however, found a negative or no effect in relation to restorative treatment and exodontia, and suggested “a poor performance of the incorporation of oral health in FHS” [12].
Few studies have been done to analyze the dentist inclusion into the OHT [67], and to assess its impact on epidemiological indicators [12, 67, 69]. Ely et al. [13] add that there is little evidence of the beneficial impact of the OHT. This statement is in line with a study that points out that the incorporation of the OHT into the FHS is producing results that could be better, taking into account the size of the investment made in the program and the proposed change of the traditional model [12]. In this sense, the way strategies are being implemented in each location is crucial to their success [12, 67]. For Mattos et al. [7], “the lack of training of managers certainly impacts considerably on the way the implementation of the new care model has been happening in the Brazilian municipalities”.
The OHT were inserted in Niteroi-RJ, in 2010, and, in this municipality, the dentists participated in an introductory course to know the territory, population profile and methodology of the Family Medical Program (FMP) of the municipality, besides having a schedule set in the weekly agenda of dental health professionals for permanent education along with the other members of the FMP team. These professionals carry out activities with specific groups, home visits, interdisciplinary meetings and activities at schools, kindergartens and other community institutions [70], corroborating the expectations of the new Oral Health model proposed by the federal government.
3.4. Challenges of the OHTs in the FHS
With all the advances that occurred in the attention to OH in Brazil after its implantation in the FHS, there are still reports of factors that prevent its full success. Soares [71] described in his study that, although Brazilian OH policies have made significant progress regarding federal government participation and the constitution of norms, they still present challenges regarding the implementation process and the participation of state and municipal governments. Ordinance 648/2006 assigns the responsibility of the states to allocate resources to compose the tripartite funding of PHC, and the municipalities have the responsibility to “guarantee the necessary infrastructure for the operation of the Basic Health Units, providing them with material resources, equipment and sufficient inputs” [2]. It is clear, therefore, that although the federal government passes on an incentive for the implementation and maintenance of the OHT, it is not solely responsible for this.
The FHS has as its foundations the development of relationships of bonding and accountability between the teams and the surrounding population, the guarantee of the continuity of health actions, and the longitudinality of care [2, 72]. Therefore, the turnover of professionals, due to the precariousness of the employment relationship and the form of hiring to work in the OHT, found in some studies [3, 7, 8, 19, 20, 22, 43, 48, 51, 73], has proved to be a complication. Instability, the precariousness of labor relations and the lack of a job and salary plan interfere with the workers' interest in the system and the commitment to work and community [43, 50]. Another factor that may be compromising the professional's dedication to the FHS is the dissatisfaction with low remuneration [3, 8, 20, 48], and/or the salary discrepancy with other members with a college degree of the family health team [18, 19, 48].
Studies also reported failure to meet the weekly workload recommended by the MoH of 40 hours [8, 43] and this may interfere in the formation of the link with the community and in the development of prevention, promotion and rehabilitation activities [8]. In this sense, the municipalities should ensure full-time compliance by all professionals [2].
Another factor that was characterized as a challenge for the OHT was the repressed demand, reported by some authors [3, 6, 20, 40, 43, 46, 48, 49, 51], which can lead to an excessive workload and interfere with the OHT's performance in integrating with the team and complying with the principle of access universality. In addition, it can lead to the dentist wear [40], be associated with the compromise of the quality of the service [48], and hinders forming the link with the assigned population [43] and maintaining the service offer [31].
Another issue, already pointed out as a “critical node” by Baldani et al. [19], in 2001 in Paraná, was the difficulty of referrals of complex cases, a fact confirmed in later studies [8, 18, 20]. One of the bases of the reorientation of oral health, described in Decree 267/2001, is the integrality of the care provided to the enrolled population; however, guaranteeing this right has become a challenge for oral health, since the expansion of the secondary and tertiary care network did not keep pace with the growth in PHC's service offers. With this in mind, and in order to increase care with services offered at the secondary and tertiary levels, the federal government created a financial contribution to the PNSB for the implantation and/or improvement of DSCs [29, 74], and ordinance 648/2006 placed the municipalities in charge of organizing the flow of users and guaranteeing their reference to services outside the scope of PHC [2]. However, it is not recommended to open DSCs in municipalities that do not have a properly structured PHC [75]. However, a recent study has shown that DSCs are failing to absorb the demand for specialized treatment, generating large queues and compromising the wholeness of care [42, 76].
“The FHS approach to the dentist work goes far beyond clinical work because it is a logic of thinking about health in a comprehensive and extended way” [50]. “In the context of oral health, public health policies must guarantee access to comprehensive dental care for vulnerable individuals” [77]. In this sense, the provision of oral health services in Brazil has advanced from a panorama of the limited supply of procedures of low complexity to the accomplishment of specialized procedures, aiming at the integrality of the care [34]. However, to Costa et al. [77] “there is still a lot to do so that, in fact, healthcare is integral”. The structuring of care implemented in PHC and access to secondary care directly influence care completeness [78]. Thus, the oral health care network needs to be expanded, refined and solidified [79].
CONCLUSION
The federal government's proposal to include OHTs in the FHS, replacing the traditional models of oral health care, was an important step towards bringing dental care to the population in a more ethical and equitable manner, with a focus on family and making the teams responsible for the oral health problems of the population of a geographically delimited territory, in accordance with the UHS principles.
In fact, with the increase in the financial contribution destined by the federal government to this area, a great change has taken place in the epidemiological scenario of oral health, with improvements in the indicators regarding the population's access to dental treatment. Nevertheless, studies also report the absence of a positive impact on the quality of the dental service, when comparing areas with or without OHT inserted in the FHS.
The literature points as causes: lack of planning for the insertion of the OHT, the lack of qualification of the professionals to integrate the FHS, the precariousness of the form of hiring and the employment bond, the devaluation of the professionals, the difficulties of changing the work process and integration of the OHT with the rest of the family health team, and the technical training of the dentist.
Therefore, the financial investment alone was not sufficient to meet all the proposals of the PNSB, and that even after 15 years of the implementation of the OHT in the FHS, many changes are still necessary. In addition to a plan by the managers for the implementation of the OHT in the FHS of their municipalities, it is necessary to train and value the professionals, in order to have a real commitment of the OHT with the population and with the new care model.
CONSENT FOR PUBLICATION
Not applicable.
CONFLICTS OF INTEREST
The authors declare that there is no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
This study was supported by the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq – National Council for Scientific and Technological Development) and the Research Program of the Faculdade Dinâmica do Vale do Piranga (PROAPP/FADIP).

